
Abstract
This study aims to extend our knowledge regarding attitudes toward euthanasia. Specifically, the effect of patient’s age and illness type. 123 participants were randomly assigned to 1 of 4 groups completed the Assessing Right to Die Attitudes (ARDA) questionnaire after reading a patients age (79 vs. 29 year old) and illness type (cancer vs. depression) description. Findings revealed more positive attitudes toward euthanasia when the patient was physically ill, as opposed to mentally ill. Participants’ attitude towards euthanasia was more positive when the patient was elderly. Illness type as a function of the patient’s age did not significantly influence attitudes towards euthanasia. The results of the current study reinforce the individual influence of illness type and of patient age on attitudes toward euthanasia, and suggest additional avenues for further research regarding their combined influence.
One of the most important issues on the public agenda in Western countries and in the State of Israel is euthanasia. Developments in medicine and healthcare enable us to prolong the lives of people suffering from incurable illnesses for many years, though their quality of life may be significantly impaired, and they do not necessarily want to extend their lives (Yun et al., 2011). In addition, people attribute great importance to quality of life and often want to control the time, location, and method of their own death (Schroepfer et al., 2009). This creates a conflict between the value of preservation of life through medical healing and treatment, and personal autonomy that may undermine this value (Boudreau & Somerville, 2014).
The term “euthanasia” originates from the Greek word “euthanatos”, meaning “good death” (Reichenberg, 1987). Euthanasia refers to the intentional cessation of a person's life, usually at his or her request (though not necessarily), due to terminal illness and/or incurable suffering (Sanson et al., 1998). Euthanasia is a highly controversial issue. Its opponents consider life to be a supreme value and claim that humans do not have the right to end their own lives or help others end their lives. On the other hand, advocates argue that value of life cannot be separated from quality oflife, and that a person has the right to make decisions regarding his or her own life. Therefore, a life of suffering can justify the decision to terminate it (Broeckaert et al., 2010; Roelands et al., 2015).
Two main distinctions on this matter in the legal and medical literature relate to types of euthanasia and the patient’s wishes. Euthanasia can be either active or passive. Active euthanasia means taking action to terminate a patient's life, whereas passive euthanasia refers to withholding medical care that can prolong the patient's life, or stopping existing treatment. As for the patient's wishes, there is a distinction between voluntary and explicitly choosing euthanasia (When the patient has a clear mind and has the ability to make conscious decisions) and how it will be applied, as opposed to involuntary euthanasia at a stage in which the patient is unable to make a decision by himself, and instead it is the spouse or legal guardian who make the decision (Sanson et al., 1998).
According to Nortje (2013), attitudes toward euthanasia are more complex than taking a stance for or against euthanasia, and are influenced by a variety of factors. The extent to which a person accepts or rejects the possibility of euthanasia may depend in part on his or her religious beliefs (Aghababaei et al., 2011), which may affect his or her decisions and behaviors (Caddell & Newton, 1995). Some religions believe that if an individual does not value future life, death is an acceptable alternative, while other religions condemn taking life under any circumstances, claiming this to be immoral (Allen et al., 2006). It seems that people who are not affiliated with religions that consider actively ending life to be unacceptable, tend to be more supportive of euthanasia (Caddell & Newton, 1995). On the other hand, the stronger the person’s religiosity or conscience, the greater their negative attitude towards euthanasia (Aghababaei et al., 2011).
Active euthanasia is illegal in most countries, but there are several countries in which legislation permits it under certain conditions, such as in the Netherlands, Belgium and Luxembourg. These countries even allow euthanasia for those suffering from mental illnesses (Demedts et al., 2018; Thienpont et al., 2015). In Canada, euthanasia is legal and permitted for patients suffering from terminal illnesses that cause unbearable physical or psychological suffering. Nevertheless, the use of euthanasia in mental illnesses patients is still controversial since they are not considered as a terminal ill (Statutes of Canada, 2016). There are also countries in which legislation allows physician-assisted suicide, defined as intentionally using lethal drugs following a patient's request (Materstvedt et al., 2003), such as Switzerland and the United States (Radbruch et al., 2016).
Jewish tradition attributes supreme moral value to the preservation of life, and forbids artificially shortening human life (Kinzbrunner, 2004). On the other hand, Jewish tradition does not require prolonging life using artificial means, and therefore passive euthanasia is permitted (Richards & Bergin, 2000). In 2005, the 'Dying Patient Law' 1 was enacted in Israel, prohibiting active euthanasia, assisted suicide, and termination of continuous medical care. However, the same law allows cessation of non-continuous treatment and withholding treatment that can prolong human life under certain conditions (Jotkowitz & Glick, 2009; Schicktanz, Raz & Shalev, 2010). The process of recognizing physician-assisted suicide began in June 2014, when the Knesset Legislative Affairs Committee approved a physician-assisted suicide bill that permits physicians to provide a lethal injection for terminally-ill patients who have reached the last six months of their lives. However, this proposal was rejected by the Knesset in 2016 (Schweda et al., 2017).
The type of disability is another factor that affects attitudes towards euthanasia. Disability is a broad term that encompasses ideologies regarding what constitutes a non-normative and socially non-ideal existence, and what is deemed incompatible with cultural standards (Robinson-Wood, 2009). The concept of disability is shaped by socio-cultural, institutional, and political factors (Moore & Feist-Price, 1999). Disability can include a variety of impairments – physical, cognitive, sensory, developmental, psychiatric, and a combination of these. Socialization processes associated with negative thoughts and feelings about disability have been shown to affect life satisfaction among peoples with disabilities (Alston, Harley & Middleton, 2006).
Society holds stereotypes about illnesses and disabilities, and particularly about psychiatric disabilities (Smart, 2009). There tend to be more negative stereotypes about mental illness than about physical illness (Imhoff, 2016). This may be due to the prevalent ambiguity regarding mental disabilities and the difficulty in understanding them, as opposed to physical illnesses that are more understandable to society (Smart, 2009). One stereotype is related to the autonomy of patients and their ability to make informed decisions about their lives, including about their medical care (Blackhall et al., 1995). People with physical illness are perceived by others as more autonomous in making decisions about their lives, compared to those with mental illness (Angermeyer et al., 2013).
One of the reasons terminally ill patients request euthanasia is because of their fear of losing control over their lives (Schroepfer et al., 2009). This fear of losing control and independence has been found to be greater than the fear of death itself among terminally ill patients (Hough, 2010). Corrigan et al. (2000) found that people with schizophrenia or depression feel a greater sense of control regarding the outcome of their treatment (e.g. hope, resilience, better chances of recovery) than cancer patients, and therefore euthanasia is perceived as more legitimate for cancer patients. Social acceptance is another factor perceived as affecting attitudes toward euthanasia, and is defined as the extent to which a person is perceived as worthy of integration into social groups (Martin et al., 2000). The public tends to socially distance individuals suffering from depression more than patients with physical illness (Link et al., 1999). Hence, it can be concluded that the more socially acceptable the illness, the greater the legitimacy of euthanasia.
Another distinction that has been identified is between suffering from a terminal illness and suffering from a non-terminal illness, while euthanasia process is perceived as more complex for patients suffering from non-terminal illnesses (Smets et al., 2010; Steck et al., 2013) such as unbearable mental suffering due to a psychiatric disorder (Cohen et al., 2014). It is more difficult to assess the degree of suffering from a mental illness than from a physical condition, which is more measurable (Behaegel et al., 2015; Liégeois, 2013). Moreover, the complexity of assessing the patient's mental competence makes it more difficult to determine whether a psychiatric disorder can be cured, compared to physical illness (Cohen et al., 2014). In addition, the course of some mental illnesses includes periods of remission in which the individual experiences diminution of the symptoms (American Psychiatric Association, 2013). These periods of remission make it difficult to legally define a medical condition as untreatable (Shaffer et al., 2016). Moreover, personal decisions can be more complicated in cases of severe mental disorders (Owen et al., 2013), as desiring death may be a part of the disorder itself (Cohen et al., 2014).
Overall, in most developed societies, despite traditional religious and legal prohibitions regarding ending human life at the individual’s request, euthanasia receives public support (Emanuel et al., 2016). Empirical evidence showing support for euthanasia is based on research of physical and terminal illnesses such as cancer or advanced neurological diseases (Schuklenk & van de Vathorst, 2015; Wilson et al., 2000). At the same time, the perceived minimal autonomy of mentally ill patients causes a lack of support for euthanasia in cases of mental illness (Rae et al., 2015).
Another variable that influences attitudes toward euthanasia is patient age. Studies show that there is greater legitimacy for euthanasia for elderly patients (Frileux et al., 2003; Van Holsteyn & Trappenburg, 1998). A study conducted in the Netherlands between 1984–1993 showed that the average age at which euthanasia was performed in men was 62 years (range 15 – 94 years), with the decade of life in which euthanasia was most prevalent being 60–69. Among women, the average age was 65 years (range 17 – 95 years) and the prevalent decade being 70–79. One of the explanations for this was the tendency to think that the elderly suffer from more terminal illnesses than younger people (Onwuteaka-Philisen et al., 1997). In addition, society perceives older people as having more control over their life decisions. A study conducted in the US among mental health profession students showed that students were more supportive of active euthanasia for elderly patients than for young ones. One explanation for this was their belief in the elderly person’s autonomous ability to make life-ending decisions (Bevacqua & Kurpius, 2013).
The stance of the Israeli public regarding active euthanasia and physician-assisted suicide is unknown and there the minimal research available on this topic covers mainly doctors and nurses. Wenger and Carmel (2004) found that 44% of doctors support legalization of active euthanasia. Among nurses, it was found that 63% support active euthanasia, and 85% support it when the patient is suffering (Musgrave et al., 2001). A qualitative study carried out among social workers found that they believe that one must not lose hope to save a patient's life, even when it seems hopeless (Leichtentritt, 2011). A study conducted in 2006 examined social science students' attitudes toward euthanasia based on their degree of religiosity and the type of euthanasia (passive or active). It was found that degree of religiosity influences attitudes toward euthanasia, so that more religious students are less supportive of euthanasia than the more secular ones (Soen, 2005). The goal of this study is to help expand existing knowledge about attitudes towards euthanasia among the Israeli public in general and particularly among students, while examining the effect of illness type and patient age on their attitudes.
In light of the positive attitudes toward euthanasia in relation to physical illness compared to mental illness (Levin et al., 2020) and to older versus younger patients (Bevacqua & Kurpius, 2013), and especially considering the prevailing belief that elderly people’s illnesses are more terminal, while in the cases of younger patients there is greater hope for healing and recovery (Onwuteaka-Philisen et al., 1997), the purpose of the current study is to examine how illness type and patient age influence the participants’ attitudes toward euthanasia. Based on findings from previous studies, our first hypothesis refers to the connection between illness type and attitudes toward euthanasia, so that attitudes will be more positive regarding patients with physical illnesses. The second hypothesis refers to the relationship between patient age and attitudes toward euthanasia, so that attitudes will be more positive with regard to an elderly patient. The novelty of the present study is its examination of the combined effect of these two variables on attitudes toward euthanasia. Thus, our third hypothesis considers the differing attitudes toward euthanasia as a function of illness type and patient age, so that regarding older patients, the gap in attitudes towards euthanasia between cases of mental and physical illness will be greater than the gap when comparing these types of illness among young patients.
Patient age and illness type will be presented by case descriptions of patients aged 77 or 29, with either cancer or depression. Attitudes toward euthanasia will be assessed based on a measurable score in the Assessing Right to Die Attitudes (ARDA) questionnaire (Rogers, 1996). According to the research hypotheses, participants who read a case description of a patient suffering from cancer will receive a higher score on the ARDA questionnaire than those who read a case description of a patient suffering from depression. In addition, participants who read a case description of a 77-year-old patient are expected to score higher on the ARDA questionnaire than participants who read a case description of a 29-year-old patient. Furthermore, the expectation is that among the participants who read descriptions of an elderly, 77-year-old patient with either cancer or depression, there will be a larger gap in the ARDR questionnaire scores in favor of cancer compared to participants presented with a 29-year-old patient.
Method
Participants
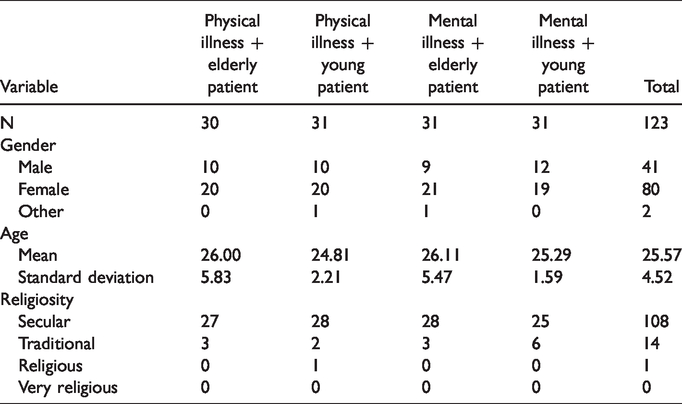
The current study included 123 undergraduate Social Science students, of whom 80 were women, 41 were men and 2 indicated their gender as “other”. Student ages ranged from 20 to 56 (M = 25.52, SD = 4.19). The students were recruited through social networks and participated voluntarily or for an academic credit. They were randomly assigned to the different experimental conditions.
Measures
Patient age and illness type was defined using case descriptions that were adjusted for the current study and were based on the case descriptions used in the Levin et al. (2020) study. Each description presented an ill man who was suffering terribly and wanted to end his life by active euthanasia. The differences between the case descriptions were in the independent variables, resulting in four conditions: a 77-year-old cancer patient, a 77-year-old depression patient, a 29-year-old cancer patient, and a 29-year-old depression patient.
To measure attitudes toward euthanasia, participants were asked to fill out an attitude questionnaire on euthanasia. The questionnaire used was the Hebrew version of the Assessing Right to Die Attitudes (ARDA) questionnaire (Rogers, 1996), which was developed by Rogers (1996) and translated specifically for the current study using a repeat translation procedure. The original ARDA questionnaire was used to measure attitudes toward euthanasia after manipulating the case descriptions used in Levin et al. (2020). The ARDA questionnaire is a 21-item self-report questionnaire depicting attitudes toward euthanasia. Responses were measured on a Likert scale ranging from 'strongly disagree' (1) to 'strongly agree' (7). For example: “Euthanasia gives Peter a chance to die with dignity”. The scale was generated by calculating the mean scores for all 21 items, after reversing inverted items (2, 4, 6, 11, 13, 16, 17, and 21, e.g., “Taking Peter's life is wrong no matter what the circumstances”). In the current study, the Hebrew version of the ARDA questionnaire demonstrated satisfactory internal consistency, with Cronbach's α = .73.
Procedure
Participants were randomly assigned to one of the four study conditions and fill in the ARDA questionnaire regarding attitudes toward euthanasia, and to fill in socio-demographic information.
Results
Before examining the hypotheses of this study, we analyzed whether the demographic variables (i.e., age, gender, and degree of religiosity) correlated with attitudes toward euthanasia. Pearson correlation was used to analyze the relationship between participant age and attitude toward euthanasia, but no such relationship was found (
Descriptive Statistics of Study Group Variables.
Two-way analysis of variance, 2 (physical/mental illness) * 2 (elderly/young patient), was conducted to test the effect of these variables on participants' attitudes toward euthanasia. The mean scores and standard deviations of attitudes toward euthanasia, as a function of illness type and patient age are presented in Table 2. In accordance with the first hypothesis, which predicted a more positive attitude towards euthanasia in cases of physical illness, the main effect for illness type yielded an F ratio of F(1, 122) = 32.001, p < .001, indicating a significantly more positive attitude towards euthanasia in cases of physical illness
Mean and Standard Deviation of Attitudes Toward Euthanasia, as a Function of Illness Type and Patient Age.
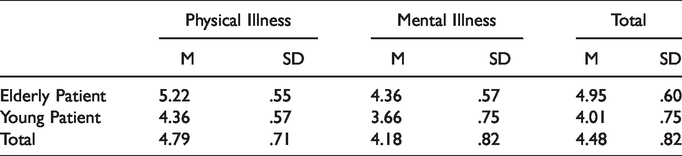
In line with the second hypothesis, which predicted a more positive attitude towards euthanasia regarding elderly patients, the main effect for patient age yielded an F ratio of F(1, 122) = 75.751, p < .001, indicating a significantly more positive attitude towards euthanasia when it came to an elderly patient (
Contrary to the third hypothesis, there was no statistically significant interaction between the combined effects of illness type and patient age on attitudes toward euthanasia (P>.05). No significant differences in attitudes towards euthanasia for elderly versus young patients were found based on the illness type variable, although the interaction was found to lean in the direction of the hypothesis.
Discussion
The purpose of the present study was to examine the relationship between illness type and patient age on attitudes toward euthanasia, following previous studies that have shown how each of these variables separately effect attitudes toward euthanasia.
Consistent with the first hypothesis, our findings show a more positive attitude toward euthanasia regarding patients with physical illness compared to patients with mental illness. Similar to this finding, a study conducted in Canada regarding students’ attitudes toward physician-assisted euthanasia found significant support for patients with physical illness (multiple sclerosis) versus mental illness (schizophrenia or depression), while the latter were perceived as experiencing less suffering than the former (Davidson, 2017). Similar results were also seen in Kouwenhoven et al. (2013), in which physicians and nurses in the Netherlands showed greater support for euthanasia for cancer patients than for patients with chronic depression, on the grounds that physical illness is perceived as more difficult or, alternatively, more legitimate for euthanasia. In addition, qualitative differences were seen in attitudes toward personal requests for euthanasia, based on types of illnesses that could affect the stance of the individual. For example, attitudes toward people suffering from a terminal medical condition who were expected to die in the near future, differed from attitudes toward people perceived as physiologically healthy with a depressive disorder, who requested their own death (Gopal, 2015). A possible cause is the apparent external suffering caused by physical illness that is often lacking in mental illness and may be related to stereotypes about mental illness (Hewitt, 2013). Therefore, the public should be made more aware of the severity of mental illness, however, in a manner that will be beneficial to these patients without reinforcing the negative stigmas against them.
Despite the significant difference in attitudes towards euthanasia for physical versus mental illness, one can see that the overall attitude towards euthanasia in cases of mental illness in the current study is positive. A study of psychologists in Canada found greater support for euthanasia for physical versus mental illness. However, the results were surprisingly positive, indicating that 28.9% of psychologists supported or expressed a neutral stance on euthanasia for mental illness (Karesa & McBride, 2016). Possible explanations for the results obtained in the current study may be related to the characteristics of the participant sample. First, all subjects are college students, i.e. people acquiring academic education. Higher education has been found to correlate with fewer stereotypical social attitudes, especially in relation to mental illness (Eisenberg et al., 2009). In addition, this positive stance can also be explained by the young age of most participants in the study. Studies show a negative correlation between participants’ age and attitudes toward euthanasia, so that support for euthanasia decreases with age (Lee et al., 2017; Velan et al., 2019). It is possible that the higher level of support stems from the fact that younger people tend to demonstrate more permissive and liberal attitudes compared to older ones (Twenge et al., 2015). Moreover, this positive attitude towards euthanasia can also be explained by the fact that the current study sample consists mostly of secular subjects. A correlation was found between secularism and support for euthanasia, so that the lower the level of religiosity, the greater the support for euthanasia (Aghababaei et al., 2011).
Our findings also confirmed the second hypothesis, as people expressed a more positive attitude toward euthanasia when it came to an elderly patient than to a young patient. Similar findings were found among U.S. students who more strongly supported end-of-life care procedures for cancer patients aged 80 than for patients aged 22 (Stephens et al., 2014). This can be explained by the students' lesser ability to empathize with people far from their age, as opposed to the empathy they feel towards their peers which arouses fear regarding their own end of life (Stephens et al., 2014). Similar findings were also seen among mental health counseling students who were more supportive of euthanasia for patients aged 77 compared to patients aged 25, since the autonomy of the elderly patient was perceived as greater (Bevacqua & Kurpius, 2013). Another possible explanation is a widespread social perception in the Western world, whereby medical care should be prioritized for young patients compered to elderly patients (Diederich et al., 2011). Therefore, in a situation where the patient is perceived as having autonomy to decide on his or her life, euthanasia is seen as more legitimate. Hence, it is necessary to try and understand the extent of the patient's great suffering regardless of perceived autonomy due to the patient’s age, and to give suffering, as reflected by the patient’s experience, a more honorable place in making a decision to end his or her life.
The third hypothesis, which relates to the influence of illness type on attitudes toward euthanasia as a function of patient age, was not confirmed, although the results obtained pointed in the direction of the hypothesis. It may be that the gap found in euthanasia support for the elderly between the two illnesses types was not significant due to the perception of elderly people’s ability to control their lives. Findings indicate that elderly people are perceived as more capable of making a decision about ending their lives as a result of their long life expectancy, the positive and negative experiences they have encountered and endured, as well as aging-related changes that include deteriorating health and poorer social status in Western societies. These perceptions may make people view the desire to die among elderly as more reliable and rational than among younger adults (Frey & Hans, 2016).
Another possible explanation for the lack of support for the third hypothesis could be the participants' religiosity, which may be an intervening variable in this study. There were proportionally more religious participants in the experimental group in which participants were exposed to a young patient suffering from a mental illness than in the other groups. Due to the negative correlation between religion and euthanasia support (Aghababaei et al., 2011), it is possible that the gap between groups would have been greater if there had been a proportional ratio between the groups. However, since there were few religious subjects in the study, the conclusions are limited in this context. Therefore, in future research, it is advisable to sample subjects that are diverse in their level of religiosity and to examine whether there is a variable that can moderate the effect of religiosity.
An interesting finding is that in the interaction between illness type, patient age, and attitudes toward euthanasia, positive attitudes toward euthanasia were seen in the case of mental illness in the elderly, compared to negative attitudes with regard to young patients. These findings may indicate a change in perceptions of mental illness in the elderly population (although it is still perceived as less severe than physical illness). More comorbidity was found among elderly people (over the age of 70) with depression than among young adults (Kim et al., 2016). It is possible that the difference in the current findings between the groups is due to differences in perception of the severity and/or the healing ability of mental illness among young versus elderly patients. According to Berghmans et al. (2013), mental illness can lead to severe suffering and have a significant impact on a person's lifestyle, caused by the symptoms of the illness, psycho-social components (e.g., employment opportunities), and adverse effects of long-term use of medication, and therefore their suffering is no different from the suffering caused by terminal physical illness.
It seems that physical and emotional pain triggers similar areas in the brain (Kross et al., 2011). However, the findings of the current study show that the participants perceive mental illness as less painful than physical illness. In general, future research should try to address biases and stigmas related to mental illnesses versus physical illnesses. In particular, future research can be based on these findings and examine the perception of pain in mental illness compared to physical illness. In addition, the positive attitudes toward euthanasia in the case of mental illness, especially among elderly, may be related to the fact that most of the participants in the study were social sciences students. As mentioned, it was found that people involved in this field have a more positive attitude toward mental illness (Karesa & McBride, 2016). Therefore, it is worthwhile to sample students from other departments and examine their attitudes as well.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Note