
Abstract
Few studies of death preparation in South Korea are available. This article describes South Koreans’ experiences of death and a funeral in a hospital setting to improve health care providers’ ability to care for dying patients and their family. Using Colaizzi’s phenomenological method, we conducted semistructured interviews with 40 South Koreans who had lost a family member in a hospital setting. Participants’ statements were classified into 12 themes, 5 theme clusters, and 3 categories: (a) vagueness of funeral culture, (b) distortion of meaning in funeral culture, and (c) the need to prepare for death and process grief. Our findings are relevant to hospital-based health care providers who care for dying patients and their family. Targeted educational information could help health care providers better serve patients and family. Policy changes could improve quality of care by allowing health care providers to transition with the family from hospital units to a hospital-based funeral setting.
Introduction
Different rituals exist within different cultural contexts. Asian countries with strong Confucian values, such as South Korea, have regarded death as not simply the death of an individual but also the end of all relationships connected to the deceased (Human Understanding Design Center [HUDC], 2016; Park, 2010). In countries influenced by Confucianism, talking about death in public is not common, and talking about death with older adults has been considered impolite (Cacciatore & DeFrain, 2015; Martinson, 1998). Under the Confucian culture, filial duty has helped to develop a strong bond among family members (Lee, 2012), and its concept of filial duty made people avoid talking about someone’s death toward the elderly. Specifically, talking about the death with the parents was regarded as misbehavior or disrespect (Glass et al., 2010). There are old sayings, for example, which was shown the traditional view toward the death in South Korea: “a bad life is better than a good death” (The Korean Folklore Society, 1996, p.133).
In South Korea, dying outside of one’s home was considered negative and a poor death because it was believed that the deceased could not go to the afterlife without a certain period of funeral courtesy (Lee & Lee, 1995). Under Confucian culture, a chief mourner led the funeral who was most commonly the firstborn son of the deceased or the firstborn grandson if the firstborn son died at home. The death ritual happened at a community level, with the help of all community members under the chief mourner’s leading. However, a unique phenomenon in South Korea since the mid-1990s has been a dramatic shift in funeral procedures from home-based to hospital-based settings (Park, 2010). This phenomenon is unlike that in most other countries, including Western countries, where funeral settings are separate from the hospital (Bremborg, 2006; Hayslip et al., 2007).
One main reason for this change was the government’s approval to build hospital-based funeral settings, with the goal of reducing overspending on cemetery land due to Confucian funeral rituals. Furthermore, there was a strong social demand from the mid-1990s to find more convenient places for funerals among families who had a considerably small-sized family with and less infrastructure (Lee & Lee, 1995). Most South Korean funeral practices and facilities are now hospital-based, including 92% of funeral facilities in the capital areas of South Korea (Choi et al., 2019; Park, 2010; Song, 2003). For this reason, understanding funeral procedures and experiences has become more relevant and important to health care providers, including nurses. Clinical health care providers who care for patients at end of life need to be better prepared to anticipate what the patient and family may need to prepare for the death of the individual and the funeral (Hemer, 2018; Wang et al., 2018).
Most previous research has focused on the perspectives of hospice care workers or palliative care providers (Almeida et al., 2014; Johansson & Lindahl, 2012; Kent et al., 2012). One study reported that Korean nurses highlighted enhancing trust, rapport, and pain management as the most important palliative care interventions to support a dignified death (Jo et al., 2011). However, previous research surveying the general population in South Korea reported that knowledge of the cost related to dying and funeral procedures strongly associated with the perception of dying well (Choi et al., 2019). Together, these results suggest that there may be a gap between what health care providers view as important to dignified dying and what the general population thinks is needed to facilitate dignified dying.
An important part of preparing for death is discussing the concept and process of a funeral (Choi et al., 2019; Hsu et al., 2009). How do South Koreans experience a death and a funeral in a hospital setting? The aim of this study was to describe recent experiences of funeral procedures in South Korea and thus to improve health care providers’ knowledge of how to care for dying patients and their family members in a South Korean hospital setting.
Methods
Design
This was a phenomenological study designed to describe and understand the essential nature of the experience of a death and a funeral in a hospital setting to improve health care providers’ ability to care for dying patients and their family.
Sample
Study participants were recruited by convenience sampling by posting flyers at several community centers and hospitals in Seoul, and interested potential participants were assessed for eligibility either in person or through a phone conversation in October 2016. The inclusion criteria were based off those who had lost a loved one within 3 years and had experience as a chief mourner in the ritual, or those who had experiences as a consoler for more than 10 times in rituals. Also included were participants who lived in Seoul metropolitan area and volunteered in this study. Excluded were people who were unable to read or write in Korean or were limited in their activities of daily living such that they were unable to travel to and be interviewed in a private office room. Also excluded were people who were still experiencing grief to the extent that it was affecting their ability to carry out their daily lives.
All study participants were more than 30 years old, were residents of Seoul or the surrounding province of Gyeonggi-do, and had experienced the death of a family member within the past 3 years. To ensure that multiple age groups were represented in our sample, we set a limit of no more than eight participants in each of five age groups: 30 to 39, 40 to 49, 50 to 59, 60 to 69, and older than 70 years. There were 40 participants: 25 male and 15 female. The mean age of the participants was 50.20, and the age range was from 30 to 82. Prior to data collection, institutional review board approval was obtained from Seoul Medical Center in Korea. All participants signed an informed consent form before engaging in this study. All participants were ensured that the interview would be used for this study only, and recordings of the interview would be deleted after finishing data analysis.
Procedure
The interview guide was developed by five funeral ritual experts and HUDC staff. The data were collected for 3 months from the in-depth interviews by HUDC staff and funeral ritual experts including the author Sungwon Park. The overall interviews were directed by the staff.
The initial interview asked open-ended questions based on three main categories of their view of a funeral: participants’ perception of funeral ritual experience, funeral ritual experience, and what they had difficulty in the funeral ritual and needed to overcome it. Generally, questions started “How much do you know about funeral culture?”, “Tell us about a recent experience you had of a funeral and what happened?”, and “What was the most difficult point in preparing for the funeral?” After that, participants were asked more detailed questions: “How do you think about Korean ritual culture?”, “Could you explain why you think about it?”, and “Could you explain more about your experience?” Each interview was conducted in a private room such as an office room in the HUDC, Seoul. Before conducting the interview, we told participants to let us know if they have any discomfort (e.g., temperature of the room, taking a rest) during the interview. The average duration of the initial interview was approximately 1 hour. All interviews were recorded after obtaining the consent of the participants to prevent missing data. When each interview finished, the contents of the interview were transcribed immediately by the researchers who had been trained using the same interview techniques. The transcription of data was reconfirmed with the recordings by all of the researchers to check the level of accuracy. Depending on the content of the interview, one or two additional face-to-face interviews could follow to collect more information when the answers were ambiguous or not enough to analyze, or a phone interview was conducted to clarify the meaning of the interview questions and answers to check if our analysis was aligned with what the participant had intended to say. The recorded file was stored on a USB drive and HUDC’s online platform for 3 years (until October 2019) under the participants’ agreement. The additional interviews took 15 to 30 minutes, but phone interviews lasted 10 to 15 minutes. It was not recorded and used for the purpose of checking members and the created themes created.
Data Analysis
Interview recordings were transcribed verbatim. To ensure confidentiality, participant names were replaced with numbers. Regarding phenomenological analysis, Colaizzi’s (1978) method was used for the analysis (see Figure 1). In the first phase, the transcribed interview contents and the written records of participants’ nonverbal expressions were reviewed, and the impression of the overall experience was examined. In the second phase, investigators as a team repeatedly reviewed the transcripts and extracted sentences that conveyed the essence of the participants’ experiences. After finding phrases or sentences that were repeatedly stated or contained the essential meanings, the extracted sentences were then confirmed by the team and integrated into one sentence. In the third phase, investigators identified the essential meanings in the key statements and rewrote them. In the fourth phase, the general and abstract statements were classified into themes, clusters of themes, and categories for analysis. To classify the statements, investigators held meetings to cocheck the results of the analysis by reading each statement again to confirm the classification of the sentences. In the fifth phase, the themes, clusters of themes, and categories were described in general. In the sixth phase, the essential structure of the funeral culture experience was described through themes, clusters of themes, and categories. Before conducting the seventh phase, all transcripts were reviewed again by the team to reconfirm the results of coding and achieve an acceptable interrater reliability. In the seventh phase, the validity of the analysis of the results was reconfirmed by six selected participants of the study.
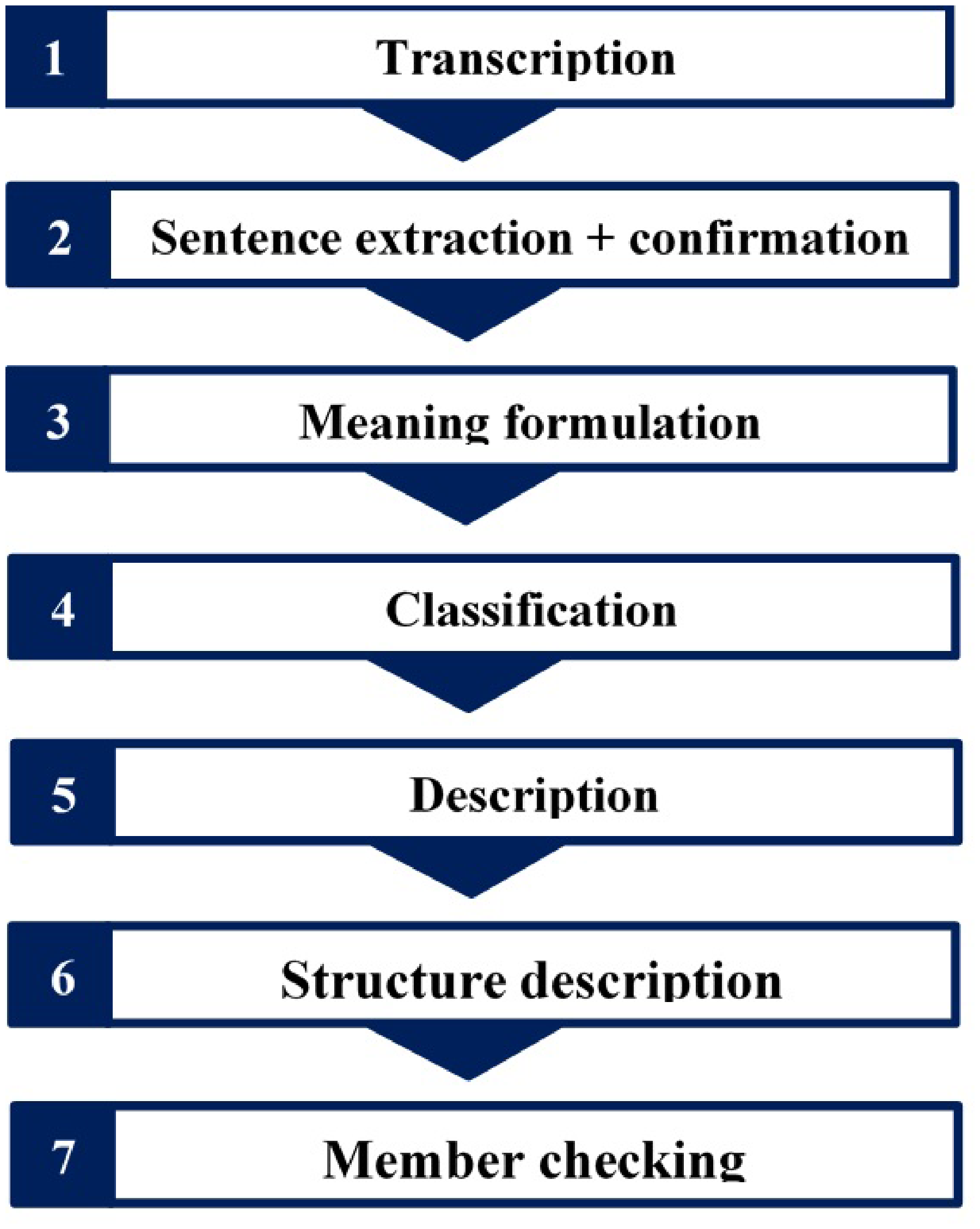
Phenomenological Method of Transcript Analysis Following Colaizzi (1978).
Results
A total of 40 South Korean males and females between the ages of 30 and 82 participated in an individual interview focused on death and funeral experiences as either a chief mourner or a bereaved family member. Of our 40 participants, n = 25 (62.5%) were male, 47.5% were university graduates, and 30% considered themselves to be nonreligious, whereas 70% were religious such as Christian. In addition, 75% were married, and 52.5% had been the chief mourner for the experience discussed in the interview (see Table 1).
Participant Characteristics (N = 40).

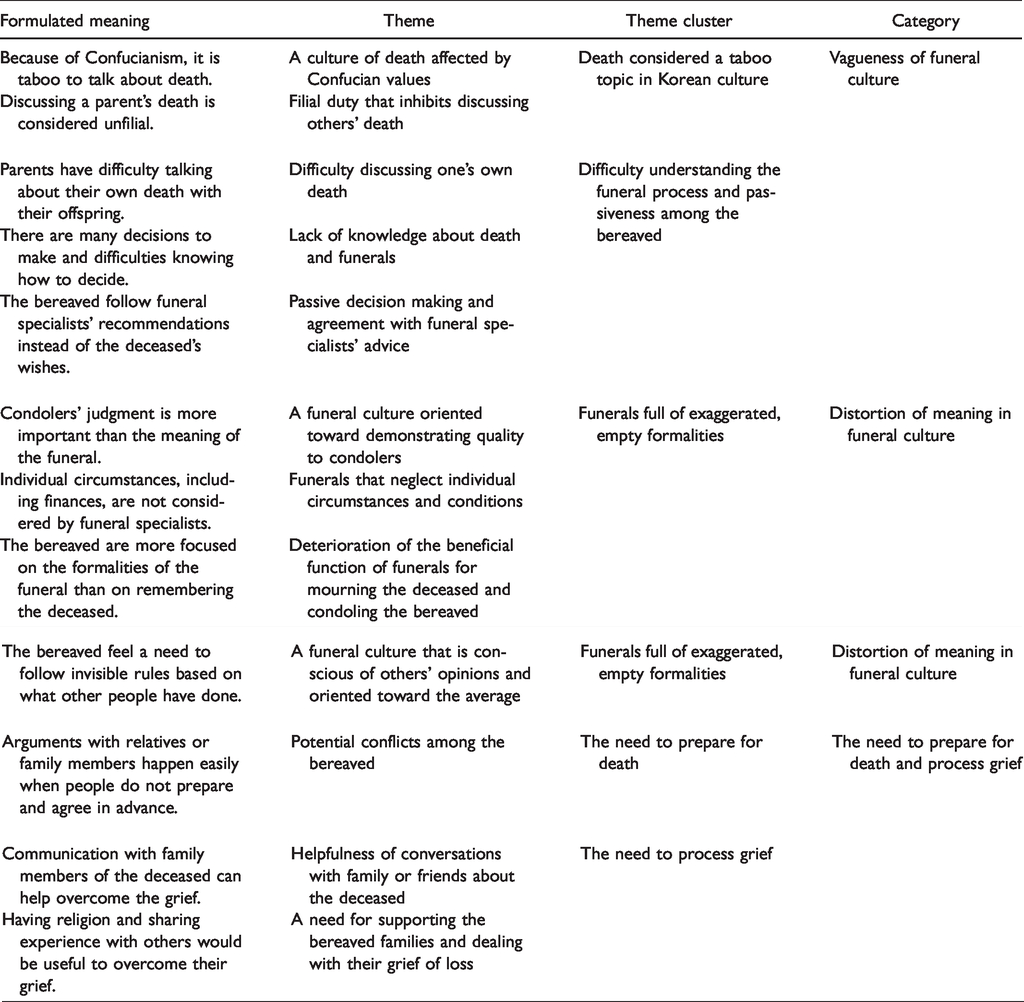
We extracted 418 key statements from the transcribed interviews. These statements were classified into 12 themes, 5 clusters of themes, and 3 categories, as described in the following sections and summarized in Table 2.
Themes, Theme Clusters, and Theme Categories.
Category 1. Vagueness of Funeral Culture
Death Considered a Taboo Topic in South Korean Culture
Three themes were related to this theme cluster: a culture of death affected by Confucian values, filial duty that inhibits discussing others’ death, and difficulty discussing one’s own death. In part due to their traditional Confucian values, study participants who were more than 40 years old said they had difficulty discussing death and also reported a pessimistic perception of death. Confucian culture suggests that, although the spirit survives after physical death, there is no place for the spirits of the deceased to rest. This pessimistic view of the afterlife resulted in participants reporting a belief that people should fully commit to their current life rather than prepare for or embrace death. Participants also mentioned that filial duty in general originates from Confucian culture, indicating the duty for parent’s death lies on descendants such as a son or daughter, was strongly emphasized in South Korean culture and that discussions about death between parents and offspring were considered an unfilial act that could be interpreted as wishing for the parents’ death. This made it even more difficult for participants to discuss death and the funeral process within their family. I gave a lot of thought about death. How I would … . I told myself I should embrace death as another natural part of my life, rather than clinging to life itself. But if I share this thought with my sons and daughters, I think they would believe that I’m thinking in this way because they have not been good enough to me, because they have not fulfilled their filial duty. I do believe it is an act to talk about death like this, both to my deceased parents and as a child of parents too. So, this is why … . I cannot talk (about death) to my sons and daughters. I just keep it to myself. I just hope my sons and daughters do not grieve too much over my death … . I hope not … (Participant 11, 59 years, male, the deceased: mother) Back in the days when I was young, there was a saying that sons and daughters become sinners as their parents pass away. The people of my generation now follow the contemporary funeral practices, but back in the old days, people used to hold funeral rites for three years due to Confucianism. It was just out of the question to talk about death back then. Some of my friends still hold these values. But I’m more open-minded (for a change in the funeral culture). (Participant 2, 68 years, female, the deceased: mother)
Difficulty Understanding the Funeral Process and Passiveness Among the Bereaved
This theme cluster was extracted from these two themes: lack of knowledge about death and funerals, and passive decision making and agreement with funeral specialists’ advice. Most of the study participants said that they did not encounter funerals frequently and did not know much about funeral procedures. They depended on funeral specialists to guide them through the funeral procedures, and they took a more passive role in the funeral themselves. Interestingly, a lack of understanding of the funeral process was reported not only by participants who had lost a family member unexpectedly but also by participants who had foreseen and prepared for the death of a family member who was seriously ill. What I found difficult was … not knowing the people I was supposed to contact and so on. And there were also a lot of things at the hospital that I had to make decisions on (regarding the funeral process). I did not know which were good, which were bad or which were too much, as the whole experience was not the one that I got to have much before. I think most people would go through difficult times when making those decisions in their first funeral experience. (Participant 34, 30 years, male, the deceased: father)
Category 2. Distortion of Meaning in Funeral Culture
Funerals Full of Exaggerated, Empty Formalities
This theme cluster was extracted from four themes: a funeral culture oriented toward demonstrating quality to consolers, funerals that neglect individual circumstances and conditions, deterioration of the beneficial function of funerals for mourning the deceased and condoling the bereaved, and a funeral culture that is conscious of others’ opinions and oriented toward the average. Participants stated that the funeral rituals are more focused on performances by family members, not on consoling the bereaved, and that they rely on empty formalities. The bereaved who participate in the funeral appear to be more conscious of how others think and judge them during the proceedings rather than of being sincerely respectful of the deceased. There should indeed be some formality in the process of funerals, but certain aspects have become just too formal … . That makes them depend on the average or standard (to be prepared the funeral ritual), following how others do. I think this is why the mourning for the deceased or consoling the bereaved became comparatively less significant. The outward quality-oriented nature of the funeral culture itself has become the problem. (Participant 21, 29 years, male, the deceased: grandfather) In the process of considering the funeral’s costs and conditions, people often end up paying much attention to the formality. I think what is most important in the end for the bereaved is the way other consolers think and judge them. Things such as formality and custom, or other societal aspects lead to an excessive and exaggerated form of funerals. (Participant 25, 57 years, male, the deceased: father)
Category 3. The Need to Prepare for Death and Process Grief
The Need to Prepare for Death
This was related to the one theme: potential conflicts among the bereaved. Participants who had had prior discussions and had arranged for funerals in advance reported that they did not experience discord or conflicts within the family and that they were able to support each other in overcoming hardships after the funeral. However, participants who did not have prior discussions reported serious discord or conflicts within the family, and some described the dissolution of relationships. Participants suggested that, if people are given the chance to prepare for death in advance, either alone or as a family, it would make the funeral process less difficult and decrease the probability of familial conflict. I do not see it (death) happening anytime soon, but I do think we need to be prepared (for death). We had arguments (with kin) because we were not prepared (in advance for death). There was a massive conflict. We were all very disgruntled at each other on the day of the funeral and were on the verge of blowing up right after the funeral … . The funeral culture, in my experience, led our family to fall apart. Others around me, 8 out of 10, also went through the same experience. (Participant 8, 39 years, female, the deceased: husband) In my case, my family and I had discussed the place of burial in advance and decided to handle the death of my mother according to the situation when it happened. My mother had asked us to bury her when she died because she dreaded going into the fire even after she died. In my opinion, we need to discuss death and funeral procedures before like my mother did. That’s why my family and I did not argue with each other. Even though I was sad after my mother died, I was able to overcome my grief with the emotional support from my family. (Participant 16, 38 years, male, the deceased: grandfather)
The Need to Process Grief
This was related to the two themes: helpfulness of conversations with family or friends about the deceased and a need for supporting the bereaved families and dealing with their grief of loss. Participants reported that their amount of grief was high immediately after the passing of their family member. To help process their grief, they turned to other family members, to other people with similar experiences, or to religion. Among these various methods, sharing memories of the deceased with other family members was reported to be the most helpful. In addition, some participants identified a need for special programs that would help family members process grief and return to their daily lives. It (the grief) fades away to some degree over time (after the passing away of the loved one), but at the time of the lost, the grief I felt was just too immense. I thought it would be helpful to undertake psychological counseling (after the passing of the loved one), but I ended up not taking it as the perception of psychological counseling was quite negative in my country. What was fortunate was that my family members actively communicated with each other and we went on a trip together (as a means to overcome the grief). During that period, we talked about my mother a lot by sharing beautiful memories we had when she was alive, and focusing on the happy times with her made us smile. I think that is how we managed to overcome the grief of losing our loved one. The bond in the family has become stronger ever since. If we were not there for each other, it would have been hard for us all to deal with the death. (Participant 16, 38 years, male, the deceased: mother) I could also find peace by talking to others with the similar experience (of funerals). I could see that I was not the only one suffering from the grief and that I could overcome it … and such. In addition, at first, we rarely talked about my mom just after finishing the funeral to overcome the grief. After a while, with my sisters, we talked about how grateful we were what our mom did for us, and that was quite comforting. (Participant 35, 40 years, female, the deceased: mother) First of all, support and consolation within family. I talked to my husband a lot. We had many conversations about the memories of my dad whilst we were going through the belongings and mementos of my dad. Second, maybe because I was a religious person, but communicating with the people with the same faith also helped me. I had a belief (that my father went to a place of peace and love). As for me, if the support from my family and my religious faith were not there, I would have never been able to overcome the grief as I did now. (Participant 36, 47 years, female, the deceased: father)
Discussion
This phenomenological study explored participants’ experiences of a death and a funeral in a hospital setting in the hospital in the cultural context of South Korea. Themes identified included vagueness in the current and changing funeral culture, loss and distortion of meaning in funeral culture, and lack of preparation for death and for overcoming grief.
The first and second theme categories—vagueness of funeral culture and distortion of meaning in funeral culture—are closely related to South Korean culture. To change the negative perceptions of death in South Korean culture, individuals’ perception of death must change. A previous study of Lee and Kim (2018) that explored funeral culture among 500 South Koreans reported that 76% of participants said they had not prepared for their funeral or death. Because funeral culture and funeral facilities are perceived as unwanted facilities, participants did not prepare for their own death and funeral though they were aware of the necessity of preparation for death and a funeral (Lee & Kim, 2018). health care providers are in a position to support patients and family members in the hospital in understanding what aspects of the funeral culture will be important to them as they go through death and funeral procedures. In the study of Han (2019), it was noted that special assistance was needed from health care providers by the patients and families for both medical and nonmedical decisions, such as death preparation, funeral procedures, family issues, and economic support. In terms of “death preparation” was to the meaning of prepare for the funeral procedures, which was drawn directly from the interview contents.
The third theme category in our study demonstrated participants’ need to prepare for death and to process grief. Prior education on death, beliefs, and culture influences individuals’ preparation for and attitudes toward death (Wang et al., 2018). For a dignified death, people desire to prepare for death, including leaving a will and knowing the process of funeral or death before an unexpected death might happen (Kim et al., 2003). Lack of understanding of death preparation needs may lead health care providers to misunderstand the care and information that families and patients need for a dignified death in South Korea, which research indicates including a keeping beautiful memories about the deceased and placing no burdens on their families or friends (Chung & Cho, 2017; Gordon et al., 2014). Thus, research is needed to better understand the current culture of death preparation and funeral practice in South Korea and to inform hospital nursing practice. In addition, global trends show a departure from the ideology of death as taboo and a movement toward preparing for death (Gordon et al., 2014). In alignment with this trend, South Koreans have also been moving toward talking more about death in advance, but there is still a traditional cultural expectation that people, and especially men, should not been seen expressing their emotional feelings, such as sadness or grief, in public (Park & Jo, 2002). This expectation may be similar in other countries with a Confucian culture, including first-generation South Korean immigrants, who often pursue connections and alignments with their South Korean cultural and social heritage (Jo & Doorenbos, 2009a).Global trends show a departure from the ideology of death as taboo and a movement toward preparing for death (Gordon et al., 2014). In alignment with this trend, South Koreans have also been moving toward talking more about death in advance, but there is still a traditional cultural expectation that people, and especially men, should not been seen expressing their emotional feelings, such as sadness or grief, in public (Park & Jo, 2002). This expectation may be similar in other countries with a Confucian culture, including first-generation South Korean immigrants, who often pursue connections and alignments with their South Korean cultural and social heritage (Jo & Doorenbos, 2009a).
Based on our three categories of themes, three types of interventions can be recommended: (a) community interventions to begin conversations about death and funeral procedures, (b) education on funeral processes, funeral experiences, and funeral aftercare for health care providers working in hospitals, and (c) policy changes in hospitals. Community-level engagement in conversations about death and funeral processes is one way to promote change in the general population and culture. One of the more efficient ways to change negative perceptions of death among patients in hospitals is education on death preparation (Kang, 2011; McClement et al., 2007; Wang et al., 2018).There is a gap between humanistic death education and the current situation in which most deaths occur in hospitals in South Korea because current education is based on the premise of a natural death. Thus, people cannot prepare for death practically because they tend to overlook funeral procedures and decision making for a funeral (Suh, 2016). Because there is a lack of practical education and a negative perception of death and funeral culture, people are inhibited from being provided the proper education on death and funerals. Therefore, it is necessary to improve negative social perceptions of death.
In the United States, Five Wishes (Fivewishes.org) is an advance care planning organization that offers training and resources and promotes community-based conversations. The Five Wishes conversation guide for individuals has been translated into South Korean and is available for use in the community. Considering the South Korean community context, there also appears to be a need to establish culturally acceptable community programs that address the vagueness of funeral culture and distortions of meaning in funerals. We recommend developing a death preparation program for healthy people in the community, such as a modified version of the Five Wishes questions aligned with the South Korean context.
In addition, education on death and the funeral process should be provided to health care providers, as nursing staff have the most interaction with patients and family members during the dying process. Patients and families look to health care providers when they need explanations about death and funeral procedures. In other words, education is needed on the funeral process and aftercare, such as how to help families overcome grief. Studies by Kang (2011) and McClement et al. (2007) have shown that death preparation training helps reduce death anxiety for patients as well as for family members. A recent systematic review found that education and emotional support provided to the bereaved helped them process their loss and grief (Wilson et al., 2017). Aligned with these previous studies’ results, some participants of this study answered that the emotional care and preparation of a loved one’s death was helpful for overcoming the grief. Although grief is a natural phenomenon of experiencing the death of someone such as a family member, participants need information on which types of help can reduce their grief from health providers. In previous studies, nurses’ awareness of differences in customs and rituals among those who are grieving may influence the nursing care provided (Clements et al., 2003; Hemer, 2018). Education would enhance health care providers’ abilities to support patients before death and to support the bereaved family afterward. Based on the results of this study, education is needed for how to perceive death and what kind of support can help for the family of the bereaved to overcome grief. At the same time, the family needs to be informed of the funeral procedures to improve their ability to manage the funeral from the beginning.
Health care providers should be educated to be considerate of cultural differences and accept their patients’ attitudes when they talk about death preparation with patients and family members in the hospital setting. Education of practicing health care providers is important and should include respect for traditional death rituals, sacred space, and religious and cultural concerns that comfort the family and demonstrate respect for the deceased. For instance, fundamental elements of death education need to include understanding the meaning of death among Koreans, death and the religious afterlife, the acceptance of death affirmatively, ethical issues related to the process of dying, and decisions on what to leave behind (Kim et al., 2014).
Based on the results of this study, health care providers should be informed and educated about the experiences of a death and a funeral in a hospital setting. First, they need to learn how to assess their patient’s and family’s attitude toward death and the factors influencing their attitudes and how to change any negative attitude about death. Second, they need to gain knowledge of funeral procedures and use this knowledge to explain the process of death and funeral procedures. Last, health care providers should learn how to and be able to provide concrete ways of overcoming grief. Thus, recommendations for health care providers’ education could improve the health care quality for patients and their family members. In addition, the study recommendation could extend to apply for health care providers in hospitals that serve South Koreans, South Korean immigrants, or patients from other Confucian cultures.
We also recommend that hospital policies be updated to ensure that health care providers have enough time and support to provide care to dying patients’ and their family members, regardless of hospital unit. Hospital policy should also focus on health care providers’ capacities because it is nurses who care for dying patients and need to educate family members as well as patients about preparing for death and a funeral to support dignified dying (Jo & Doorenbos, 2009b).For example, each hospital unit could create a space where dying patients can pass away with family members under a health care provider’s guidance. In addition, policy could be changed so that health care providers could continue supporting the family members until they have fully transitioned to the hospital-based funeral setting.
Limitations
This study focused on South Korean culture and their funeral context. As this study had current Korean funeral culture as its background, our findings may not be generalizable to other cultures. Other Confucian cultures may have different funeral experiences because South Korea changed funeral policy in the mid-1990s. The result of this study could be biased because more male participants joined this study, especially as the role of a chief mourner.
Conclusions
This study used a phenomenological approach to explore experiences of a death and a funeral in a hospital setting in South Korea. The study participants described having a difficult time with the vagueness of current funeral culture, distortion of meaning in the funeral culture which means focusing on the ritual preparation more than missing a spending time with a loved one who deceased, and lack of knowledge about how to prepare for death and process grief. Notably, most of the key statements that participants reported were associated with funeral rituals. Although we make preliminary recommendations based on our results, further studies are recommended, including studies on how to facilitate community conversations regarding death and funeral processes. Other possible future directions include focusing on teaching cultural competency regarding funeral rituals and death preparation to health care providers. health care providers have an important role in caring for dying patients and their family members and are in a key position to make a difference during death preparations. A basic knowledge of South Korean funeral procedures and rituals could help health care providers in South Korea provide better care for patients as well as families. To better support the unique cultural aspects of South Korean funerals, we recommend customized education and programs regarding death preparations at the community level, education for health care providers, and hospital policy changes that support health care providers’ capacity to provide education on death preparation and to help families transition to the funeral setting.
Footnotes
Acknowledgments
The authors are thankful to HUDC staff for sharing the data and for Hyunjong Kim, the director of HUDC, for supporting the study. Also, the authors express their appreciation to those who collected the data—Hansol Paeng and Seulgi Ku—and funeral ritual experts including Dr. Phildo Lee.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The content is solely the responsibility of the authors and does not necessarily represent the official views of the Seoul Medical Center or the National Institutes of Heatlh.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was major supported by the 2016 ‘User Research Study for Improving Funeral Culture Service’ project of Human Understanding Design Center, Seoul Medical Center. Additionally, this work was supported by the National Institute of Nursing Research of the National Institutes of Health (award number K24NR015340).