
Abstract
Completing an advance directive offers individuals the opportunity to make informed choices about end-of-life care. However, these decisions could be influenced in different ways depending on how the information is presented. We randomly presented 185 participants with four distinct types of advance directive: neutrally framed (as reference), negatively framed, religiously framed, and a combination. Participants were asked which interventions they would like to receive at the end of life. Between 60% and 70% of participants responded “accept the special interventions” on the reference form. However, the majority (70%–90%) chose “refuse the interventions” on the negative form. With respect to the religious form, 70% to 80% chose “not decided yet.” Participants who refused special life-sustaining treatments were older, female, and with better prior knowledge about advance directives. Our findings imply that the specific content of advance directives could affect decision-making with regard to various interventions for end-of-life care.
According to game theory, people make decisions based on the values and probabilities inherent in a situation. Thus, it is possible to predict what kind of action an individual will choose if every possible value and probability are known in a specific situation. Game theory was conceived as a normative model that postulated an idealized and rational agent as a decision maker. However, Tversky and Kahneman (1981) claimed that the behaviors of real people do not follow the assumptions of game theory. They demonstrated that the framing of alternatives can significantly affect decision-making. This means that the “framing effect,” that is, the way an object is presented or how information is worded and phrased, can prompt an irrational and emotional reaction that, in turn, influences a particular decision. Several psychologists also demonstrated that a person’s cognition could be affected by the content(s) of a situation or condition, which can determine the information processing that people use in making choices. For example, Rettinger and Hastie (2001) revealed that, despite using the same measures of the subjective values and probabilities of the options, casino gambling as a metaphor for game theory was associated with different behaviors than in the following content-domain scenarios: legal traffic tickets, financial stock investment, and academic course grades. Most participants preferred the safe option and adopted an avoid-the-risk strategy in the gambling scenario but chose the risky option and calculation strategy in the stock scenario. Their choice between risk-prone and risk-averse options was almost equal in academic and legal scenarios. A morality strategy was used more often in the legal scenario. Considering mental representations, more of the total propositions were recalled in the legal scenario. Number propositions were recalled more frequently in the legal and stock scenarios. The results demonstrated a fundamental role of content in the process of decision-making through affecting judgments, decision strategies, mental representations, and the ultimate choice (Rettinger & Hastie, 2001).
An advance directive is a legal document in which a competent person makes provision for medical and health-care decisions in the event she or he becomes mentally incompetent to make such decisions (Culver & Gert, 1990). Advance directives provide instructions to help a person make free and informed choices. However, according to the notion of framing effects, it is possible that medical decisions could be influenced in different ways depending on how the information in an advance directive is presented. This diversity of language could potentially affect an individual’s perception in regard to his or her end-of-life care at an unconscious level; this may nullify the original goal of advance directives, which implies the right to a dignified death by one’s own choice. Therefore, this study evaluated the influence of the specific content of advance directives on decisions related to end-of-life care options.
Methods
Study Participants
One hundred and eighty-five community-dwelling people participated in this study. Subjects were recruited from seven different community centers in Seoul, South Korea. With permission, we visited regular meetings at the centers and explained the aims of the study to attendants. Subjects who were willing to participate were included if they were more than 18 years old and competent to make a decision. We excluded subjects who were health-care professionals and those who lacked decisional capacity, including those with severe dementia. Of the 200 questionnaires distributed, 185 were returned and the valid response rate was 100%.
Study Design
Outline of Four Distinctive Forms of Advance Directive.
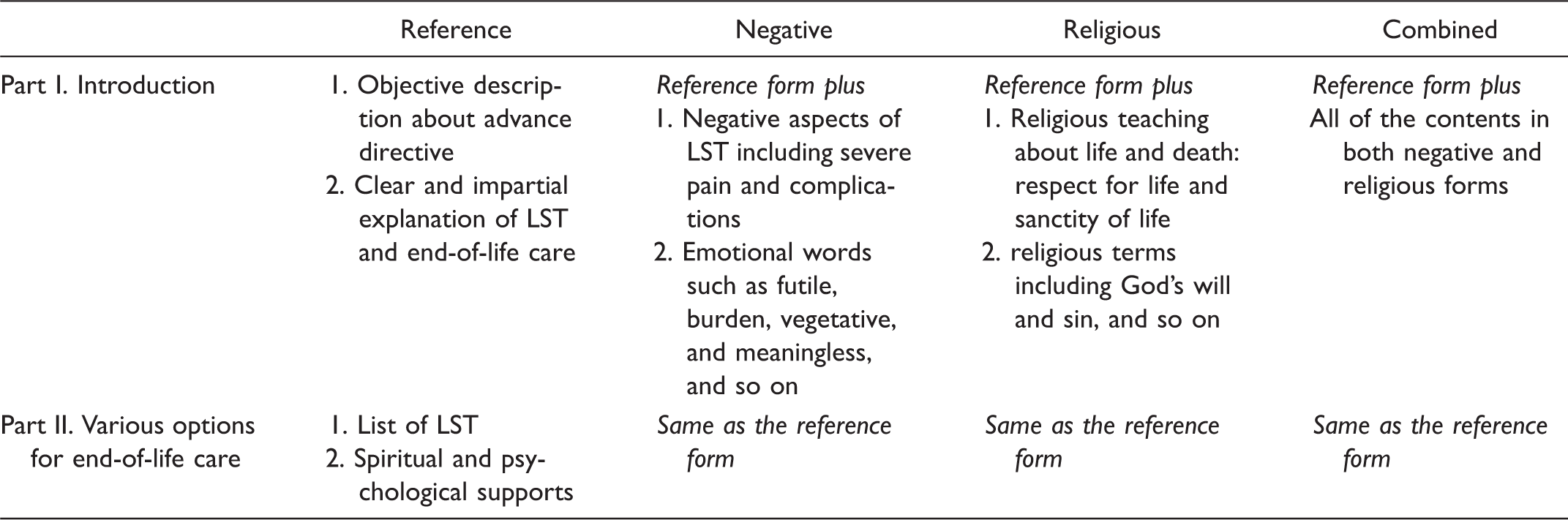
Note. LST = life-sustaining treatments.
Life-sustaining treatments were divided into special and general forms based on the necessity of specialized medical knowledge and specific medical devices, equipment, or facilities. General life-sustaining treatment consisted of providing nutrition and hydration, oxygen supply, maintaining temperature, helping with voiding and defecation, preventive measures for pressure ulcers, pain control, and so on. Special life-sustaining treatment included cardiopulmonary resuscitation (CPR), ventilator, dialysis, inotropics, and so on. This differentiation was established by the Guidelines Enactment Special Committee in Korea (Lim, Hong, & Lee, 2015). In addition, psychological and spiritual or religious counseling were added to the list as options that participants could choose for their end-of-life care.
We also collected demographic data including age, gender, religion, and political leanings and examined the degree of importance of participants’ religious and political viewpoints on decision-making, and whether participants were well-informed about end-of-life care. The degree of importance of religion and participants’ knowledge about advance directives as well as physician-assisted dying and euthanasia were each rated on a 5-point Likert-type scale (for the degree of importance, 1 = low importance and 5 = very important; for the degree of knowledge, 1 = not knowledgeable and 5 = very knowledgeable), while the degree of importance of political standing was measured using a 3-point scale (1 = weak and 3 = strong).
Participants chose one of the four distinct advance directives randomly: All four forms were placed in front of the participant without any information that each questionnaire was distinct and different from the others. Researchers tried to design the whole process so as not to influence each participant’s choice.
This study was approved by the institutional review board of Dongguk Institute, and all subjects gave informed consent to participate in the study.
Statistical Analysis
All statistical tests were interpreted as significant at the 5% level (two-sided for among group comparisons of study outcomes). All outputs were produced using SPSS, Version 20 (SPSS Inc., Chicago, IL). Continuous data were summarized by group and overall by number of observations, mean value, standard deviation, odds ratio, slope, and 95% confidence intervals for the mean. Categorical data were summarized by means of frequencies (counts and percentages) per group. One-way analyses of variance with post hoc tests (with Bonferroni correction) were used to test differences among groups. The data were analyzed by Student’s t test for two-group comparisons. All categorical data were analyzed using Pearson’s χ2 test and binomial test.
Results
Sample Characteristics
Demographic Characteristics (Total Participants, n = 185).
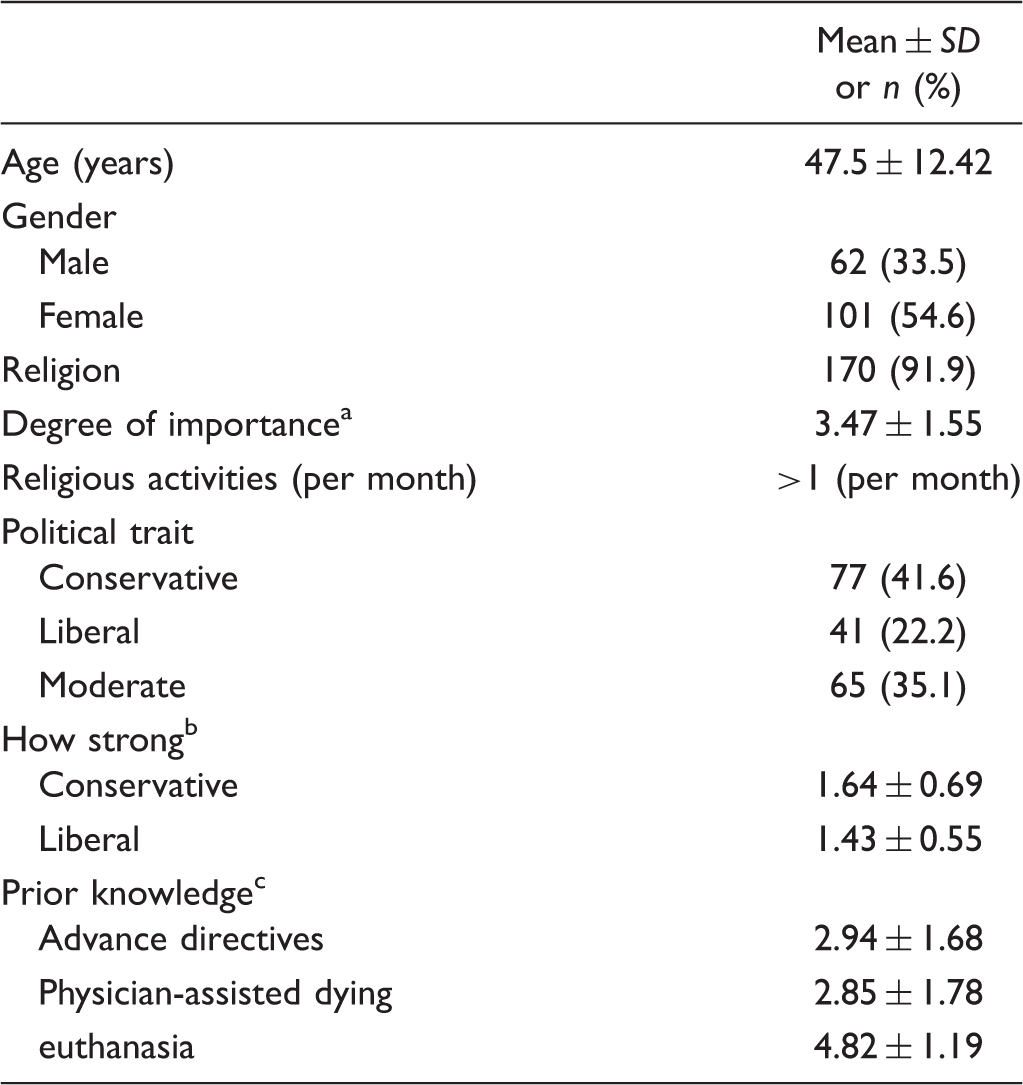
Note. SD = standard deviation.
aDegree of importance from 1 (low importance) to 5 (very important). bDegree of political convictions from 1 (weak) to 3 (strong). cDegree of prior knowledge from 1 (not knowledgeable) to 5 (very knowledgeable).
Responses to Life-Sustaining Treatments by Advance Directives
The Responses to Four Distinctive Forms of Advance Directive.

Note. Data are expressed as n (%). p values are derived from χ2 tests. AD = advance directive; CPR = cardiopulmonary resuscitation.
In terms of general life-sustaining treatments, most participants expressed a preference for all interventions across the forms. The forms containing negative or religious content affected decision-making similarly, but the effects were not marked.
Regarding preferences for psychological and spiritual or religious counseling, response trends were similar to those for general life-sustaining treatments. More than 70% of participants expressed a preference for counseling. Negative or religious content had much less influence on preferences for counseling compared to its effect on preferences for special life-sustaining treatments.
The Effect of Gender on Decision-Making Related to Life-Sustaining Treatments in Advance Directive.
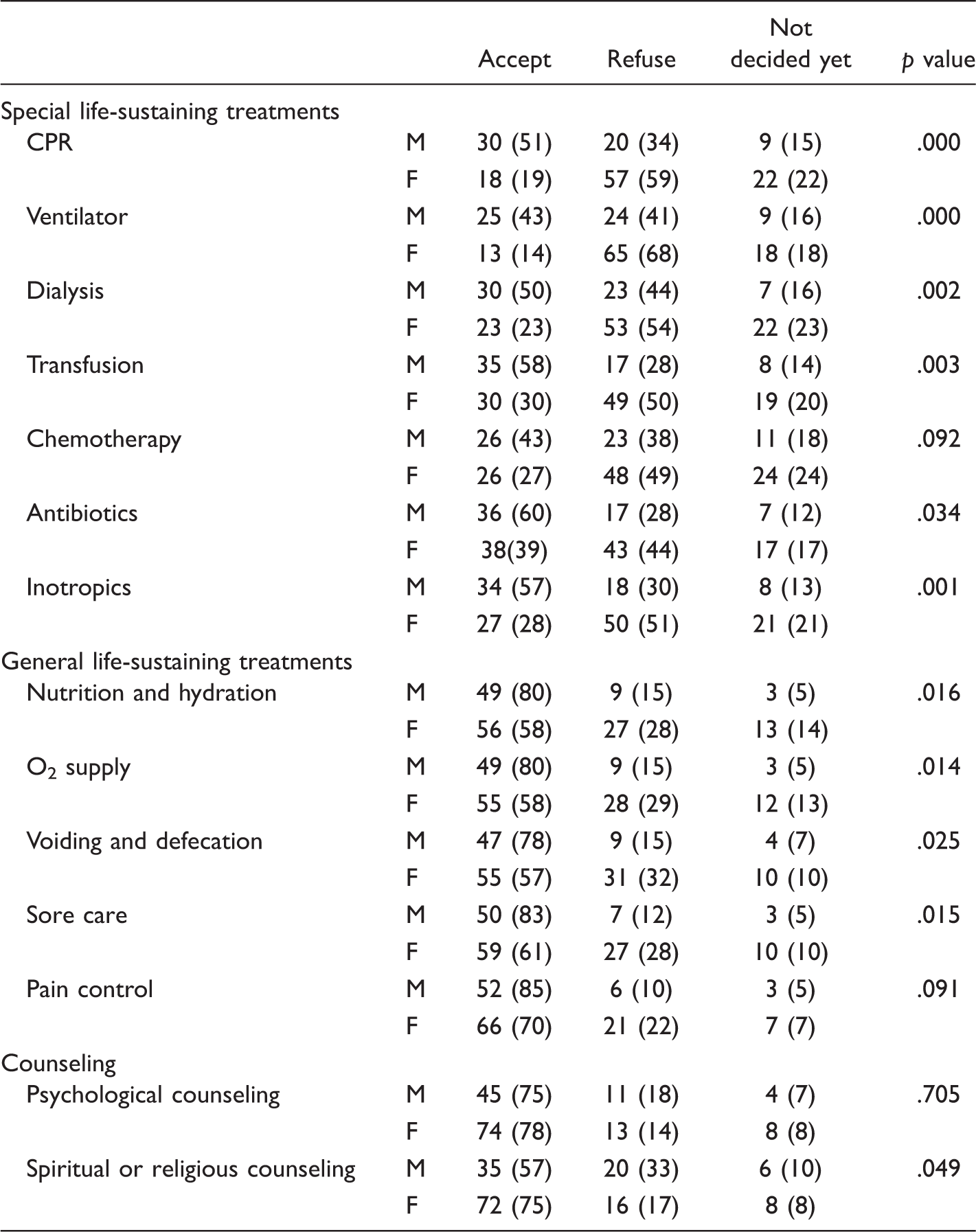
Note. Data are expressed as n (%). p values are derived from χ2 tests. CPR = cardiopulmonary resuscitation; M = male; F = female.
The Effect of Age on Decision-Making Related to life-Sustaining Treatments in Advance Directives.

Note. Data are expressed as mean ± standard deviation years old. p values are derived from one-way analysis of variances. CPR = cardiopulmonary resuscitation.
Discussion
Recently, the act on decisions on life-sustaining treatment for patients in hospice and palliative care or at the end of life, which addresses advance directives and advance care planning, was legislated in Korea and has taken effect since February 4th, 2018. This act is anticipated to provide a legal basis for various forms of end-of-life care and promote a patient’s autonomy and right to make decisions. However, the decision-making process is complex and easily influenced by intrinsic and extrinsic factors (Hash, Bodnar-Deren, Leventhal, & Leventhal, 2016). Moreover, a recent article showed that many patients misinterpret the goal of interventions. The framing effect is one of the most powerful factors affecting a patient’s decision-making (H. R. Lee, Lim, Yun, Kang, & Kim, 2018). Although the framing effect has been studied in various medical situations, the effect of the word(s) and content in advance directives on individual’s decision-making has not been thoroughly evaluated. Malloy, Wigton, Meeske, and Tape (1992) evaluated three separate hypothetical scenarios related to decisions about CPR, mechanical ventilation, and tube feeding in 201 community-dwelling elderly participants. One of the three case scenarios served as a reference and the remaining two were described in a positive or negative way. Participants chose the intervention 12% of the time in the negative scenario, 18% of the time in the reference scenario, and 30% of the time in the positive scenario. Seventy-seven percent of the participants changed their minds more than once when they encountered different scenarios with the same intervention. Our study showed similar results: Participants did not accept special life-sustaining treatments when they encountered the negative form of scenarios.
This study also evaluated religious content in advance directives, and our results demonstrated that participants were undecided with respect to special life-sustaining treatments, although less so when deciding on general interventions. It is likely that religious teachings make people more likely to defer their judgments of whether to accept or refuse a life-sustaining treatment. Religious concerns should be addressed more carefully in advance care planning because it is possible that religious practices limit the range and flexibility of options and choices by restricting the authority of an agent, which may lead to confusion and controversy (Grodin, 1993). Moreover, the interaction between negative content and religious teaching content is very complex; further study is needed to evaluate the exact role of advanced directives framed in religious terms in real clinical settings.
Prior knowledge regarding advance directives meaningfully influenced decision-making related to CPR and ventilator care. The more knowledgeable the participants were, the more likely they were to refuse interventions. However, no relationships were observed with respect to prior knowledge of physician-assisted suicide and euthanasia. Although there are several reports that political preferences can affect personal decisions and behavior (Haidt, Graham, & Joseph, 2009; Hannikainen, Miller, & Cushman, 2017), we did not find any significant effects of political traits on decision-making. It is also interesting that gender exerted a significant influence upon decision-making about life-sustaining treatments. Attitudes about advance care planning differed according to gender (Perkins, Cortez, & Hazuda, 2004); men considered only functional outcome regarding their end-of-life wishes and feared harm from the health system. Women felt empowered by the system and expressed various end-of-life wishes. More attention should be paid to avoid biased traditional gender roles and social prejudice for proper advance care planning. One of the important methods to overcome the effect of these factors would be continuous and extensive education about advance directives.
There are various ways in which content influences the final decision. One is that the content of advance directives could directly affect decision-making. Another is that there might be a mediator(s) that links content and final decision. For example, the wording of information can provoke tremendous emotional weight (Peppin, 1995), which can affect the individual’s ability to make sound and reasonable decisions. However, as Seo and Barrett (2007) demonstrated, individuals with superior decision-making performance are better able to identify and distinguish their current emotional state. Thus, the effect of emotion may depend upon how it is experienced, managed, and used in decision-making processes. According to dual-process theory, reasoning is involved in utilitarian moral judgments, but affective processes are important in deontological moral judgments (Horne & Powell, 2016). Despite controversy regarding the role of emotion in moral dilemmas, and the weak link between emotional responses and moral judgments, it is evident that emotions can be a source of bias (Gross & John, 2003) or a key player in decision-making (Slovic, Finucane, Peters, & MacGregor, 2007). Emotions can motivate morally relevant actions (Greene & Haidt, 2002; Preston & de Waal, 2002) and lead to moralization (Haidt, 2001). According to our results, it is possible that the specific content of each advance directive provoked different emotional responses from the participants. Further study will be needed to evaluate the role of emotion in decision-making related to advance directives.
There are several limitations to this study. First, the length and readability of the four distinct forms of advance directive were not comparable. Mazur and Hickam (1990) reported that even when framing influences are controlled, preferences can be affected by other attributes of summary data, namely, the amount of data presented. However, in this study, there were no significant differences with regard to accuracy, clarity, and completeness of the descriptions in the questionnaire. Second, racial and ethnic differences are well-documented in advance care planning (McAfee, Jordan, Sheu, Dake, & Kopp Miller, 2019; Nayfe, Marcoux & Jutai, 2019), even though there may be stark differences in marital, parental, educational, and socioeconomic status among members of a racial group. Carr (2012) reported that Asians are 58% less likely than Whites to have end-of-life discussions, but the former are 56% more likely to have living wills than the latter. Asians show tendencies to rely on formal documents and do not want to engage in discussions about dying (S. K. Lee, 2009). Further study would be needed to extrapolate the results to other ethnic groups and evaluate which ethnic groups are more likely to be affected by the content of advance directives. Third, as participants in our research were presented with hypothetical scenarios, it is plausible that their preferences could be different if they were confronted with real-life situations or if they faced terminal illness. Finally, the study showed that religiously framed advance directives influenced decision-making about end-of-life care. Individuals who consider themselves religious exhibit particular attitudes toward death (Lynn, Curtis, & Lagerwey, 2015). Most participants in this study were Buddhists. Therefore, it was difficult to determine whether responses to life-sustaining interventions and attitudes toward death varied according to individuals’ faith backgrounds.
It is important for free and informed consent to assess the content of advance directives and develop strategies to discourage the use of potentially persuasive language. First, advance directives should be written in a neutral manner, without using value-laden words such as pain, burden, and futile, because these words might evoke an emotional response or a negative assessment of quality of life. Second, as advance directives have psychosocial and legal implications in addition to medical implications, experts across disciplines, including health-care professionals, lawyers, social workers, and psychologists, should work together to create neutrally framed advance directives. Finally, as advance directives do not operate in isolation from care planning discussions, physicians or health-care personnel should discuss end-of-life care with patients in a manner that is neither biased nor prejudiced.
Conclusions
It is clear that the specific content of advance directives can affect decision-making with regard to various medical interventions related to end-of-life care. More attention should be paid to understand the effect of the content of advance directives and to facilitate the appropriate and autonomous decision-making related to end-of-life care.
Footnotes
Acknowledgments
The authors would like to express their sincerest thanks and appreciation to Matthew Bro for his valuable support and flawless grammatical editing of this article.
Declaration of Conflicting Interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Dongguk University, but it had no role in protocol design, collection or analysis of the data, or interpretation or writing of the results.