
Abstract
We recruited 242 elderly suicides and 242 controls above 60 years to conduct face-to-face interviews by psychological autopsy to examine the psychometric characteristics of the Duke Social Support Index (DSSI) in rural China. DSSI had high internal consistency, with Cronbach’s αs of .89 and .90 in suicides and controls, respectively. DSSI was significantly and negatively correlated to loneliness in both samples. Confirmatory factor analysis basically supported the original structure of DSSI, but Item 4 had low factor loading in controls. In conclusion, DSSI has satisfactory reliability and acceptable validity in evaluating social support in the elderly suicide study in China.
Introduction
Suicide, an important public health and social problem, has aroused extensive concern in the world (Khazaei, Armanmehr, Nematollahi, & Rezaeian, 2017; Turecki & Brent, 2016). According to the report by World Health Organization in 2014, over 800,000 people, namely, one person every 40 seconds, die by suicide. China, where suicide was ranked as the fifth cause of death among the whole population (Phillips, Li, & Zhang, 2002), has made an overwhelming contribution to global suicide rate, accounting for approximately 22% of global suicides, or roughly 200,000 suicides every year (Hvistendahl, 2012). In China, suicide rate in rural area was 3 times higher than that in urban area. Although the difference in suicide rate between rural and urban area is increasingly smaller, the suicide rate of rural population is still higher than that of urban rate (Sun, Guo, Zhang, Jia, & Xu, 2013; Wang, Chan, & Yip, 2014; Zhang, Sun, Liu, & Zhang, 2014). The overall suicide rate has decreased apparently in recent years, while the rate of the elderly suicide increased (Wang et al., 2014). During 2013 and 2014, the elderly suicides accounted for 38.2% of overall suicides, while older adults shared only 8.9% of the total population (Zhong, Chiu, & Conwell, 2016). The average annual elderly suicide rate in China was 34.5 per 100,000 (Zhong et al., 2016). So, it is crucial to pay more attention to the elderly suicides in rural China.
Suicide among older adults is associated with physical health (Conwell, Duberstein, & Caine, 2002; Harwood, Hawton, Hope, Harriss, & Jacoby, 2006; Karbeyaz, Celikel, Emiral, & Emiral, 2017), mental disorder (Chiu et al., 2004; Karbeyaz et al., 2017; Wærn et al., 2002; Yeh, Ng, & Wu, 2017), and some socioeconomic factors (Crnek-Georgeson, Wilson, & Page, 2017; Karbeyaz et al., 2017; Liu, Qin, & Jia, 2018; Torresani, Toffol, Scocco, & Fanolla, 2014). Social support, as an important protective factor for various socioeconomic factors, has a significantly negative influence on suicide (Hollingsworth et al., 2018; Kleiman & Liu, 2013; Kleiman, Riskind, & Schaefer, 2014; Poudel-Tandukar et al., 2011; Zadravec Sedivy, Podlogar, Kerr, & De Leo, 2017). Zadravec Sedivy et al. (2017) conducted an ecological study in the relationship between social support and suicide rates in 75 regions of 23 European countries and found social support had a protective effect against suicide on a regional level for both genders, especially for males. Kleiman and Liu (2013) found social support was negatively correlated to the likelihood of a lifetime suicide attempt in two nationally representative samples: U.S. sample (odds ratio = 0.68, p < .001) and English sample (odds ratio = 0.93, p < .01), after controlling for a variety of related psychopathological and demographic variables. Hollingsworth et al. (2018) discovered that perceived burdensomeness mediated the relationship between perceived social support and suicide ideation and the relationship between social connectedness and suicide ideation in college students, which indicated a lack of social support could result in the feeling of being a burden to others, leading to suicide ideation further. In China, there were studies demonstrating that social support was negatively associated with suicide among the whole population (Zhang, Conwell, Zhou, & Jiang, 2004) and the older adults (Liu et al., 2018). In addition, enhancing the social support networks is one of the four steps in suicide prevention guidelines formulated by the United Nations (1996). All these elucidate that social support acts as an independent factor for suicide and an ameliorable factor to decrease suicide rate. So, it is important to measure the level of social support in suicide research studies.
Social support can be measured by various instruments, such as the Social Support Inventory with 27 items in two-part question (Sarason, Levine, Basham, & Sarason, 1983), the Multidimensional Scale of Perceived Social Support with 12 items in 7-point Likert-type format (Zimet, Dahlem, Zimet, & Farley, 1991), and the Social Support Network Inventory with 10 items in 6-point Likert-type response (Flaherty, Gaviria, & Pathak, 1983). But the Duke Social Support Index (DSSI; Koenig et al., 1993) and the Social Support Rating Scale (SSRS; Xiao, 1994) were often used to evaluate the social support in China. SSRS is a self-report questionnaire with 10 items in three dimensions: subjective support, objective support, and utility of support. It evaluated the social support from family, friends, neighbors, colleagues, and various organizations. It has satisfactory reliability and validity in various Chinese population (Li, 2017; Lu, Jia, Zhang, et al., 2011; Su, Wei, Ling, & Tang, 2009; Yang, Feng, & Xia, 2006). Due to its few items and being made on the basis of Chinese culture, it has been widely applied to explore the relationship between social support and suicide in many Chinese research studies (Chen, Ma, & Fan, 2008; Lu, Jia, & Ma, 2011; Sun & Jia, 2014). To our knowledge, this scale was few used in psychological autopsy (PA) research studies. And maybe it is inappropriate to make comparison with results from other countries by SSRS because it is more apt to Chinese environment. In addition, there have been few references about the comparison between the level of social support by SSRS and by other scales in other countries.
DSSI has been extensively used to study the relationship between social support and suicide (Hu, Jiang, & Liu, 2005; Zhang et al., 2003; Zhang & Zhou, 2009). Mao et al. (2015) found DSSI had satisfactory reliability and acceptable validity, and it was better to adjust several items in the older adults by stratified cluster random sampling strategy in a rural elderly population. Jia and Zhang (2012) examined the psychometric characteristics of DSSI in young rural Chinese suicides and controls both aged 15 and 34 years and got similar conclusion. However, these two research studies are either young suicides or general elder population, and there are not much related studies on the examination of DSSI among completed suicides in rural and elderly Chinese. So, this study recruited 242 completed suicides and 242 matched controls both aged 60 years and older to measure the psychometric characteristics of DSSI among elderly suicides and controls in rural China, further to pave a way for the research studies about the relationship between suicide and social support or other-related factors.
Method
Subjects
Based on 1:1 matched case-control design, 242 elderly cases and 242 controls were recruited. Cases were the older adults who were aged 60 years or above and conducted completed suicide during October 8, 2011 to September 5, 2015. Controls were matched on gender, age (±3 years), same or neighboring community, and without suicide history. All suicides and controls were chosen from 12 rural counties from disease surveillance points of Shandong, Hunan, and Guangxi province, which were located in Eastern China, South Central China, and Southern China, respectively. According to death certification system, the project cooperators from the Center for Disease Control and Prevention of each county helped identify and contact cases, with the assistance of village doctors or leaders. They were also responsible for finding suitable controls from the same or near village to match suicides.
Procedures
We conducted face-to-face interview with control himself and two informants of each control and suicide by PA, which was a scientific and systematic method to reconstruct suicidal deaths through informants (Beskow, Runeson, & Asgard, 1991; Isometsa, 2001). The first informant was usually one next of kin, for example, a spouse, a parent, a son, or a daughter. The second informant was always a friend, a neighbor, a colleague, or a remote relative. PA, widely used in suicide studies in China, has been proved to have good validity and reliability (Phillips, Yang, et al., 2002; Yang et al., 2005; Zhang et al., 2002, 2003; Zhou, Jiang, & Zhang, 2006). Interviews were conducted between 2 and 6 months after suicide in order to try to avoid bereavement reaction and minimize recall bias (Conner et al., 2012). After the written informed consent, trained interviewers began interview in a separated room of the village clinic or the interviewee’s home. The average interview time was about 3 hours.
Instruments
Demographic characteristics
Demographic characteristics included gender, age, education (illiteracy, primary school, middle school, high school and above), marital status (stable vs. unstable; stable marital status refers to being married and living with a spouse and unstable marital status refers to being never married, divorced, widowed, or not living with a spouse), employment (employed, unemployed, and retired), family annual income (≤3,600 RMB, 3,600∼10,000 RMB, and ≥10,000 RMB, according to the tertiles), living alone (yes vs. no), religion belief (yes vs. no), superstition (yes vs. no), and family suicide history (yes vs. no).
Duke Social Support Index
The DSSI (Koenig et al., 1993) is a self-report questionnaire to assess social support, including 23 items in three dimensions. There are 4 items expressing social interaction (SIS), 7 items demonstrating subjective social support (SSS), and 12 items stating instrumental social support (ISS). SIS and SSS are designed on a 3-point Likert-type format, while ISS is dichotomous. The total score varies from 11 to 45, with higher scores reflecting more social support. The corrected Cronbach’s α of the University of California Los Angeles Loneliness Scale-6 (ULS-6) was .89 in completed suicides and .90 in controls.
Simplified ULS
The initial ULS-20 (Stephan, Fath, & Lamm, 1988) was deleted 12 items and became ULS-8 (Russell, Peplau, & Cutrona, 1980). The psychometric properties of the ULS had been widely evaluated (Neto, 2014; Russell et al., 1980; Swami, 2009; Wilson, Cutts, Lees, Mapungwana, & Maunganidze, 1992; Wu & Yao, 2008). Zhou, Li, Hu, and Xiao (2012) evaluated it among the older adults in rural China and deleted two items further. The six items are all positive loneliness, on a 4-point Likert-type, from 1 (never) to 4 (always). The range of total score is from 6 to 24, and higher score means more serious loneliness. The ULS-6 has been assessed to have good reliability and validity in Chinese culture (Zhou et al., 2012). In this study, the corrected Cronbach’s α of the ULS-6 was .94 in completed suicides and .91 in controls.
Integration of information
The responses from two informants were largely similar. However, there were also inevitable differences, so it was necessary to integrate different information. For the demographic characteristics and suicide behavior, we relied on the information provided by the first informant. For the diagnosis of mental disease, we tended to adopt the positive response. For the DSSI and ULS-6, we were inclined to use lower score of DSSI and higher score of ULS-6.
Data analysis
IBM SPSS Statistics 24.0 (online edition) and AMOS 24.0 were used for statistical analyses. t Tests or Kolmogorov–Smirnov Z tests were used to compare continual variables. χ2 tests were used to compare categorical variables. The Cronbach’s α was conducted to test internal consistency of DSSI. Spearman correlations between ULS-6 and three dimensions of DSSI and the whole DSSI were examined for criterion-related validity. Confirmatory factor analysis was used to assess construct validity. Models were evaluated by χ2, Goodness-of-Fit Index, Adjusted Goodness-of-Fit Index, Comparative Fit Index, and root mean square error of approximation (Carleton et al., 2013).
Ethical issues
This study was approved by the institutional review board of Shandong University, Central South University, and Guangxi Medical University. All experiments involving human participants were performed in accordance with relevant guidelines and regulations. Trained interviewers explained the aim and procedure of the research and other information that interviewees want to know to all participants. Written informed consent was obtained from all participants before the interviews.
Results
Demographic Characteristics
Among 242 suicides and 242 controls, 135 (55.8%) of them were male for each group. The mean age was 74.4 (standard deviation [SD] = 8.2) years in suicides and 74.1 (SD = 8.2) years in controls.
As shown in Table 1, compared with controls, suicides were more likely to be unemployed, living alone, superstitious, and to have unstable marital status, less social support, and more feeling of loneliness. However, there were no statistically significant differences in education, family annual income, religion, and family suicide history between suicides and controls.
Demographic Characteristics in Suicide and Control Samples.
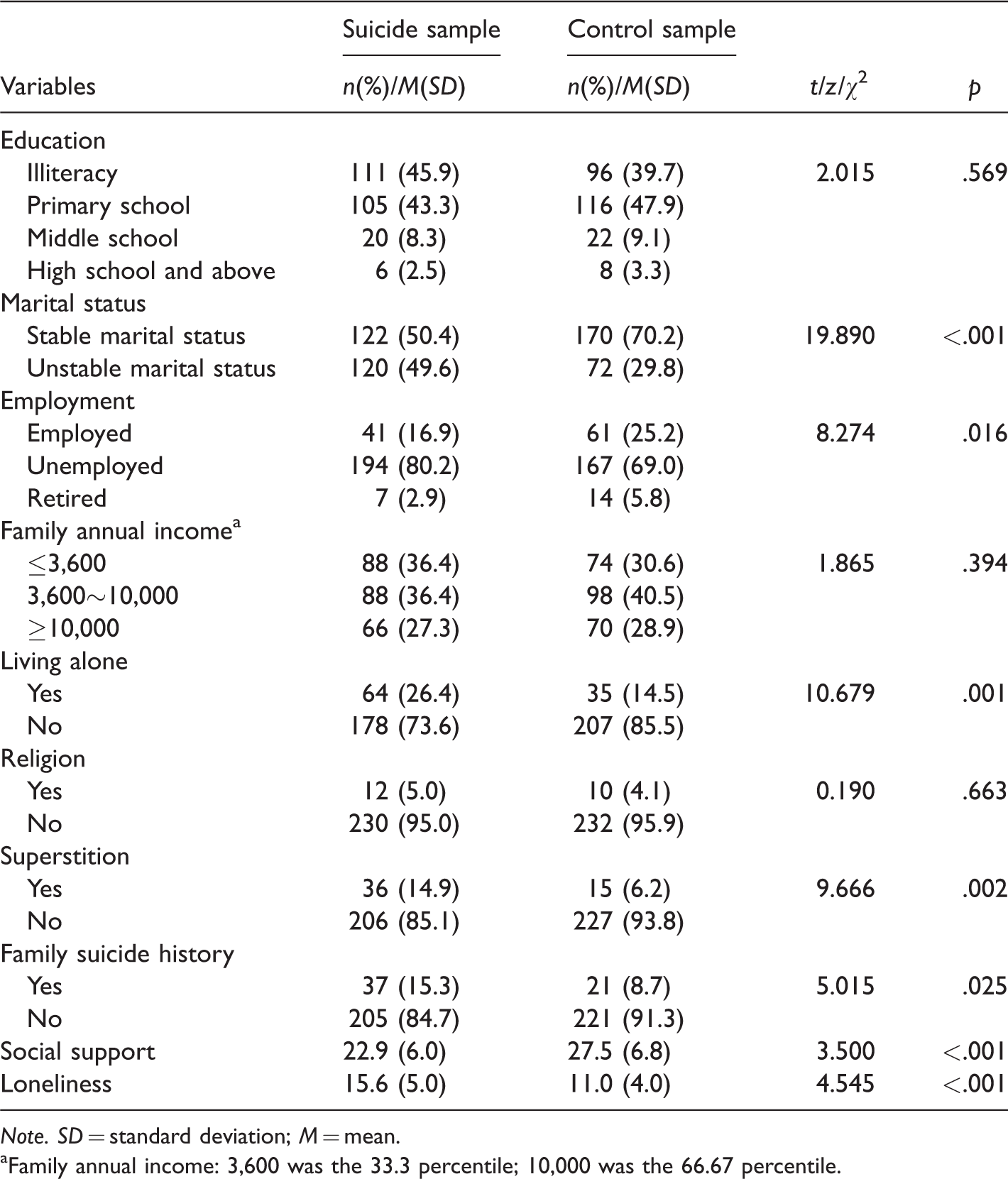
Note. SD = standard deviation; M = mean.
aFamily annual income: 3,600 was the 33.3 percentile; 10,000 was the 66.67 percentile.
Reliability
Table 2 showed mean, SD, corrected item-total correlation, and Cronbach’s α coefficients if item deleted of DSSI in both suicide and control samples. The corrected Cronbach’s α of the DSSI was .89 in completed suicides and .90 in controls. In the suicide sample, the Cronbach’s α was .54 for SIS, .89 for SSS, and .92 for ISS. In the control sample, the Cronbach’s α was .54 for SIS, .92 for SSS, and .91 for ISS. Cronbach’s α coefficients if item deleted ranged from .88 to .89 in suicides and varied from .88 to .90 in controls.
Mean, SD, Corrected Item-Total Correlation, and Cronbach’s α If Item Deleted of Duke Social Support Index in Suicide and Control Samples.

Note. SD = standard deviation; M = mean.
Validity
Table 3 presented that the total DSSI and three subscales were all negatively related to loneliness in male, female, and total suicide and control samples, which verified satisfactory criterion validity.
Correlation Between Scores of Loneliness and Subscales of DSSI and Total DSSI Among Male and Female in Suicide and Control Samples.
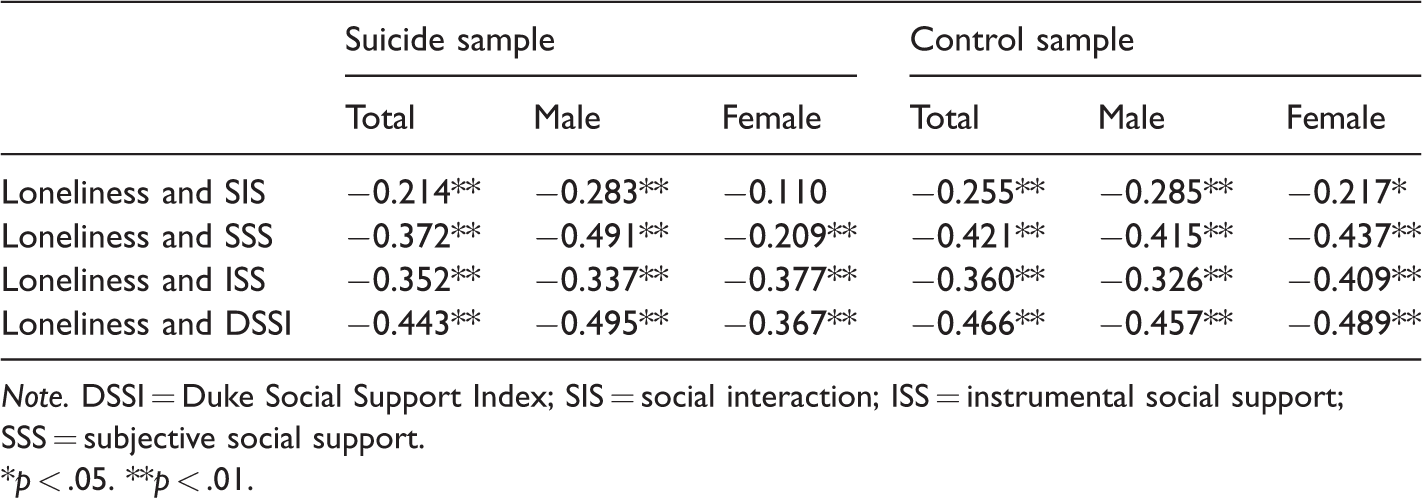
Note. DSSI = Duke Social Support Index; SIS = social interaction; ISS = instrumental social support; SSS = subjective social support.
*p < .05. **p < .01.
As shown in Table 4, confirmatory factor analysis was conducted to confirm the three-factor model. Goodness-of-Fit Index, Adjusted Goodness-of-Fit Index, and Comparative Fit Index were approximately or above 0.80 for both suicide and control samples. The values of root mean square error of approximation were about 0.09 among suicides and controls. Factor loadings in every factor were 0.31–0.80, 0.48–0.86, and 0.60–0.79 in suicides and 0.28–0.73, 0.49–0.88, and 0.55–0.79 in controls, respectively. Apparently, Item 4 had lower factor loadings in both suicides and controls. These results basically fitted the original structure of DSSI.
Factor Loadings of Each Item in SIS, SSS, and ISS of Duke Social Support Index From Confirmatory Factor Analysis in Suicide and Control Samples.

Note. SIS = social interaction; ISS = instrumental social support; SSS = subjective social support; GFI = Goodness-of-Fit Index; AGFI = Adjusted Goodness-of-Fit Index; CFI = Comparative Fit Index; RMSEA = root mean square error of approximation.
Discussion
This study aimed to assess the reliability and validity of DSSI in the elderly suicides and controls in rural China. The findings indicated that DSSI had satisfactory reliability and acceptable validity in Chinese culture, which was consistent with the previous study (Jia & Zhang, 2012). In terms of demographic characteristics, some differences between suicides and controls were statistically significant, which was also similar to the previous findings (Liu et al., 2018; Zhang et al., 2004).
Many studies have proved that DSSI has good internal consistency in various Chinese populations. For instance, the Cronbach’s α coefficient was .84 for suicide group and .79 for control group in young rural Chinese population (Jia & Zhang, 2012). Another study showed high Cronbach’s α of .88 in a rural elderly population (Mao et al., 2015). In this study, the Cronbach’s α coefficients were both above .89 in suicides and controls, indicating good internal consistency and satisfactory reliability of DSSI in the elderly suicide research in rural China.
The relationship between social support and loneliness has been tested (O’Donovan & Hughes, 2007; Wright, 2005; Yildirim & Kocabiyik, 2010; Zhang, Gao, Fokkema, Alterman, & Liu, 2015). So, it is suitable to use loneliness to assess the concurrent validity of DSSI. In this study, the ULS-6 was adopted, which had high degree of internal consistency and validity in Chinese culture (Zhou et al., 2012). In the total samples, both in suicide group and control group, loneliness was statistically correlated to SIS, SSS, ISS, and DSSI, indicating DSSI had good concurrent validity. Most of results in Table 3 were statistically significant (p < .01), whereas there was no statistical significance in the relationship between loneliness and SI among female suicide sample (p > .05) and no strong statistical significance among female control sample (p < .05). Maybe it is because majority of Chinese females pay most attention to taking care of family and have few friends and few interactions with the world outside family after their marriage. But they are pleased to do so and do not feel lonely.
The three-factor model of DSSI had an acceptable goodness of fit in the suicide and control samples in rural China. In addition, the factor loadings of most items were high, except Item 4 (0.31 in suicide sample, 0.28 in control sample). Item 4 was how often did you go to meetings of clubs, religious meetings, or other groups that you belonged to in the past week or in the past week before suicide. It could be due to cultural diversity. Different from Western countries, the rural Chinese might not understand the meaning of club and group and seldom participated in collective activities.
Despite the reliability and validity of DSSI had been reported in China, this was the first study to assess DSSI in suicide research by PA among the older adults in rural China. It paved the way for the further study of the relationship between the elderly suicide and social support and of other risk factors in the elderly suicides in rural China. What’s more, samples in this study were recruited from three provinces of China, making the research more representative.
There are also some limitations in this study. First, in the light of PA, some data were collected from informants. Although the reliability and validity of PA has been proved in previous studies (Phillips et al., 2002; Zhang et al., 2002, 2003; Zhou et al., 2006), the information bias is inevitable. Second, in consideration of interview time and expenditure, we did not add SSRS in the questionnaire and did not conduct test–retest reliability. ULS-6 as a criterion for concurrent validity might not be appreciated and it might be better to use SSRS.
Footnotes
Acknowledgments
The authors are very grateful for the support of Shandong University, Central South University, and Guangxi Medical University. The authors also appreciate all the Center for Disease Control and Prevention cooperators, village doctors or directors, interviewers, and interviewees from Shandong, Hunan, and Guangxi.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the American Foundation of Suicide Prevention to Dr. Liang Zhou under Grant No. SRG-0–169-12.