
Abstract
This study examined the relationship between continuing bonds (CBs) among 50 bereaved youth (ages 11–17) and their bereaved adult caregivers, and predictors of CBs among youth. Results indicated there was not a significant relationship between caregiver CB and youth CB. However, significant relationships were found between youth bereavement symptomatology, their relationship to the deceased, and youth CB. Specifically, youth with higher levels of symptomatology and those who lost an immediate family member were more likely to maintain CBs. Results suggest the need for practitioners to incorporate grief symptomatology and CBs in assessment and intervention with bereaved youth.
Although grief is a universal experience impacting the lives of many children and adolescents each year, not much study has been afforded to this population. Further, the concept of a continuing bond (CB) or ongoing relationship to the deceased and its role as adaptive or maladaptive in the bereavement process is in its infancy of research among adult populations and is largely unstudied among bereaved youth. Although several studies have examined bereaved adults and a CB (e.g., Field, Gal-Oz, & Bonnano, 2003; Field, Nichols, Holen, & Horowitz, 1999), very few have had primary aims to do so with bereaved children or adolescents (e.g., Foster et al., 2011; Wood, Byram, Gosling, & Stokes, 2012). In addition, only a few studies have examined CB and bereaved children as an aside of a larger research project and aim (e.g., Hogan & DeSantis, 1992; Nickman, Silverman, & Normand, 1998; Silverman, Baker, Cait, & Boerner, 2003; Silverman, Nickman, & Worden, 1992; Silverman & Worden, 1992). A fairly recent topic of study, caregiver CBs to the deceased, and its relationship to child CBs to the deceased has not thoroughly been investigated in the literature. The purpose of this study was to examine the relationship between CBs among youth and their adult caregivers. Further, the relationship between caregiver and youth bereavement symptomatology was investigated and predictors of CBs among youth were identified.
CBs Defined
Attachment theory is widely used today to hypothesize the strong impact that early attachment relationships have on an individual’s adult relationships (Noppe, 2000; Stroebe, Schut, & Stroebe, 2005). Bowlby (1980) stressed that at every age, people’s lives revolve around the intimate attachments they form. Attachment has been referred to as primal or instinctual indicating that it is natural for attachment bonds to continue following separation, abuse, divorce, or death (Bonanno & Kaltman, 1999; Noppe, 2000; Shaver & Tancredy, 2001). While research on CBs among children and adolescents is limited, it has revealed that a majority of bereaved children make attempts to maintain some form of connection to the deceased after death (e.g., Bowlby, 1980; Foster et al., 2011; Silverman & Nickman, 1996; Silverman & Worden, 1992). The bereaved experience CBs in a variety of ways and such bonds have important implications in mourning behaviors and coping following a death. The nature and type of this relationship is different for each bereaved individual (Noppe, 2000). Benore and Park (2004) defined continuing attachment as “the bereaved person’s belief in an active, on-going relationship with the deceased” (p. 9). They described numerous representations of such relationships among the bereaved and deceased. These included maintaining attachment through memories, completing rituals or sharing stories, feelings of “spirit” or “presence,” manifestations through dreams or flashbacks, assuming qualities or characteristics of the deceased, maintaining belongings as linking objects to the deceased, allowing the deceased to remain as an active role model, and having direct communication by visiting the cemetery or through prayer. The continued attachment is often formed as a mental representation of the deceased in which survivors imagine what the deceased would say or do in certain situations. In addition, they may attempt to reflect on memories or to seek out previously unknown information about the person who died (Boerner & Heckhausen, 2003). Klass (1993) discussed that CBs often take the form of an “inner representation” of the deceased (p. 345). Indications of the inner representation included sensing the deceased’s presence, believing the deceased continues to influence the survivor’s life, hallucinations, and the incorporation of the deceased’s traits into the survivor’s personality. The aforementioned inner representation is commonly achieved through linking objects, memories of the deceased, and religious practices and beliefs (Klass, 1993).
Stroebe et al. (2005) noted that although a bereaved individual will eventually accept that the deceased is not physically present, he or she will almost always remain a part of the survivor’s continued life. In this vein, CBs can be maintained even after one completely accepts the death of a loved one (Field, Gao, & Paderna, 2005). Survivors are often acutely aware of the physical loss while experiencing the emotional presence to the deceased (Hogan & DeSantis, 1992). Consistent with the instrument used to measure this construct, this study defines CB as an “ongoing relationship with the deceased” (Rubin et al., 2009, p. 309; Rubin, 1999).
Just as no two people mourn exactly alike, it is assumed that the nature of expression and strength of a CB largely differs between all bereaved children, adolescents, and adults. Minimal research has explored the association between adult caregiver CBs and those of their bereaved youth counterparts. Walsh and McGoldrick (2013) note that most bereavement studies focus on either youth or parental bereavement, but it is essential for researchers to investigate the family unit and consider accompanying family dynamics of adaptation following a death. In a qualitative study of 42 families bereaved by the death of a child to cancer, Foster et al. (2011) identified that both parents and their surviving children maintained continuing bonds to the deceased. Of note, 100% of parents and 92% of bereaved siblings experienced “purposeful reminders” of the child who died and only 18% of parents and 8% of siblings reported having “nonpurposeful” or unexpected reminders of the deceased (p. 426). A few of the purposeful reminders included talking or writing to the deceased, thinking about the person who died, maintaining personal belongings of the deceased, using visual reminders such as looking at pictures or videos, and engaging in memorialization activities such as visiting the cemetery or maintaining ashes (Foster et al., 2011).
Factors Influencing the Continued Relationship With the Deceased
Very few studies have included an exploration of youth CBs, and even fewer studies have primarily aimed to examine the relationship between caregiver CBs and youth CBs. Although bereavement practitioners frequently encounter children expressing CBs, little is known about this construct. The current study also helped fill the gap in the literature by examining the relationship between CBs and youth symptomatology. The following primary research questions were asked: (a) To what extent are caregiver CB and caregiver symptomatology associated with youth CB? and (b) To what extent are caregiver CB and youth CB associated with youth symptomatology? In addition, the following exploratory question was examined: (a) What caregiver variables, youth variables, demographic variables, and death-related variables significantly impact youth CBs? This study explored the following nine variables and their potential influence on CBs among youth: caregiver CBs, caregiver symptomatology, youth CBs, youth symptomatology, child’s age/developmental level, spirituality, time elapsed since death, nature of death, and relationship to the deceased.
Method
Participants and Procedures
This study was approved by the University of South Florida institutional review board. Youth participants were clients of one of the two bereavement centers affiliated with a large not-for-profit hospice provider in the United States. Collectively, the centers serve approximately 800 bereaved adults and youth per year through various supportive services including support groups facilitated by trained peer-facilitators or mental health professionals, weekend bereavement camps, and individual counseling. Most services are free of charge and the centers often receive referrals when a youth is identified as having experienced a death. One primary adult caregiver of each youth (bereaved by the same death as the child) also participated. Participants were required to be English speaking, and youth were between the ages of 11 and 17 years old.
Current eligible clients participating in any of the centers’ bereavement programs (e.g., support group, individual counseling, and bereavement camp) were sent recruitment letters via e-mail and standard mail. Eligible clients were also provided recruitment letters and information about the study in person by their bereavement counselors. Those interested in participating were scheduled for data collection appointments at which time assessment packets were completed.
Caregivers and youth were in separate rooms when completing study instruments. The principal investigator and trained staff members of the bereavement center administered the surveys. Average time of instrument completion was 25 minutes, and families received one US $20 gift card as compensation for participation.
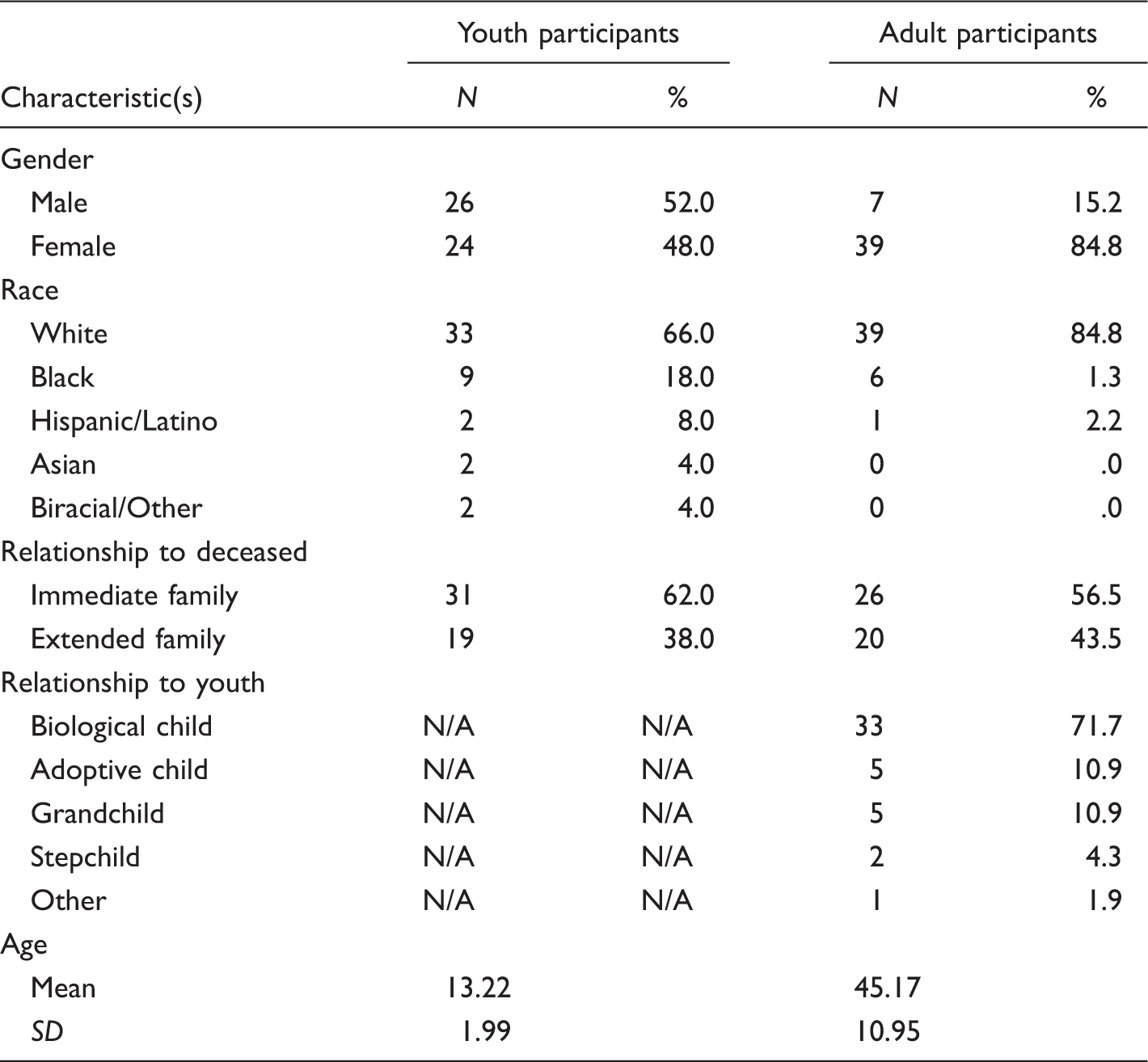
The sample consisted of 50 bereaved youth age 11 to 17 with a mean age of 13.32 (SD = 1.99) and their 46 adult caregivers with a mean age of 45.17 (SD = 10.95). Of these 46 families, 42 consisted of one caregiver with one participating youth, and four were made up of one caregiver with two participating siblings.
Measures
Demographic Questionnaire
A demographic form was completed by the adult caregiver to ensure accuracy of data collection and included descriptive variables such as gender and race/ethnicity. The caregiver section assessed for caregiver demographic and death-related variables including age, relationship to youth participant, and relationship to the deceased. The youth section assessed for youth demographic and death-related variables including age, relationship to the deceased, child’s religion, degree of family religious belief or observation, child’s age at time of death, cause of death, and nature of death.
Two-Track Bereavement Questionnaire (TTBQ)
Subscales from the TTBQ (Rubin et al., 2009) were utilized to measure caregiver symptomatology, caregiver CB, and youth CB. The instrument’s two axes are often referred to as “tracks,” and each track includes Likert-type scale items on a 5-point continuum (e.g., true, mostly true, partly true, mostly not true, and not true). Total scores and subscale scores for the TTBQ are divided by the total number of items and indicated on a 1 to 5 scale with 1 indicating very low scores and 5 indicating very high scores. The TTBQ was developed based on the Two-Track Model of Bereavement (TTMoB). Through a multidimensional analysis, the TTBQ seeks to understand the bereavement process by evaluating both the bereaved’s “general biopsychosocial functioning” on Track I and the nature of the “ongoing relationship with the deceased” on Track II (Rubin et al., 2009, p. 309; Rubin, 1999).
Track I of the TTBQ was used to measure caregiver symptomatology and comprised 26 items from the General Biopsychosocial Functioning and Traumatic Perception of the Loss subscales. The General Biopsychosocial Functioning subscale includes 14 items related to problems in functioning after the death. Higher scores indicate increased symptomatology and difficulties since the death. The Traumatic Perception of Loss subscale includes 12 items related to the difficulty integrating the experience of loss, the traumatic circumstances or perceived trauma of the death, and the sudden nature of the death. Higher scores indicate higher perception of trauma (Rubin et al., 2009). In the current study, the overall reliability was α = .89 (General Biopsychosocial Functioning, α = .84; Perception of Trauma, α = .81).
Track II, the relationship to the deceased, comprised 30 items from three subscales (Relational Active Grieving, Close and Positive Relationship to the Deceased, and Conflictual Relationship with the Deceased) and was used to measure caregiver CB and youth CB in this study. Track II evaluates the features of the CB to the deceased by analyzing whether the attachment characterizes one of disorganization or reorganization (Rubin, 1999; Rubin et al., 2009). The Relational Active Grieving subscale includes 16 items examining how the bereaved is relocating the relationship to the deceased from one of presence to one of memory. Higher scores indicate an “intensity of contact in the relationship” (Rubin et al., 2009, p. 324). The Close and Positive Relationship to the Deceased subscale includes eight items and focuses on the relationship to the deceased 2 years prior to the death. Higher scores indicate a “more intense and positive” preloss relationship (Rubin et al., 2009, p. 324). The Conflictual Relationship to the Deceased subscale includes six items related to the nature of conflict present in the relationship 2 years prior to the death and “thoughts of the conflict” experienced by the survivor in the week preceding scale completion (Rubin et al., 2009, p. 325). Higher scores indicate higher conflict in the ongoing relationship to the deceased.
Track II, used to measure Adult CB, had an internal consistency of α = .86 (Relational Active Grieving, α = .89; Close and Positive Relationship to the deceased, α = .87; Conflictual Relationship to the Deceased, α = .72). Given that the TTBQ has only been utilized with adults, and the lack of measures of CBs for youth, Track II was adapted and piloted for use with youth before it was administered for the present study. The first author made minor modifications of clarification to a few instrument items such as adding the word “ache” next to the word “yearn” and adding the phrase “feeling comfortable around each other” next to the phrase “sense of comfort or flow.” The instrument was pilot tested using a sample of eight bereaved youth (16% of the current sample size) from one of the bereavement centers for the current study, and these youth were not included in the final study sample. When administered to the pilot sample, the overall 30 item Track II youth version had an internal consistency reliability of α = .88 (Relational Active Grieving, α = .86; Close and Positive Relationship to the Deceased, α = .88; Conflictual Relationship to the Deceased, α = .67). Therefore, Track II of the TTBQ was utilized to measure youth CB in the current study. When administered in the current study, the overall scale demonstrated good reliability on the total score, α = .84; Relational Active Grieving subscale, α = .88; and Close and Positive Relationship to the Deceased subscale, α = .85, but the Conflictual Relationship to the Deceased subscale had a lower reliability (α = .47).
Strengths and Difficulties Questionnaire (SDQ)
To date, there is not a well-validated measure of child bereavement symptomatology. Because symptoms of bereavement include sadness, depression, anxiety, somatic complaints, fears, and behavioral disturbances, many youth bereavement researchers and practitioners use general scales assessing emotional or behavioral factors among children such as the Child Behavior Checklist (CBCL; e.g., Sandler et al., 2003; Worden & Silverman, 1996). This study utilized the SDQ self-report scale for youth ages 11 to 17 (SDQ 11–17) (Goodman, 1997) to measure youth symptomatology. The 25-item SDQ was chosen over the 117-item CBCL due to its brevity and its strong correlation with the CBCL (Goodman & Scott, 1999). The instrument items are on a 3-point scale (not true, somewhat true, certainly true) with a score range of 0 to 40. The internal consistency of the SDQ in this study was α = .80.
Spiritual Well-Being Scale (SWBS)
An adapted version of the SWBS (Ellison, 1983) was utilized to measure spirituality among youth participants. The SWBS has been widely used to measure spirituality in a number of studies among diverse populations (Paloutzian & Ellison, 2009). This study utilized an adapted 10-item version of the SWBS previously used in a study of 134 adolescents ages 14 to 18 (Cotton, Larkin, Hoopes, Cromer, & Rosenthal, 2005). The adapted version includes 5 items each from the Religious Well-Being and Existential Well-Being subscales. The adapted version is on a 5-point Likert-type scale (strongly agree, agree, neither agree or disagree, disagree, and strongly disagree) with a score range of 10 to 50. The internal consistency of the adapted 10-item SWBS in this study was α = .82.
Analysis
All data were analyzed using the Statistical Package for the Social Sciences (SPSS), Version 21.0. Prior to conducting statistical analyses, SPSS entries were double checked against the hard copies of data collection instruments to ensure accuracy. In addition, data were screened for missing data and assumptions of each parametric test were verified. Because less than .02% of all scale data points for youth and adult participants were missing, a mean substitution was employed. Bivariate correlations were conducted among study variables and a linear multiple regression analysis was conducted to identify predictors of youth CB to the deceased. A rejection level of .05 was set prior to conducting analyses. Due to the small sample size, and exploratory nature of this study, a type I correction was not employed. Prior to linear multiple regression analysis, a power analysis was conducted which revealed a sample of 50 participants with three predictor variables would yield a level of power of .83 for a cumulative R2 = .20.
To further explore the dyadic relationship between youth and caregivers, the data were analyzed following the actor–partner interdependence model described by Cook and Kenny (2005) and the actor–partner model (APM) described by Gonzalez and Griffin (2012), using 50 caregiver–youth dyads as the unit of analysis rather than the 96 study participants. Specific to this study, the analysis was undertaken to examine the extent to which youth symptomatology could be predicted by both the youth’s and their caregiver’s CB with the deceased. Unlike some other dyadic analysis approaches (e.g., latent variable approach), the APM model uses observed variables directly (Gonzalez & Griffin, 2012). Gonzalez and Griffin (2012) further noted that the APM model is preferred when investigators want to examine interrelations between individuals in a dyadic relationship, more specifically, how the data from one member of the dyad predicts the other member’s data as is the focus in this study.
Results
Demographics
Youth (N = 50) and Adult (N = 46) Participant Characteristics.
Instrument Statistics for Key Variables.
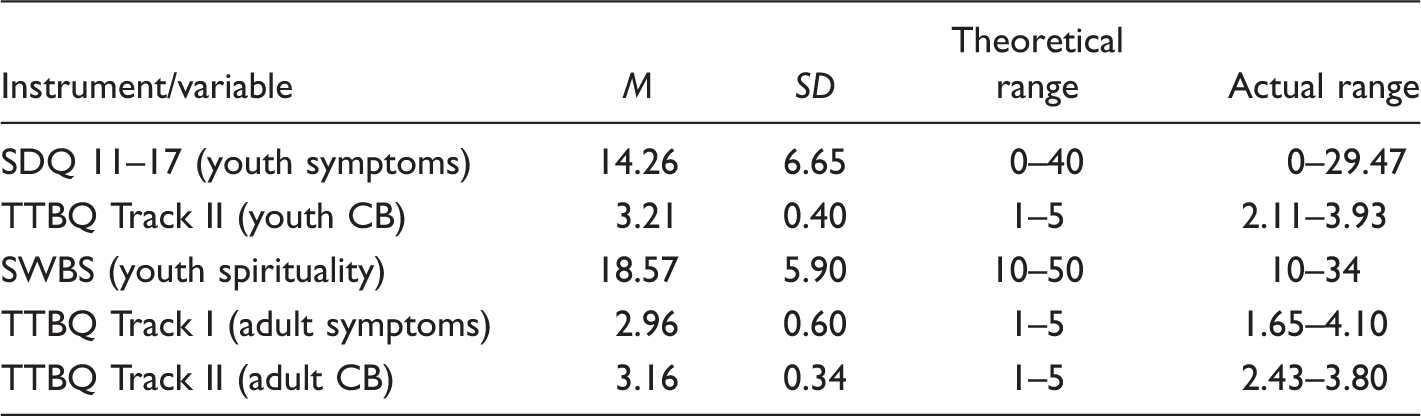
Note. SDQ
Correlations Among CB and Symptomatology
Predictor Variable Correlation With Youth CB and Regression Analysis.

Note. The variable “relation to deceased” was dichotomized for this analysis and coded as 1 = immediate family and 2 = extended family. SDQ
**p < .001. *p = .05.
To investigate and more accurately interpret the findings, a correlational analysis of youth symptomatology and the three distinct subscales of the TTBQ Track II were conducted. Findings revealed that youth symptomatology was positively associated with a close and positive relationship to the deceased (r = .48, p < .001) indicating that youth with stronger preloss and ongoing relationships to the deceased experienced higher grief-related symptoms following the death. In addition, youth symptomatology was positively associated with relational active grieving (r = .53, p < .001) indicating that while the SDQ is not a measure designed specifically for grief, it is correlated with a subscale intended to measure ongoing symptoms of relational grief in humans. However, youth symptomatology was not significantly associated with a conflictual relationship to the deceased (r = .24, p = .09). It is unclear whether this finding is precise because this particular subscale had low reliability (α = .47) among youth in this sample. Although not initially hypothesized, a bivariate analysis was also conducted to determine whether a positive association between caregiver CB and caregiver symptomatology existed in this sample as was revealed among youth CB and youth symptomatology. Findings indicated a similar correlation among caregivers (r = .51, p < .001).
To explore the dyadic relationship between youth and caregiver symptomatology and CB, an APM analysis was conducted, and findings were consistent with the bivariate correlations.
As shown in Figure 1, there are two actor pathways (Paths a and d) in this APM analysis that represent the extent to which an individual’s CB score (either the youth or the caregiver) is associated with their symptomatology score. In addition, the two cross-dyad, cross-variable pathways (Paths b and c) represent the effect of the caregiver’s CB score on their youth’s symptomatology as well as the influence of the youth’s CB on their caregiver’s symptomatology.
Youth caregiver model of continuing bonds and symptomatology. *p < .1.
Examination of the results of this analysis indicate that although youth CBs with the deceased were significantly and positively associated with their level of symptomatology (r = .60, p < .01), accounting for 35% of the variance in their symptomatology scores and that caregiver CBs were also significantly and positively associated with their level symptomatology (r = .51, p < .01) accounting for 26% of the variance in their level of symptomatology, neither caregivers’ nor youths’ CB scores were significantly associated with the symptomatology of the other person in the dyad (rcaregiver to youth = −.08, p = .58 or ryouth to caregiver = .17 p = .23). Furthermore, this analysis also revealed no significant relationships between the level of caregiver and youth CB with the deceased (r = .03, p = .84) or between the level of caregiver and youth symptomatology (r = .08, p = .56).
Predictors of Youth CB
A linear multiple regression analysis was conducted to identify the variables that were predictors of youth CB to the deceased. A total of three predictor variables were entered into the linear multiple regression model based on their significant bivariate correlations to youth CB (see Table 3). The predictor variable correlations to youth CB were as follows: youth symptomatology (r = .60, p < .001), youth spirituality (r = .30, p < .05), youth relationship to the deceased (dichotomous variable as “immediate family” and “extended family”; r = .29, p < .05).
The results, shown in Table 3, indicate that the predictor model was significant, R2 = .427, F(3, 46) = 11.45, p < . 001, and accounted for 39% of the variance in youth CB (adjusted R2 = .39). Examination of the standardized β coefficients indicated that youth symptomatology (β = .57, p < .001) and relationship to the deceased (β = −.24, p = .05) significantly contributed to the model with youth symptomatology being the strongest predictor of CB. Specifically, youth with higher levels of symptomatology were more likely to maintain a CB with the deceased as were youth who lost an immediate family member.
Given there was a lack of independence among several of the cases (i.e., four caregivers each had two participating children), a sensitivity analysis was conducted by rerunning the regression analysis without the four sibling cases. The results of this analysis did not alter the findings presented above that included all youth.
Discussion
Findings from this study supported the hypothesis that there was a relationship between youth symptomatology and youth CB. However, this study did not reveal an association between caregiver CB and youth CB. There was also no relationship evident between caregiver symptomatology and youth CB or any of the three subscales of the youth CB measure. Given the complexity of CBs and because this is one of the first studies to measure the construct in a quantitative manner among youth, this finding is very informative and warrants further discussion. Previous research demonstrated that caregiver support and positive parenting can have a positive impact on youth symptomatology (Haine, Sandler, Millsap, & Ayers, 2006), coping (Rask, Kaunonen, & Paunonen-Ilmonen, 2002; Silverman & Worden, 1992), and posttraumatic growth (Wolchick, Coxe, Tein, Sandler & Ayers, 2008). In addition, Silverman et al. (2003) reported the manner in which a surviving parent copes with a death and provides support impacts how well a child copes with a negative legacy CB. Further, Cerel et al. (2006) reported that caregiver symptomatology, specifically lower levels of caregiver depression, was associated with better postdeath outcomes among youth.
One possible explanation that caregiver symptomatology was not associated with youth CB could be that regardless of caregiver symptomatology, the manner in which caregivers are coping with the symptomatology and their ability to apply positive parenting strategies and affirm a healthy family environment may be more impactful on youth CBs than the symptomatology itself. It is likely that some caregivers have higher symptomatology but may be coping with the death more effectively than other caregivers reporting lower symptomatology. Coping behaviors and the accompanying ability to positively attend to the needs of youth under their care might have a significant impact on youth CBs. Further, youth whose caregivers are coping better may engage in more open conversations about their own CBs, thereby helping youth understand this aspect of grief.
Developmental considerations informed by the age of youth participants in this study may provide an alternative explanation. It is common for adolescents to have frequent conflicts with their adult caregivers and to seek emotional support from outside sources such as peer friendships (Walsh & McGoldrick, 2013). Therefore, an adolescent’s CB to the deceased may not be as intertwined with their primary caregiver’s CB as it might be for a younger child. It is also is possible that similarity of CB may differ as a function of kinship connection or relationship to the deceased, as it might be expected if a caregiver’s relationship to the decedent was that of parent, while the youth’s relationship to the decedent was that of nephew.
Another explanation could be because the grief process is a unique and individual one in which no two people experience exactly the same way. If CBs are a natural and expected human response to grief, then they might occur among youth regardless of adult caregiver symptomatology. Furthermore, if the bereavement experience for each individual consists of two continuums including both biopsychosocial functioning and the ongoing relationship with the deceased (Rubin, 1999), then it would seem more reasonable for youth symptomatology to be associated with youth CB and caregiver symptomatology to be associated with caregiver CB as was demonstrated in this study.
Although not previously examined among youth, results from the adult bereavement literature supporting this study’s findings are mixed. As an example, Field et al. (1999) revealed it may be the type of CB expressed by adults that depicts whether it is adaptive (e.g., finding comfort through memories of the deceased) or maladaptive (e.g., finding comfort through the use of deceased’s possessions). In contrast, Field et al. (2003) suggested that regardless of CB expression, at 5 years postdeath, CBs were strongly associated with increased grief symptomatology but had much lower associations with “general psychological symptoms” (p. 116). Reisman (2001) suggested that CBs for adults are adaptive when the bond is a “symbolic” one (e.g., memories, rituals on meaningful dates, linking objects) and maladaptive when it is a “concrete” one (e.g., keeping deceased’s possessions in exactly the same location as if they will return; p. 456). Due to the diversity of findings and the inability of studies to depict the time order of variables (Field et al., 2003), it has been difficult for researchers in the adult bereavement field to make any definitive suppositions about the adaptive or maladaptive nature of CBs.
Another explanation of the revealed association between CB and symptomatology among youth and adults could be that CBs are an adaptive part of the bereavement process and youth or caregivers with higher symptomatology more actively seek a CB with the deceased in an effort to assist in their coping and buffer their feelings of grief. In contrast, it could be explained that CBs are actually maladaptive and survivors with stronger CBs to the deceased experience more difficulty coping and more symptoms of grief as a result. Overall, it appears CBs are adaptive when they are used to assist the bereaved in coping with the transition from a relationship of physical presence to one of memory and “the relationship is reorganized in a way that the bereaved is no longer preoccupied with or severely distressed by thinking about the loved one’s physical absence” (Boerner & Heckhausen, 2003, p. 207). This is consistent with a recently published 10-year longitudinal study of CBs among 37 bereaved parents. Rubin and Shechory-Stahl (2013) reported all participants maintained a CB to the deceased, and general functioning/symptomatology was dependent upon the kind of CB maintained. Positive memories and emotions associated with the deceased were related to more positive outcomes, while negative recollections were associated with poorer long-term outcomes.
Of particular interest is the finding that youth symptomatology was associated with a close and positive relationship to the deceased. This could be because youth who experience a closer preloss relationship to the deceased may also have a stronger attachment bond to that person. Therefore, when a death occurs, their grief symptoms are likely to be more intense than someone with a moderate or mild attachment to the deceased. This is consistent with Servaty-Seib and Pistole (2006), in which emotional closeness to the deceased was indicated as a predictor of grief symptomatology among adolescents. In addition, a study of 91 bereaved adults revealed that participants who reported a closer attachment to the deceased experienced increased grief symptomatology (Wayment &Vierthaler, 2002).
Predictors of Youth CBs
This study also provided the first tentative predictors of CBs among youth. Results indicated that although spiritual well-being was associated with youth CB at the bivariate level, nature of the relationship to the deceased and youth symptomatology were two predictors of CBs among youth. Youth symptomatology was revealed as the strongest predictor of youth CB in this study. It is possible that youth with stronger symptomatology might actively seek and maintain CBs as a way of coping with their grief-related symptoms. In contrast, it could be argued that such bonds are maladaptive and further exacerbate symptoms of grief among youth. Although grief work theory suggests severing ties to the deceased is necessary (Attig, 1996; Noppe, 2000), attachment theorists would likely argue that grief symptoms and CBs are normal aspects of the bereavement process and both must be incorporated into bereavement assessment and intervention (Bonanno & Kaltman, 1999; Noppe, 2000). Similarly, the TTMoB, used to develop the TTBQ, suggests that practitioners should address both general functioning and ongoing relationship to the deceased when working with bereaved populations (Rubin, 1999). Findings from this study further contribute to these tenets of attachment theory and its role in grief and bereavement, specifically in the CBs humans maintain following a death. In addition, its findings support the importance of addressing both aspects of bereavement, overall symptomatology and the ongoing relationship to the deceased.
Most previous studies of youth, bereavement, and CBs have focused on a singular type of loss relationship (e.g., parent, sibling, and grandparent) leaving a large gap in the literature and no evidence in terms of the impact relationship plays in CBs among bereaved youth. Therefore, the finding that relationship to the deceased is a predictor of CBs among youth is of primary importance. A tentative explanation is that youth who experienced the death of an immediate family member may have a closer preloss relationship and attachment, thereby experiencing a stronger CB following the death. This predictor relationship is one that should be further explored through future research.
Although nonsignificant in the predictor model, spiritual well-being was correlated with youth CB. This finding is consistent with qualitative studies of CBs in which spirituality and a belief in the afterlife may play a significant role in developing and maintaining CBs (e.g., Richards, Acree, & Folkman, 1999; Silverman & Nickman, 1996; Steffen & Coyle, 2011).
Limitations
Despite the key findings, there were several limitations to this study that may have impacted results. Although the sample included children and adults in rural and urban communities, the selection was based on availability and included only those families already connected with one of the two children’s bereavement centers. The participating grief centers are free of charge and often receive referrals by school personnel and families when a youth is identified as having experienced a death, not necessarily due to having significant symptomatology. Therefore, it remains difficult to ascertain whether those in this study have abnormally high CBs or symptomatology compared to youth not receiving services. In addition, participants completed the instruments at different points along the service continuum. Some respondents participated in the study after receiving numerous individual counseling sessions, grief support group sessions, or other grief interventions (e.g., bereavement camp), whereas others completed instruments during their first visit prior to any intervention or only after attending a weekend community bereavement camp. Further, some adult caregivers may have received either support group sessions or individual counseling sessions that were unknown to the investigator. For this reason, the results of this study cannot be generalized to all bereaved clients (youth or adults) in the general population and not connected to services at a grief counseling center.
The sampling method also limited variability among some of the demographics under study such as race/ethnicity and relationship to the deceased in which peer deaths were excluded. Almost 85% of the adult participants in this study were female which could have impacted results. Finally, even though the TTBQ is an already established measure with strong validity and reliability, it was designed primarily for clinical use and Track II of the TTBQ was adapted and used with youth for the first time in this study. The long-term reliability and validity of the TTBQ Track II as a valid measure of CBs among bereaved youth is not yet known. Further, while the Track II subscale, conflictual relationship to the deceased, had an acceptable internal consistency (α = .67) in the pilot study sample, it had a lower reliability (α = .47) when administered to the full study sample. This could limit the validity and generalizability of the study results in regards to this subscale.
Despite these limitations, the findings from this study offer some unique insights regarding the predictors of CBs among bereaved children or adolescents, an area in which to date, few studies have been conducted. The study also provides foundational work in establishing a measure to assess CB in bereaved youth.
Implications for Practice and Research
This study’s findings suggest practitioners should assess the nature of the preloss relationship to the deceased. Because preloss closeness can be associated with increased symptoms of grief, it is essential for practitioners to evaluate both the relationship to the deceased and level of closeness and attachment in the relationship prior to the death. In addition, practitioners should assess both positive and negative aspects of the relationship to the deceased and develop interventions to resolve areas of conflict, which may be impeding the bereavement process. Furthermore, in accordance with the TTMoB (Rubin, 1999), this study’s findings reveal it is imperative for both aspects of the bereavement process (symptomatology and CBs) to be addressed in interventions for youth.
In this vein, it is essential for researchers to develop a reliable and valid instrument measuring childhood and adolescent bereavement. Ideally, one measure capable of assessing bereavement symptomatology in both youth and adults would ensure valid comparisons among family members. Because this study revealed relationship to the deceased is a predictor of CBs among youth, it is imperative this variable be included in future studies of childhood and adolescent bereavement, particularly those in which CB is being assessed. Comparing this study using a sample of younger children to determine whether similar CB/symptomatology relationships exist would also provide opportunity for the TTBQ to be adapted and piloted for use with another age-group. Since the majority of caregivers in this study were female, it would be beneficial to replicate this study with a more adequate representation of male caregivers. Further, research should also be conducted to determine whether the relationship between youth symptomatology and CBs exists within a larger sample. Given caregiver symptomatology was not associated with youth CB, additional investigation into the relationship between family dynamics such as conflict, caregiver coping, and postdeath parenting strategies and youth CBs would be informative. It would also be beneficial to determine whether symptomatology and CBs are related among siblings. In addition, researchers might study the ways in which expressions of CBs are shared within a family system. This is consistent with the suggestion of Walsh and McGoldrick (2013) to include family dynamics in the future study of bereavement. Finally, a longitudinal design investigating CBs among youth, specifically reviewing whether such bonds are adaptive or maladaptive over time and at certain points along the bereavement continuum, would greatly enhance the current knowledge base, especially among bereaved youth. Longitudinal research of this kind could also reveal whether youth modify the nature and type of CB expressions as they progress through different developmental stages.
Footnotes
Authors’ Note
The authors would like to thank Chapters Health System, the bereavement center staff and counselors, and the families who participated in this study. They would also like to thank Dr. Simon Shimshon Rubin for his contributions to the field of bereavement research and for granting permission to adapt the Two-Track Bereavement Questionnaire (TTBQ) for use with youth.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.