
Abstract
Aortic dissections and aneurysms (ADA) are associated with significant morbidity and mortality, and location of death for these patients is important in determining impact on end of life care. We analyzed the Centers for Disease Control and Prevention Wide-ranging Online Data for Epidemiologic Research database. Black and Hispanic backgrounds had decreased odds of dying at home from ADA. Married or educated individuals tended to die at home at a higher rate than unmarried individuals. Overall, we have shown place of death in individuals with ADA is different among individuals of different demographics.
Aortic dissections and aneurysms (ADA) are associated with significant morbidity and mortality (Pacini et al., 2013). Despite preventative measures, death remains imminent in these patients (Pacini et al., 2013). The location of death is an important determinant of end-of-life experience (Cross et al., 2019). Recent data show decedents dying at home has surpassed the hospital in United States in 2017 (Cross et al., 2019). In perspective, it is imperative to analyze the place of death for patients with ADA.
We analyzed the Centers for Disease Control and Prevention Wide-ranging Online Data for Epidemiologic Research database. Data of ADA related cause of mortality was selected from year 2004–2017 using International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD 10 codes; I71). We included natural deaths between 2004 and 2017 for which ADA was identified as underlying cause of death or initiated the events directing leading to the death as demarcated by the death certificate. These variables were examined: place of death and demographic characteristics, i.e. age, ethnicity, race, education, and marital status. Chi-squared test was used for categorical variable and association with place of death was assessed using multivariable logistic regression model.
Between January 1, 2004 and December 31, 2017, 155,745 deaths were attributed to ADA. Of which 3.7% were Hispanics, 87.1% Whites, 9.6% Blacks, 2.8% Asians, and 0.4% American Indians. Over the years, deaths rates significantly increased in females (40.8 to 41.6%), Blacks (8.9% to 10.7%), Asians or Pacific Islanders (2.2% to 3.6%) and American Indians (0.3% to 0.5%); and decreased in males (59.2 to 58.8%), and Whites (88.6% to 85.2%) (P < 0.001). The overall proportion of deaths in the hospital decreased from 60.3% to 51.4%, while it has increased at home from 11.9% to 17.0% and at hospice from 0.1% to 3.4%. Older decedents had higher odds of dying at nursing home and hospice compared with younger decedents (Table 1). Compared with men, women had higher odds of dying at a nursing home and hospice. Conversely, Hispanics had higher odds of dying at a hospital and lesser odds of dying at home, nursing home and hospice compared with non-Hispanics. Similarly, compared with Whites, Blacks had higher odds of dying at a hospital and lesser odds of dying at home and nursing home. Decedents with higher education and those who are married had higher odds of dying at home.
Association Between Place of Death and Decedent Characteristics (Odds Ratio [95% CI]).
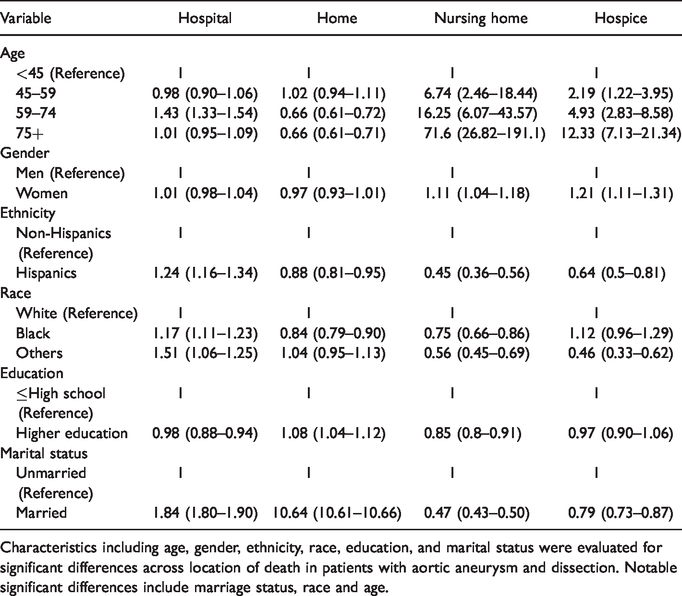
Characteristics including age, gender, ethnicity, race, education, and marital status were evaluated for significant differences across location of death in patients with aortic aneurysm and dissection. Notable significant differences include marriage status, race and age.
Our analysis provides novel insights into the end-of-life experience of patients who die from ADA. Literature shows disparities tend to play a role in end-of-life care (Welch et al., 2005). Our data shows decedents from Black and Hispanic backgrounds have decreased odds of dying at home from ADA, despite that being the location preferred by patients. More men died at home compared to women in several studies including ours (Washington et al., 2015). Literature suggests women tend to be in the caregiver’s role more often than men (Washington et al., 2015). We noted a significant difference in place of death among decedents with certain social stratifications. Our data are concordant with the literature suggesting that marriage plays a significant role in health outcomes (Robards et al., 2012). Married individuals tended to die at home at a strikingly higher rate than unmarried individuals suggesting a role for having a medical decision maker or caregiver be a spouse. These data are also suggestive of the association of higher education with higher health care literacy and decision-making. It appears that educated patients may be better at expressing their wishes to die at home as reflected in our data. Further research is needed to elucidate if racial, ethnic, or educational disparities in location of death represent a lack of access to home supports or hospice services, or if they reflect differences in culture and care preferences.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.