
Abstract
Despite the support with legislation in Turkey regarding extended autonomy and advance directive, there is no clear provision and sufficient practice on the subject. Turkish doctors and nurses are generally unfamiliar with the conception of extended autonomy or advance directive, which raises dilemmas in terms of life-support choice, and this situation can even affect clinical decision-making processes. This study investigated the awareness level about extended autonomy and advance directive in Turkey and assessed doctors and nurses’ attitudes toward patient autonomy. This was a quantitative descriptive study. It was found that the 46.8% of the respondents supported the principle of extended autonomy in health service delivery. However, 53.8% of the respondents had poor knowledge regarding advance directive. Majority (77.9%) of the respondents indicated that the legislative arrangements should be made concerning the principle of extended autonomy and the advance directive, which is its field of application.
According to Kant (1785), the first philosopher who applied the concept of autonomy to an individual, autonomy was the basis of the value of man and every intellectual being. Kant suggested that man is both the determiner and the implementer of his or her actions. Faden and Beauchamp (1986) state that the autonomy is related to individual sovereignty, freedom to make choice, choosing his or her own moral position, and to accept the responsibilities of these choices. Dworkin (1988), who has important opinions in terms of autonomy discussions, indicates that autonomy involves independence, freedom of movement, freedom of will, and critical thinking.
It is known that the interventions in the case of illness causes certain risks and may have profound consequences regarding the life of the patient. Therefore, the patient has the right to know which intervention is to be made in his or her body in detail and to decide to allow it or not based on self-determination. The right to self-determination is considered to be inherent in autonomy. Bioethics perception emphasizes that the remedy for situations where autonomy will be lost is providing more autonomy. The principle of extended autonomy needs to be implemented to ensure that patients express their desires and decisions for times when their decision-making ability is lost and to alleviate the psychosocial burdens on their relatives and health professionals. This study is designed to measure the knowledge and attitude of doctors and nurses on extended autonomy and advance directive (AD), which is intensively discussed in international literature.
The Principle of Extended Autonomy and the Current Situation of AD in the World
In the principle of extended autonomy, it is accepted that when a decision given at the time of the person’s decision-making ability is intact, then it is generally valid at the time he loses his or her decision-making capacity. In this case, the decision of the person is extended to cover the period in which there is no decision-making capacity. The moral principle that forms the basis for such an advance decision-making process is called the principle of extended autonomy (Veatch, 2003).
In the literature, the autonomy applied by individuals with AD is referred to as prospective autonomy (Cantor, 1993), future-oriented autonomy (Dresser, 1994), precedent autonomy (Dworkin, 1988), and extended autonomy (Quante, 2017; Veatch, 2003). The concept of extended autonomy that has emerged over the last 30 years is more of a negative freedom. Measures and principles have been developed to ensure or increase the freedoms of patients against the intervention of others. This understanding rejects the intervention which the doctor knows is the best one for the patient but instead, it predicts that each individual can position his or her life in the best possible way (Coggon & Miola, 2011). The principle of extended autonomy has found an application field with AD. AD generally includes information such as living will and durable power of attorney for health care.
Living will: It is defined as written documents, which are designed for individuals to express their choice of treatment (by decision-making or restriction on specific therapies) in order to use when they do not have the capacity to make decisions in the future (Doukas, 2013). Durable power of attorney for health care: Where the patient cannot make a decision on his or her own behalf, it determines who will act as the decision maker (Beauchamp & Childress, 2001; Doukas, 2013). In Germany, this concept is referred to as vorsorgevollmacht (Ünver & Kaya, 2017) and as vorsorgeauftrag in Switzerland (Yücel, 2018).
Although the origins of AD goes as back as the 1930s, there has been a significant development in the United States since 1990 when the law called the Patient Self-Determination Act (PSDA) was issued (Hunsaker & Mann, 2013). When the rate of AD use was examined in the American population between 2000 and 2010 for those aged 60 years and over, the rate of AD was found to be increased from 47% in 2000 to 72% in 2010 (Silveira, Kim, & Langa, 2010). In the United States, a survey on elderly people shows that 73% of the participants had AD and 28% did not share their directives with anyone (Inoue, Ihara, & Terrillion, 2017).
Some European countries such as Austria, Germany, and Switzerland have changed their laws and civil laws so that the patient can make life-ending decisions and give ADs. This shows that end-of-life decisions are accepted as a special subject for individual zone (Veshi & Neitzke, 2015). According to studies; in Germany, while only 10% of the population gave ADs in 2012 (Evans et al., 2012), this rate increased to 25% in the next few years (Leder et al., 2015); 64% of people who have a fatal disease in France have appointed health-care proxy and 6% of them have created ADs stating their life and health wishes (Trarieux-Signol et al., 2014); and 14% of the Australian population has ADs (White et al., 2014). In Canada, 76% of people who received long-term care had DNR (do-not-resuscitate; Perry & Lawand, 2017).
The Situation in Turkey
With respect to Turkey’s legislation, there are no regulations that directly mention ADs. However, according to the Regulation on Patient Rights, Article 24, “if a patient is not in a position to explain his/her request during medical intervention, his/her previous requests for medical intervention is taken into consideration,” is an article which can be interpreted as the enabler of AD. It is emphasized in the same article that “in recurrent diseases, where competence is lost from time to time, the patient may be asked to give informed consent for medical intervention for periods when he loses competency” which makes possible for people to create AD. Despite the support with legislation in Turkey, there is no clear provision and sufficient practice on the subject. The right to request refusal or cessation of treatment, which is one of the most mentioned subjects in the AD, is specified in Article 25 of the Regulation on Patient Rights. Organ and tissue transplant, one of the other information in the AD, has become legal with the Law on Organ and Tissue Transplantation. As per Article 14, where there is no organ or tissue transplantation information, the informed consent of the patient’s guardian is required, and this situation imposes heavy responsibility for the patient’s proxy. On the other hand, there are no special provisions for DNR in Turkish legislation. With the article 13 of the Regulation on Patient Rights, euthanasia is prohibited.
Method
Study Design and Sample
This is a quantitative descriptive study about the opinion and information of health professionals (doctors, assistant doctors, and nurses) in the city of Konya in Turkey, regarding to the extended autonomy, AD, and patient right. Doctors and nurses who are working in a hospital environment were included in this study because these professionals are more likely to deal with patients in severe and delicate clinical situations. This study addresses the following questions:
What are the attitudes and knowledge of health professionals about the principle of extended autonomy, AD, and patient autonomy? Do health professionals have a relationship between their title and their field of expertise, and on their perspective on the principle of extended autonomy and AD?
The research population consisted of health professionals working in two different medical faculty hospitals in the city. According to data from the Provincial Health Director in 2017, the total number of doctors and nurses working in the two study hospitals were 2,249. The minimum number of samples should be 328 for this study based on sample size calculation. Random sampling methods were applied for sample selection. In the study, data were collected from health professionals via face to face interview between September and December 2017. Total 372 data were collected for the study. The collected data were analyzed to determine socio-demographic characteristics of the participants and their awareness and attitudes towards both patient autonomy and principle of extended autonomy and AD.
Instrument
In this study, data were collected from the study participants by using a questionnaire. The questionnaire was prepared by the researchers using the relevant local and foreign literature. The questionnaire consisted of 47 questions. Moreover, 10 of these questions were about sociodemographic information of the participants, 22 of them were (5-point Likert-type scale 1 = strongly disagree, 5 = strongly agree) attitude questions, and 15 questions related to the knowledge level of health professionals about the studied context. Prior to the data collection, the questionnaire was pretested to assess its clarity, sequencing, and time needed to complete. The result of the pretest was used to improve the phrasing of questions in the questionnaire.
Ethical Considerations
To carry out the study, written permission was obtained from Necmettin Erbakan University Meram Faculty of Medicine, Drug and Non-Medical Research Ethics Committee. After receiving the Ethics permission, the study was approved by two medical hospital (Necmettin Erbakan University Meram Medical Faculty Hospital and Selcuk University Medical Faculty Hospital) managers.
Analyses
A descriptive and exploratory data analysis used such as frequency, percentage, average, and standard deviation. For the comparative analysis of the proportions of dichotomous variables (association between these variables), we applied the chi-squared (χ2) test of independence. The significance level for this test was set at p < .05. While calculating the relationship level of variables, Contingency Coefficient (c) was examined in r × r pcs tables and Cramer’s V value (φc) was examined in r × c pcs tables.
Results
Sample
In the study, 61.6% of the participants were women, 64.2% were married, and 52.4% were postgraduate degree holders. The mean age of the health professionals was 30.66 years (standard deviation (SD) = 9.11), and the average seniority was 8.29 years (SD = 7.66). In addition, 32.2% of the participants were assistants doctors, 15.9% of them were doctors, and 51.9% were nurses. Moreover, 52.5% of the health professionals work in medical sciences department, 41.9% in surgical sciences department, and 5.6% in basic sciences department.
Knowledge Scores
The knowledge questions focused on measuring the participants’ general knowledge of extended autonomy and ADs. When asked who should be the decision maker for the unconscious patient, majority selected the option of legal agent (34.8%) followed by his or her own doctor (29.8%), a commission of doctors (28.3%), and the rate of the AD was only 5%. More than half of the participants (62.1%) know that it is impossible for the unconscious patients to use their autonomy, 34.9% of the participants stated that it is possible for the patient to use his or her autonomy, and ADs can be taken in the period when the patient is in a conscious state. Considering how the participants evaluated the extension of the patient’s autonomy, approximately half (46.8%) supported it, 33.2% stated that it could be expanded in some cases, while 20% stated that the patient’s autonomy should not be extended. Moreover, 55.9% of the doctors, 71.4% of the assistant doctors, and 42.7% of the nurses who were evaluated showed poor levels of knowledge regarding AD.
Attitudes Toward Extended Autonomy and AD
Even if it was not included in the patient’s informed consent, one third of the doctors and nurses (34.6%) agreed in performing everything which is needed for the benefit of the patient (Table 1). More than three quarters (77.9%) of the participants stated that AD requires clear identification with legislation (Table 1). AD is a guideline for health care and more than three fifths of the respondents (65.1%) supported its issuance by anyone who is in a conscious state (Table 1). The majority of the participants (70.3%) supported the consideration of the previously announced wishes of unconscious patients during a medical intervention (Table 1). More than half of the participants (52.9%) agreed to the suggestion that the patient with a DNR directive should not be interfered with regard to his or her decision (Table 1). The suggestion asserting that since the patient will become a new person when he or she is unconscious, his or her previous instructions should not be followed, which is also an important issue of discussion in the creation of AD, did not get enough support from the participants (48%; Table 1).
Participation Status of Doctors and Nurses on Implementation of the Principle of Extended Autonomy in the Provision of Health Services and Distribution of Score Averages.
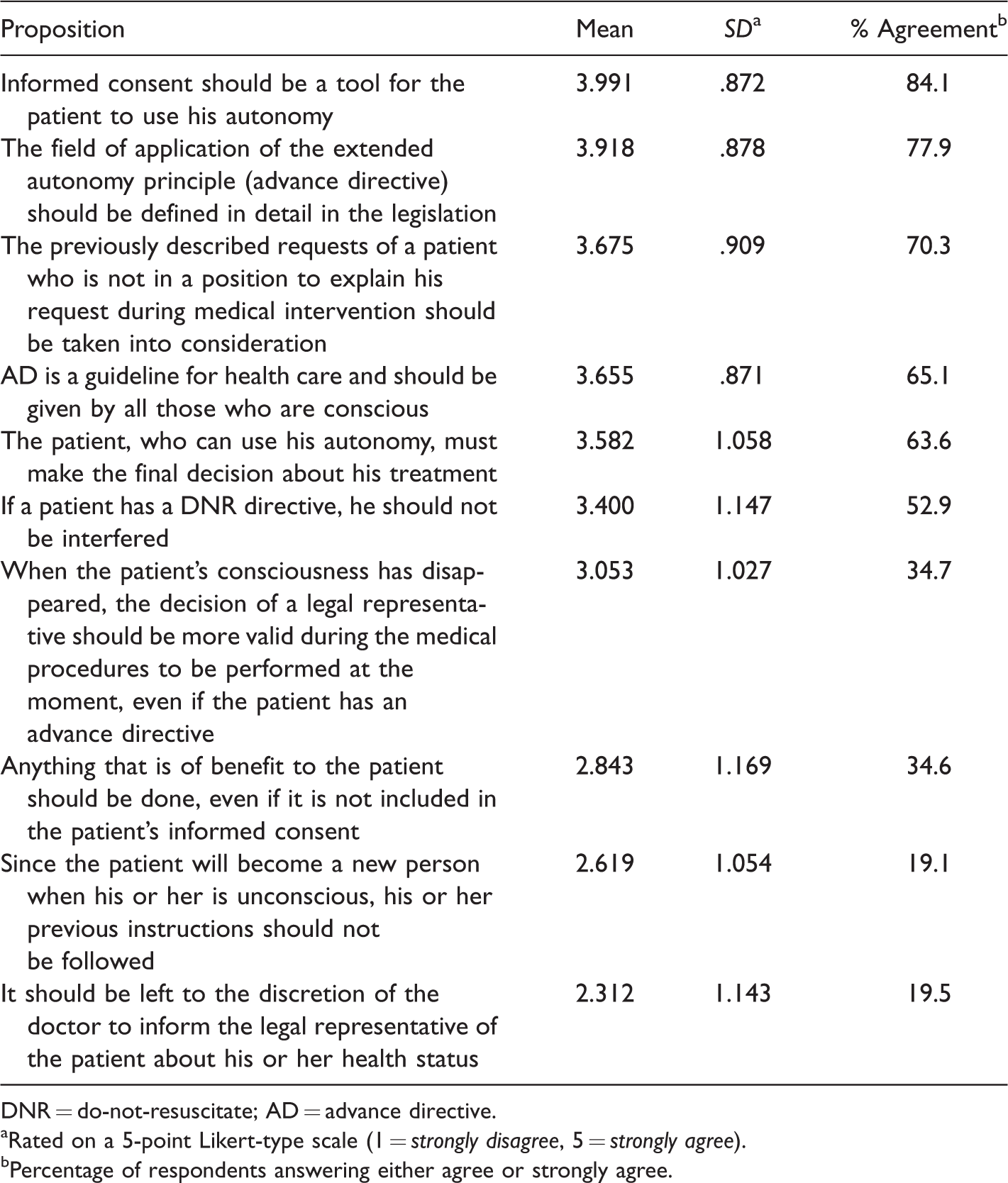
DNR = do-not-resuscitate; AD = advance directive.
aRated on a 5-point Likert-type scale (1 = strongly disagree, 5 = strongly agree).
bPercentage of respondents answering either agree or strongly agree.
Relationship Between Sample and Its Attitude
Chi-squared tests showed that a significant (p = .008) relationship (φc = .156) was found between the area of expertise of health professionals and the opinion related to using the unconscious patient’s autonomy (χ2 = 17.52). According to the study findings, nurses (50%) and medical sciences division doctors (30%) have the most paternalistic approach (Table 2). A significant (p = .002) relationship (φc = .171) was determined between the experience time of the participants and their knowledge of ADs whether it takes part in Turkish legislation (χ2 = 21.440). The notable proportion of highly experienced employees (32.1%) stated that AD is included in Turkish legislation (Table 3). A meaningful relationship was found between the training level of the participants and that AD requires clear identification with legislation (p = .000; χ2 = 32.485; φc = .211) and the consideration of the previously announced wishes of unconscious patients during a medical intervention (p = .004; χ2 = 21.440; φc = .174). As the level of education increased, participants were more likely to support AD.
Relationship Between the Specialization of the Doctors and Nurses and the Unconscious Patient’s Use of His or Her Autonomy Discussion.

aPearson Chi-Square.
bCramer’s V p < .05.
Relationship Between Doctors’ and Nurses’ Experience and Their Regulatory Information on Advance Directive.
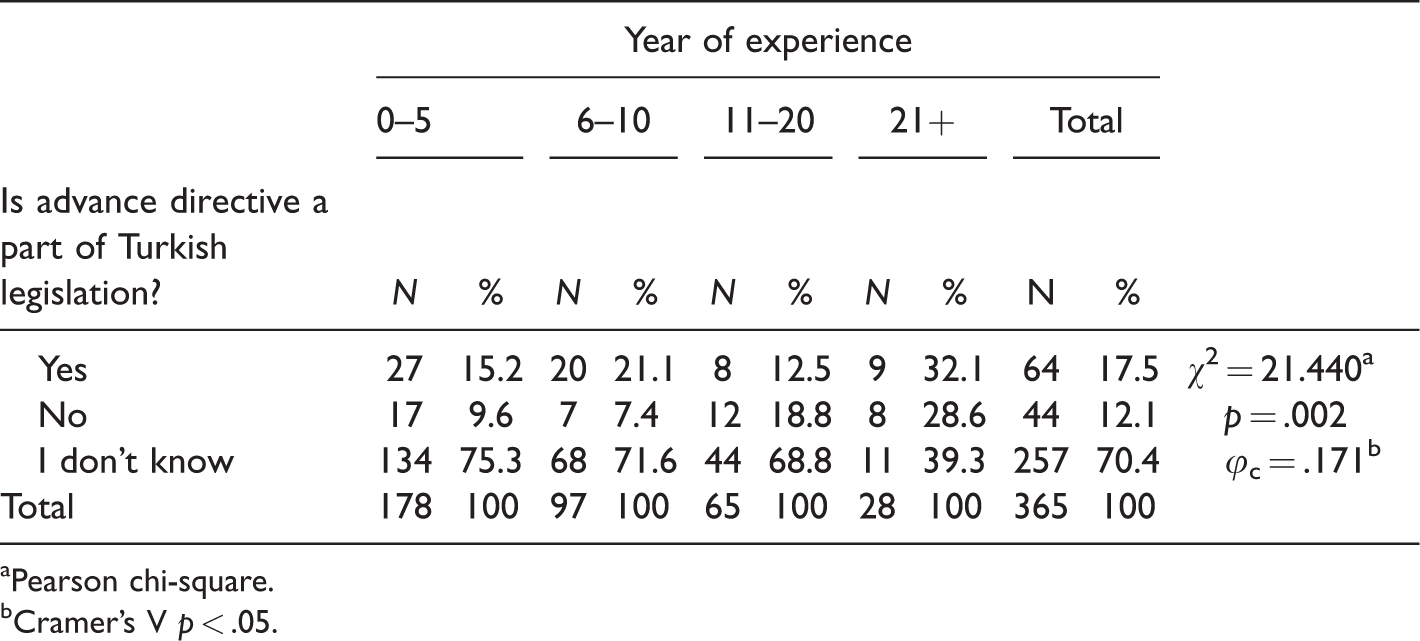
aPearson chi-square.
bCramer’s V p < .05.
In the research, the majority of the participants selected the legal agent option about who should be the decision maker for the unconscious patient, also AD selected least. In the study conducted in six European countries, 44% of the participants responded as “I express my wishes before I lose my ability to make decisions, for example, the living will” to the question of “who would you like to take health care decisions on behalf of you if you lose the capacity to make decisions had the following answers” (Daveson et al., 2013, p. 421). Compared to other European countries, family members in Turkey are more involved in the personal lives of each other. It is also a country where individuality and loneliness have recently increased.
For the implementation of AD, not only clinical applications but also an area suitable for cultural interpretation and adaptation needs to be defined. At the same time, AD is more general than “Who and for whom decisions?” This is an excellent case for testing a significant intercultural change (Biller-Andorno & Brauer, 2010). Turkey’s cultural structure is constantly changing. Moreover, 92.3% of the population live in big cities and 65% are nuclear families. Although 16% of the population live alone, the average household size is 3.4 (Türkiye İstatistik Kurumu, 2018). These rates indicate that the society becomes lonelier each year and that the elders will live alone or in a nursing home. In addition, people with chronic diseases can survive for a long time with the technological advances. This brings social and psychological problems for patients. All these show that the Turkey in the future will be needing the regulations and practices with regard to AD.
According to studies, 62.2% of health professionals in Brazil and 96.4% of nurses in Portugal were found to have no knowledge on AD (Antonio et al., 2015; Silva, Neves, & Silva, 2014). As a result, in the United States, oncology nurses have high AD knowledge (Jezewski & Feng, 2007). In Ohio, 95% to 99% of nurses were found to have correctly responded to AD (Lipson, Hausman, Higgins, & Burant, 2004). Our data indicate that more than half of the participants evaluated were to be found poor in terms of knowledge on AD. The results of our study were close to the countries that were not actively using this practice, despite the fact that AD was legal, and it was found to be different with the countries where the AD was used actively. The difference makes us think that the knowledge of AD increases when it is implemented.
In a study conducted in Canada, approximately 90% of doctors and in a study conducted in Japan, 55% of doctors reported that they would consider AD for the periods when patients lost their decision-making skills and supported the use of AD (Hughes & Singer, 1992; Masuda et al., 2003). Our data indicate that the majority of participants supported these propositions: The previously described requests of a patient who is not in a position to explain his or her request during medical intervention should be taken into consideration; AD is a guide application and should be given by anyone who is conscious.
In the United States, the rate of generating AD is slightly higher than in other countries; this may be due to earlier implementation, compared to other countries, as well as the provision of trainings on AD to the American public. Even if AD becomes legal, it requires a certain process to implement it parallel to culture and society’s values. Therefore, the rate of implementation may not rise immediately in every country which has laws and regulations on the matter.
Nurses who had more than 21 years of professional experience reported greater knowledge of AD (Coffey et al., 2016). In Brazil, no significant difference was observed between the groups, and most of the health professionals (82.1%) were not aware of the legal regulations related to AD in Brazil (Antonio et al., 2015). In a study conducted in France, most doctors and nurses (60%) reported that they were not familiar with the legal framework related to AD (Ledoux et al., 2013). When compared with other countries, it was found that nurses in the United States had more knowledge and experience of AD (Coffey et al., 2016).
In our findings, significant relationship was determined between the experience time of participants and their knowledge of ADs whether it takes part in Turkish legislation or not. The majority of the respondents have no information as to whether Turkey’s legislation in AD. It was determined that the participants who have 21 years or more experience have more information. In Turkey, it is clear that legal regulations should be made in the context of AD.
As a central component of the life-sustaining treatments often addressed in AD, decisions about DNR orders are an important consideration in end-of-life treatment preferences (Triplett, Black, Phillips, Schwartz, & Anderson, 2008). Our data indicate that more than half of the participants agree upon the suggestion that the patient with a DNR directive should not be interfered. The high level of responses of the participants not to intervene in the patient with the DNR orders reveals that the health-care professionals are looking positively at extending patient autonomy. Nearly half of the doctors do not know whether it is legal in Turkey of DNR orders (Kuvaki et al., 2014). In addition, almost half of the doctors stated that DNR instruction was given in the clinic and a significant part of them had given DNR instructions (Gül, Kucuza, & Yalım, 2016). For instance, in Canada, 76% of people who received long-term care had DNR (Perry & Lawand, 2017).
Conclusion
This study elucidated the knowledge and attitude of doctors and nurses on extended autonomy and AD. It has been found that doctors and nurses support extended autonomy. However, it is seen that there is a lack of knowledge on how to put AD into practice. The fact that AD is not known by the majority of the participants reveals that it is necessary to take faster steps on this issue. It may be useful to organize different scientific activities across the country in order to increase awareness and knowledge on AD. In the legislation, the dilemmas that support both patient autonomy and paternalist approach are reflected in the behavior of health professionals. Article 19 of Regulation on Patient Rights and similar regulations strengthen the paternalistic approach of health-care professionals. These regulations can be revised with respect to patient autonomy. Researches should be done on the cultural structure and expectations of the Turkish society, and how this situation is regarded among the public should be determined. AD can be included in the legal system in more detail, and a law on this issue should be enacted.
Summary
There are no clear regulations and practices on extended autonomy and advanced directive in Turkey. According to our results, 77.9% of Turkish doctors and nurses think that the law should clearly define them.
Footnotes
Authors’ Note
This article was developed from the master thesis titled “The principle of extended autonomy in health services from the point of doctors and nurses: A field research”. The thesis was approved by Necmettin Erbakan University, Institute of Health Sciences in June 2018.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.