
Abstract
This study was designed to promote enhanced self-efficacy and decreased stress levels for family caregivers at a hospice care hospital, thus increasing their quality of life. This is achieved through group flower arranging sessions. The objectives are to (a) enhance self-efficacy scores for family caregivers of Calvary patients, (b) decrease stress levels for family caregivers of Calvary patients, and (c) disseminate results to other hospices. The results show that the flower arranging sessions resulted in significantly increased self-efficacy and decreased stress and associated problems for the caregiver participants. Implications and suggestions for future research are discussed.
Introduction
Family Caregivers
Family and friends often become the informal caregivers to terminally ill spouses, siblings, and others. They support and supplant the role of professionals resulting in personal stress and compassion fatigue. Informal caregivers are the main providers of end-of-life care (Tang, 2009). The availability of an informal caregiver support system is often a major determinant of whether a dying patient can remain at home (Burns, Abernethy, Grande, & Currow, 2013).
The level of burden for those who care for relatives with cancer is greater than a relative who is old and unable to function independently. The diagnosis may contribute to this increased burden. The diagnosis of cancer evokes fear and stress in both patients and family. End-of-life caregivers are primarily female (75.1%), and most are spouses 41.5% with an average age of more than 60 years; and many have their own age-related health problems (Applebaum & Breitbart, 2012). Most caregivers provide physical, emotional, and sometimes financial support (Perez et al., 2018). End-of-life caregivers also frequently assist with bereavement support for other family members, manage funeral arrangements, advocate for the decisions of their loved one, or make decisions when their family member cannot (National Hospice and Palliative Care Organization, 2013).
The negative effects of this caregiving have been described as compassion fatigue, burden, and caregiver stress (Schroeder & Lorenz, 2017). Risk factors for compassion fatigue have been identified as including life stressors; decreased life satisfaction; a lack of social, collegial, and administrative support; and difficulty maintaining professional boundaries (Kim, Shaffer, Carver, & Cannady, 2015). Compassion fatigue is not limited to family caregivers; in fact among nurses, oncology nurses are reported to be at highest risk because of their intense, intimate, caring interactions with terminally ill patients and their families (Barber, 2013). It does need to be noted that there are also positive effects from caring for a loved one including—knowing that a family member is receiving excellent care, personal growth, and increased meaning and purpose in life (Schroeder & Lorenz, 2017).
Assisting caregivers to develop coping skills will enhance their life as well as positively impact the cancer patient’s final days (Gaugler, Eppinger, King, Sandberg, & Regine, 2012). Caregivers with greater levels of resilience and self-efficacy have reported lower levels of psychological illness, reduced rates of compassion fatigue, and greater levels of well-being (Bandura, 1977; Merluzzi, Phillip, Vachon, & Heitzmann, 2011). This project focused on strategies to increase caregiver feelings of self-confidence in this new role and decrease their stress levels.
Flower Arranging
Flowers evoke many responses including love, caring, and beauty. Human reactions to flowers involve smell, texture, and color which provide an aesthetic attraction. For end-of-life patients in a hospital setting, flowers can enhance their last days and experiences with their loved ones (Huss, Yosef, & Zaccai, 2018). Flower essences bring feelings of calm, peace, and reduction of stress. A team of researchers at Rutgers (Haviland-Jones, Rosario, Wilson, & Mcguire, 2005) explored the link between flowers and life satisfaction in a 10-month study of participants’ behavioral and emotional responses to receiving flowers. The results in their study show that flowers can moderate moods and result in an individual’s expression of joy and happiness. They found these effects on moods were long-term and participants reported a decrease in depression, anxiety, and anger. The authors further noted that “flowers make intimate connections. The presence of flowers led to increased contact with family and friends.” (https://aboutflowers.com/quick-links/health-benefits-research/emotional-impact-of-flowers-study/). Alston (2010) reported that flower therapy increased the feelings of well-being and increased the participation of patients diagnosed with depression in small groups. It is anticipated that the use of flower arranging by caregivers will also result in positive outcomes.
Flowers have the added benefit of olfactory stimulation in addition to the pleasing visual impact. The American Cancer Society has noted how the use of aromatherapy with essential oils from plants can improve the quality of life and reduce side effects resulting from treatments (https://www.cancer.gov/about-cancer/treatment/cam/patient/aromatherapy-pdq#section/_3). We predicted that the process of selecting favorite flowers and creating a pleasing arrangement which would be placed in the patient’s room would result in similar positive benefits for patients and caregivers as well as increase the caregiver’s confidence in exerting a positive impact on the patient’s life.
Self-Efficacy
Caregiver self-efficacy is conceptualized as individuals’ beliefs in their ability to carry out activities and tasks specific to care giving. Bandura (1977) theorized that individuals with higher levels of self-efficacy will have a greater level of success in completing care-giving tasks, lower levels of psychological and physical illness, reduced rates of burnout, and greater levels of well-being than those with low levels of self-efficacy. Caregivers with greater levels of resilience and self-efficacy have reported lower levels of psychological illness, reduced rates of stress, and enhanced feelings of well-being (Merluzzi et al., 2011). Thus, increased self-efficacy may buffer the stress associated with this role.
Hypotheses
This aim of this study is to find an association between (a) flower arranging and the stress level of caregivers, (b) flower arranging and self-efficacy (i.e., Obtaining Respite and Controlling Upsetting Thoughts) of caregivers, and (c) demographic factors and self-efficacy or stress levels. We also examine the impact of flower arranging on self-efficacy, feelings, and stress. We make the following hypotheses: Hypothesis 1 (H1): There will be a significant association between flower arranging and the stress level of caregivers. Hypothesis 2 (H2): There will be a significant association between flower arranging and the self-efficacy of caregivers. Hypothesis 3 (H3): There will be a significant association between flower arranging and problems caused by the stress of caregivers.
Method
Participants
A convenient sampling technique was used to select the sample and 71 caregivers were recruited for this study. Their family members or friends became terminally ill and were receiving care in the Calvary Hospital.
Procedure
The project initially included engaging family caregivers in two activities: photo collage designing and flower arranging. However, we were not able to obtain sufficient participants for the photo collage sessions. Calvary social workers continue to offer the collage activity, and as data are obtained, the results will be reported. This article describes the flower arranging program over a 4-month time period and results.
The sessions were held in the Family Care Center where soothing music is played in the background and coffee and tea are available. The flower arrangements were used to enhance the patient’s personal room environment. Family caregivers were invited to this center for other activities including Lunch and Learn educational sessions, drumming, and massage among other modalities. They could also drop in for individual counseling as needed. The Family Care Center staff at Calvary Hospital encouraged participation and assisted during the sessions.
Enob (http://www.enob.org/newyork/) is a community nonprofit 501-(c) (3) organization whose mission is to provide cultural and arts experience for underserved populations. Specifically, this organization brings concerts to disabled and hospitalized patients as well as flower arranging classes under their logo Spreading Happiness (Spreading Happiness (n.d.)). This group provided the weekly flower arranging classes for up to 10 caregivers. Enob brought all needed supplies including seasonal flowers and containers and provided expert instruction. During these classes, an informal support network was formed as family caregivers shared materials, ideas, and concerns. Informal conversations went beyond encouragement for each other’s flower creations to sharing their feelings about impending loss of loved ones. Many participants shed tears and were able to express feelings of fear in this safe setting. The end result—a beautiful flower arrangement was then brought to the patient’s room and enhanced the visual and olfactory room environment. It was determined by Calvary Hospital that flowers are not contraindicated in patient rooms since it is a hospice setting.
Data Collection Instruments
Caregiver self-efficacy assessment
The Revised Scale for Caregiving Self-Efficacy (Steffen, Mckibbin, Zeiss, Gallagher-Thompson, & Bandura, 2002; Appendix), which has excellent alpha coefficients (.8 for each of the three subscales), was reviewed for use in this project. This scale measures three domains of caregiving self-efficacy: Obtaining Respite, Responding to Disruptive Patient Behaviors, and Controlling Upsetting Thoughts. Two sections are appropriate for this study; however, the component focused on Self-Efficacy for Responding to Disruptive Patient Behaviors is not. The other two components: Self-efficacy for Obtaining Respite and Controlling Upsetting Thoughts about caregiving were used. There were five questions in each domain, which asked the participants to rate their degree of confidence ranging from 0 (i.e., Cannot do) to 5 (i.e., Can do). We also asked participants to report their stress level and indicate to what extent is dealing with the stress causing their problems with sleep, appetite and eating habits, mood stability, memory, and sense of well-being using a Likert-type scale of 0 to 5. Toward the end of the survey, they were asked to give additional comments.
Modified self-efficacy scores
Participants completed the Modified Revised Scale for Caregiving Self-Efficacy (Steffen et al., 2002; Appendix) before and after each flower arranging or collage making project. This scale measures two domains of caregiving: Obtaining Respite and Controlling Upsetting Thoughts. Additional questions relevant for this study have been added.
Participant satisfaction scores
A Likert-type scale was developed to assess pre- and postactivity stress scores for each participant as well as open-ended comments describing participant satisfaction with each activity, the instructions, materials, schedule, and overall project activities and to solicit feedback for future changes.
Data Analyses
The data obtained were analyzed through descriptive and inferential statistics including two-sample t test, repeated measure analysis of variance (ANOVA), and paired-sample t test.
Results
Participants
The data on sample demographic characteristics were analyzed using descriptive statistics. The data in Table 1 show that most of the participants (54.3%) were 51 to 76 years old. Majority of the participants (92.9%) were females and 7.1% were males. They self-identified as Hispanic (41.7%), Caucasian (31.4%), African American (20%), and Asian (1.4%). One participant did not provide the optional demographic information. Calvary Hospital is located in Southeastern Bronx, New York. This population distribution is representative of Bronx, where most of the participants reside.
Distribution of Participants According to Their Age, Gender, and Ethnicity as well as County of Residence.

Note. N = 71.
Stress Level
A paired-sample t test was conducted to compare the stress levels before and after the intervention of flower arranging (Figure. 1). There was a significant decrease in the stress level after the intervention (mean [M] = 3.06, standard deviation [SD] = 1.38) than before the intervention—M = 1.75, SD = 1.25; t(70)= –7.717, p = .000. According to our 5-point Likert-type scale, 0 indicates very high stress level and 5 indicates low stress level. The stress score from the posttest was 1.3 points higher than that from the pretest (95% confidence interval [CI] [1.648,0.971]). The effect size (Cohen’s d) is 0.91. These results suggest that flower arranging had a significant positive effect on reducing the stress level of family caregivers.
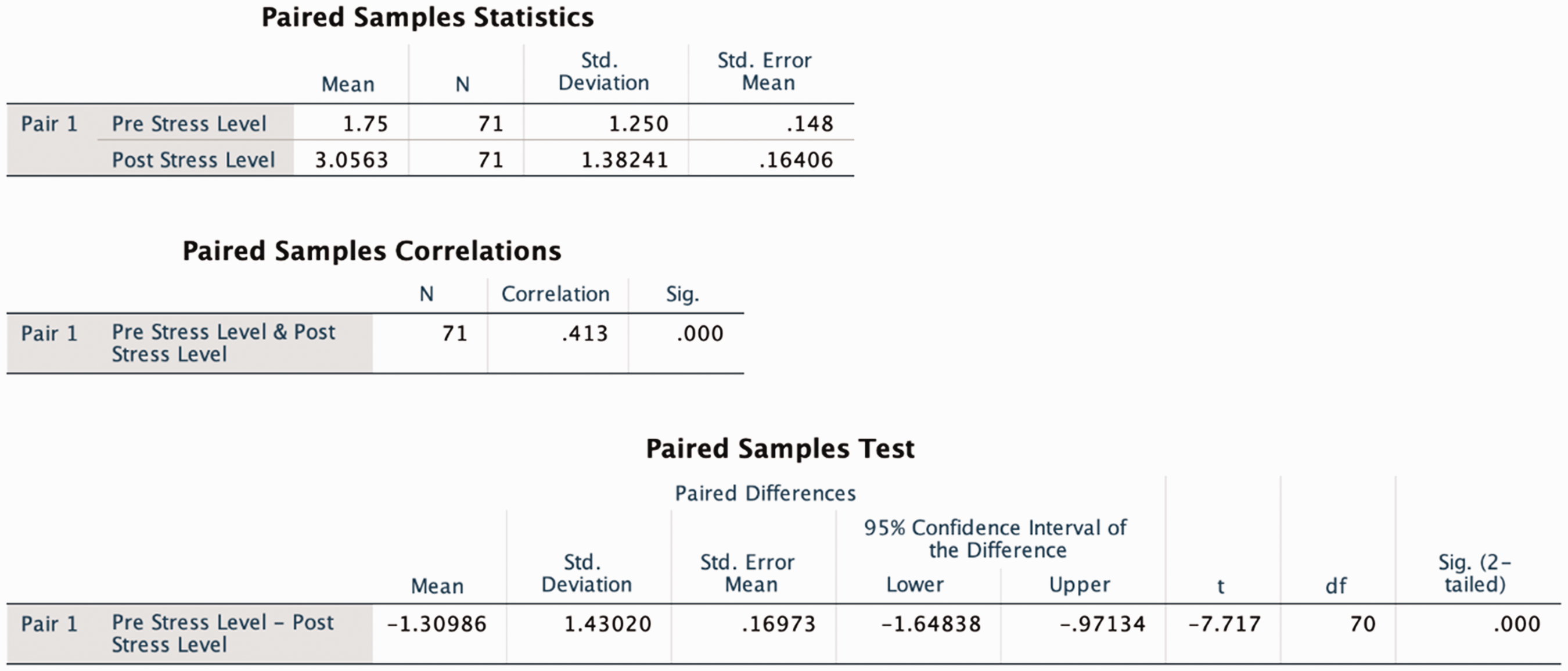
Paired-sample t-test results showing the stress levels before (prestress level) and after (poststress level) flower arranging. N = 71.
Self-Efficacy
Although 71 participants took the pretest before the intervention and participated in the flower arranging sessions, only 16 completed the self-efficacy test in the posttest. The reason is the rest of the participants (55) were anxious to get back to their loved one, thus only completing the posttest on the Stress section. Therefore, we have a pretest with a sample size of 71 and a posttest with a sample size of 16.
We removed the data on stress from the 55 participants who did not complete the posttest. We ran a paired-sample t test to determine whether there was an association between flower arranging and self-efficacy (i.e., Obtaining Respite and Controlling Upsetting Thoughts; Figure 2). We set the alpha value to .1. There was a significant difference in self-efficacy scores before (M = 2.9688, SD = 1.026) and after (M = 3.0875, SD = 1.098) the flower arranging intervention; t (15)= –1.8, p = .092. The effect size (Cohen’s d) is 0.45. These results suggest the flower arranging significantly increase the participants’ sense of self-efficacy.
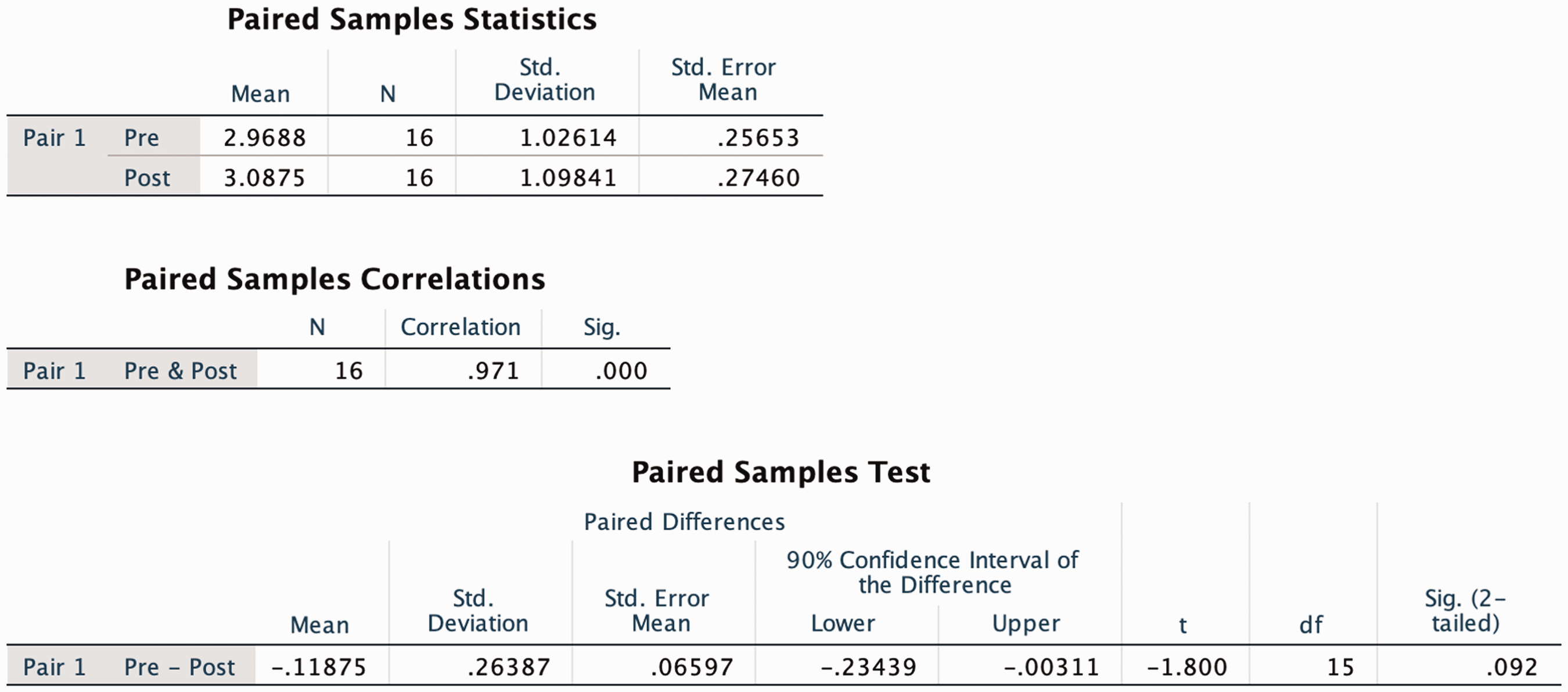
A paired-sample t test was conducted comparing participants’ self-efficacy scores before and after the flower arranging. N = 16.
Self-Efficacy Scores Comparison Between Age Groups
The self-efficacy scores before and after the flower arranging (N = 16) were disaggregated by age groups (Figure 3). A repeated-measures ANOVA with age as an independent factor and self-efficacy scores as a within-subjects factor was run. The analysis revealed no main effect between the self-efficacy scores and the age groups, F(2, 13) =.776, p = . 48.

The result of a repeated-measures ANOVA with age as an independent factor and self-efficacy scores as a within-subjects factor. N = 16.
Self-Efficacy Scores Comparison Between Gender
The self-efficacy scores before and after the flower arranging (N = 16) were disaggregated by gender (Figure 4). A repeated-measures ANOVA with gender as an independent factor and self-efficacy scores as a within-subjects factor was run. The analysis revealed no main effect between the self-efficacy scores and the gender groups, F(1, 14) =1.174, p = . 297.
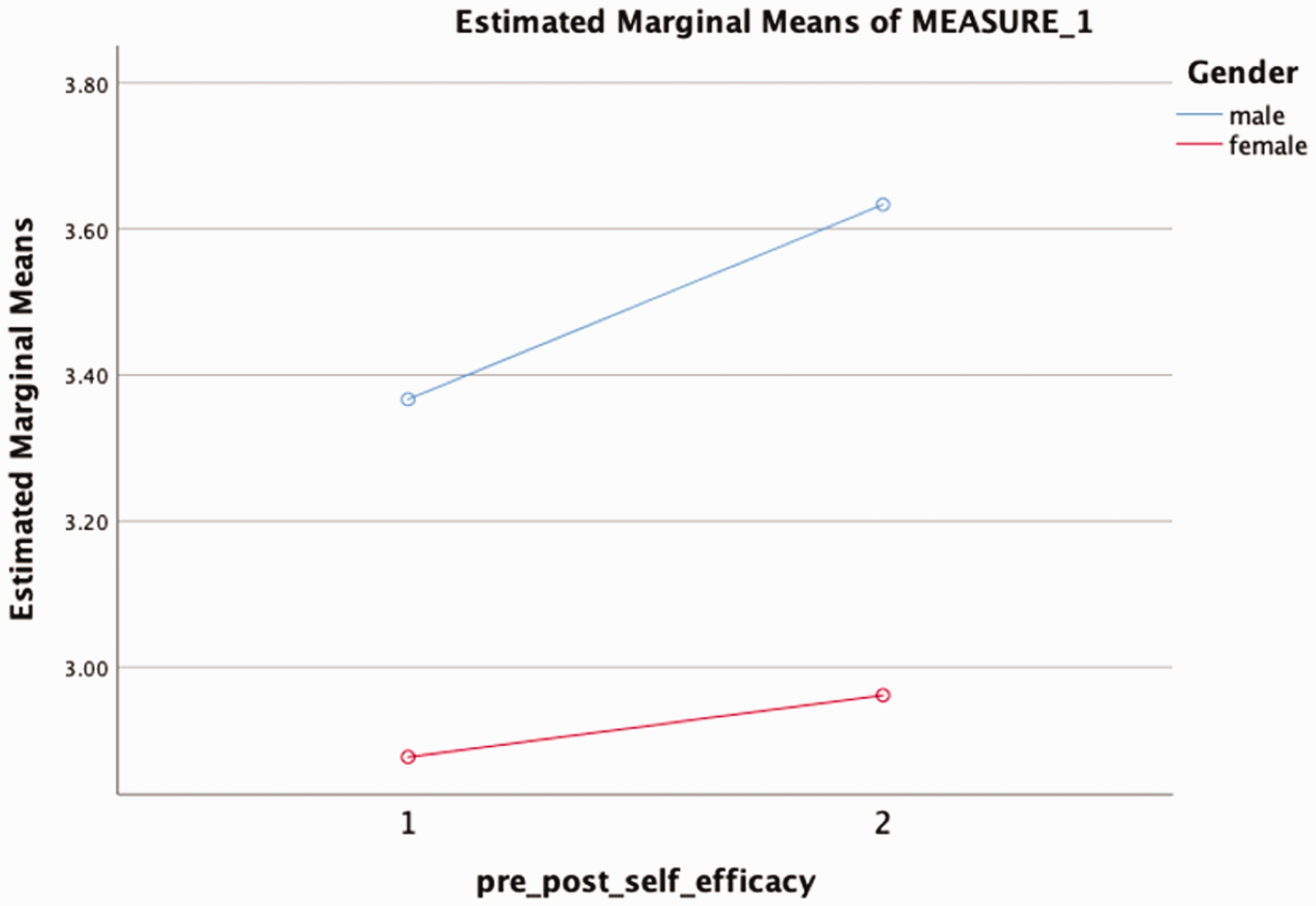
The result of a repeated-measures ANOVA with gender as an independent factor and self-efficacy scores as a within-subjects factor. N = 16.
Self-Efficacy Scores Comparison Between Ethnicity
The self-efficacy scores before and after the flower arranging (N = 16) were disaggregated by ethnicity (Figure 5). A repeated-measures ANOVA with ethnicity as an independent factor and self-efficacy scores as a within- subjects factor was run. The analysis revealed no main effect between the self-efficacy scores and the ethnicity groups, F(3, 12) =.193, p = . 899.
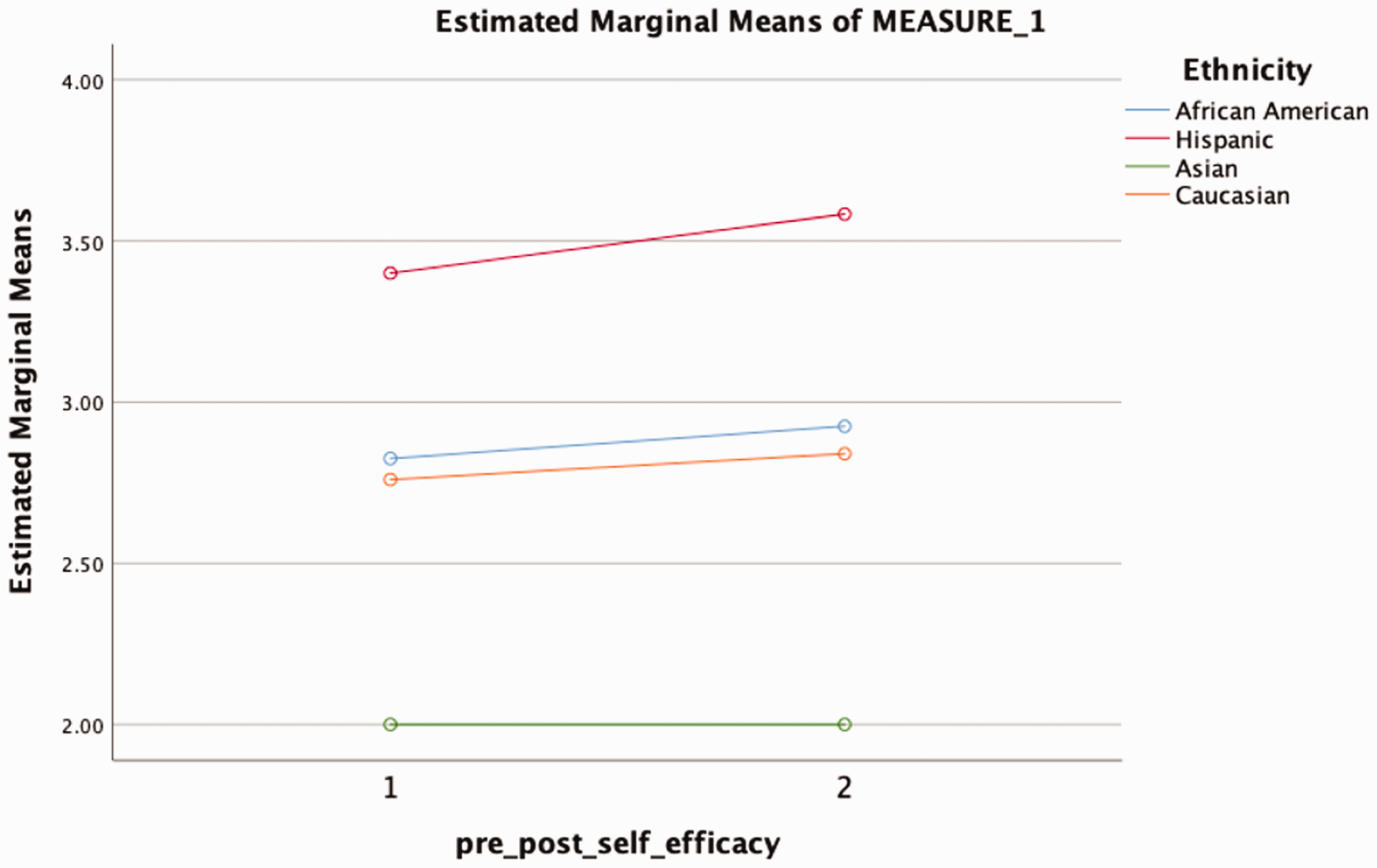
The result of a repeated-measures ANOVA with ethnicity as an independent factor and self-efficacy scores as a within-subjects factor.
Problems Caused by the Stress (i.e., Sleep, Appetite and Eating Habits, Mood Stability, Memory, and Sense of Well-Being)
A paired-sample t test was conducted to compare the stress level before and after the intervention of flower arranging (Figure 6). We removed one set of pre- and posttest data points from one participant who did not complete the posttest. Therefore, our sample size is 70. There was a significant decrease in the frequency of problems caused by stress after the intervention (M = 2.38, SD = .841) than before the intervention—M = 2.54, SD = .853; t(69)=2.462, p = .016 (95% CI [0.03, 0.286]). The effect size (Cohen’s d) is 0.29. According to our categorical scales, the lowest level of 0 indicates not at all and the highest category of 4 indicates very frequently. These results suggest that flower arranging had a positive effect on reducing the problems caused by the stress of caregivers.
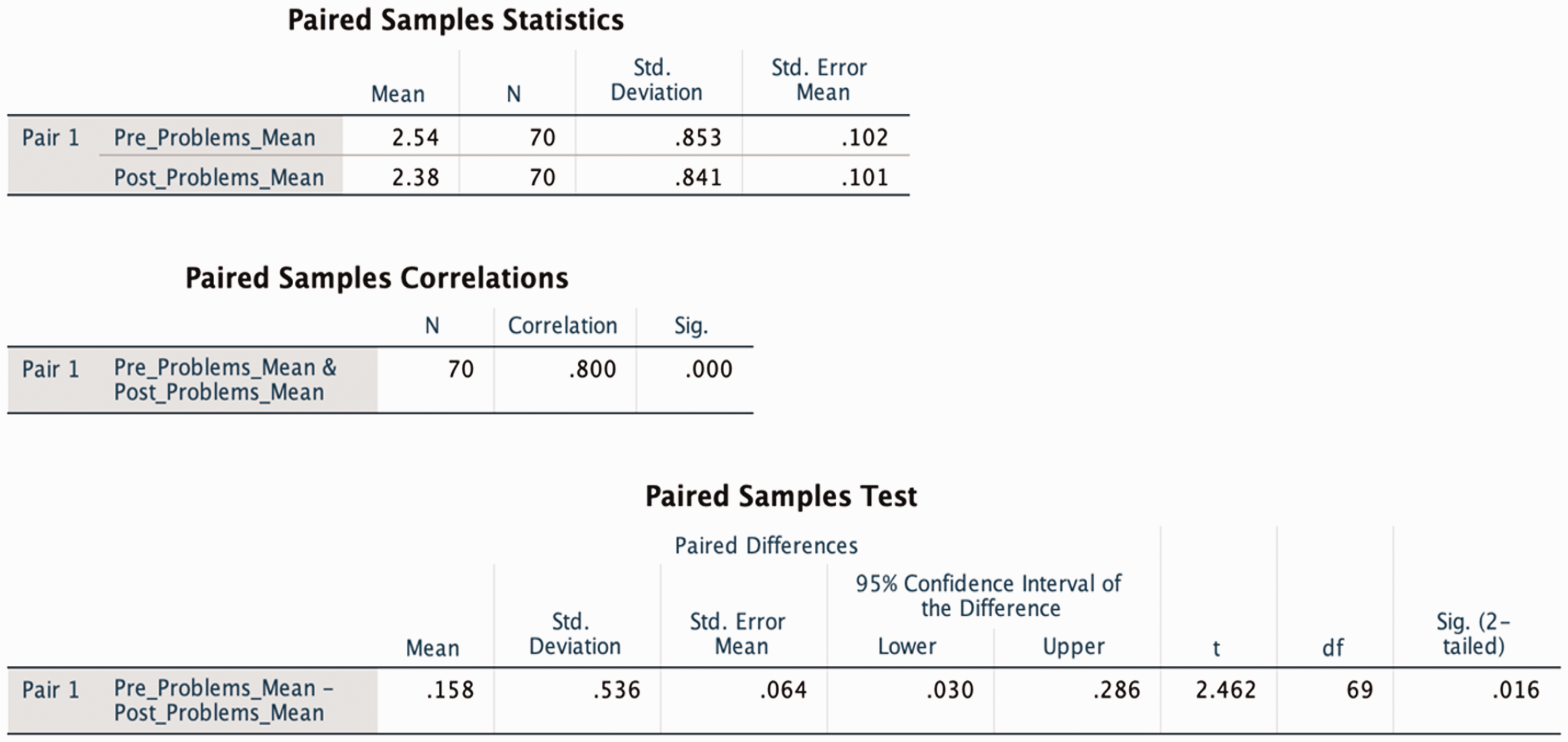
A paired-sample t test was conducted comparing the problems caused by stress before and after the intervention of flower arranging. N = 70.
Problems Caused by the Stress Based on Age Groups
The problems caused by stress before and after the flower arranging (N = 70) were disaggregated by age. A repeated-measures ANOVA with age as an independent factor and problems by stress as a within-subjects factor was run.
The analysis revealed no main effect of between age groups, F(3, 64) = .208, p = . 891, in general, but there is a significant interaction between problems caused by stress and age groups, F(3, 64) = 2.861, p = .044. Alpha is .05 and the effective size is .126. As is shown in Figure 7, the 18 to 36 age groups reported much less problems caused by stress after flower arranging.
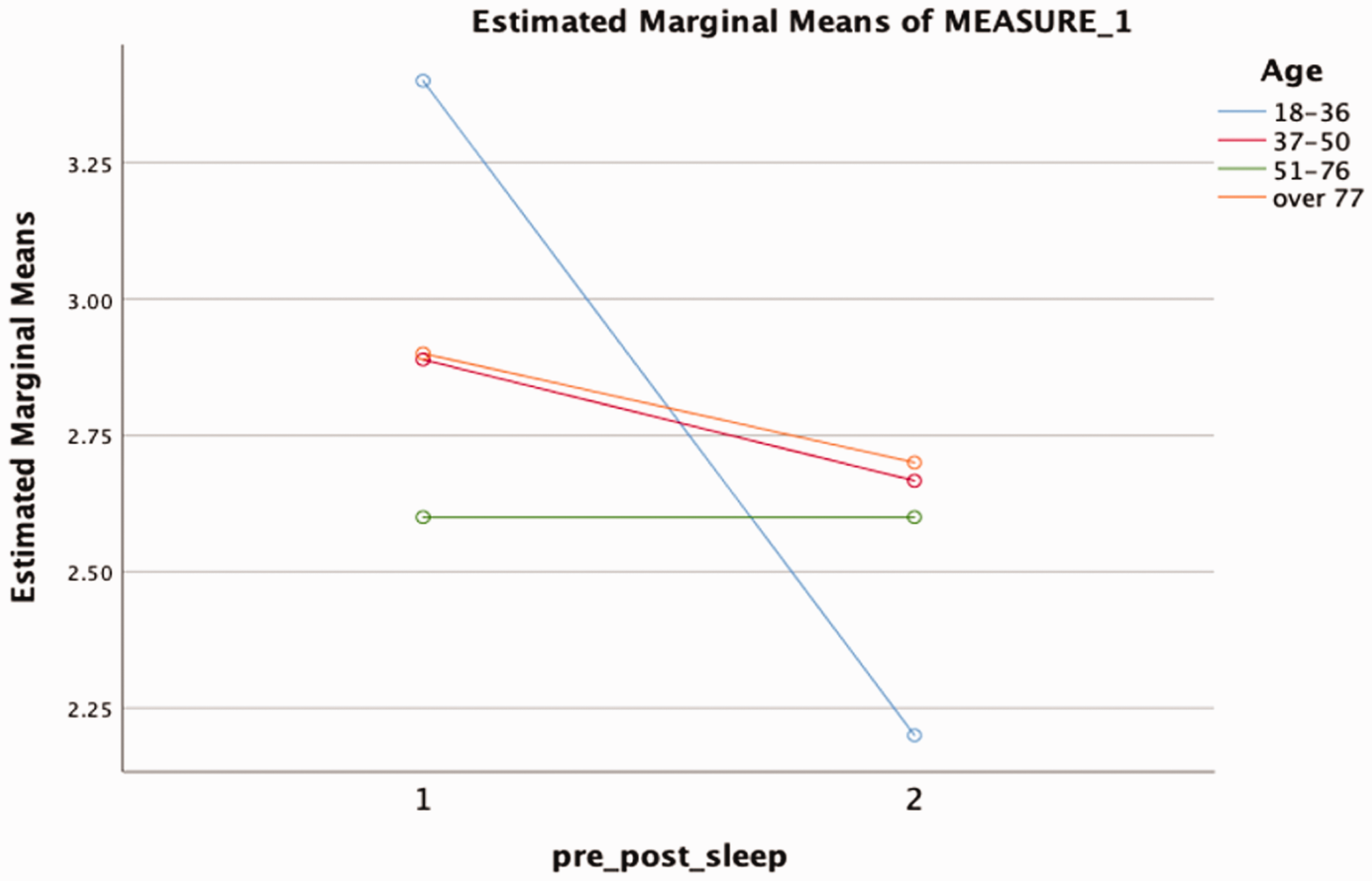
The result of a repeated-measures ANOVA with age as an independent factor and problems by stress as a within-subjects factor.
Problems Caused by the Stress Based on Gender
The problems caused by stress before and after the flower arranging (N = 70) were disaggregated by gender. A repeated-measures ANOVA with gender as an independent factor and problems by stress as a within-subjects factor was run. Although males reported less problems caused by stress (pretest: M = 3.00, SD = .707; posttest: M = 2.4, SD = 1.342) than females (pretest: M = 2.76, SD = 1.088; posttest: M = 2.62, SD = 1.054), the difference is not statistically significant (Figure 8).
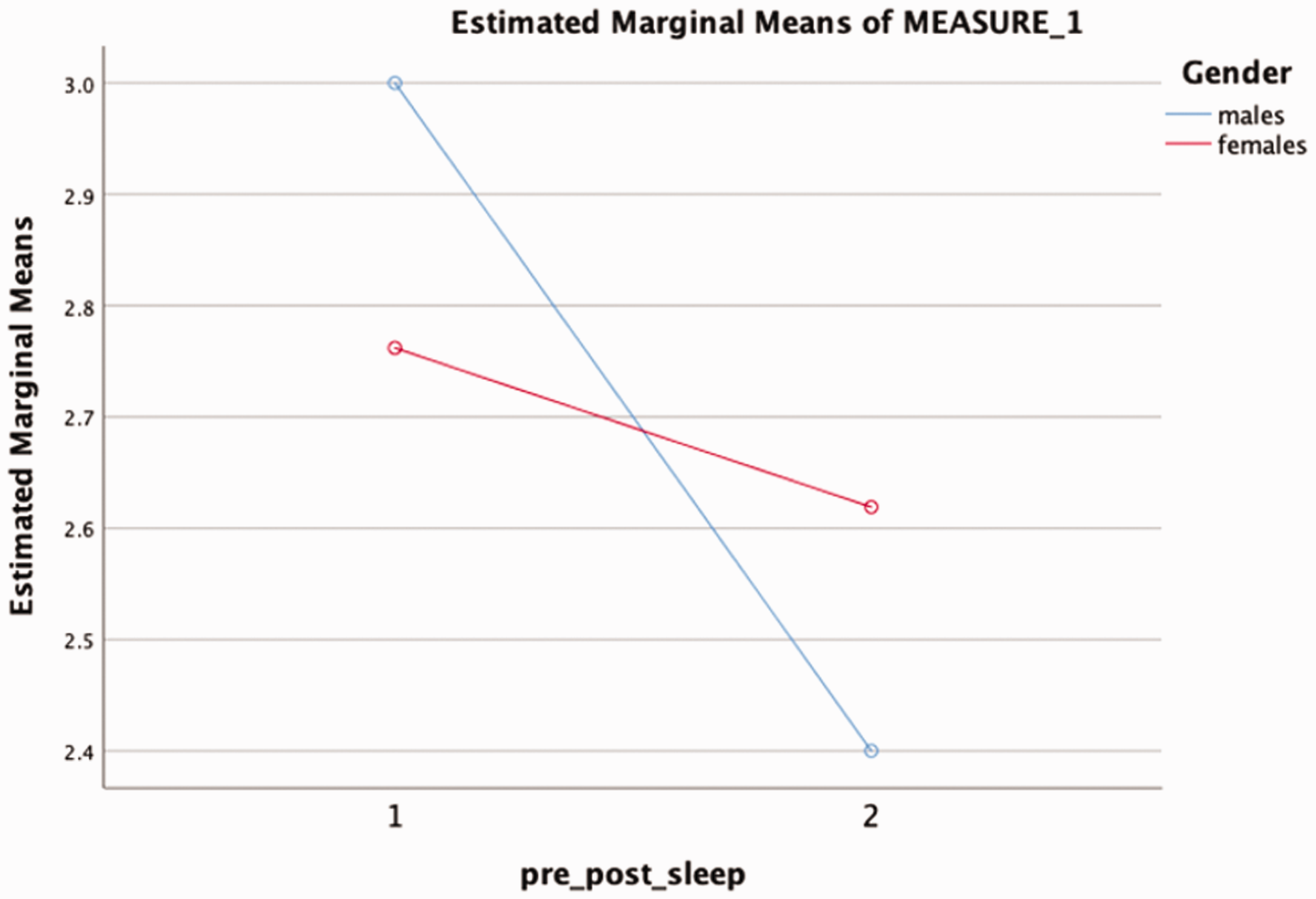
The result of a repeated-measures ANOVA with gender as an independent factor and problems by stress as a within-subjects factor.
Problems Caused by the Stress Based on Ethnicity
The problems caused by stress before and after the flower arranging (N = 70) were disaggregated by ethnicity. A repeated-measures ANOVA with ethnicity as an independent factor and problems by stress as a within-subjects factor was run. The analysis revealed no main effect between the problem caused by stress and the ethnicity groups, F(3, 64) =.394, p = . 758; Figure 9).
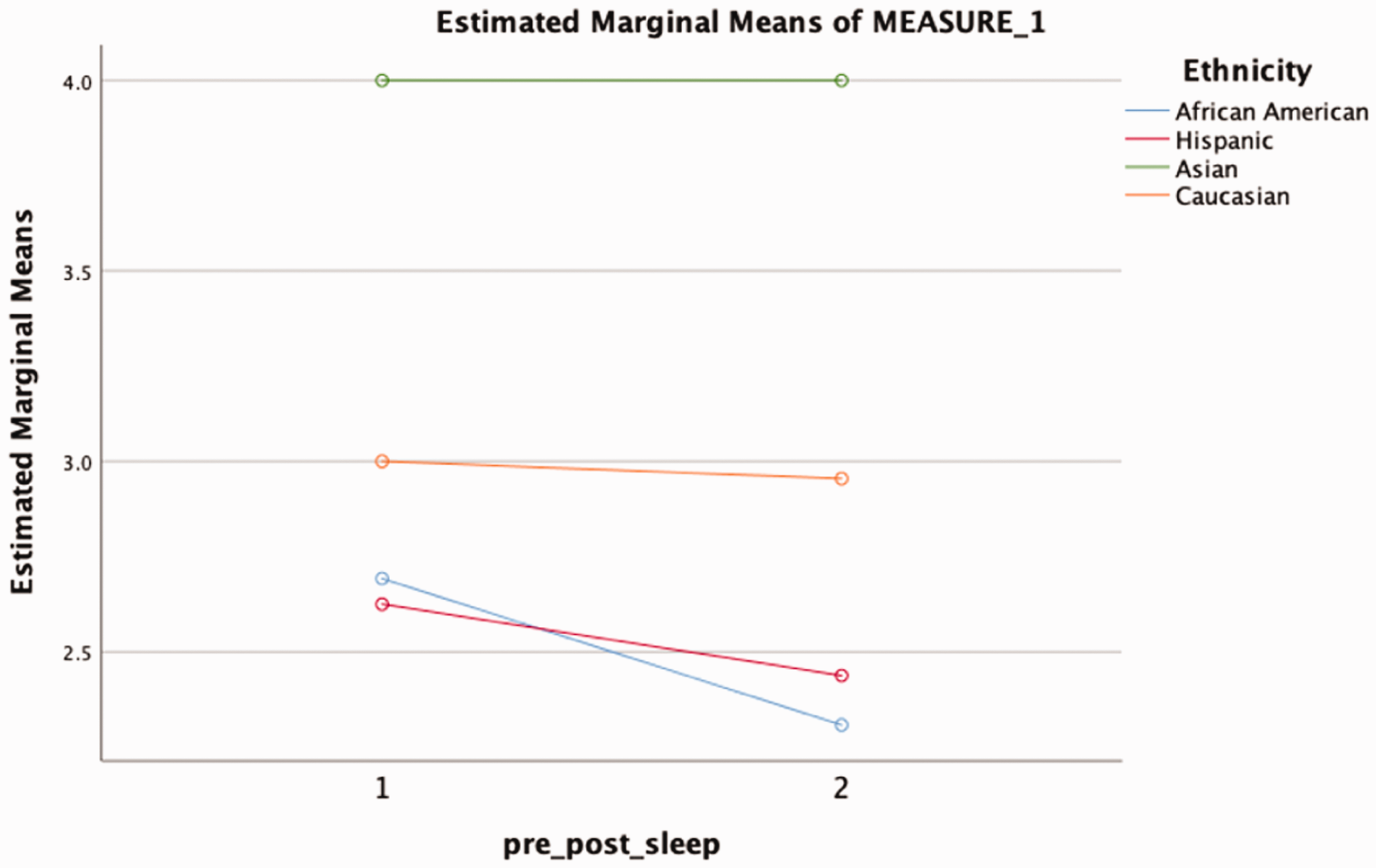
The result of a repeated-measures ANOVA with ethnicity as an independent factor and problems by stress as a within-subjects factor.
Qualitative Analysis of the Comments From Caregivers
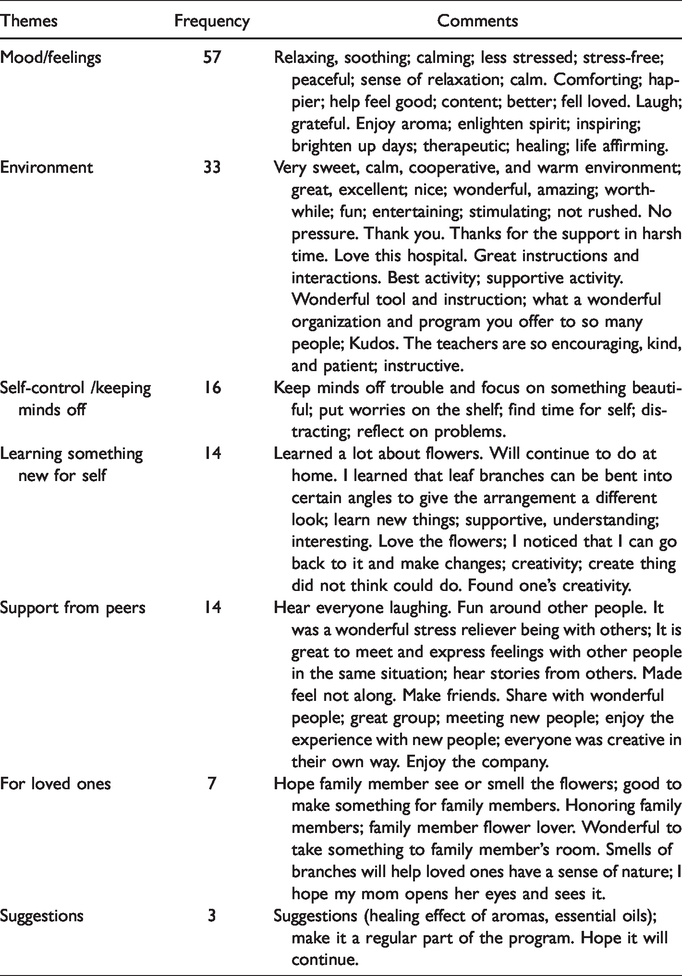
Toward the end of the survey, caregivers were asked to give comments (Table 2). Overall, all the comments are positive. We captured seven common themes listed later. They include mood or feelings, environment, self-control to keep minds off, learning something new for oneself, support from peers, for loved ones, and suggestions. Figure 10 shows the frequency of the themes being touched upon. Caregivers’ improved mood or feelings were mentioned the most (57 occurrences), followed by the instructional environment of flower arranging (33 occurrences). Some participants acknowledged flower arranging helped keep their minds off the stressful situation (16 occurrences) or allowed them to learn something new (14 occurrences). They liked the support they got from peers during those flower arranging sessions (14 occurrences) and described the hope of having their loved one appreciate the final flower artifact. Some also gave suggestions expressing the wish for the project to sustain.
Representative Comments From Caregivers Regarding Their Flower Arranging Experiences.
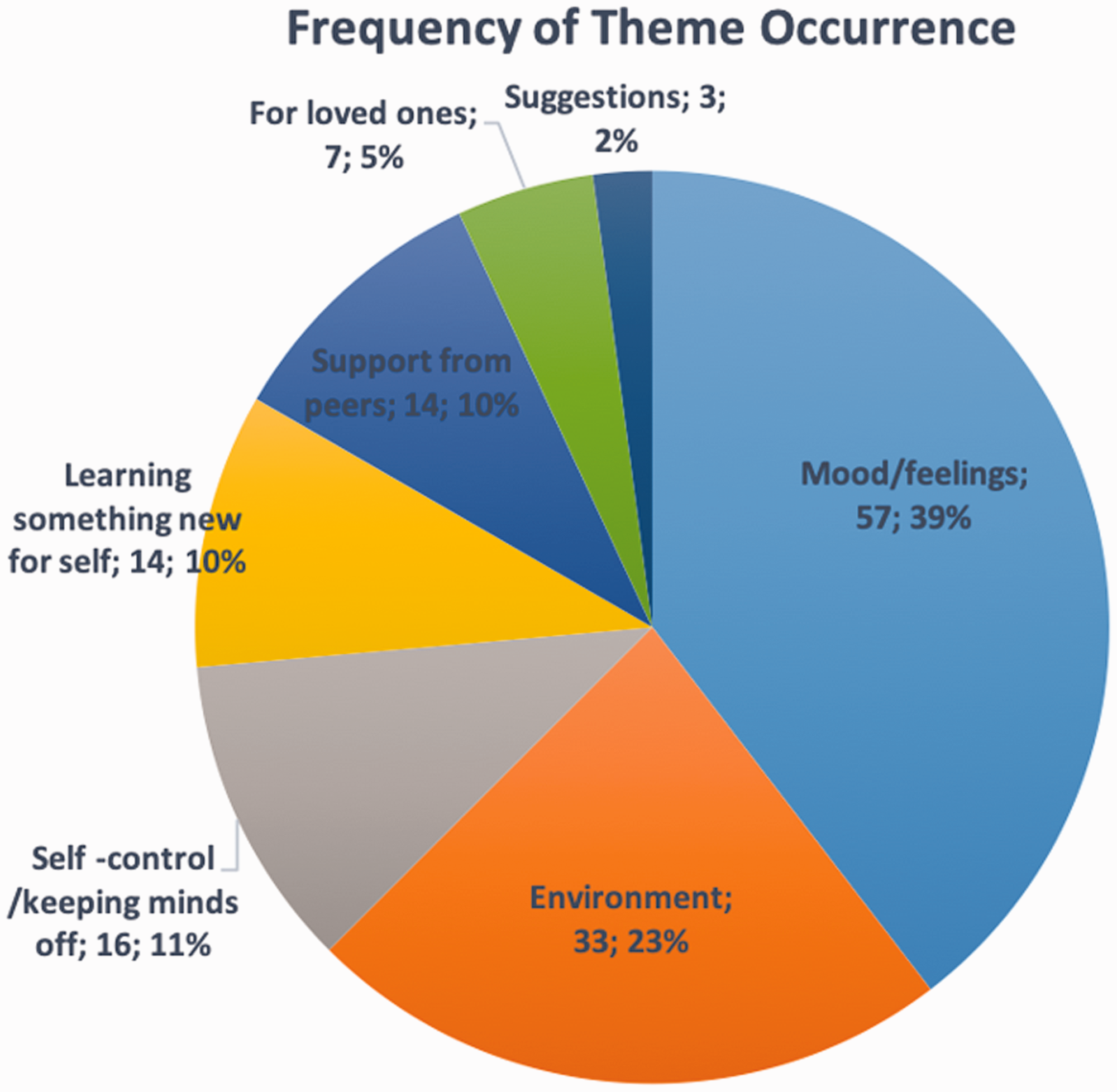
Frequency of the theme occurrence based on the comments from caregivers.
Discussion and Future Plans
In reviewing the Flowers for Healing class, Calvary Hospital recognized that this program was valuable in many ways. From the start, it had been well-received among family members, patients, and the Hospital as a whole. As the aforementioned results indicate, this intervention demonstrated significant effects of flower arranging in all the three areas: self-efficacy, stress, and the problems caused by stress.
Family member feedback consistently supported that the program was relaxing, healing, comforting therapeutic, and educational. Family members reported that they loved to be able to bring the flowers back to their loved ones at times brightening the patients’ moods and at other times simply brightening the room itself. This type of program allowed family members the opportunity to actively do something for their loved ones while simultaneously taking time for themselves to engage is a stress-reducing activity. As one family member explained: I cannot express the joy I felt each day when I entered my Mother’s room and saw my creation. The education I received was priceless; I feel encouraged to now keep flowers on display in my home. As I shared with you, for many years my Mother had an extensive garden with vegetables and flowers. Recently, the only plants we have had outside have been the roses and other flowers. Up until her illness in October, every day when my Mother got home, she would ask me to take her around to look at her flowers in the yard. I was able to give her a surprise while at Calvary with a beautiful arrangement I had made. When I walked in the room I told my Mother that I made her a gift. I put the arrangement in her hands and she said “It's beautiful!” It was the first time Mommy spoke to me in two days. When I told her that I made it for her, she gave me a kiss and said “I Love You”. It is great to meet and express feelings with other people in the same situation. I loved it. So much fun being around others that are caring for a loved one (not alone). Being here is a good distraction and relaxing. This class gives me the opportunity to share with wonderful people. It was the first time I was able to laugh in months. It really helped my stress level. I feel loved. Today was a special day. It was interesting to listen to the families and their stories. It makes me realize that I am not alone in my pain and discomfort. I love the class. I make friends with others in my same situation. This is the best activity. I love this hospital.
Calvary Hospital found this program to be an asset to the Family Care Center’s programming. It has been supported by the hospital at the highest levels, and therefore, the Hospital made the decision to shift budgeted funds and continue providing the Flowers for Healing class.
Unfortunately, as noted earlier, we were not successful in recruiting participants for the intervention of photo collaging. Perhaps, the association of photo collages with memorial services, the lack of a shared group atmosphere, or concerns that it would take time away from caring for their loved one played a role in this result.
To further the impact of the grant, results will be disseminated through journals and conferences. A program manual will be developed to allow other hospice facilities to replicate the program.
Footnotes
Appendix
Rate your degree of confidence from 0 to 5 where a 0 confidence means that you cannot do it at all, a 5 confidence means you are certain you can do it.
Please circle your response below each statement and make your ratings based on what you can do today, as the person you are NOW rather than on the person you used to be, or the person you would like to be.
1. How confident are you that you can ask a friend/family member to stay with your loved one for a day when you need to see the doctor yourself?
2. How confident are you that you can ask a friend/family member to stay with your loved one for a day when you have errands to be done?
3. How confident are you that you can ask a friend or family member to do errands for you?
4. How confident are you that you can ask a friend/family member to stay with your loved one for a day when you feel the need for a break?
5. How confident are you that you can ask a friend/family member to stay with your loved one for a week when you need the time for yourself?
6. How confident are you that you can control thinking about unpleasant aspects of taking care of your loved one?
7. How confident are you that you can control thinking how unfair it is that you have to put up with this situation?
8. How confident are you that you can control thinking about what a good life you had before your loved one’s illness and how much you’ve lost?
9. How confident are you that you can control thinking about what you are missing or giving up because of your loved one?
10. How confident are you that you can control worrying about future problems that might come?
11. Please rate your current stress level: (please circle your answer below)
To what extent is dealing with the stress of caring for your loved one causing you problems with your (please circle your answer below each item)
17. Your age: 18–36 ____ 37–50____ 51–76____ over 77_____
18. Your gender: male____ female____
19. Your ethnicity: African American __ Hispanic __ Asian__ Caucasian__ Other___
20. County of residence:______________________
Thank you for your participation!
Authors’ Note
IRB approval for the project was obtained through Calvary Hospital including the placement of the flower arrangements in patient rooms.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was made possible through generous funding by Dr. Anne Frost through the Irving A. Hansen Memorial Fund.