
Abstract
Traditional models of palliative care are largely inaccessible to homeless persons, and their preferences regarding end-of-life care are poorly understood. The purpose of the present scoping review is to summarize the burgeoning gray and academic literature on end-of-life care for homeless persons. Five medical databases, seven social science databases, and four gray literature databases were searched, resulting in 57 relevant titles. Six themes emerged: (a) Characteristics of homeless persons who require end-of-life care; (b) preferences and concerns of homeless persons approaching the end of life; (c) the role of spirituality for homeless persons at the end of life; (d) barriers to care at the patient, provider, and institutional or structural levels; (e) inclusive models of palliative care; and (f) implications for policy and practice. Practitioners and homeless persons must negotiate many obstacles in the provision and receipt of palliative care. However, there is tremendous potential and opportunity to improve the quality of life at the end of life for this vulnerable population.
Introduction
Homeless persons have higher rates of early mortality than the general population, often as a result of inconsistently managed or inadequately treated disease, comorbid medical conditions, or substance abuse (Fazel, Geddes, & Kushel, 2014). According to the 2016 Annual Homeless Assessment Report to Congress, in 2016, roughly 550,000 people were experiencing homelessness on a given night in the United States (M. Henry, Watt, Rosenthal, & Shivji, 2016). Homeless persons are less likely than the general population to have their needs met effectively by medical services (Podymow, Turnbull, & Coyle, 2006; Schanzer, Dominguez, Shrout, & Caton, 2007; Zur & Jones, 2014) and often die without having had access to consistent medical care or palliative care at the end of life (Baggett, Hwang, & Connell, 2013; Hibbs et al., 1994; Page, Thurston, & Mahoney, 2012; Schanzer et al., 2007) .
Palliative care is a holistic patient-centered philosophy of care that aims to optimize the quality of life for terminally ill patients and their families through symptom relief and pain management (Rome, Luminais, Bourgeois, & Blais, 2011). The palliative care approach also emphasizes psychosocial and spiritual well-being in the context of terminal illness (National Hospice and Palliative Care Organization, 2017; World Health Organization, 2018). Palliative care is typically delivered by an interdisciplinary team in diverse settings, including in-hospital and long-term care facilities, at home, and in residential hospices (Canadian Hospice Palliative Care Association, 2018).
Some studies have shown a significant reduction in pain at the end of life for patients receiving palliative care (Higginson & Hearn, 1997; Miller, Mor, Wu, Gozalo, & Lapane, 2002). Other research has shown improved family-centered outcomes, such as emotional and spiritual well-being, self-efficacy (Gelfman, Meier, & Morrison, 2008), and greater patient and family satisfaction with end-of-life palliative care compared with conventional care (Brumley, Enguidanos, & Cherin, 2003; Casarett et al., 2008; Ringdal, Jordhøy, & Kaasa, 2002).
Accessing palliative care may be challenging for homeless persons because they often do not live in environments that are conducive to traditional end-of-life care provision (Page et al., 2012). Moreover, palliative care facilities may be reluctant to admit homeless persons due to concerns regarding behavior and lifestyle (e.g., drug and alcohol abuse), which has led to many homeless persons dying in public spaces or in emergency departments (Page et al., 2012).
There is some evidence that implementing hospice palliative care for terminally ill homeless persons may result in significant cost savings (Podymow et al., 2006). This is consistent with previous research showing that palliative care in all settings reduces health-care expenditures in the general population (Smith, Brick, Hara, & Normand, 2014).
Increasingly, there have been calls for further research on how best to provide adequate care to this underserved population (Ahmed et al., 2004; MacWilliams, Bramwell, Brown, & O’Connor, 2014). The purpose of this scoping review is to examine the literature on the needs and preferences of homeless persons regarding end-of-life care, the deployment of hospice palliative services for homeless individuals, including identifying models of end-of-life care for homeless persons, and the barriers to accessing such care. This search builds on the seminal work of Hudson, Flemming, Shulman, and Candy (2016), who conducted a systematic review of qualitative research on the challenges to access and provision of palliative care for homeless persons, and Sumalinog, Harrington, Dosani and Hwang (2017), who systematically reviewed end-of-life care interventions for homeless persons. We identified the need for an updated review due to the fact that this literature is burgeoning, with six relevant articles published in 2017 and early-2018 alone. Furthermore, we were aware of a broader literature than Hudson et al. (2016) and Sumalinog et al. (2017) were able to access because of their exclusion of nonintervention quantitative studies and gray literature and omission of some pertinent databases. This additional literature provides added nuance and understanding of this important topic. We also wish to expand the discussion regarding client needs and preferences, a gap that has previously been identified by a number of researchers. As will be summarized later, we located an additional 40 relevant articles to further the valuable work accomplished in previous studies.
Methods
A computerized search of the literature was conducted in March 2018. A total of 16 databases, including 5 medical databases, 7 social science databases, and 4 gray literature databases were searched: Medline (1966–), PsycINFO (1967–), Social Work Abstracts (1968 to March 2018), Embase (1980–), HealthSTAR (1975–), Age Line, CINAHL (1982–), Social Sciences Abstracts (H.W. Wilson), ASSIA (1987–current), Social Services Abstracts (1979–), Sociological Abstracts (1952–), Cochrane, Health Canada, OAIster, Opengrey, and New York Academy. A manual search through reference lists in selected literature was also conducted.
The following keywords were used: (homeless* OR “under housed” OR “marginally housed”) AND (palliat* OR hospice* OR “end of life care” OR “home care” OR homecare OR “care at home” OR “domestic health care” OR “home health care” OR “shelter based care”) AND (terminal* ill* OR “terminal diagnosis” OR “terminal disease” OR dying)
These search terms were approved by both a social science librarian and a medical research librarian at the University of Toronto.
Inclusion and Exclusion Criteria
Peer-reviewed and gray literature was considered appropriate for review if the primary focus was end-of-life care for homeless or underhoused persons or if significant sections of the material focused on end-of-life care for this population. Promotional material and articles written in a language other than English were excluded. No date parameters were specified in order to ensure a robust search.
Data Extraction
As presented in Figure 1, the database searches described earlier resulted in 68 unique titles. Titles and abstracts were then reviewed independently by two researchers. From these, 26 articles were identified for full-text review. An additional 34 articles were identified in manual searches of reference lists. Of these, seven were excluded on the basis of language or being unavailable for full-text review. The full texts of the remaining articles were reviewed by two independent researchers. Articles were excluded for violating the inclusion or exclusion criteria outlined earlier, including being not homeless-specific or an inappropriate source (e.g., promotional material). In the case of a discrepancy between evaluators, agreement was obtained through discussion. In addition, four articles were identified from other sources (e.g., Internet searches).

Identification of studies, inclusion, and exclusion assessment. *Primary reason for exclusion: not focused on homelessness or end-of-life care. **Primary reasons for exclusion: article not readily available; not published in English.
Results
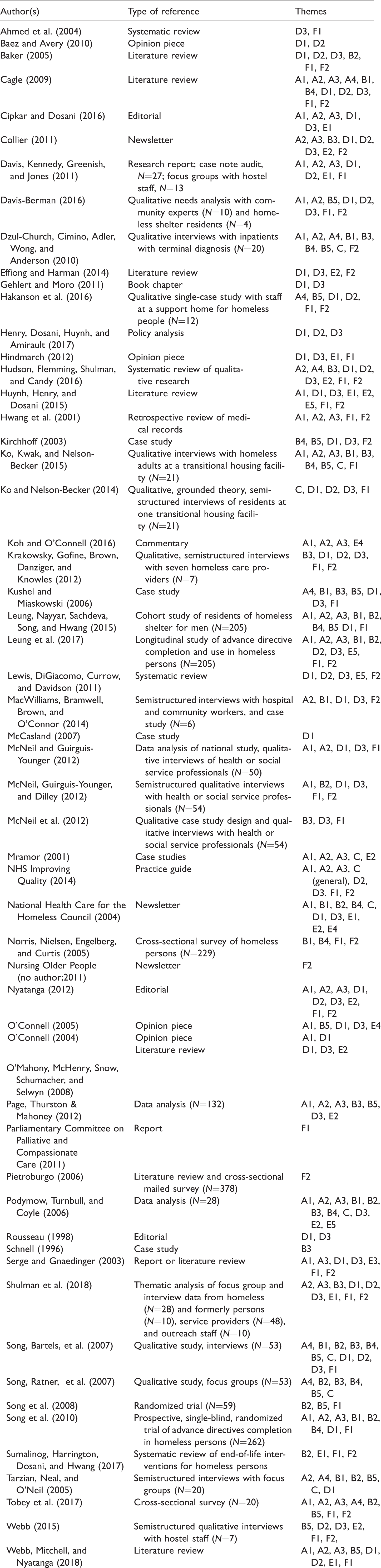
A total of 57 academic and gray literature articles were identified for review (see Table 1). Six main themes were identified:
Data From Articles Included in the Review (N = 57).
Characteristics of homeless persons who require end-of-life care;
Preferences and concerns of homeless individuals approaching the end of life;
The role of spirituality for homeless persons at the end of life;
Barriers to care at the patient, provider, and institutional or structural levels;
Models of palliative care that are inclusive of homeless persons; and
Implications for policy and practice for homeless persons at the end of life.
Included articles are mapped to themes and subthemes in Table 1. The coding legend is given in Table 2.
Coding Legend of Main Themes and Subthemes Identified in the Review.

Client Characteristics
The literature identified a high prevalence of chronic health problems, substance abuse and mental health challenges, and past exposure to death and loss as common among homeless persons.
Physical health
Homeless individuals disproportionately die prematurely with estimates of the average age of death ranging from 46 to 49 years (Page et al., 2012; Podymow et al., 2006). The homeless population have a high incidence of HIV or AIDS (Dzul-Church et al., 2010; McNeil & Guirguis-Younger, 2012; McNeil, Guirguis-Younger, & Dilley, 2012; O’Connell, 2004, 2005; Podymow et al., 2006; Serge & Gnaedinger, 2003) and chronic conditions such as diabetes (Huynh, Henry, & Dosani, 2015; Hwang et al., 2001; Koh & O’Connell, 2016; McNeil, Guirguis-Younger, & Dilley, 2012; NHS Improving Quality, 2014; O’Connell, 2004; Serge & Gnaedinger, 2003) and cancer (Dzul-Church et al., 2010; Podymow et al., 2006). Homeless persons are more likely to die from preventable causes (Davis, Kennedy, Greenish, & Jones, 2011; National Health Care for the Homeless Council, 2004; O’Connell, 2004; Serge & Gnaedinger, 2003).
Substance abuse
Substance abuse among homeless individuals is frequently reported in the literature (Dzul-Church et al., 2010; NHS Improving Quality, 2014; Page et al., 2012; Podymow et al., 2006; Tarzian, Neal, & Neil, 2005). Substance abuse is associated with serious health conditions such as HIV or AIDS and alcohol cirrhosis, hepatic disease, malnutrition, dementia, traumatic brain injury, and risk of overdose (Davis et al., 2011; McNeil & Guirguis-Younger, 2012; Podymow et al., 2006) and may complicate palliative care provision.
Mental health
The high prevalence of serious mental illness and complex trauma among homeless persons can make the provision of palliative care more challenging (Cagle, 2009; Collier, 2011; Davis et al., 2011; Hwang et al., 2001; Koh & O’Connell, 2016; Podymow et al., 2006; Shulman et al., 2018; Tobey et al., 2017; Webb, Mitchell, Nyatanga, & Snelling, 2018). In a qualitative study of hostel and health-care providers, Davis et al. (2011) found that low mood, panic, and anxiety were prevalent in the weeks and months prior to death among hostel residents. Depression is also common among the dying homeless (Davis et al., 2011; Tobey et al., 2017; Webb et al., 2018).
Exposure to death
Many papers reviewed noted that the experience of homelessness is underscored by frequent experiences with death and loss which profoundly shape homeless persons’ understanding of their own terminal illnesses and perceptions of end-of-life care (Cagle, 2009; Dzul-Church et al., 2010; Hakanson et al., 2016; Song, Bartels, et al., 2007; Song, Ratner, et al., 2007; Tarzian et al., 2005; Tobey et al., 2017). Past experiences with the health-care system were often poor and led homeless persons to expect inadequate or unsatisfactory care (Kushel & Miaskowski, 2006; Song, Ratner, et al., 2007).
Preferences and Concerns
Thirty-one papers discussed homeless persons’ preferences regarding palliative care, including those around medical care and advance care directives, dying in place, contact with family, and fears and concerns related to death and dying.
Medical care
A commonly reported concern among homeless palliative patients was whether they would receive adequate pain management (Dzul-Church et al., 2010; Song, Bartels, et al., 2007). Patient substance abuse was seen as a complicating factor in delivering appropriate pain management due to concerns about drug-seeking behavior and nonadherence to treatment regimens (Kushel & Miaskowski, 2006; MacWilliams et al., 2014).
There was considerable diversity regarding the desirability of life-prolonging interventions (Ko, Kwak, & Nelson-Becker, 2015; National Health Care for the Homeless Council, 2004; Norris, Nielsen, Engelberg, & Curtis, 2005; Song, Bartels, et al., 2007; Song et al., 2010; Tarzian et al., 2005). In a study of underhoused inpatients with terminal illnesses, Dzul-Church et al. (2010) noted that participants perceived that prolongation of life was associated with pain and was thus feared by most of the participants. Ko et al. (2015) reported similar findings, indicating that artificial life-prolonging interventions were perceived by some participants in their study as painful and interfering with the peaceful death they desired. Contrary to these findings, Cagle (2009) and Leung, Nayyar, Sachdeva, Song, and Hwang (2015) found that homeless individuals facing a terminal illness were highly likely to desire resuscitation. Similarly, Norris et al. (2005) found that homeless persons were more likely to choose resuscitative measures than physicians, suggesting that homeless individuals may receive less aggressive treatment than they would choose for themselves if physicians acted as surrogate decision makers or if their preferences were not well documented.
Advance care directives
Thirteen papers discussed the receptiveness of homeless individuals to formulate advance care directives (Baker, 2005; Leung et al., 2015, 2017; McNeil, Guirguis-Younger, & Dilley, 2012; National Health Care for the Homeless Council, 2004; Podymow et al., 2006; Song, Bartels, et al., 2007; Song, Ratner, et al., 2007; Song et al., 2008, 2010; Sumalinog et al., 2017; Tarzian et al., 2005; Tobey et al., 2017). Song et al. (2010) found that rates of advance directive completion among a sample of homeless individuals were comparable to those of the general population.
Some research concluded that advance care directives were effective in empowering a client in asserting some control over his or her care (Baker, 2005; Podymow et al., 2006; Song, Bartels, et al., 2007; Song, Ratner, et al., 2007; Song et al., 2008). In a randomized trial of advance directive completion among homeless persons, Song et al. (2008) reported that among participants who completed advance directives, the prevalence of worry about end-of-life care and dying decreased from 50% to 12.5%. Recent research by Leung et al. (2015) has provided convergent evidence that advance directive completion tends to reduce worry about end-of-life care among homeless persons.
However, several barriers to creating advance care directives have also been identified in the literature, including a fear of loss of autonomy, a perception of advance directives as paternalistic and controlling (Song, Bartels, et al., 2007; Song, Ratner, et al., 2007), distrust of health-care professionals (Ko & Nelson-Becker, 2014; Tobey et al., 2017), and feeling misunderstood by family (Tobey et al., 2017). One qualitative study found that discomfort with the topic of end-of-life care was a deterrent to engaging in advance care planning (Ko & Nelson-Becker, 2014). Tarzian et al. (2005) reported that homeless participants preferred meeting outside of formal health-care settings to discuss advance care planning, suggesting, perhaps, a role for social service workers, who may have more frequent contact with homeless persons than health providers in initiating these conversations.
Dying in place
A number of papers mentioned the preference held by the majority of dying homeless individuals to die in shelters as opposed to hospitals (Collier, 2011; Dzul-Church et al., 2010; McNeil, Guirguis-Younger, Dilley, Aubry, et al., 2012; Page et al., 2012; Podymow et al., 2006; Schnell, 1996; Shulman et al., 2018) . The preference to die in shelters was due in part to the relationships established with staff (Dzul-Church et al., 2010; McNeil, Guirguis-Younger, Dilley, Aubry, et al., 2012; Podymow et al., 2006). In addition, several authors commented that it is common for homeless persons to have had past negative experiences that resulted in a general distrust or fear of hospitals or health-care professionals (Dzul-Church et al., 2010; Huynh et al., 2015; Ko & Nelson-Becker, 2014; Krakowsky, Gofine, Brown, Danziger, & Knowles, 2012; Kushel & Miaskowski, 2006; Song, Bartels, et al., 2007; Song, Ratner, et al., 2007).
However, a minority of homeless persons preferred to remain in hospital for a number of reasons, including being less of a burden on family (Dzul-Church et al., 2010), 24-hour care and direct access to physicians (Krakowsky et al., 2012), and better treatment success rates in hospital for potentially reversible conditions (Podymow et al., 2006). Many health-care professionals argue that the best quality care is received in hospital; however, Krakowsky et al. (2012) noted that it is important to consider the many dimensions of quality care and “to appreciate the desire of an individual to die in a familiar, comfortable environment” (p. 269).
Contact with family
There was considerable variation in the reported preferences of homeless persons regarding contact with family before death (Cagle, 2009; Dzul-Church et al., 2010; Kirchhoff, 2003; Ko et al., 2015; Leung et al., 2015; National Health Care for the Homeless Council, 2004; Norris et al., 2005; Podymow et al., 2006; Song, Bartels, et al., 2007; Song, Ratner, et al., 2007; Song et al., 2010). Some papers noted that the majority of homeless palliative care patients preferred to reunite or repair relationships with estranged families at the end of life (Kirchhoff, 2003; Ko et al., 2015; Podymow et al., 2006). In contrast, Song et al. (2007) found that the majority of their sample preferred not to contact family. The latter was attributed in part to previous abandonment by family and to meaningful relationships formed with staff and friends on the street. Interestingly, the majority of participants in two studies on the completion of advance directives among homeless persons (Leung et al., 2015; Song et al., 2010) identified a family member as a surrogate decision maker. This is consonant with Norris et al.’s (2005) finding that the majority of homeless study participants preferred that a family member make medical decisions for them if they were incapacitated. For those without family and those not wanting family involvement, most preferred that a physician make medical decisions for them if they were unable.
Fears
Based on the literature, homeless persons seem to share some fears and concerns about death and dying that are not common in the general population. Many authors cited fears of dying alone and anonymously (Dzul-Church et al., 2010; Hakanson et al., 2016; Kirchhoff, 2003; Ko et al., 2015; O’Connell, 2005; Song, Bartels, et al., 2007; Tobey et al., 2017; Webb et al., 2018) and fear of disrespect of their body or having their body disposed of in ways that are culturally inappropriate or not congruent with their personal wishes (Song, Bartels, et al., 2007; Tarzian et al., 2005). In addition, many papers indicated that lack of respect for an individual’s wishes was a common fear, likely due to past negative interactions with systems and service providers (Dzul-Church et al., 2010; Page et al., 2012; Song, Bartels, et al., 2007; Song, Ratner, et al., 2007; Tarzian et al., 2005). In some studies, homeless participants feared a loss of autonomy that could result from accepting medical care (Dzul-Church et al., 2010; Kirchhoff, 2003; Ko et al., 2015; O’Connell, 2005; Song, Bartels, et al., 2007; Webb et al., 2018). A further testament to the negative interactions with the health-care system was the fear, cited by Kushel and Miaskowski (2006), that care would be withheld at the end of life due to previous experiences of being denied health care. Participants in a qualitative study exploring homeless persons’ perspectives of a good or bad death expressed fears of suffering irremediable physical pain as a result of an accident, drug overdose, violence, or disease (Ko et al., 2015). Some studies reported that some homeless individuals avoided medical investigation and advance care planning altogether due to fears of death and dying, generally (Shulman et al., 2018; Webb, 2015).
Spirituality
Ten papers addressed spirituality among homeless persons in palliative care (Dzul-Church et al., 2010; Ko et al., 2015; Ko & Nelson-Becker, 2014; Mramor, 2001; NHS Improving Quality, 2014; National Health Care for the Homeless Council, 2004; Podymow et al., 2006; Song, Bartels, et al., 2007; Song, Ratner, et al., 2007; Tarzian et al., 2005). Spirituality or religion was variously understood as a coping strategy, a source of strength, and a critical component of a good death (Ko et al., 2015; Ko & Nelson-Becker, 2014; National Health Care for the Homeless Council, 2004; Song, Bartels, et al., 2007). Particularly, faith in a higher being was related to a sense of fatalism about life (Ko & Nelson-Becker, 2014; Tarzian et al., 2005) and that one was not alone in dying (Song, Bartels, et al., 2007). Two articles found a tension between this fatalistic understanding of life and the completion of advance care directives, as planning for the future was considered unnecessary if one placed trust in a higher being to take care of them (Ko & Nelson-Becker, 2014; Tarzian et al., 2005). Tarzian et al. (2005) reported some homeless palliative patients felt that relying on life-sustaining interventions compromised their faith in God and was therefore not preferred, while others felt morally compelled to use life-sustaining interventions, as they were given through God.
Barriers
Our review identified 43 papers that addressed barriers for homeless persons in accessing palliative care. Of these, 36 reported on barriers at the patient level, 19 at the provider level, and 34 on broader institutional or structural barriers.
Patient-level barriers
Patient-level barriers were further grouped into four domains: (a) beliefs or expectations, (b) behaviors, (c) logistical or environmental, and (d) social support.
Beliefs or expectations
Several papers discussed homeless persons’ lack of trust in health providers (Cagle, 2009; Collier, 2011; Davis et al., 2011; Hakanson et al., 2016; B. Henry, Dosani, Huynh, & Amirault, 2017; Ko & Nelson-Becker, 2014; Krakowsky et al., 2012; Lewis, DiGiacomo, Currow, & Davidson, 2011; McNeil & Guirguis-Younger, 2012; Shulman et al., 2018; Song, Bartels, et al., 2007; Tarzian et al., 2005; Webb et al., 2018) primarily as a result of past experiences with, or internalized, stigma and discrimination. Some papers also cited lack of awareness of or misconceptions about hospice (Hindmarch, 2012; Lewis et al., 2011) as possible barriers to accessing appropriate end-of-life care.
Behaviors
Noncompliance in recommended care (Gehlert & Moro, 2011; Kushel & Miaskowski, 2006; MacWilliams et al., 2014) and the deprioritization of health needs by homeless persons in order to meet more immediate needs (e.g., food and shelter, substance use, caring for a pet; Kirchhoff, 2003; Ko & Nelson-Becker, 2014; Kushel & Miaskowski, 2006; NHS Improving Quality, 2014) were among the reported behavioral barriers to accessing palliative care.
Barriers for homeless persons with serious and persistent mental illness and substance use issues in accessing palliative care were addressed in several papers. Persons with mental illness and substance use issues may avoid medical care (Baez & Avery, 2010; Davis et al., 2011; NHS Improving Quality, 2014; Shulman et al., 2018), lack skills and knowledge to navigate the health system (Baker, 2005), lack insight into their condition (Davis et al., 2011), have difficulty communicating their needs (Collier, 2011; Hakanson et al., 2016), or have wandering tendencies (McCasland, 2007) that present challenges for residential or inpatient hospice. In one qualitative study of health and social services professionals involved in health services provision to homeless persons (N = 50; McNeil & Guirguis-Younger, 2012), participants indicated that homeless persons who use illicit drugs may not prioritize their health needs and minimize contact with health-care providers. Patients’ reluctance to use prescription narcotics due to fears and misconceptions about addiction or relapse (Cagle, 2009; National Health Care for the Homeless Council, 2004) was also cited as a barrier to adequate palliative care.
Logistical or environmental
Several papers cited the lack of a stable environment—including, power sources for medical equipment, refrigeration for medication, and telephone service—as impediments to palliative assessment, intervention, and longitudinal continuity of care (Baker, 2005; Cagle, 2009; Gehlert & Moro, 2011; Kushel & Miaskowski, 2006; National Health Care for the Homeless Council, 2004; O’Connell, 2004, 2005; Serge & Gnaedinger, 2003; Webb et al., 2018). Lack of transportation (Gehlert & Moro, 2011; Kushel & Miaskowski, 2006; Lewis et al., 2011) and loss or theft of belongings (Kushel & Miaskowski, 2006; Webb et al., 2018) were also identified as barriers to adequate end-of-life care. Finally, because many homeless persons are transient and have tenuous connections with health and community services, they may not have an established source of preventative or primary care to diagnose chronic and terminal conditions or refer to specialist palliative care (Cipkar & Dosani, 2016; National Health Care for the Homeless Council, 2004; O’Mahony et al., 2008; Rousseau, 1998; Serge & Gnaedinger, 2003; Webb et al., 2018).
Social support
The absence of a primary caregiver was reported in a number of papers as a significant barrier to accessing hospice services for homeless persons who are often estranged from their families of origin (Baker, 2005; Cagle, 2009; Effiong & Harman, 2014; Gehlert & Moro, 2011; Hakanson et al., 2016; Kirchhoff, 2003; Kushel & Miaskowski, 2006; Lewis et al., 2011; McNeil, Guirguis-Younger, Dilley, Aubry, et al., 2012; National Health Care for the Homeless Council, 2004). Although a number of different palliative care delivery models exist, the majority of care is home-based and relies to a large extent on the availability of an informal caregiver (Cagle, 2009; Lewis et al., 2011). The absence of advocates to help homeless persons navigate the health-care system, and surrogate decision makers (i.e., health-care proxies) to make decisions on behalf of those who lack capacity, were also identified as important barriers to care (Gehlert & Moro, 2011; Ko & Nelson-Becker, 2014; Kushel & Miaskowski, 2006; Serge & Gnaedinger, 2003).
Provider-level barriers
Provider-level barriers can be subcategorized as (a) attitudes and beliefs about homeless persons, (b) knowledge gaps, and (c) diagnostic and prognostic challenges.
Attitudes and beliefs
Barriers related to negative attitudes and behaviors of health providers toward homeless persons were reported in several papers (Davis et al., 2011; Davis-Berman, 2016; B. Henry et al., 2017; Ko & Nelson-Becker, 2014; Lewis et al., 2011; NHS Improving Quality, 2014; Nyatanga, 2012; Song, Bartels, et al., 2007; Webb, 2015; Webb et al., 2018). According to Cagle (2009), health professionals may hold tacit stigmatizing beliefs about homeless persons that may impede access to appropriate end-of-life care. Other papers cited mainstream providers’ attitudes toward, and lack of understanding or experience with, mental illness and challenging behaviors as potential barriers (Baker, 2005; Cagle, 2009; Shulman et al., 2018). Baez and Avery (2010) noted that terminally ill patients with schizophrenia are often not offered hospice services. In addition, providers may be reluctant to provide analgesic intervention due to fears of substance abuse in the homeless population and perceptions of or misconceptions about homeless persons’ “drug seeking” behavior (Cagle, 2009; Davis-Berman, 2016; Song, Bartels, et al., 2007; Webb et al., 2018).
Knowledge gaps
Collier (2011) reported that many providers do not receive sufficient training to work effectively with marginalized populations. Similarly, some authors cited providers’ lack of knowledge about the unique issues affecting homeless persons, and discomfort in discussing issues of death and dying and homelessness, as barriers to appropriate palliative care for this population (Davis-Berman, 2016; Krakowsky et al., 2012; Shulman et al., 2018). Alternatively, palliative treatment provision in the context of ongoing illicit substance use may be particularly challenging (Hakanson et al., 2016). Finally, previous research suggests that providers have variable understanding of palliative care (Webb, 2015).
Diagnostic and prognostic challenges
Five papers noted the particular challenge for providers in making diagnoses and estimating prognoses for homeless persons with comorbid physical and mental health issues, and for those with inconsistent engagement in the health-care system (Davis et al., 2011; Hakanson et al., 2016; NHS Improving Quality, 2014; Shulman et al., 2018; Webb et al., 2018). Because disease trajectories are difficult to predict, opportunities to discuss preferences for end-of-life care, engage in advance care planning, and refer to appropriate services are often missed (Davis et al., 2011; Shulman et al., 2018; Webb et al., 2018). Incomplete or inadequate medical information represents a particular challenge to staff supporting homeless individuals at end-of-life (NHS Improving Quality, 2014; Webb, 2015).
Institutional or structural barriers
Among the most prevalent barriers at the institutional or structural level are (a) the incongruity of existing models of care with homelessness, (b) systemic financial barriers, (c) ethical and jurisdictional challenges, and (d) multiple oppression.
Incongruity of systems of care
Several papers address the incongruity of existing models of palliative care with the realities of homelessness (Cagle, 2009; Cipkar & Dosani, 2016; Collier, 2011; Hindmarch, 2012; Kirchhoff, 2003; Krakowsky et al., 2012; O’Connell, 2005; Shulman et al., 2018). The current end-of-life care system is premised on assumptions that patients will have an informal support network and a stable residence (McNeil, Guirguis-Younger, & Dilley, 2012; Song, Bartels, et al., 2007). Most hospices are not equipped to care for patients who do not have permanent residences (O’Mahony et al., 2008), and many programs are reluctant to enroll patients who do not have informal caregivers (Rousseau, 1998), as providing care to persons without capacity and without a surrogate decision maker is often very resource-intensive (Effiong & Harman, 2014; MacWilliams et al., 2014).
Likewise, shelters and other residential facilities for homeless persons may not be resourced to care for terminally ill people (Cagle, 2009; Davis-Berman, 2016; Page et al., 2012; Serge & Gnaedinger, 2003) and may have operating policies that are not conducive to the provision of end-of-life care (e.g., prohibiting the storage and administration of narcotics, requiring that residents be actively seeking employment; Cagle, 2009; Shulman et al., 2018).
Hospital environments are, likewise, largely inconsonant with the provision of palliative care to homeless persons. A qualitative study of 4 homeless individuals and 10 community experts serving homeless and nonhomeless poor found that chronically sick homeless persons are often undertreated in hospital and have early and inappropriate discharge dispositions (Davis-Berman, 2016). According to Nyatanga (2012), in the context of homelessness, the concept of discharge must be reexamined. Fragmentation in existing systems, coupled with complex referral processes, leads to gaps in care for dying homeless persons, with frequent referrals, a lack of accountability by a single organization to coordinate care, and limited choice regarding care options (Davis-Berman, 2016; Shulman et al., 2018; Webb, 2015).
Institutional policies prohibiting alcohol and illicit drug use preclude many homeless persons from accessing mainstream end-of-life care services (McNeil & Guirguis-Younger, 2012; McNeil, Guirguis-Younger, & Dilley, 2012; NHS Improving Quality, 2014; Podymow et al., 2006; Serge & Gnaedinger, 2003). One small (N = 7) qualitative study of homelessness and palliative care (Krakowsky et al., 2012) found that many homeless persons’ access to palliative care is compromised because the system is not oriented toward a harm reduction philosophy of care. Harm reduction services were identified in another study (McNeil, Guirguis-Younger, Dilley, Aubry, et al., 2012) as a critical point of entry to and source of end-of-life care for homeless persons who use alcohol and illicit drugs; however, participants in this study noted that residential harm reduction programs are not adequately resourced to provide end-of-life care to clients.
Financial barriers
A number of papers discussed financial barriers to palliative care, including inadequate insurance coverage for homeless persons (Davis-Berman, 2016; Gehlert & Moro, 2011; Kushel & Miaskowski, 2006; McNeil, Guirguis-Younger, & Dilley, 2012; National Health Care for the Homeless Council, 2004; Rousseau, 1998; Song, Bartels, et al., 2007). Effiong and Harman (2014) identified the high costs of providing home hospice to unbefriended persons as a barrier to care. The Medicare hospice benefit is not adjusted for the cost or intensity of care, creating a disincentive for hospice providers to enroll patients requiring complex palliative interventions.
Ethical and jurisdictional challenges
Some papers discussed moral and ethical challenges for providers around decision-making for homeless terminally ill persons who lack surrogate decision makers (Gehlert & Moro, 2011; Ko & Nelson-Becker, 2014; Kushel & Miaskowski, 2006). Gehlert and Moro (2011) indicated that this issue is compounded by a lack of statutory authorization in most states for physicians to assume default surrogacy without judicial involvement. Further, Webb (2015) noted that palliative care provision in environments not designed for end-of-life care presents professional jurisdiction and role boundary issues, which are contrary to the holistic ethos of palliative care.
Multiple oppression
Issues of intersectionality were pervasive in the literature. Homeless persons may be multiply oppressed and socially excluded due to several intersecting marginalized identities (e.g., homelessness, mental health status, and race). Minority ethnic communities face particular barriers in accessing specialist palliative care, including communication challenges, social deprivation, ethnocentrism, and gate-keeping (Ahmed et al., 2004; Hindmarch, 2012). Persons with severe and persistent mental illness may have undesirable behaviors that are unwelcome in the health-care community (Baker, 2005). The limited availability of hospice services in low-income urban areas (Lewis et al., 2011), lack of outreach by hospices to the homeless population (Effiong et al., 2014), and lack of data on older homeless persons (Nyatanga, 2012) are also important structural barriers.
Models of Care
Palliative care models identified in the literature can be broken down into four major categories: (a) shelter- or hostel-based palliative care, (b) residential inpatient hospice palliative care, (c) long-term inpatient medical care, and (d) respite inpatient medical care. The first two categories provide palliative care specifically, while the last two categories provide palliative care as a natural extension of other types of health care that are initially offered.
Shelter-based palliative care
St. Nicholas Hospice Care in the United Kingdom (Hindmarch, 2012), Palliative Education and Care for the Homeless (PEACH) in Toronto (Dosani, 2014), St. Mungo’s Broadway in the United Kingdom (Davis et al., 2011), Malachi House in Cleveland (Mramor, 2001), and the Supportive Care Program at St. Vincent’s Hospital in New York (National Health Care for the Homeless Council, 2004) are five examples of shelter- or hostel-based palliative care services. Although each program is unique, there are common features among them, including meeting the patient where they are geographically, working in collaboration with professional health-care providers, and consulting with or receiving care directly from palliative care specialists to provide end-of-life care in a homelike environment (Cipkar & Dosani, 2016; Davis et al., 2011; Dosani, 2014; Hindmarch, 2012; National Health Care for the Homeless Council, 2004).
Some creative innovations include educational interventions and bereavement support for shelter staff and shelter users, as well as for palliative health-care providers (Davis et al., 2011; Dosani, 2014). Dosani (2014) identified the importance of providing support for terminally ill homeless persons as early as possible to maximize the effectiveness of the care. To do so requires shelter staff to have the knowledge to recognize when palliative care is indicated and to counsel shelter users on the potential benefits and risks of engaging in such care.
Residential inpatient hospice palliative care
Unlike shelter-based palliative care, residential inpatient hospice palliative care is a model of care in which a residence is open exclusively to house people who require palliative care and who have no one, either formally or informally, to appropriately care for them elsewhere. Elements found in the majority of residential inpatient hospice palliative care programs that are inclusive of homeless persons include services offered exclusively to homeless persons (Collier, 2011; Effiong et al., 2014; Page et al., 2012; Podymow et al., 2006), the goal of providing safe and supportive housing for people who do not have access to this elsewhere (Collier, 2011; Effiong et al., 2014; National Health Care for the Homeless Council, 2004; O’Mahony et al., 2008; Page et al., 2012; Podymow et al., 2006), collaboration with outside interdisciplinary health-care professionals (Collier, 2011; Effiong et al., 2014; O’Mahony et al., 2008; Podymow et al., 2006), provision of both acute care and palliative care interventions (Effiong et al., 2014; Podymow et al., 2006), and respect for patients’ wishes to return to life on the street if this is what feels most comfortable (Effiong et al., 2014; Podymow et al., 2006).
By offering services exclusive to homeless persons, these programs are able to cultivate an environment that is comfortable and home-like for patients who may not feel this sense of security in a paternalistic hospital setting (Collier, 2011; Effiong et al., 2014; National Health Care for the Homeless Council, 2004; O’Mahony et al., 2008; Page et al., 2012; Podymow et al., 2006). Bringing in palliative care specialists from hospitals or the community ensures that patients in residential hospice settings receive similar levels of care as those who are being cared for in a hospital setting. Unlike traditional palliative care programs, some of these residential inpatient hospice palliative care programs offer the option for patients to receive acute care and palliative care interventions simultaneously. This is in recognition of the reasoned desire that many homeless persons have to regain enough strength and overall health to return to their life on the street (Effiong et al., 2014; Podymow et al., 2006).
One model of care implemented an outreach program whereby staff promoted the program directly to homeless persons living on the street or in shelters (O’Mahony et al., 2008). Another model of care used a harm reduction approach to manage substance abuse, assisted with end-of-life care planning and considerations, and held a service for each individual after they passed away (Podymow et al., 2006).
Long-term subsidized housing providing medical care
Long-term subsidized housing providing medical care was only discussed in one of the articles. Serge and Gnaedinger (2003) reviewed case studies of several care providers for homeless persons, including three long-term subsidized housing programs that include medical care services for homeless persons. Although palliative care is not the intended purpose, the residents are older adults, many of whom do in fact end up spending their final days in these facilities. Because of this, palliative care is provided as a natural extension of primary health care that is provided.
Elements found in many of the long-term subsidized housing programs providing medical care include subsidized rent, meals, and facilities for basic daily necessities (e.g., bathing, laundry, etc.), on-site access to an interdisciplinary medical team, and a focus on maintaining dignity at the end of life (Serge & Gnaedinger, 2003).
Respite inpatient medical care
Inpatient respite services typically provide acute or postacute medical care for homeless persons who are not ill enough to require hospitalization but are too ill to be discharged to a shelter or the street (Doran, Ragins, Gross, & Zerger, 2013). Three articles discussed the provision of end-of-life care to homeless persons within respite facilities (Koh & O’Connell, 2016; National Health Care for the Homeless Council, 2004; O’Connell, 2005). Although medical respite programs may not be equipped to provide the same level of pain management as specialist palliative or hospice services (National Health Care for the Homeless Council, 2004), they have the potential to improve continuity of care, enhance dignity, and offer an innovative solution to better meet the end-of-life needs of homeless persons (Koh & O’Connell, 2016; National Health Care for the Homeless Council, 2004).
Costs of palliative care for homeless persons
Lewis et al. (2011) demonstrated that the end-of-life care costs are significantly higher for lower income individuals than for those with higher incomes. For homeless persons, the cost differences in health care arise from such factors as multiple comorbidities (e.g., substance abuse issues, mental health issues, disease, etc.), the necessary increases in support from health-care providers because of a lack of personal supports, and more frequent hospital readmissions and emergency calls (Lewis et al., 2011). The establishment of more accessible pathways to palliative care for homeless persons has the potential to substantially reduce the end-of-life care costs for this population (Huynh et al., 2015).
Implications for Policy and Practice
Suggestions for care providers
Of the articles that met our inclusion criteria, 32 articles suggested solutions to improve palliative care delivery for homeless persons. Many articles suggested care providers use a patient-centered model of care (Cagle, 2009; Krakowsky et al., 2012; NHS Improving Quality, 2014; Serge & Gnaedinger, 2003; Shulman et al., 2018; Webb, 2015). An emphasis was placed on the importance of the therapeutic alliance and the ability to build trust and deliver compassionate and respectful care (Baker, 2005; Hakanson et al., 2016; Ko & Nelson-Becker, 2014; McNeil, Guirguis-Younger, Dilley, Aubry, et al., 2012; Serge & Gnaedinger, 2003). Ko and Nelson-Becker (2014) recommended that care providers gain a deeper understanding of cultural differences and values when providing end-of-life care to homeless persons. Three articles suggested that care providers consider spirituality when delivering end-of-life care (Ko et al., 2015; Ko & Nelson-Becker, 2014; Parliamentary Committee on Palliative and Compassionate Care, 2011).
The importance of preserving dignity at the end of life and after death is particularly salient to the experiences of many homeless persons (Hakanson et al., 2016; NHS Improving Quality, 2014). In a Swedish qualitative single-case study of support home staff, participants described “redignifying” dying homeless persons by, for example, dressing patients neatly for visitors, even when it is expected that no one will come (Hakanson et al., 2016).
Emerging research suggests that advance directives improve the quality of end-of-life care for homeless persons. Completion of advance directives through shelter-based intervention and with nonspecialist or counseling guidance may drastically increase advance directives completion rates and utilization in this population (Leung et al., 2015, 2017; Song et al., 2008).
A harm reduction and pain management strategy was also suggested as an effective care philosophy (Baker, 2005; Cagle, 2009; Davis et al., 2011; B. Henry et al., 2017; Kushel & Miaskowski, 2006; McNeil, Guirguis-Younger, Dilley, Aubry, et al., 2012; Serge & Gnaedinger, 2003; Webb et al., 2018). Webb et al. (2018) recommended the use of transdermal patches and immediate- and modified-release analgesics to mitigate the difficulties associated with storing and administering medications. Setting realistic treatment goals and prioritizing the most significant care concerns may simplify care management, as homeless persons often have extremely complex health profiles (Hakanson et al., 2016). Hwang et al. (2001) reported that homeless persons receive less outpatient care in the year prior to death than the general population. As such, the authors recommend that clinicians take advantage of hospitalizations to offer interventions that would ordinarily be delivered in a primary care setting.
To obtain the best outcomes, improved education of care providers was suggested (Ahmed et al., 2004; Cagle, 2009; Huynh et al., 2015; McNeil, Guirguis-Younger, & Dilley, 2012; McNeil, Guirguis-Younger, Dilley, Aubry, et al., 2012; McNeil & Guirguis-Younger, 2012; McNeil, Guirguis-Younger, & Dilley, 2012; Serge & Gnaedinger, 2003; Shulman et al., 2018; Song, Bartels, et al., 2007; Tobey et al., 2017; Webb, 2015; Webb et al., 2018). McNeil and Guirguis-Younger (2012) suggested addiction and the end-of-life training for staff working with homeless populations. Some authors (Davis-Berman, 2016; Nyatanga, 2012; Song, Bartels, et al., 2007) recommend that education should be provided to health-care providers about the realities of homelessness in order to increase access and awareness.
Caring for homeless persons at the end of life may confer a significant emotional burden (Shulman et al., 2018; Webb, 2015). Support from peers and employers is critical for staff who frequently function as family to homeless individuals (Davis-Berman, 2016; Hakanson et al., 2016; Webb, 2015). Although it may not be feasible for many homeless persons to reconcile with family from whom they are estranged prior to death, practitioners may help to cultivate a sense of community and connectedness at the end of life (Ko et al., 2015).
A number of innovative resources have been developed to assist service providers in the delivery of effective end-of-life care to homeless persons. For example, the NHS Improving Quality (2014) published a guide to support hostel staff and health professionals engage homeless persons in the end-of-life planning and care. The guide covers each step in end-of-life care pathway, including initiating discussions, care planning and coordination, and care provision in the final days of life and after death. Similarly, Davis et al. (2011) developed a flow diagram of potential care pathways for hostel residents with liver failure, including key points at which opportunities for support, intervention, and referral may be expedient.
Implications for policy and service delivery
Twenty-six articles suggested service- and policy-level solutions to provide better access to care for homeless persons at the end of life. Several articles focused on increasing access to hospice services by providing care where they are (i.e., on the streets or in shelters), minimizing requirements for admission to hospice care, and greater collaboration between health and social service providers (Baker, 2005; Cagle, 2009; Collier, 2011; Davis-Berman, 2016; Dzul-Church et al., 2010; Effiong et al., 2014; B. Henry et al., 2017; “Homeless People Need Better Access,” 2011; Kirchhoff, 2003; Krakowsky et al., 2012; MacWilliams et al., 2014; McNeil, Guirguis-Younger, & Dilley, 2012; NHS Improving Quality, 2014; Nyatanga, 2012; Serge & Gnaedinger, 2003; Shulman et al., 2018; Webb et al., 2018). Webb (2015) suggested that allowing hostel staff and other support personnel to access residents’ medical information may facilitate more equitable and expedient end-of-life care. Parallel planning among primary and secondary care may help to identify individuals who will benefit from palliative care as early in illness trajectory as possible (Webb et al., 2018).
Four articles discussed the need for services in a home-like environment (Baker, 2005; Collier, 2011; Dzul-Church et al., 2010; Krakowsky et al., 2012). Several authors endorsed street-based palliative care and outreach programs (Baker, 2005; Cagle, 2009; Serge & Gnaedinger, 2003). Song et al. (2010) indicated that making advance directives part of the official medical record may increase their accessibility at the time of need, ensuring that homeless persons’ preferences will be met. Leung et al. (2017) endorsed more active measures to increase utilization of advance directives by substitute decision makers and practitioners, including automatic alerts within electronic medical records and secure online repositories.
Serge and Gnaedinger (2003) suggested that the most pressing need for homeless persons at the end of life is supervised long-term residential beds with 24-hour nursing care. Resources are needed to provide homeless seniors flexibility in residential placement, a quiet and peaceful environment, access to a geriatric assessment and treatment unit, and a noninstitutional setting with private or semiprivate rooms (Serge & Gnaedinger, 2003). A number of articles focused on the need for change at a policy or governmental level, including increasing funding for hospices and other palliative care settings to provide equitable access for homeless persons (Lewis et al., 2011; Nyatanga, 2012; Parliamentary Committee on Palliative and Compassionate Care, 2011; Pietroburgo, 2006; Serge & Gnaedinger, 2003), implementing national palliative and end-of-life care strategies, and providing universal coverage for palliative care services on the basis of medical necessity (Parliamentary Committee on Palliative and Compassionate Care, 2011).
Discussion
It is beyond the scope of this review to critically appraise the methodological rigor of the existing empirical evidence or to provide an in-depth analysis of the selected gray and academic literature. In general, there appears to be broad recognition of the heterogeneity of the homeless population and the need for flexible, person-centered services to meet their end-of-life care needs. The findings also suggest that there is a rich and diverse knowledge base regarding the end-of-life needs and preferences of homeless persons and the barriers to accessing appropriate care at various levels of deployment. What emerges strongly from this review is the need to address patient-, provider-, and structural-level barriers in parallel in order to optimize care for homeless persons. In particular, improved education and training for care providers, resourcing of atypical and innovative environments for palliative care provision, greater collaboration among service providers, and an emphasis on compassionate care will help to achieve greater equity in palliative and end-of-life care for homeless persons.
Conclusions
Practitioners and homeless persons must negotiate many challenges in the provision and receipt of palliative care. However, there is tremendous potential and opportunity to enhance dignity and patient autonomy and improve the quality of life at the end of life for this vulnerable population. Future research focusing on evaluating the effectiveness and financial viability of models of care, the perspectives of homeless persons regarding palliative care, the unique needs and preferences of cultural and ethnic minority homeless populations, and increasing the accessibility and utilization of advance directives by surrogate decision makers and practitioners would strengthen the evidence base and inform more effective end-of-life care delivery for homeless persons.
Footnotes
Acknowledgments
The authors gratefully acknowledge the contributions of Dr. Esme Fuller-Thomson, Factor-Inwentash Faculty of Social Work, University of Toronto, who provided guidance in the formulation of the literature search and feedback on an earlier version of the manuscript. The authors also wish to thank the University of Toronto librarians, Jenaya Webb and Judith Logan, for their kind assistance in reviewing and approving the search terms.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.