
Abstract
Ensuring use of valid and reliable scales for evaluating death anxiety that are relevant to the cultural context where they are applied is essential. The purpose of the study was to conduct a systematic review of the psychometric properties of Templer’s Death Anxiety Scale (DAS) across cultures. PubMed, Scopus, Web of Knowledge, SID, and Magiran databases were systematically searched for studies published between 1970 and 2017 using Mesh terms. Two independent researchers used Quality Assessment of Diagnostic Accuracy Studies and Checklist of Standards for Reporting of Diagnostic Accuracy to evaluate study quality. Included studies were conducted in Iran, United States, Italy, China, Egypt, Spain, and Australia. Overall study quality was acceptable in 15 evaluated articles. However, findings demonstrated that two (one study), three (seven studies), four (four studies), and five factors (three studies) were extracted across the respective studies. Confirmatory concurrent validity was assessed in two studies. While Templer’s DAS has stood the test of time as a commonly used index of capturing the conscious experience of death anxiety, there are psychometric inconsistencies in identified factor solutions across cultures. Findings emphasize the need for continued evaluation of how the DAS is translated in specific countries with assessment in relation to other death construct tools.
Introduction
Death anxiety is a distressing but common human experience evoked by reminders of mortality. Fears evoked by the reality of death may be associated with existential angst and can trigger avoidant self-protective psychological responses that are maladaptive to many life situations (Sharif Nia et al., 2014). Further death anxiety may be a factor associated with mental health conditions including anxiety, depressive, and posttraumatic stress disorders (Iverach, Menzies, & Menzies, 2014). Characteristics such as age, developmental stage, gender, spiritual and religious beliefs, presence of life-threatening conditions, sociocultural norms, life experiences, and death exposures impact the occurrence of death anxiety (Lehto & Stein, 2009; Li, Mardhekar, & Rodriquez, 2017; Soleimani, Lehto, Negarandeh, Bahrami, & Chan, 2017). Although death anxiety is a ubiquitous phenomenon across the human experience globally, manifesting both consciously and unconsciously, it may be expressed differently across cultures internationally (Chen et al., 2016; Peters et al., 2013; Sharif Nia, Pahlevan Sharif, et al., 2016).
Globally, nurses are at the forefront in supporting patients who are facing life-threatening stressors (Sharif Nia, Ebadi, Lehto, & Peyrovi, 2015). Although it is recognized that death and dying curriculum is essential to better prepare nurses in the care of patients facing death (Sharif Nia, Lehto, Ebadi, & Peyrovi, 2016), nurses may not personally perceive that they are equipped to care of patients facing death anxiety (Peters et al., 2013). Nurses and other medical personnel may experience death anxiety themselves when faced with reminders of mortality increasing the relevance of readily available objective assessment indices for application in health-care environments (Peters et al., 2013).
Accurate assessment of death anxiety is imperative given empirically supported relationships to adaptation (Jong et al., 2018). The multitude of death anxiety studies provides a clear indication of the wide relevance of the concept across disciplinary fields (Henrie & Patrick, 2014; Mejia, Hyman, Behbahani, & Farrell-Turner, 2016; Saini, Patidar, Kaur, Kaur, & Kaur, 2016; Tong et al., 2016). The importance of factors such as religiosity, spirituality, and cultural norms including gender socialization related to the presence of death anxiety have also been identified (Krause & Hayward, 2014; Soleimani, Lehto, Negarandeh, Bahrami, & Sharif Nia, 2016). Although there are several scales available that evaluate death anxiety, the most commonly used scale is the Death Anxiety Scale (DAS) that was developed by Templer and that was first published in 1970 (Sharif Nia, Lehto, et al., 2016). However, Lester and Castromayor claimed early that the DAS does not discriminate between death fears for oneself and for others and was less strongly associated with the fear of others’ dying than were other components of death anxiety (Lester & Castromayor, 1993). The DAS scale was originally published as a 15-item measure (Templer, 1970) with a more widely used 51-item extended format published in 2006 (Templer et al., 2006). The short-form version (15-items) incorporates a yes-no question format and is scored from 0 to 15 with higher scores indicating higher levels of death anxiety (Templer, 1970). The DAS extended-form utilizes a 5-point Likert-type scale that is scored between 1 (completely disagree) to 5 (completely agree). Higher scores on this version also indicate higher death anxiety (Sharif Nia et al., 2014). While there are many studies that have evaluated the psychometric properties of the DAS, the scales’ validity has not been substantively assessed with a pooled evaluation (Neimeyer, Moser, & Wittkowski, 2003). Some researchers recommended that DAS would be more suitable to assess the fear of death separately from the fear of dying and to measure these fears for oneself and for others, giving four separate measures of death anxiety (Lester & Castromayor, 1993). Indeed, while over the past five decades, many researchers have used the DAS scale in their studies, an overall picture of the psychometric properties of the scale is still largely absent. Previous studies using a variety of methods identified different factor structures but the relationships among the specified models have been unclear. Moreover, findings of the past studies indicate the strong scholarly interests in understanding this concept among different group of patients. However, limited comprehensive conclusions have been achieved. Thus, there has been limited systematic appraisal of cross-cultural findings to determine evidence for widespread application in clinical settings across cultures. Given globalization and the subsequent pressure of multiculturalism in health-care settings internationally, it is essential to evaluate the best evidence of death anxiety assessment comparatively in both healthy and medically ill populations across the world. Therefore, this study responds to this gap by conducting a systematic review of the research papers evaluated psychometric properties of Templer’s two DAS instruments in various contexts. The two DAS instruments are the most commonly applied versions across cultures globally.
Methods
This study adhered to the preferred reporting items for systematic reviews guidelines (Panic, Leoncini, De Belvis, Ricciardi, & Boccia, 2013). The sample is based on articles that systematically evaluated the psychometric properties of the DAS instruments.
Search Strategy and Selection Criteria
A systematic review of International databases including PubMed, Scopus, Web of Science, and Google Scholar, and Iranian databases including SID and Magiran was conducted to evaluate the studies published between January 1, 1970 and August 5, 2017. Mesh terms included “psychometric,” “validity,” “reliability,” “death,” “anxiety,” “scale,” [with the use of OR and AND operators] and were used for assessment of the identified databases (more information about search strategy is depicted in Table 1).
Search Stages.
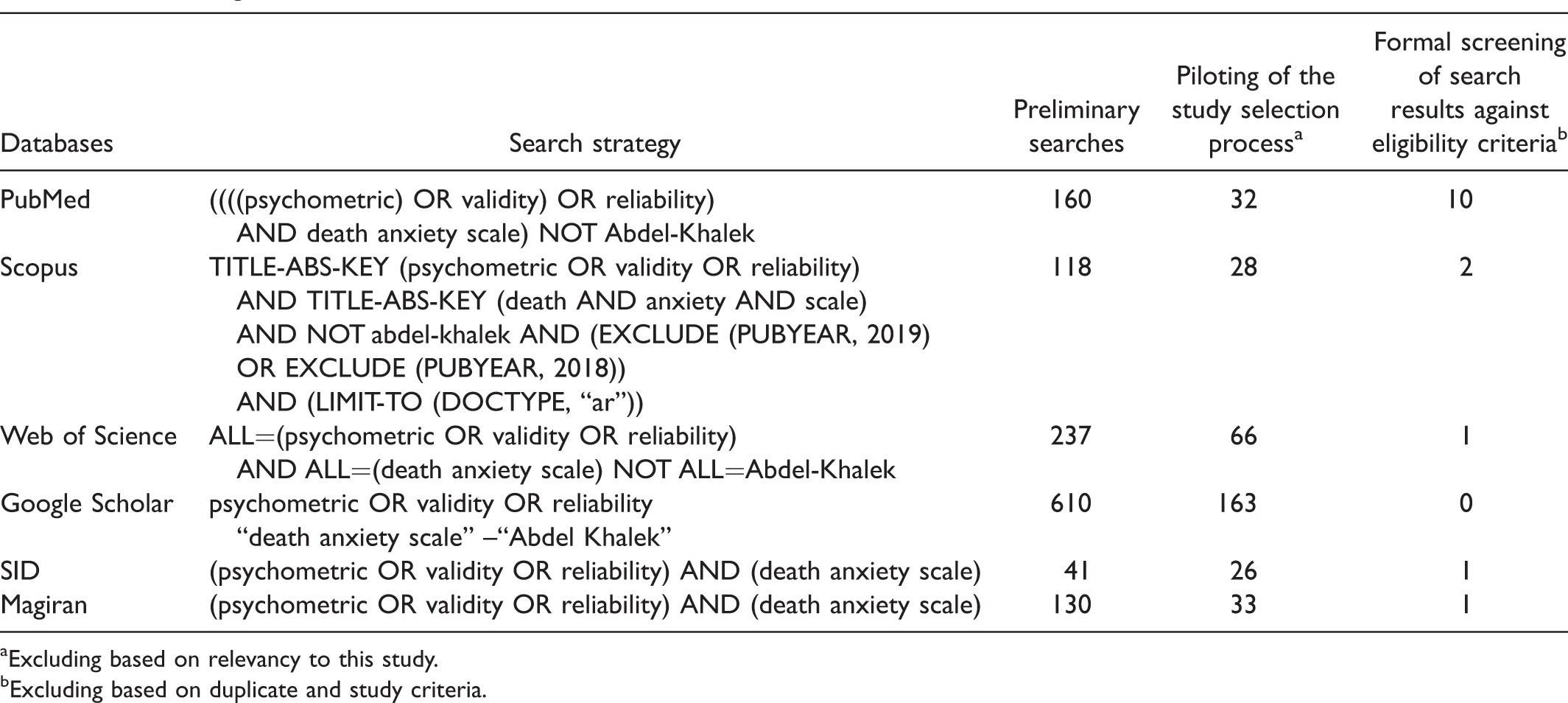
Excluding based on relevancy to this study.
Excluding based on duplicate and study criteria.
First, selected studies from preliminary search were entered to Endnote software and duplicates were removed. Original articles were obtained and then assessed in detail for inclusion by two doctorally prepared researchers. Studies needed to meet both of the following criteria for inclusion: (a) use of Templer’s DAS scales in study and (b) psychometric evaluation (assessment of reliability, validity, and diagnostic accuracy of the DAS). Studies that lacked details of validity and reliability assessments (e.g., factor structure), had an inadequate sample size (<50 participants), and were published in languages other than English or Persian were excluded. Figure 1 illustrates the stages of selecting the articles based on preferred reporting items for systematic reviews guidelines. In next stage, quality assessment was done.
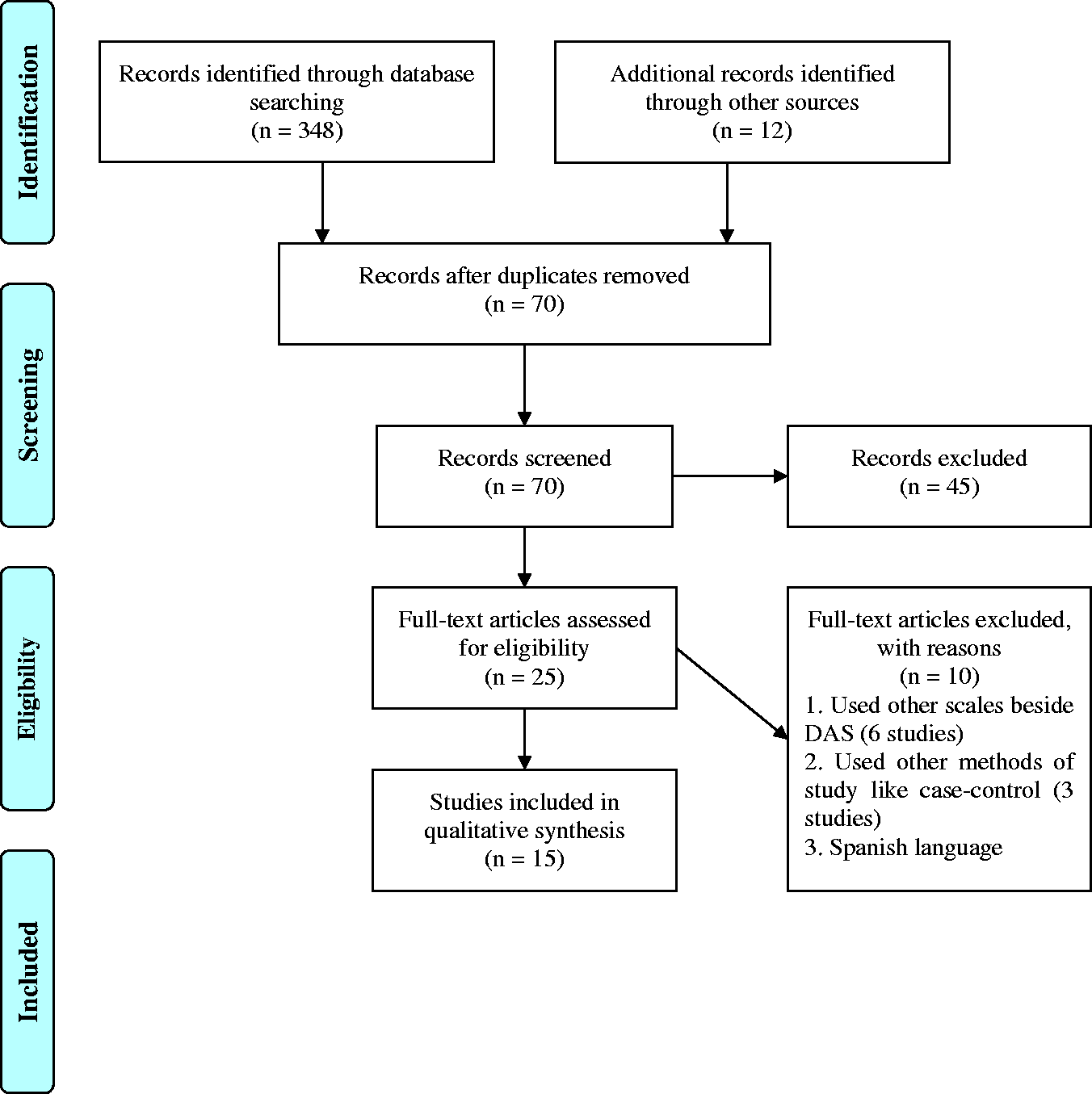
PRISMA diagram.
Quality Assessment (Risk of Bias)
Two researchers independently assessed the quality of the studies incorporated in the review using revised versions of two bias risk assessment tools, the Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) (Whiting et al., 2011) and the checklist of Standards for Reporting of Diagnostic Accuracy (STARD) (Bossuyt et al., 2003). While both of these tools examine risk bias in the accuracy and comprehensiveness of study reports, our findings suggested that incorporating both tools simultaneously but with revision of specific items strengthened the examination of the studies under scrutiny (Oliveira, Gomes, & Toscano, 2011). QUADAS-2 consists of 14 items with a three-option answers (i.e., yes, no, and unknown) that points to the internal consistency of the study under review (Whiting et al., 2011). The 25-items checklist of STARD, on the other hand, was used to check the study design quality (including sample collection and data). The flexibility associated with combining these two tools ensured their consistency with the goals of the study aimed at assessing the validity and reliability of DAS in a cross-cultural analysis (Oliveira et al., 2011). Thus, three items (Items 10–12) and five items (Items 1, 12, 18, 21, 23) from the QUADAS-2 and STARD checklists were omitted from the quality review assessment. To ensure that the process used to evaluate quality was consistent, we ensured interrater reliability by using standardized procedures for both independent analyses, and then compared findings from the two assessments to ensure parallelism in interpretation (Miles, Huberman, & Saldana, 2020).
Data Collection and Construct Validity Assessment
The following information was extracted for each study: author(s), year of publication, country of origin, type of study design, mean age of participants, type of sample, sample size, setting, number and name of factors, reliability assessments, and major findings or outcomes. To assess the construct validity in the studies, weighted averages of the percentage of extracted variances were estimated. Although there are differences between principal component analysis (PCA) and exploratory factor analysis (EFA) used to extract factors, many researchers used them interchangeably and PCA is often used when EFA would be more suitable (Hahs-Vaughn, 2016). EFA focuses on the shared variance of the variables whereas PCA focuses on the total variation among the variables; thus, the percentage of extracted variance of PCA will be greater than EFA (Park, Dailey, & Lemus, 2002). In the social and behavioral sciences, it is common to find around 60% of the total extracted variance explained in factor analysis model (Child, 2006).
Results
Table 2 describes a summary of the papers features entered into this study.
Characteristics of the Studies Selected for the Systematic Review.

Note. DAS = Death Anxiety Scale; ICC = intraclass correlation coefficient.
*One dimension only.
The 15 studies that were surveyed for this review were published between 1970 and 2017. Sample sizes ranged from 50 to 584 participants. Three studies used the DAS-51 and 12 used the DAS-15. The mean age of participants in the studies was 18.84 years (SD = 1.08) to 51.7 years (SD = 15.13). These studies were conducted in Iran (Rajabi & Bohrani, 2001; Sharif Nia et al., 2017; Sharif Nia et al., 2014; Sharif Nia, Pahlevan Sharif, et al., 2016; Soleimani, et al., 2016; Soleimani, Pahlevan Sharif, Allen, & Sharif Nia, 2017; Soleimani, Yaghoobzadeh, Bahrami, Sharif, & Sharif Nia, 2016; Tavakoli & Ahmadzadeh, 2011), the United States (Royal & Elahi, 2011; Templer, 1970), Italy (Saggino & Kline, 1996), China (Yang et al., 2016), Egypt (Abdel-Khalek et al., 1993), Spain (Tomás-Sábado & Gómez-Benito, 2002), and Australia (Warren & Chopra, 1979). Data were collected from war Veterans (Sharif Nia et al., 2014; Family caregivers of cancer patients (Soleimani, Bahrami, et al., 2016)), cancer patients in hospital oncology wards (Royal & Elahi, 2011; Soleimani, Lehto, et al., 2016; Soleimani, Yaghoobzadeh, et al., 2016; Yang et al., 2016), healthy university students (Abdel-Khalek et al., 1993; Rajabi & Bohrani, 2001; Tavakoli & Ahmadzadeh, 2011; Templer, 1970; Tomás-Sábado & Gómez-Benito, 2002; Warren & Chopra, 1979), volunteer subjects (Saggino & Kline, 1996), and cardiac patients (Soleimani, Pahlevan Sharif, et al., 2017) in hospital settings. The sample utilized in data collection was not apparent in one study (Saggino & Kline, 1996). Most of the studies did not report the time that it took to collect the survey data from the respective participants.
Construct Validity Using Factor Analysis
With the exception of one study, all studies evaluated the DAS utilizing a factor analysis statistical technique (Table 3). While the majority of the studies (n = 12) used PCA to extract the factors, two studies used maximum likelihood EFA. It is recognized that the factor extraction method can alter the structure of the covariance matrix. Two, three, four, and five factors were extracted in one (Royal & Elahi, 2011), seven (Saggino & Kline, 1996; Sharif Nia, Pahlevan Sharif, et al., 2017; Soleimani, Bahrami, et al., 2016; Soleimani, Yaghoobzadeh, et al., 2016; Soleimani, Lehto, et al., 2016; Soleimani, Pahlevan Sharif, et al., 2017; Warren & Chopra, 1979), four (Sharif Nia et al., 2014; Sharif Nia, Pahlevan Sharif, et al., 2016; Tomás-Sábado & Gómez-Benito, 2002; Yang et al., 2016), and three studies (Abdel-Khalek et al., 2008; Rajabi & Bohrani, 2001; Tavakoli & Ahmadzadeh, 2011) respectively. The weighted average of the percentage of extracted variances by PCA with 15 and 51 items was estimated 51.45% and 46.08%, respectively. Although no fixed threshold exists, certain percentages have been recommended. For example, researchers in humanities and psychological studies have commonly identified the explained variance as low as 50% to 60% (Hair, Black, Babin, & Anderson, 2013; Pett, Lackey, & Sullivan, 2003).
Factor Analysis and Internal Consistency of the DAS.
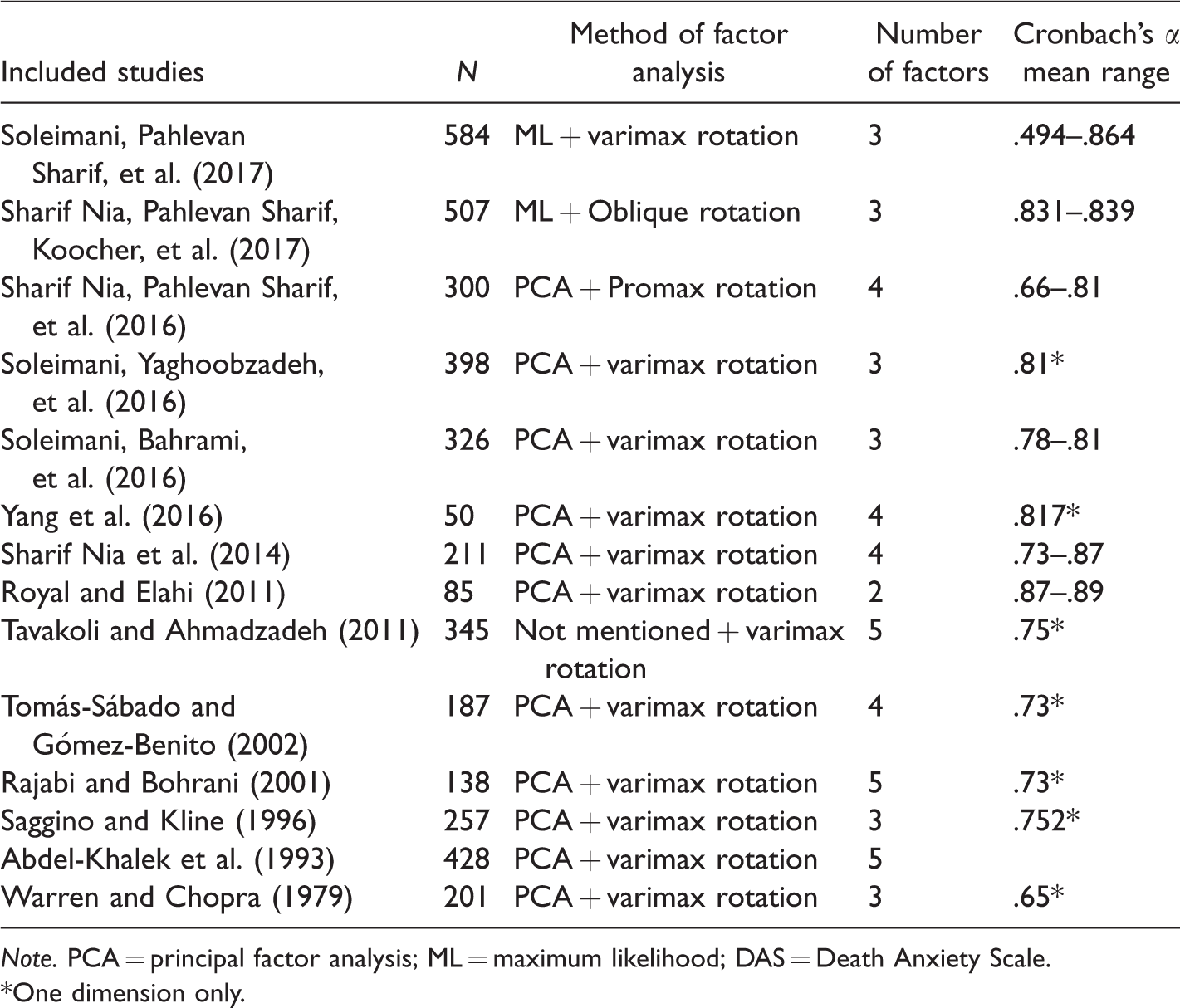
Note. PCA = principal factor analysis; ML = maximum likelihood; DAS = Death Anxiety Scale.
*One dimension only.
Concurrent Validity Using Pearson Correlation Test
Where reported, we display concurrent validity findings in Table 4. Concurrent validity was assessed using the same tool in two studies (Rajabi & Bohrani, 2001; Templer, 1970). Tools that were used to report concurrent validity included general anxiety scales and fear and concern about death scales.
Concurrent Validity of the DAS Using Pearson’s r.
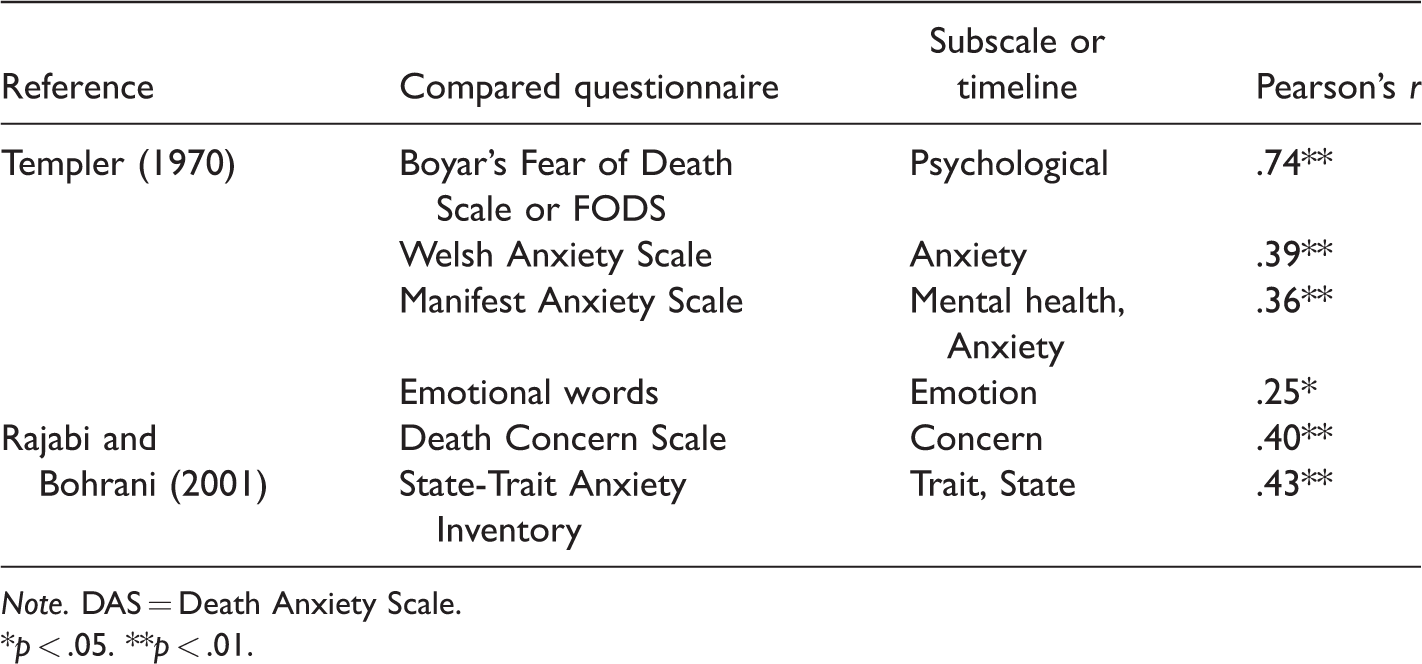
Note. DAS = Death Anxiety Scale.
*p < .05. **p < .01.
Anxiety scales
The validity of DAS was assessed by comparative evaluation with other anxiety scales in two studies. The correlation of the DAS was compared with the Welsh Anxiety Scale, Welsh Anxiety Index, and Manifest Anxiety Scale (.36, p < .001) in Templer’s (1970) original paper reporting the psychometrics of the new instrument. The DAS has also been compared with the State-Trait Anxiety Inventory (.43, p < .001) (Rajabi & Bohrani, 2001).
Fear and concern about death scales
Two studies reported correlation matrices of the DAS with the Fear of Death Scale and the Death Concern Scale (Rajabi & Bohrani, 2001; Templer, 1970). The findings demonstrated significant correlations, with the association more significant in the first study (.74, p < .001) compared with the Death Concern Scale (.40, p < .001). In Templer’s (1970) original study, the concurrent validity of the DAS was also evaluated using comparative links to emotional words (.25, p < .05).
Review the Quality of Studies
The studies that focused on the validation of DAS were evaluated to assess the risk using the revised versions of QUADAS-2 and STARD described previously. In general, the quality of studies was acceptable based on the risk assessment tools (see Figure 2). The risks for bias that were noted include possibility of loss of important results, lack of descriptions of the study inclusion and exclusion criteria, and issues relative to the acceptability and management of selected samples. Also, the interreliability between two reviewers was calculated using intraclass correlation coefficient (QUADAS-2 = 0.828; 95% CI [0.489, 0.942]; and STARD= 0.702; 95% CI [0.113, 0.900]) showed acceptable range.
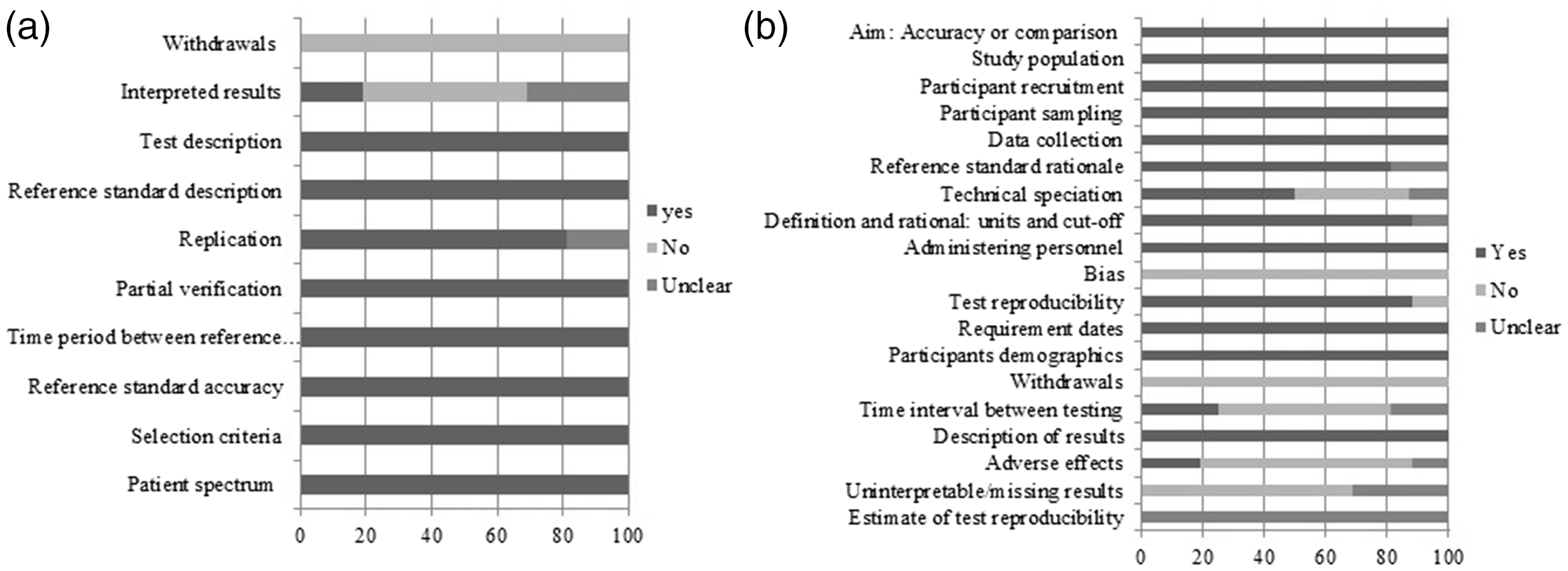
Reporting quality of DAS validity studies as per as modified QUADAS-2 (a) and STARD (b). Note that criteria that are “Unclear” or not reported, “No” introduces a risk of bias.
Discussion
Studies evaluating the concept of death anxiety have substantially grown since the development of the DAS scales by Templer and his associates almost five decades ago. This work has been conducted in multiple countries and in samples ranging from psychiatric and medically ill groups to healthy university students and professional caregivers. Our study’s contribution is a systematic assessment of the psychometric research that has evaluated the DAS instruments across such diverse groups cross-culturally using systematic quality evaluation methods. While this is not the first study to report mismatches between Templer’s original scale and translated findings into other languages (Sarıkaya & Baloğlu, 2016), it provides an organized review of studies published in English.
The international samples from the studies represented people from Asia, Europe, Australia, and the United States. Most of the studies included in the analysis were from the country of Iran. The emphasis from the country of Iran reflects university research programs that have primarily evaluated the impact of death anxiety using the Templer DAS tools in clinical and nonclinical groups. The narrow representation globally is a limitation for international application of the DAS tool. Research incorporating and comparing the DAS to other death anxiety instruments created in other countries (Abdel-Khalek, Lester, Maltby, & Tomás-Sábado, 2009), and also reflecting data from other parts of the world in countries such as Africa and South America is warranted.
While the DAS is one of the first tools to measure death anxiety, there has been extensive research evaluating death perceptions, beliefs and attitudes, and concerns and fears (Neimeyer et al., 2003; Abdel-Khalek et al., 2009). While this growing body of research has made a strong contribution to better our understanding of factors associated with death anxiety, the broad and varied application of this work have stymied the ability to generalize findings across cultures. Furthermore, while there have been new tools to evaluate death anxiety in other cultures (e.g., Abdel-Khalek et al., 2009; Sarıkaya & Baloğlu, 2016), there has been a dearth of research that has focused on the development and assessment of death anxiety tools that can be used to diagnose death anxiety in health-care settings. Thus, this study is useful in that it systematically appraises studies that have incorporated the DAS across cultures utilizing a standardized strategy. Strengths of the systematic review are that the incorporated studies were similarly divided among healthy populations and patients with life-limiting or threatening conditions. The observation of inconsistent numbers of factors identified in the psychometric evaluation of the DAS is an important but not entirely surprising finding of this review. There may be differences in translation of the instrument content in the respective countries. There may also be differences in the cultural manifestation of death anxiety across the various international regions.
Construct validity, especially factor analysis, is at the heart of measurement of psychological constructs (Nunnally & Bernstein, 1994). Given that PCA retains an accounting for a maximal amount of items, total extracted variance versus in the EFA approach account for common variance, thus extracted variance in PCA will be greater than EFA. PCA does not discriminate between shared and unique variance (Osborne, Costello, & Kellow, 2008). During EFA, the shared variance of an item is separated from its unique variance and error variance to reveal the underlying factor structure; thus, only shared variance appears in the solution (Osborne, 2008). Some researchers recommend that EFA is preferable to PCA. PCA is a data reduction method, whereas the object of factor analysis is to expose any latent variables that cause the manifest variables to covary (Gorsuch, 1997).
Limitations
Given only seven databases were used in the study, the possibility exists that certain relevant publications containing death anxiety measures were not identified, a common challenge when conducting systematic reviews. Furthermore, given our initial review targeted article abstracts, it is plausible that information about the measures psychometrics were included in the text of omitted articles. Another limitation includes that concurrent validity was assessed using similar measures in only two of the included studies (Rajabi & Bohrani, 2001; Templer, 1970).
Conclusion
The threat of death is a fundamental and universal concern across cultures globally. Efforts to avoid and escape aversive thoughts and emotions about mortality may contribute to psychiatric morbidity. It is essential that the presence of death anxiety is appraised utilizing accurate assessment tools for patients facing life-threatening stressors as well as in caretakers of patients facing death. While Templer’s DAS has stood the test of time as a commonly used index of capturing the conscious experience of death anxiety across cultures, psychometric inconsistencies in identified factor solutions remain. The review findings emphasize the need for further studies that evaluate how the DAS is translated in specific countries and that evaluate it in relation to other tools that examine death anxiety.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors are grateful to the Deputy of research and technology of Mazandaran University of medical sciences (Sari, Iran) for contribution to financial supports. Also this study was approved by Iran national committee for ethic in biomedical research (Code: IR.MAZUMS.REC.1398.391).