
Abstract
Social expectations influence how we cope with loss and how people in our social networks respond to us. Wortman and Silver outlined Western cultural assumptions, or myths, about mourning, thought to influence judgments of one’s grief response. In particular, the two myths hypothesized to affect social judgments about grievers’ adjustment were related to (a) the intensities of the grief response and (b) the duration of the grief response. We assessed if these myths affected the attributions of potential support providers in a convenience sample of 510 Amazon Mechanical Turk community participants. The results indicated preheld expectancies that expressing and processing loss is important to recover from grief was related to attributions about the adjustment of spousally bereaved grievers in vignettes. However, any level of grief symptoms displayed in vignettes was associated with participants, indicating they would discourage expression of grief and distance themselves from the person grieving.
Keywords
Testing the Myths of Coping With Loss on Social Judgments of Grievers
“Am I coping correctly?” The loss of a loved one can elicit not only the experience of grief but also self-judgments and judgments from others about the appropriateness of one’s grief response. These judgments are hypothesized to be influenced by Western cultural “myths of coping with loss,” the common social expectations about the appropriate way to mourn. In an influential article, Wortman and Silver (1989) summarized factors influencing social and self-attributions about the grief process, the myths of coping with loss, which were derived from folk beliefs, bereavement theories, and cultural mores that are common to Western society. These coping myths have been hypothesized to have become a sort of standard against which social attributions about the appropriate course of mourning is based, yet this hypothesis has not been tested empirically despite the fact that these coping myths are largely contradicted by the empirical findings on grief. These coping myths or societal expectations are important to study, given the effect they may have on social exchanges in the context of bereavement and the adjustment of those who have experienced loss of a loved one.
Key Factors Comprising the Myths of Coping With Loss
Severity of Grief Expression
The central feature of the coping myths described by Wortman and Silver is the expectation that grievers should exhibit distress after a loss to “process” the loss and recover from it. Otherwise, if the person does not complete the “requirement of mourning” by engaging in the necessary “grief work” (active mourning, displays of distress, and working through the emotions associated with grief) as theorized originally in psychoanalytic theory, catharsis would not occur, and the person would remain attached to the lost “object” rather than reengaging with their environment. The ongoing, unconscious cathexis in the lost object would be associated with the escalating use of defense mechanisms and ultimately delayed grief reactions (Bowlby, 1980; Freud,1917/1957).
While the details of psychanalytic theories of grief have not been adopted by Western society as a whole, the premise that grief work is necessary for the resolution of grief has persisted (e.g., Middleton, Raphael, Martinek, & Misso, 1993). Failure to express grief can cause the griever to be judged as callous, self-centered, or unable to attach to others: Violating social norms and expectations after a loss such as expressing positive emotions or engaging in self-enhancement led to an increase in negative attributions from independent raters and worse social adjustment ratings from social supporters (Bonanno, Field, Kovacevic, & Kaltman, 2002). In a qualitative study, community participants reported a belief in stage theories of grief, with the need to express one’s grief and not avoid “grief work” (Costa, Hall, & Stewart, 2007). In addition, participants rating reactions to grievers in vignettes were more likely to ascribe negative qualities and desire social distance from grievers expressing higher grief severity, despite the type or characteristic of the loss (Eisma, 2018; Eisma, te Riele, Overgaauw, & Doering, 2019) However, prospective studies of grief recovery trajectories suggest that showing minimal distress, displaying positive emotion, and experiencing a quick recovery toward preloss functioning were the most common grief trajectory and linked to better health outcomes (e.g., Bonanno, Moskowitz, Papa, & Folkman, 2005; Bonanno, Wortman, & Nesse, 2004; Stein, Folkman, Trabasso, & Richards, 1997).
Time Since Death
An extension of the aforementioned myth also discussed in detail by Wortman and Silver is that working through loss by engaging in grief work is expected to facilitate recovery. The time period in which the expression and resolution of grief might occur is less well defined in this framework. A number of time frames have been proposed through the years when attempting to define the border between normal and abnormal grief, ranging from 14 months (Horowitz et al., 1997), 12 months in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition-proposed criteria for persistent complex bereavement disorder, and 6 months for the International Classification of Diseases 11th Revision criteria for prolonged grief disorder (PGD). The implication being that shorter periods of grieving are normative, but longer periods are associated with pathology. In an international sample using vignettes, grief was expected to occur early in the loss (2 weeks) and then decrease relatively quickly (6 months), with significant differences in grief expectations soon after a loss compared with 15 months after a loss; however, social distance preferences did not change based on length of time since death (Penman, Breen, Hewitt, & Prigerson, 2014). These findings were supported both in an Australian community sample, which found expectations that grief should be expressed not avoided, social support is important for recovery (despite evidence that support relationships often deteriorate after a loss, e.g., Breen & O’Connor, 2011), and grieving too long is maladaptive (Costa et al., 2007), and in a vignette study with college students, where grievers expressing positive emotion 1 month after the loss were rated negatively and 1 year after the loss were rated as having inappropriate negative emotions (Miller, 2015). Research suggests that intense grief reactions that last more than 6 months tend to persist (e.g., Bonanno et al., 2004; Simon et al., 2011). Generally, in society at large, it is unclear whether there are specific societal expectations for how long might be too long to grieve a loved one.
Gender of the Person Bereaved
Gender of the griever may also impact social judgments of the grief response. If a female does not express grief or a male does, they might be judged negatively for violating expectations of gender roles (Kubitz, Thornton, & Robertson, 1989). However, studies in bereavement, which have historically oversampled older widowed women, suggest that men may be more impacted by losing a spouse (see M. S. Stroebe, 1994; M. S. Stroebe, Hansson, Stroebe, & Schut, 2001; Stroebe, Schut, & Stroebe, 2007; Versalle & McDowell, 2005). Differences in coping styles may interact with social expectations (Nolen-Hoeksema, Parker, & Larson, 1994; M. Stroebe, 2001). Men may be more inexpressive, grieve more through action-oriented coping (Golden, 1996; Stillion & McDowell, 2001–2002), and focus more on secondary stressors related to the loss than women (Bennett, Gibbons, & MacKenzie-Smith, 2010). Women are more likely to use emotion-focused coping (Bennett et al., 2010) and may be judged as interpersonally attractive if high-intensity grief is expressed after the death of a loved one (Kubitz et al., 1989). Despite studies indicating gender differences in grief expression and coping after a loss, recent studies have found that social expectancies for male and female grievers are the same (Miller, 2015; Penman et al., 2014). However, raters indicated that they would be more likely to interact with a bereaved woman regardless of type of death (stroke or car crash) than a bereaved man (Penman et al., 2014).
The Significance of Social Attributions for Those Bereaved
The myths of coping with loss describe cultural assumptions about the mourning process. However, stage theories of grief, the requirements of mourning, grief work, and delayed grief are incongruent with empirical evidence (see M. Stroebe, Schut, & Boerner, 2017). Yet, these myths still pervade cultural expectations. For instance, despite Elizabeth Kübler-Ross herself recanting her five stages of grief model (Kübler-Ross,1969/2003; Kübler-Ross & Kessler, 2014) as inaccurate, it is well known in popular culture and even still cited in textbooks in the medical fields (Corr, 2018; Holman, Perisho, Edwards, & Mlakar, 2010). The persistence of these grief theories on influencing the broader culture leads people to make inaccurate attributions of grief responses that can have negative implications for the postloss recovery of grievers.
When we are stressed, we are more likely to reach out to others for support. This support provides a sense of self-efficacy and control over one’s environment, buffering the impact of stress (e.g., Bowen et al., 2014; Mehl & Pennebaker, 2003). The protective function of social support is important after a loved one dies, due to the increased risk of physical illness and morbidity after a loss (see Burke & Neimeyer, 2013 for a review), both for those who lost a spouse generally and for those who develop pathological grief reactions (Ghesquiere et al., 2012; Schultze-Florey et al., 2012; Vitlic, Lord, Carroll, & Phillips, 2015; Zisook et al., 2014). Adaptive engagement with potential support providers can allow space for the bereaved to process feelings and thoughts about the loss, encouraging exploration of current and future self-conceptions that have been disturbed because of the loss (Keller & Nesse, 2006; Thoits, 1995). Negative social feedback has been related to experiencing distress (Eisenberger, Lieberman, & Williams, 2003), and responses to negative social reactions are met with avoidant coping and increased self-blame reactions (e.g., Ullman, Filipas, Townsend, & Starzynski, 2007).
If, soon after their loss, someone grieving a loss finds social interactions addressing their grief to be negative, constrained, or unhelpful, this constraint can be interpreted as feedback from others that coping is inappropriate, reflected in a griever’s self-appraisals which question core self-concepts (Thoits, 1986). Negative social feedback can cause the bereaved to question meaningful aspects of identity: “What’s wrong with me,” “Am I coping poorly,” or “Who am I?” Social stressors and other socially related contextual factors can lead to and maintain psychopathology (Gore & Cross, 2014; Holahan, Moos, Holahan, & Brennan, 1997). However, adaptive engagement with potential support providers can encourage exploration of current and future self-conceptions that have been disturbed because of the loss (e.g., Bonanno & Kaltman, 1999; Lepore, 2001; Thoits, 1995). This process of identity exploration can result in grief resolution and a relatively quick return to preloss functioning, or it can lead to identity disturbance and problematic grief reactions (e.g., Papa & Lancaster, 2016).
Support providers want to help but erroneously think that helping means presenting a cheerful/optimistic façade. This creates a conflict between feeling anxious to interact yet wanting to present a happy front—causing ambivalence and anxiety over interacting with the griever. Anxiety on the part of the social support provider can also leave the griever feeling constrained. Helgeson and Cohen’s (1996) review suggested that support providers sometimes think that discussing the death is bad for the bereaved—it upsets the support provider as well. Reassurance (“I know how you feel”) may help the provider feel dutiful for providing support but may be perceived by the griever as condescending or minimizing the problem (Lehman, Ellard, & Wortman, 1986; Wortman & Dunkel-Schetter, 1979). Constrained social support is purported to make exposure to loss-related stimuli even more distressing. It may also inhibit making sense of the loss and interferes with getting help with coping strategies that might be effective (Lepore, Silver, Wortman, & Wayment, 1996). Those experiencing social constraints reported more stress and worse health (Juth, Smyth, Carey, & Lepore, 2015; Lepore & Revenson, 2007). Messages received from the social environment can result in physical and psychological implications for those grieving.
The Current Study
The purpose of the current study is to examine the extent that individuals subscribe to the belief that “grief work” is necessary to the resolution of grief and the time frame that resolution might be expected to occur. These expectancies were examined to explore whether they affect how participants in the study made judgments of how someone bereaved is coping with their loss and how much social discomfort they would feel interacting as potential social support providers for people who were spousally bereaved. Social response for grievers was a main outcome for the current study, measured by how likely potential support providers would be to discourage displays of distress, force cheerfulness, or use platitudes. In addition, a decreased willingness to interact and desire for social distance was also included, conceptualized as a negative social response that results in social cognitive processing for the griever, which can impact bereavement outcomes, measuring how likely participants would be to interact socially with the griever, through avoidance or exclusion from social activities. Further, gender was examined to explore if the gender of the person expressing grief would affect these relationships.
Considering that the “myths” of coping with loss conflict with empirical evidence, this was a test of whether potential support providers use the myths of coping with loss (Wortman & Silver, 1989) in their attributions about people coping with grief. Using near-identical vignettes varied on (a) the level of grief symptom severity expression in the vignettes (no severity, low severity, high severity); (b) the stage in the coping process (time since death: 2 months vs. 2 years); and finally, (c) the gender of the griever (female or male) to test hypotheses about coping based on gender stereotypic responses. These factors plus preexisting beliefs based on psychoanalytic, attachment, and stage theories about the need for grief work and the length of time it takes for grief to resolve were assessed to identify whether they would affect ratings of coping/adjustment of the griever in the vignettes and how much social discomfort they engender.
A number of hypotheses were identified which contradict empirical evidence but are concordant with cultural expectations about coping with loss. First, it was hypothesized that (1a) increases in endorsement of the need to engage in grief work would be associated with increases in ratings of how well the grievers in the vignettes are coping/adjusted as they would tend to normalize displays of distress during grief, and (1b) higher grief work expectancies would be associated with decreased social discomfort as any distress would be viewed as normal. Second, it was hypothesized that (2a) increases in ratings of the acceptable duration of mourning would be associated with increases in ratings of coping/adjustment as distress from grieving would be normalized across the time since death presented in the vignettes and (2b) also decreases in social discomfort ratings as any distress would be viewed as normal. Finally, it was hypothesized that expression of grief by female vignette characters would be viewed as more normative and thus associated with increased coping/adjustment ratings (3a) and lower social discomfort (3b).
Method
Design
This was a 3 × 2 × 2, between-subjects study manipulating three variables through the use of vignettes: severity of grief symptoms (High, Low, No Severity); gender (Female, Male); and length of time since death (Short = 2 months; Long = 2 years). This required that 12 vignettes be constructed to evaluate all combinations of factors, one of which was randomly assigned to each participant. With 12 study cells, a priori power estimations suggested a sample size of N = 414 with medium effect sizes, oversampling to N = 510 to ensure an adequate number of subjects per cell, given the random assignment strategy.
Participants and Procedures
Five hundred and ten (N = 510) U.S. adult workers from Amazon’s Mechanical Turk (MTurk) website participated. Out of those, 116 out of the 510 participants reported that they had experienced bereavement in their life. Inclusion criteria were (a) English proficiency, (b) 18+ years old, and (c) U.S. residence. The survey took approximately 20 to 30 minutes to complete. Participants were paid 50 cents per survey. This study was fully approved by the University of Nevada, Reno institutional review board. The mean age of participants in our sample was 33 (SD = 11.53); percentage of females was 46.1% (SD = .51); 44.3% had a 4-year college degree or higher (SD = 1.6); and average income was $48, 225 (SD = $37,113 l). This is in line with other studies that found that MTurk workers tend to be slightly younger and more educated in similar comparisons with the United States (e.g., Papa, Lancaster, & Kahler, 2014). The MTurk sample, though a convenience sample, was used due to availability and because research has demonstrated MTurk samples perform similarly or better than other samples on internal, convergent, and test–retest reliability and are comparable with in-person behavioral experiments (e.g., Casler, Bickel, & Hackett, 2013; Kees, Berry, Burton, & Sheehan, 2017; Peer et al., 2017; Shapiro, Chandler, & Mueller, 2013). Using the MTurk sample allowed for a more equivalent distribution of males and females than other similar vignette studies (e.g., Eisma, 2018; Penman et al., 2014) and is equivalent in terms of higher education and younger ages to other studies (e.g., Logan, Thornton, Kane, & Breen, 2018). In terms of ethnicity, 77.5% identified as White, 8% as Asian, 8.6% as Black, 6.6% as Hispanic/Latino, 2.0% as Native Hawaiian/Native American, and 1.2% as Other.
Measures
Expectations of the grief response
Before participants read vignettes, they answered basic demographic questions (age, ethnicity, gender, income, and education level) in addition to their preperceptions about how one should cope with loss on the nine-item Grief Expectations Questionnaire created by the second and fourth authors to assess expectations of grieving based on social-cultural expectations of grieving and measure initial expectations about how one should cope with loss, based on Wortman and Silver’s, 1989 article, Myths of Coping with Loss. Participants rated seven items assessing perceptions of whether processing the emotions related to loss is required to resolve grief on a 7-point scale ranging from strongly disagree to strongly agree. Representative items are as follows: “It is necessary to mourn the death of a loved one to recover from it”; “If someone does not grieve intensely, it will come back to haunt them later”; and “If someone doesn’t express grief after the loss of a loved one, they are in denial.” Reliability of the items averaged for this Grief Work Expectancies scale were high with an alpha of α = .86. In addition, Grief Length Expectancies were assessed by ratings of “How quickly do you think someone should be able to move on after a loss of someone they love?” from 1 (immediately), 2 (within a month), 3 (within 6 months), 4 (within 1 year), 5 (within 2 years), 6 (within 5 years), and 7 (never).
Covariates
Those who have experienced loss previously may be more understanding of others grief responses, as are women (vs. men), and those who are older and more experienced with grief (e.g., Papa et al., 2014). In addition, emotional disruption may have influenced ratings. Psychopathology screens were collected from participants after they rated their perceptions of the griever. These included depressive symptoms measured by the Patient Health Questionnaire-9 (Kroenke, Spitzer, & Williams, 2001), a widely used, brief diagnostic screen of symptoms of a depressive episode with good psychometrics (α = .92). Anxiety symptoms measured by the Generalized Anxiety Disorder 7-item (GAD-7) scale is a common, seven-item measure of anxiety symptom severity (α = .92; Spitzer, Kroenke, Williams, & Lowe, 2006). Finally, posttraumatic stress symptoms were measured using the primary care posttraumatic stress disorder (PTSD) screen, a four-item Yes/No scale measured the presence of PTSD symptoms (α = .83; Prins et al., 2003).
Vignettes
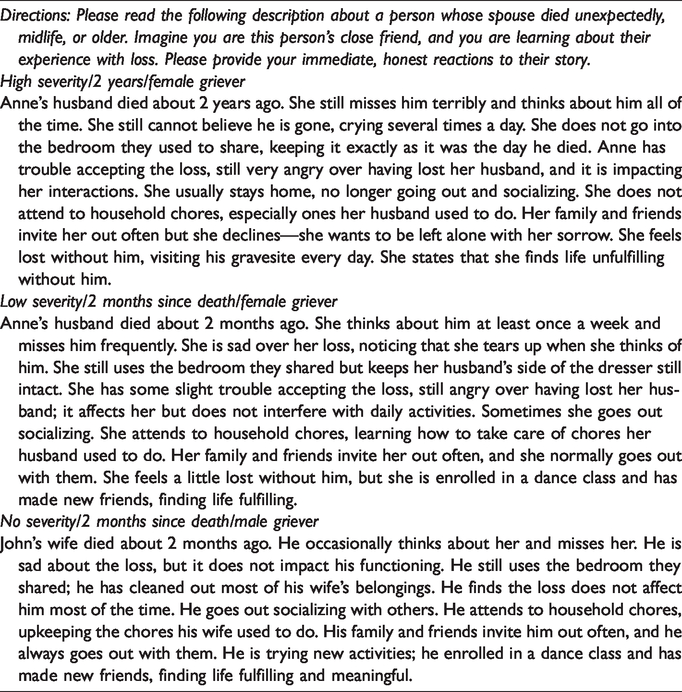
Participants were randomly assigned one vignette to read and then rated perceptions of the griever’s coping. Instructions read: “Please read the following description about a person whose spouse died unexpectedly, in midlife. Imagine you are this person’s close friend, and you are learning about their experience with loss. Please provide your immediate, honest reactions to their story.” Their perceptions of coping were rated via a 7-point Likert scale. Participants rated the griever in a vignette on three levels of grief expression severity: (a) high grief severity symptoms, (b) low grief severity symptoms, and (c) no grief severity symptoms expressed. Severity levels in vignettes were based on PGD criteria (Prigerson, Vanderwerker, & Maciejewski, 2008), including one symptom of separation distress and three cognitive, emotional, and behavioral symptoms (see Table 1 for vignette examples). Gender of the griever (e.g., Anne or John) and time since death (e.g., 2 months and 2 years ago) were manipulated in each vignette, totaling 12 vignettes, with 1 vignette randomly assigned to each participant to make attributions as a potential social support provider. Total number of participants assigned to each vignette ranged from 29 to 51 (5.7%–10.0%). Out of the N = 117 (23%) participants who reported experiencing recent loss, 4 to 15 (3.4%–12.0%) were randomly assigned to each vignette, with no significant differences in the number of previously bereaved participants across the 12 vignette scenarios (chi-squared = 9.26, p = .60).
Example of Vignettes With One Example of Each Level Manipulated in the 3 (Levels of Severity) × 2 (Time Since Death) × 2 (Gender of the Person Grieving).
Outcome variables
After reading the vignette, participants answered questions regarding judgments that the griever’s coping was ineffective and the griever’s loss reaction as inappropriate or abnormal, as well as the likelihood to discourage the griever’s displays of distress and willingness to interact with the griever (see Wortman & Boerner, 2011). Items were divided into two subscales.
The seven-item perceived coping/adjustment (PC/A) subscale consisted of times assessing “How well is this person coping with the loss,” “How affected by the death is this person,” “To what extent is this person recovered from the loved one’s death,” “How is this person’s grieving likely to impact them negatively in the future,” “This person needs to move on,” “This person is hiding their true distress,” and “This person’s loss reaction is abnormal or inappropriate.” Items were rated from 1 (not at all) to 7 (extremely). Reliability was good (α = .75). Higher scores indicate that the participant rated the griever as coping poorly.
The six-item Social Discomfort (SD) subscale consisted of ratings of how much participants would: “Feel worried that I would inadvertently say or do something inappropriate that would cause this person distress,” “Avoid this person or avoid interaction with him/her,” “Involve this person in social activities,” “Change the subject (to something more positive) when this person starts talking about the loss,” “Discourage displays of sadness/distress,” and “Find interacting with this person will be stressful and/or anxiety provoking, difficult, or uncomfortable.” Items were again rated from 1 (not at all) to 7 (extremely), and reliability was adequate (α = .69). Higher scores indicate higher social discomfort.
Results
Analysis Plan
First, potential covariates were examined to assess unacceptable collinearity and relatedness to the two outcomes, ratings of PC/A and SD after reading the vignettes. The list of potential covariates included history of loss of a loved one (0 = no, 1 = yes); gender (0 = female, 1 = male); age; depressive symptoms; anxiety symptoms; and posttraumatic stress symptoms. Assessing collinearity was done by examining a correlation table of the covariates. To examine relatedness to the two outcomes, all potential covariates were entered into a liner regression for each outcome to select which would be used to build the final model. The decision to screen covariates in this way was done to preserve power by reducing the number of predictors in our regression models.
Second, the appropriate covariates were entered into a multiple linear regression on step one in a model building approach. The second step of the model included prevignette Need for Processing, Appropriate Grief Severity, and Appropriate Grieving Time expectancy ratings. Entered in third step of the model were the manipulated aspects of the vignettes. This included gender of the griever (0 = female, 1 = males); time since death (0 = 2 months, 1 = 2 years); and severity of grief coded into two dummy codes with No Severity as the reference and Low and High Severity as comparison conditions in each dummy code.
It should be noted that gender of the person presented in the vignettes did not predict either outcome in any model or affect any other relationship in the models disproving our hypotheses regarding gender roles. Given the large number of predictors in our analyses, we subsequently dropped it from the analyses to preserve predictive power.
In the last step, the interactions between prevignette expectancies and related vignette conditions were entered. Specifically, the interaction between prevignette expectancies were examined about the appropriate amount of time to grieve and the length of time since the death in vignettes, as well as the prevignette severity expectancies and the severity presented in the vignettes. Time since death and severity of symptoms presented in the vignettes were also assessed to see if they affected social ratings separate from expectancies.
Multiple regression assumptions were assessed through examination of residuals and multicollinearity indices. All models met assumptions for multiple regression modeling. Outliers were identified as having undue influence on results after examining leverage and discrepancy indicators and were excluded from the analysis. R version 3.5.0 with RStudio Version 1.1.447 was used to complete all analyses.
Selection of Covariates
Correlations of covariates indicated that depression and anxiety measures were correlated at .80 (p < .001; Table 2). Given this level of overlap, depression was dropped from the subsequent analysis as anxiety seemed to be more relevant to discomfort at interacting with recently bereaved. Subsequent examination of multicollinearity indices in regression models confirmed this level of association distorted results.
Means, Standard Deviations, and Correlations of Potential Covariates.

Note. M and SD are used to represent mean and standard deviation, respectively. PC/A= perceived coping/adjustment; SD = social discomfort.
*p < .05. **p < .01.
The regression model examining the covariates against PC/A subscale was not significant R2 = .01, F(7, 484) = 1.12, p > .10. However, given that Age was marginally correlated with PC/A (r = .08, p = .07), it was included in subsequent analysis just to be conservative. Not surprisingly, it was a different picture for the SD subscale. The model was significant, R2 = .06, F(7, 483) = 4.36, p < .001. Participant gender (b = 1.88, p < .001) and anxiety (b = 0.96, p < .05) were significantly relate to SD. Age (b = –0.04, p = .08) and bereavement status (0 = no, 1 = yes; b = –0.04, p = .08) were marginally associated. All four variables were retained in the analyses. Income, majority versus nonmajority culture, and PTSD symptoms were all nonsignificant (p values > .10) and not retained.
Hypothesis Testing
Perceived coping/adjustment
Expectancies for grief
In looking at predictors of the PC/A scale, addition of the expectancy ratings explained a significant proportion of the variance in the PC/A scale, R2 chang e = .02, Fchange(2, 499) = 3.04, p < .05, above and beyond the covariates, suggesting that adherence to myths about grieving does impact how participants judge grievers’ coping/adjustment. Increases in Grief Length Expectancies were associated with decreases in the PC/A scale (b = –0.31, p < .05), while increases in Grief Work Expectancies were not associated with increases in PC/A ratings, (b = 0.05, p > .05).
Grief characteristics
Characteristics of grieving also impacted how participants judged grievers, R2 chang e = .09, Fchange(3, 496) = 17.91, p < .001. Assessing the effects of severity of grief in the vignettes, severity of the loss was a significant addition to the model, F(2, 497) = 26.23, p < .001. Each of the dummy codes (No vs. Low Grief Severity, b = 3.33, p < .001; and No Versus High Severity, b = 3.21, p < .001) was significant, with any level of grief associated with high ratings coping/adjustment versus no grief. Time since the death (2 months vs. 2 years) was not associated with any change in PC/A ratings (b = –0.29, p > .05).
Interaction of expectations about grief and characteristics of grieving
Adding the interactions between prevignette expectancies and related vignette conditions (Grief Work Expectancies × Vignette Severity, Grief Length Expectancies × Vignette Time Since Death) and time and severity of symptoms (Vignette Severity × Vignette Time Since Death) was a significant addition to the model, R2 chang e = .04, Fchange(3, 496) = 4.89, p < .001 (Table 3). Results indicated that the interaction of Grief Length Expectancies and Vignette Time Since Death was not significant (b = 0.18, p > .05).
Final Step of Regression Results Using PC/A and SD Ratings as the Criterion Variables.
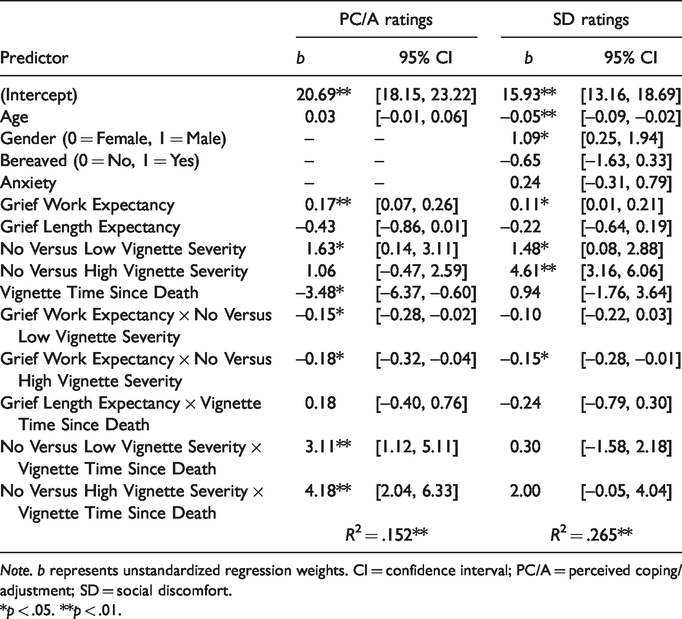
Note. b represents unstandardized regression weights. CI = confidence interval; PC/A = perceived coping/adjustment; SD = social discomfort.
*p < .05. **p < .01.
Regression Model of Perceived Coping/Adjustment Dependent Variable.
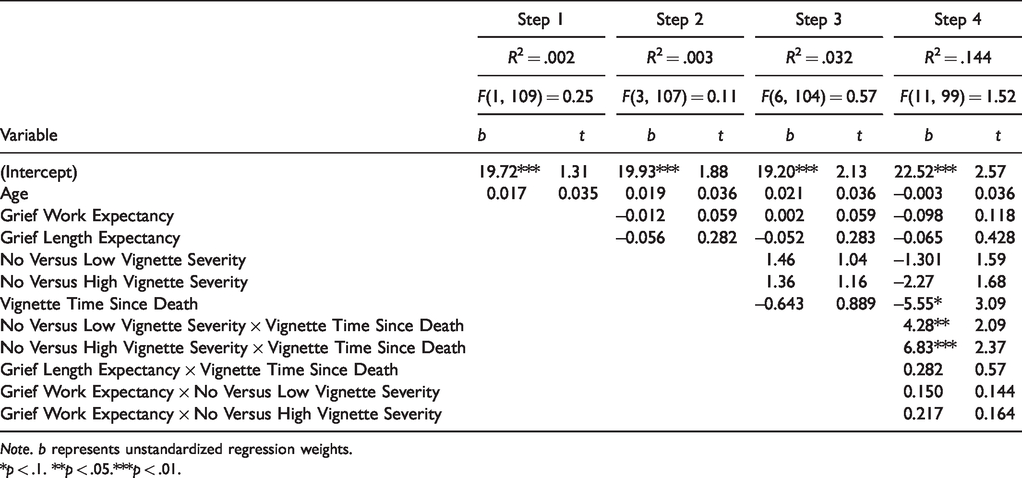
Note. b represents unstandardized regression weights.
*p < .1. **p < .05.***p < .01.
Regression Model of Social Discomfort Dependent Variable.
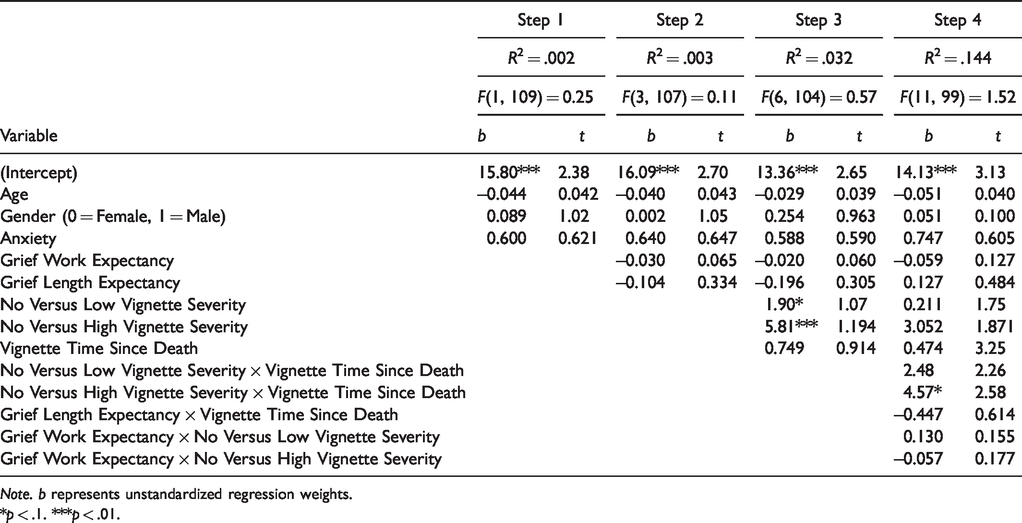
Note. b represents unstandardized regression weights.
*p < .1. ***p < .01.
The dummy-coded interaction of Grief Work Expectancies × Vignette Severity was significant, F(1, 495) = 3.79, p < .05 (Figure 1). Looking at the individual interactions, both Grief Work Expectancies × No Versus Low Grief Severity (b = –0.15, p < .05) and Grief Work Expectancies × No Versus High Severity (b = –0.18, p < .05) were significant. Simple slope analysis indicated that the simple slope of the No Grief vignettes was significantly different than zero going from the mean ±1 SD for Grief Work Expectancies (b = 0.17, p < .001), with PC/A ratings increasing as Grief Work Expectancies increased in the No Grief vignettes. The simple slopes for Low Grief Severity (b = 0.02, p > .05) and High Severity (b = –0.01, p > .05) indicated PC/A ratings were consistently high regardless of preexisting expectancies about the need for grief work (Table 4).

Interactions using PC/A ratings as criterion.
The dummy-coded interaction of Vignette Severity × Vignette Time Since Death was also significant, F(2, 494) = 8.15, p < .001 (Figure 1). Looking at the individual interactions, No Versus Low Grief Severity × Vignette Time Since Death (b = 3.05, p < .01) and No Versus High Severity × Vignette Time Since Death (b = 4.19, p < .001) were both significant. Simple slope analysis indicated that the simple slope of the No Grief vignettes was significantly different than zero going from 2 months to 2 years since the death in the vignettes (b = –3.49, p < .05), with PC/A ratings decreasing as length of time in the vignette was increased. Again, the simple slopes for Low Grief Severity (b = –0.37, p > .05) and High Severity (b = 0.70, p > .05) indicated PC/A ratings were consistently high regardless of time since death.
Social discomfort
Expectancies for grief
Adherence to myths about grieving impacts how participants judge grievers’ coping/adjustment. Looking at predictors of the SD scale, addition of the expectancy ratings explained a marginal increase in the proportion of the variance in the SD scale, R2 chang e = .01, Fchange(2, 490) = 2.36, p = .09, above and beyond the covariates. Increases in Grief Work Expectancies were not associated with increases in SD ratings (b = 0.00, p > . 05). Increases in Grief Length Expectancies were marginally associated with decreases in the SD scale (b = –0.30, p = . 06).
Grief characteristics
The characteristics of grieving presented in the vignettes impacted how participants judged grievers, R2 chang e = .20, Fchange(3, 487) = 42.76, p < .001. Assessing the effects of severity of grief in the vignettes, severity of the loss was a significant addition to the model, F(2, 488) = 62.91, p < .001. Each of the dummy codes (No vs. Low Grief Severity, b = 1.60, p < .001; and No vs. High Severity, b = 5.66, p < .001) was significant, with demonstration of any grief symptoms associated with higher ratings of social discomfort. The increase in time since the death (2 months vs. 2 years) was not associated with an increase in SD ratings (b = 0.62, p > .05; Table 5).
Interaction of expectations about grief and characteristics of grieving
Adding the interactions between prevignette expectancies and related vignette conditions (Grief Work Expectancies × Vignette Severity, Grief Length Expectancies × Vignette Time Since Death) and time and severity of symptoms (Vignette Severity × Vignette Time Since Death) was only a marginal addition to the model, R2 chang e = .03, Fchange(5, 482) = 1.93, p = .08. Results indicated that none of the interactions were significant predictors of SD ratings—Grief Length Expectancies and Vignette Time Since Death, b = –0.24, p > .05; Grief Work Expectancies × Vignette Severity, F(1, 486) = 2.38, p > .05 (despite the individual dummy code for High Grief Work Expectancies × No Versus High Severity being a significant final model)—and Vignette Severity × Vignette Time Since Death, F(2, 485) = 2.18, p > .05.
Discussion
This study sought to empirically test the myths of coping with loss, which purport that social supporters expect a griever to display distress and engage in “grief work”; otherwise, the griever will be judged as coping poorly (Wortman & Silver, 1989). It was also assessed whether there was an expected time it would take for someone bereaved to recover, in the context of current diagnostic proposals of pathological grieving, which have suggested 6 months, 1 year, and 2 years as potential markers for abnormally long reactions (Horowitz et al., 1997; Maciejewski, Zhang, Block, & Prigerson, 2007; Maercker et al., 2013; Prigerson et al., 2009). To assess these, participants were asked to imagine they were potential support providers for the bereaved person in a vignette to determine whether displays of distress would result in perceptions that the griever was coping well and engaging appropriately in the mourning process, at either 2 months or 1 year postloss.
Do People Believe Grief Must Be Worked Through?
Supporting the hypothesis around the effect of Grief Work Expectancies on attributions of adjustment, the results indicate that the participants in this study do seem to subscribe to the myth that one must process their loss (Wortman & Silver, 1989). The extent that people believe that grief needs to be “worked though” can influence perceptions of how well a griever is coping with the loss of a spouse. Increased endorsement of the belief that one must process the loss to recover from grief was associated with increases in coping/adjustment ratings across vignette conditions. There was also a main effect of severity of grief presented in the vignettes on adjustment ratings, with any person demonstrating any grief symptom being rated as coping better—in effect “going through” their loss—regardless of participants endorsement of belief in the need for grief work in the Grief Work Expectancies scale. In the moderation analysis, coping/adjustment ratings were consistently high regardless of any demonstration of symptoms in the vignettes. Interestingly, despite lower endorsement of grief work expectancies, only the “no grief” severity demonstrated a moderated effect, rating any grief expression as functioning the worst, which appear on the face of it to be consistent with the belief that grieving is necessary for adjustment despite the self-reported low expectancies.
This bias for grief work is further highlighted in the examination of the interaction between Severity × Time Since Death as presented in the vignettes. Again, those vignettes where the person was demonstrating any grief symptoms were viewed as coping better/better adjusted, regardless of time since death. Together, one might infer that endorsement of the cultural expectation that coincides with Freud’s “requirement of mourning” appears to inform many of the ratings in this study. This highlights the extent that psychoanalytic and attachment theories (i.e., Freud and Bowlby) have permeated cultural expectations of grieving.
It was surprising that gender of the griever in the vignette did not appear to impact attributions of the grievers, as there are different social expectations regarding the appropriate amount of emotional expression for men versus women. However, this finding is consistent with other bereavement studies that have failed to find gender effects impacting attitudes of sympathy for grievers (Penman et al., 2014; Versalle & McDowell, 2005).
Expectations for How Long It Is Viewed Adaptive to Grieve
Findings also speak to the expectancy for how long one is expected to grieve a spousal loss, with any grief severity still present after 2 years being rated equally as 2 months. Somewhat supporting our hypothesis regarding the effect of Grief Length Expectancies on attributions of coping, emotional disruption due to spousal loss was seen as equivalently adaptive at 2 months as it was at 2 years. This was further supported by looking at the No Grief group where coping/adjustment ratings went down for vignettes set 2 years after the loss, suggesting that participants did not think the people presented in the vignettes should have recovered from their loss by then. In fact, increases in the ratings of how long it would take before one was able to move on were associated with increased PC/A across vignettes. This is despite 59% of respondents indicating that they would expect grief to resolve within 1 year from the loss (33% indicated before 6 months); given the frequencies per item, it appears that within a year seems to be most the most accepted: immediately = 1%, within a month = %, within 6 months = 23%, within 1 year = 26%, within 2 years = 19%, within 5 years = 11%, and never = 10%.
Pitfalls for Those Bereaved
Unfortunately, at least for those who are spousally bereaved, and contrary to the myths of coping with loss, expectations that grief will involve disruption and need to be processed as signs of adaptive coping did not extend to acceptance, inclusion, or willingness to talk about the loss with the people in the vignettes. While increases in Grief Length Expectancies were marginally associated with decreases in the SD scale, when looking at the main effects after controlling for our covariates, across the board, as ratings of coping/adjustment went up with demonstration of grief symptoms, social discomfort went up as well. Interestingly, in the final model (Step 4 of the model building), increases in the Grief Work Expectancy scale were associated with increased social discomfort (Table 3).
On the whole, the results of this study indicate that while participants seemed to expect grief involves emotional disruption and takes an extended period of time to resolve, any level of symptom presentation in vignettes were associated with an increase in reported social discomfort. This highlights the catch-22 that those grieving might find themselves in. Social expectations seem to be that people who are bereaved will express and process their grief, but they may be socially isolated as a result.
This finding is well supported. For example, a recent study compared vignettes of recently bereaved people who met criteria for PGD, 2 years after a loss. Those with PGD symptoms received more stigmatizing ratings and stronger desire for social distance from potential social support providers (Eisma, 2018). These findings are also consistent with past studies where bereaved and cancer patients reported that social supporters tended to minimize the loss, force cheerfulness, and provided bromides/platitudes, which were unhelpful to cope with loss or illness, despite overlap in understanding between those bereaved and potential supporters on what kind of help those grieving a loss might require (Lehman et al., 1986). This finding is significant especially given the import the role that social support can play in postloss recovery, as unhelpful support is associated with poor outcomes (e.g., Aoun et al., 2015; Juth et al., 2015).
The finding that grieving can incur social penalties is contrary to evolutionary views of public grief expression. For example, Reynolds, Winegard, Baumeister, and Maner (2015) hypothesized that grief is a hard-to-fake signal of the ability to form bonds and dispositional cooperativeness that would evoke perceptions of individuals as quality social partners. The apparent discrepancy between Reynolds et al. (2015) and the current study’s findings may be due to the macrolevel of analysis of Reynolds et al. and the microlevel of analysis of this study. Just because grieving signals a person’s capacity to form social bonds does not mean that there would be a personal incentive for social support providers to help the bereaved work through the grief. At a universal level, people can understand the need to cope and grapple with the loss, but at an individual level, social supporters’ anxieties about interacting with the griever cause them to provide feedback that the griever is coping poorly.
Implications for False Expectations and Unhelpful Social Support
In addition to the potential social consequence for beliefs about the necessity of grief processing, there may be consequences to societally held grief work beliefs related to self-attributions about how one must cope with loss and how one might be doing as they are coping. Empirical work has consistently repudiated the need to show intense distress and work through the loss to adapt to loss successfully (see Wortman & Boerner, 2011).
Bonanno et al. (2004) found that the most common grief response from the sample was resilience—showing little to no distress following the loss and quickly returning to preloss functioning. People who showed no distress were found to be just as attached and invested in the lost relationship, opposite to what the “myths” of coping would suggest is expected from the griever, thus indicating that these societally held expectancies for grief are inaccurate. Indeed, several studies have debunked the myths of coping: Grief work was defined as avoidance, predicting poorer adjustment postloss (Bonanno, Papa, Lalande, Zhang, & Noll, 2005), and expression of positive emotions has been associated with better adjustment postloss (Keltner & Bonanno, 1997; Ong, Bergeman, Bisconti, & Wallace, 2006; Papa & Bonanno, 2008).
The present study’s findings similarly suggest that grief work and expression of distress elicit negative judgments from social support. Reactions from support providers which convey a decreased willingness to interact through avoidance or exclusion, or discouraging displays of distress by either changing the subject to something more positive or forcing cheerfulness/using platitudes to try to “cheer up” the griever and reduce the supporter’s own distress can create critical self-appraisals and unhelpful social cognitive processing on the part of the griever, potentially creating a less adaptive response to loss of a spouse (e.g., Dakof & Taylor, 1990). Verbal disclosure of thoughts and emotions can signal a need for social support and aid in cognitive restructuring and the exploration of possible selves after a loss of a close loved one (Bonanno & Kaltman, 1999; Greenberg, Wortman, & Stone, 1996; Lepore, 1997; Seery, Holman, & Silver, 2010), but doing so can also invite negative social feedback, likely due to social supporters feeling overwhelmed by the anxiety evoked in them by the griever’s distress (Gottlieb & Wagner, 1991; Lehman et al., 1986; Juth et al., 2015).
Lehman et al. (1986) hypothesized that poor interactions between grievers and their supporters may be particularly unhelpful. When potential supporters discourage open discussion about the loss and instead encourage positive reappraisal and quick recovery soon after the loss, those coping with loss may likely errantly interpret this social feedback as dispositional judgments of their own coping. In other words, the griever thinks they are not coping properly and that there’s something wrong, and they remain stuck in the grief. The same pattern may follow when someone experiencing loss exhibits no distress and returns to preloss functioning “too quickly.”
Limitations
A few limitations qualify these results. One limitation of this vignette study is that participants may have imagined grievers in a way that was less personally distressing and more tolerable. Thus, while trying to capture which factors predicted social support feedback to the griever, the interactional element that might make these processes more salient is being missed. Instead, participants were asked how they would likely judge a close friend experiencing spousal bereavement. Another major limitation of this study is that the participant did not have to interact or spend time with the griever or provide support. Given that the sample was comprised mostly of Caucasian participants, this study is limited in understanding how majority versus nonmajority status may impact perceptions of grief. In addition, the current study’s results are limited to attributes of spousal bereavement as spousal loss may produce differences in social attributions compared with other types of losses. Other studies have found that loss of a child was less negatively judged than loss of a spouse (e.g., Miller, 2015).
Another related limitation is the use of convenience sampling. It is unclear how participants self-selecting into this study might have affected the results. Perhaps only those with the strongest feeling about grief participated and the effects of grief expectancies or vignette factors on the outcomes are larger in this sample than in the general population. This is relevant as 23% of the sample responded “Yes” to, “Are you grieving the loss of a loved one now?” While there were no differences in in SD ratings, PC/A ratings, or Grief Work Expectancies scale (p values > .05), those who were bereaved were older, t(183) = –2.94, p < .01, MNot Bereaved = 4.17, MBereaved = 4.64, more likely female χ2 = 13.49, p < .001, were higher in anxiety, t(170) = –3.58, p < .001, MNot Bereaved = 1.67, MBereaved = 1.98, and had higher Grief Length Expectancy scores, t(177) = –2.91, p < .01, MNot Bereaved = 31.79, MBereaved = 35.50—all of which were significantly or marginally associated with outcomes in Step 1 of the model building, though mainly in ways that might have reduced the amount of social discomfort reported. Nonetheless, the possibility remains that self-selection changed the results in unforeseen ways.
Future Directions
This study examined if belief in the myths of coping as discussed by Wortman and Silver (1989) affect attributions of potential support providers about those who are spousally bereaved. There is very little empirical work in this area, despite the effect societal expectations might have on adjustment to grief. Although Silver, Wortman, and Crofton (1990) experimentally tested social discomfort for potential supporters of cancer patients and found negative disclosures to create discomfort and anxiety in potential support providers, future work should explore which aspects of grief expression cause discomfort in social supporters of the bereaved, despite expectations of grief work. Given this paucity, future work could focus on moderators of the expression of grief and social discomfort linked with the goal of identifying ways to facilitate access to needed social resources in the recently bereaved. Another unexplored area is the effect of Grief Work and Grief Length Expectancies on individuals coping with their own losses, discussed earlier. While these expectancies seem to affect the judgment of potential support providers, it is unclear the extent generally, or under what conditions, that these expectancies might affect how individuals might cope with their own loss.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.