
Abstract
The persistent stigmatization of suicide calls for a careful examination of the thought processes involved in perceptions of suicide. Hence, the present study is the first to apply terror management theory (TMT) and use experimental methods to examine whether reminders of death lead to increased stigma towards suicide and whether self-esteem moderates these stigmatized reactions. Consistent with the predicted effect of the death anxiety and self-esteem hypothesis, findings revealed that, for respondents with low self-esteem, thinking about their own death led to more stigma, less willingness to intervene, and allocated less money to a suicide prevention organization as compared to those who did not think about death. Findings from this study could have important implications for how we understand the psychological underpinnings of stigma and the role of death anxiety in hostile attitudes and decreased altruism – especially for mental health professionals working with individuals affected by suicide.
Introduction
Suicide attitudes are of great importance due to their potential to impact how individuals perceive and interact with those affected by suicide, including individuals who experience suicidal thoughts or behaviors and those dealing with the aftermath of another’s suicide attempt or loss (Kodaka et al., 2011). Generally defined as a person’s global and long-term evaluation toward a particular object in the environment (Eaton & Visser, 2008), attitudes play an important role in our understanding of complex social problems and in determining how we respond to these issues. Previous research has shown that while there is some indication of improvement in suicide attitudes in the context of physician aid in dying (Frey & Hans, 2016; Romer & Jamieson, 2003), suicide is still marked by stigma and individuals affected by suicide continue to be subjected to prejudice and discrimination (Andrews, 2014). Even in light of rising suicide rates in the U.S. (Kegler et al., 2017) and increased efforts to educate the public and reduce stigma, suicide stigma continues to persist. This continued persistence of stigma toward suicide calls for a more careful examination of the thought processes involved in perceptions of suicide. Hence, the present experiment applies terror management theory (TMT; Greenberg et al., 1986) as the theoretical background to examine suicide attitudes. Specifically, this study examines the interactive effects of self-esteem and reminders of death (or mortality salience; MS) on evaluations of suicide decedents and willingness to engage in prosocial behaviors in the context of suicide prevention.
Terror Management Theory
Terror management theory (Greenberg et al., 1986) originated mainly from the work of anthropologist Ernest Becker (1973) who claimed that all human behavior is driven by the fear and anxiety generated by the awareness of the inevitability of death. Greenberg and colleagues built on this idea that the fear of death is a powerful nonconscious motivator influencing human behavior and proposed a theory that has since then resulted in over 500 empirical studies supporting the theory (Greenberg & Arndt, 2011). It is important to note that the purpose of TMT was to contribute to a fuller comprehension of a broad range of behaviors affected by the uniquely human ability to understand the concept of mortality, rather than fully account for any particular behavior.
TMT posits that mortality salience can be activated without conscious involvement and that it can elicit a nonconscious, primal reaction to minimize the consequences of mortality awareness (Goldenberg et al., 2000). The same cognitive structures that allow human beings to be aware of their eventual death are also responsible for the development of mechanisms to manage death anxiety. One such mechanism is death-denying cultural belief systems, which serve to provide equanimity in the face of death-related terror (Greenberg & Arndt, 2011). Cultural worldviews are “widely shared beliefs about the nature of reality that imbue life with meaning and order and provide the opportunity for some form of death transcendence” (Landau et al., 2007, p. 478). These worldviews also offer answers to cosmological questions about human existence and universal causation, such as what is the purpose to life? Additionally, since the human body consists of organic material by which life eventually passes unto death, it is a strong source of death anxiety (Goldenberg et al., 2000). Thus, we can derive comfort from believing that human beings have unique, enduring identities with a soul because it distinguishes us from other living beings fated only to cease existing upon dying. Furthermore, cultural norms regarding the human body allow us to elevate ourselves metaphorically from flesh and bone to a higher plane of existence as objects of dignity, appeal, and spirituality, hence distancing people from the animal world.
There are two ways in which culture contributes to feeling transcendent of death: it “allows us to feel literally immortal by providing conceptions of a soul that continues beyond death” and offers “symbolic immortality by providing avenues for our identity and contributions to be preserved after our physical death” (Sullivan & Greenberg, 2013, p 20). For example, we can obtain literal immortality by maintaining religious faith that promises eternal life after death, such as found in Islam or Hinduism (Valea, n.d.); while symbolic immortality can be achieved through individual accomplishments that transcend time and make history, such as van Gogh’s Starry Night. Interestingly, in some cultures, the act of suicide is believed to promise eternal punishment (e.g., “hell”). Culture also provides a set of value standards, and a means to evaluate the behavior of others and ourselves. By choosing to comply with cultural standards of value, we are rewarded with a sense of importance and that we are connected to something greater than our individual lives. Insofar that one perceives to be a valuable contributor to a meaningful society, one will derive and maintain greater self-esteem (Landau et al., 2007). However, since cultural worldviews are socially constructed and dependent on continuous affirmation by others, one is strongly vested in seeking feedback from others to confirm the validity of his/her beliefs and to assure that he/she is adhering to the value standards set by society. Thus, according to TMT, cultural belief systems and self-esteem function to help human beings overcome deeply rooted existential terror.
To assuage the anxiety engendered by death awareness, we employ a variety of defense mechanisms. Proximal defenses are threat-focused attempts to protect oneself from death anxiety by either avoiding thoughts of death or minimizing the possibility that one could die in the near future (e.g., I do not drive drunk all that often or I have a lot of time before I could get cancer from smoking). Conversely, distal defenses of self-esteem and worldviews are less rational. The empirical support for TMT studies is copious and generated by a variety of distinct hypotheses tests (Greenberg & Arndt, 2011). The MS hypothesis used in the present study claims that if cultural worldviews and self-esteem serve to protect individuals from existential fear, then death reminders should lead to increased need for these protective psychological structures. Previous TMT studies using the MS hypothesis have shown that reminders of death lead to: (1) more vigorous efforts to follow prescribed cultural standards and heightened reliance on salient cultural values (Jonas et al., 2008); (2) harsher evaluations of individuals who threaten or violate one’s cultural worldviews (Greenberg et al., 1990; Rosenblatt et al., 1989); and (3) increased need for self-esteem and self-enhancement (Pyszczynski et al., 2004). Consistent with TMT’s claim that self-esteem confers resilience against death anxiety, some research has found that individuals with high self-esteem show a reduced effect of MS on worldview defense (Schmeichel et al., 2009). While the defense strategies used to buffer death anxiety as described by TMT do not always resemble a logical or straightforward connection to the inescapable reality of mortality, self-esteem and cultural worldviews “function by virtue of experiential linkages established very early in life between meaning and value on one hand and safety and security on the other” (Goldenberg et al., 2000, p. 201).
Present Study
The present study is the first to apply TMT to the study of suicide attitudes. The purpose of this study was to use the MS hypothesis to examine whether reminders of death lead to increased worldview defense in the context of suicide attitudes (i.e., more harsh evaluations of suicide and less willingness to engage in helpful behavior) and whether self-esteem moderates these reactions to death reminders. Suicide attitudes and pro-social behaviors were examined using three indicators: (1) attitudes toward a suicide decedent, (2) willingness to intervene against suicide, and (3) suicide prevention charity donation behavior. Specifically, this experiment predicted that, as compared to participants primed with pain-related cognitions (control condition), those primed with death-related cognitions (experimental condition) would endorse higher levels of stigma toward suicide, lower willingness to intervene, and allocate fewer dollars to a suicide prevention organization. However, it is also predicted that this effect would be moderated by the participant’s self-reported explicit self-esteem such that those with low self-esteem would have increased worldview defense against suicide as compared to those with high self-esteem.
Method
Participants
Participants were recruited online using Amazon Mechanical Turk (MTurk), an inexpensive crowdsourcing website that has become increasingly popular for survey-based research and has been supported as a reliable online recruitment method by previous studies (Crump et al., 2013; Horton et al., 2011; Paolacci et al., 2010), and were compensated $0.75 for their time. The inclusion criteria in the study were a minimum age of 18 years, English-speaking, and residing in the U.S. Participants were randomly assigned to each of the two study conditions in a 2 (MS vs. dental pain) x 2 (explicit self-esteem: high vs. low) between-subjects factorial design. The present data was collected as part of a larger data collection effort.
Procedure and Materials
Participants were told that they would take part in an anonymous study on personality and attitudes toward emotionally sensitive social issues. Following voluntary consent, participants completed a brief demographic survey to collect background information and the Rosenberg’s (1979) Self-Esteem Scale (SES). Next, participants were randomly assigned to the experimental conditions (MS vs. dental pain). Following the manipulation, participants completed a filler task in the form of a word completion activity. Participants were then asked to complete the dependent measures and respond to questions regarding their history of exposure to suicide and substance use. At the end of the study, participants were thanked and debriefed. The measures in this study were presented in the following order.
Analytic Procedure
Chi-square analyses and an independent samples t-test on participant age were used to ensure that there were no differences between experimental groups after random assignment. An independent samples t-test was also used to examine whether the MS manipulation resulted in greater death-thought accessibility for those in the MS condition. To examine the hypotheses stated previously, the sample was split into two groups based on their scores on the SES – below and above the median (low self-esteem ranged 0-15 and high self-esteem ranged 16-30). This transformation is consistent with previous TMT studies using self-esteem as a moderating variable (Schmeichel et al., 2009). A series of separate two-way analysis of variance (ANOVA) tests were conducted for morality salience (MS vs. control) x SES (high vs. low) as factors and the three measures of suicide attitudes as the dependent variables. Subsequent simple main effects tests were used to identify differences between subgroups for significant interaction effects.
Results
Participants
The sampling strategy resulted in 239 participants, with age ranging 18-77 years and an average age of 39.44 (SD = 13.23). Slightly more than half of the sample was female (54.9%, N = 129). The majority of the sample self-identified as White (75.5%, N = 178), with 8.4% Black (N = 20), 6.7% Asian-American (N = 16), 4.2% Latino (N = 10), and 4.2% Biracial (N = 10). Nearly half of the sample had completed a bachelor’s degree (45.6%, N = 109), whereas 27.2% (N = 65) had completed some college credits and 18.4% (N = 44) had obtained a PhD or professional degree. Table 1 presents additional demographic data.
Demographic Characteristics of Participants (N = 239).

Manipulation Check and Group Differences
In the word-stem completion task, participants in the MS condition wrote more death-related words (M = 2.64, SD = .78) as compared to participants in the control condition (M = 1.42, SD = .72), t(237) = −12.62, p < .001. A regression analysis showed that this effect was not moderated by self-reported explicit self-esteem. Furthermore, chi-square analyses revealed no significant differences between experimental groups on any demographic variable (p > .05).
Results of the ANOVA tests are presented in the tables below. Relevant means and standard deviations across groups and dependent variables are presented in Tables 2 to 4. As stated previously, it was predicted that participants who responded to the death prompt (MS condition) would have greater worldview defense against suicide, with higher stigma scores, lower acceptance scores, decreased willingness to intervene, and less money allocated to a suicide prevention organization, as compared to those in the control condition. However, it was also hypothesized that the MS effect would be more pronounced among participants with low self-esteem. No specific hypotheses were made for the Isolation/Depression factor as it is unclear whether endorsement of isolation and depression as being attributed to suicide would be considered as a negative or stigmatized view.
Multifactor ANOVA With Mortality Salience and Baseline Self-Esteem.

Note. Stig: stigma factor; I/D: isolation/depression factor; G/N: glorification/normalization; WIS-I: Willingness to Intervene Against Suicide – Intention subscale; Bold values indicate where the significant differences were identified by simple main effects; *p < .05.
Mean, Standard Deviation, and Percent Agreement Results for Short Form of SOSS Subscales—Including Individual Item Analysis.
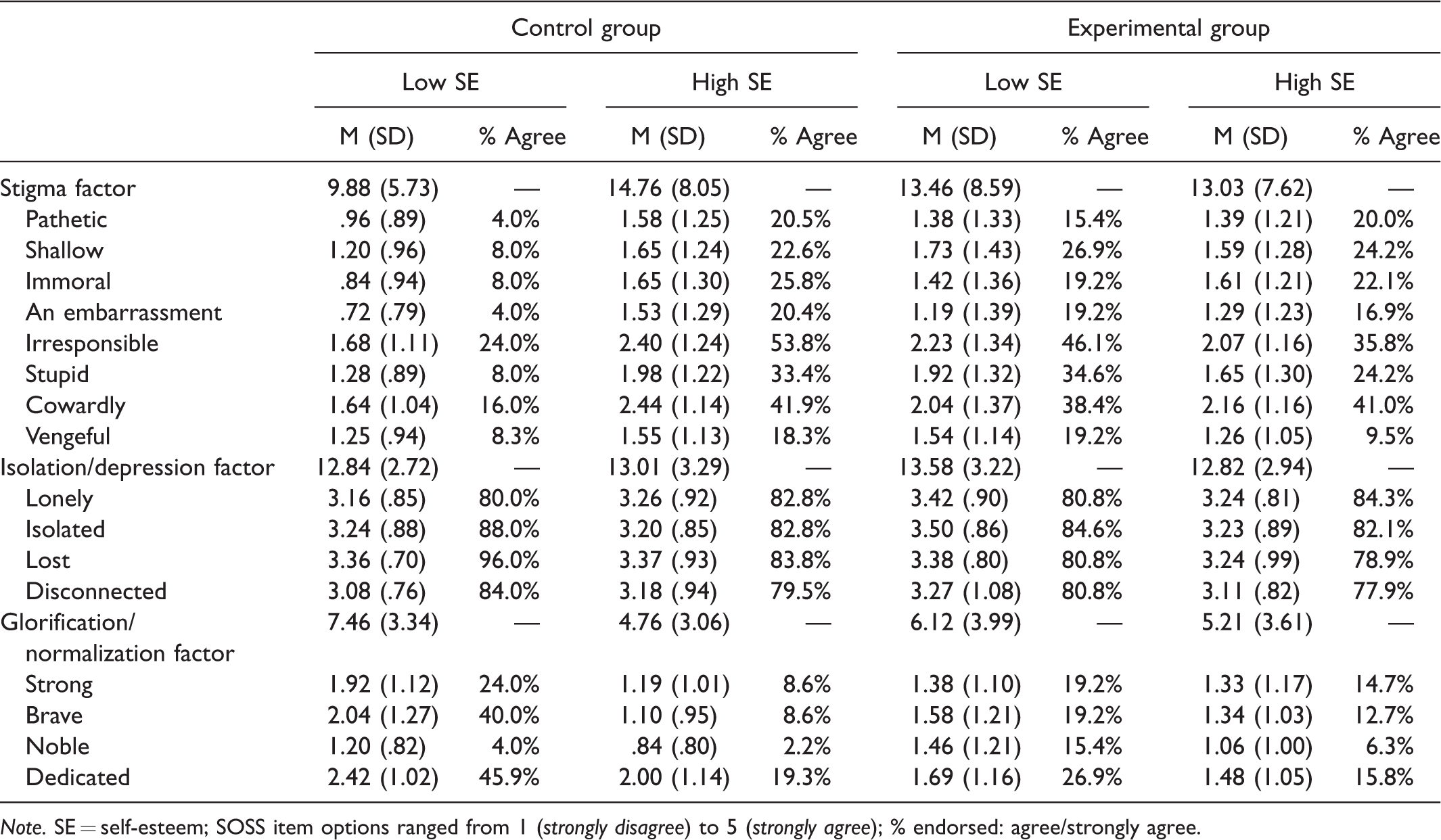
Note. SE = self-esteem; SOSS item options ranged from 1 (strongly disagree) to 5 (strongly agree); % endorsed: agree/strongly agree.
Mean, Standard Deviation, and Percent Agreement Results for Short Form of WIS-I—Including Individual Item Analysis.

Note. SE = self-esteem; WIS-I item options ranged from 0 (not at all likely) to 4 (extremely likely); % endorsed: very likely/extremely likely.
With regard to normalizing suicide attitudes, the ANOVA revealed a significant main effect of SES on the Glorification/Normalization subscale, F (1, 237) = 10.92, p < .01, indicating that participants with low self-esteem had greater endorsement of glorifying or normalizing views of suicide (M = 6.79, SD = 3.72) as compared to those with high self-esteem (M = 4.99, SD = 3.35). While participants with low self-esteem in the mortality salience condition had less accepting views (M = 6.12, SD = 3.99) than those in the control condition (M = 7.46, SD = 3.34), this difference was not statistically significant. Thus, no significant effect for mortality salience or interaction effect on glorified/normalized attitudes was found.
There were no main effects or interaction effect for mortality salience and self-esteem on the Isolation/Depression subscale.
Discussion
As TMT posits, the fear of death can have a powerful driving influence on human behavior and, as such, human beings have had to utilize certain psychological processes and structures – namely, cultural worldviews and self-esteem – to protect themselves from this existential terror (Pyszczynski et al., 1999). As discussed previously, research in support of TMT has found that when the problem of mortality becomes salient, people become highly motivated to engage in worldview defense by rejecting those who threaten their cultural belief systems and behaving in ways that promote self-enhancement – particularly among those with low self-esteem who may be more vulnerable to be affected by death-related anxiety. Hence, the present study was developed on the basis of TMT’s assumptions and sought to examine whether participants would perceive the problem of suicide as a worldview threat by reacting with more negative evaluations of a suicide decedent and whether the extent of their reactions would be mediated by their own self-esteem.
While the present study found some evidence in support for TMT hypotheses, the overall results across all dependent variables were inconsistent and incomplete. The findings for the stigma measure (i.e., SOSS-SF Stigma subscale) provided the most consistent results with the present hypothesis that morality salience among participants with relatively low self-esteem would react with harsher attitudes toward a suicide decedent. This indicates that, for the present sample, death reminders trigger terror management mechanisms when evaluating suicide decedents on negatively charged personality descriptors (e.g., cowardly, stupid) but that not all participants reacted in such manner. The finding of increased worldview defense among low self-esteem participants in this study is consistent with TMT’s theoretical basis that self-esteem functions to buffer against existential anxiety (Pyszczynski et al., 1999).
Additionally, while only providing partial support of the combined MS and self-esteem hypothesis in this study, mortality salience was found to have a statistically significant impact on the amount of money participants were willing to donate to a suicide prevention cause, such that death reminders led to substantially fewer dollars donated (adjusted average of $49.56 in MS condition compared to $71.99 in control condition). This finding, which can only be generalizable to the present sample, also aligns with one of TMT’s tenet that mortality salience increases individual’s tendency to engage in more self-indulgent and less altruistic behaviors – particularly when the prosocial behavior is associated with a cause that represents a worldview threat (Solomon et al., 2004).
However, despite the fact that the raw means for the remaining dependent variables for which specific hypotheses were made were consistent with the expected results (i.e., lower scores on glorified/normalized attitudes subscale and WIS-I for low self-esteem participants under the MS condition as compared to the control), there were no statistically significant findings regarding the impact of MS or interaction between MS and self-esteem. Interestingly, not only was self-esteem the only significant variable impacting participant scores on the SOSS-SF Glorification/Normalization subscale and the WIS-I scale, but the effect was revealed in the opposite direction: participants with relatively high self-esteem had less glorified/normalized views of a suicide decedent but indicated greater willingness to intervene against suicide as compared to those with relatively low self-esteem. This finding of higher WIS-I scores is consistent with recent research that shows a connection between increased willingness to intervene in scenarios involving “immoral” or improper behavior and high self-esteem (Moisuc et al., 2018). Taken together, less normalized suicide attitudes and greater willingness to intervene among participants with high self-esteem in this study could perhaps be interpreted as a greater resolve to act to prevent a death that is deemed unacceptable or abnormal. Moreover, research shows that the concepts of self-esteem and self-efficacy are closely interlinked (Judge et al., 2002); thus, making it plausible that participants with high self-esteem in this study responded with a greater willingness to act against suicide because they may have greater confidence in their ability to do so. It is important to acknowledge that the findings of this study may only be appropriately generalized to the present sample and not the broader U.S. population.
Limitations and Future Directions
There are several important limitations that may explain the inconsistent or null findings of the MS hypothesis in this study. With regard to the partially supported hypothesis for the donation allocation measure, it is possible that a self-report measure of self-esteem does not fully capture the full extent of the construct within an individual; and thus, making it difficult to avoid self-presentational biases and cognitive distortion when responding to a measure of self-worth (e.g., Baumeister et al., 1989). As such, there may have been an interaction between MS and self-esteem on donation behavior that went undetected due to a lack of an implicit measure of self-esteem. Indeed, past research has found that high implicit self-esteem is likely to be more effective than high explicit self-esteem to attenuate the MS effect (Schmeichel et al., 2009).
The remaining null findings may be due to several various factors and methodological limitations, including low experimental control when conducting studies on an online platform, social desirability bias, and the nature of the dependent measures that may elicit stronger or weaker MS reactions. While the online crowdsourcing MTurk platform provided a convenient way to obtain a large sample of non-college sample participants, it also introduced the problem of lower experimental control. In doing so, it was impossible to control the participant’s environment or to ensure that his/her attention was focused solely on the study and not be distracted by other stimuli. It is also possible that MTurk workers who complete online surveys are more susceptible to social desirability bias because payment for work is contingent upon approval by the person requesting the work and that payees have to ability to impact the workers’ performance ratings. Thus, even though participants were informed that that they would receive payment for completing the study regardless of how much of the survey they completed and that their responses would remain anonymous, there was nothing to prevent them from responding in a manner that they may have perceived to be the most “desirable” response so to minimize the likelihood of receiving no payment or poor performance reviews. This issue may be most relevant when participants responded to the WIS-I scale, which arguably has to highest potential for self-presentational bias as it more directly asks about prosocial intentions. Additionally, the null findings on the WIS-I scale may be attributed to the nature of the scale itself. A review of the TMT literature (Burke et al., 2010) found that studies that used measures targeting attitudes toward a person elicited more potent MS reactions as compared to dependent measures that focused on other attitudes or constructs. Lastly, while randomization procedures were used for experimental/control condition assignment to control for confounding variables, it is still possible that participants’ history of exposure to suicide (personal experience and/or exposure to others’ suicidality) may have had an impact on worldviews and attitudes toward suicide in such a way that mortality reminders would not have the expected influence on the scale responses.
Even though the results of this study did not support the MS and self-esteem hypothesis across all dependent measures, there has been more than several hundred studies replicating the effect of mortality salience on a wide spectrum of topics and behaviors (Burke et al., 2010; Greenberg & Arndt, 2011; Pyszczynski et al., 2004). Future research investigating the relevance of mortality salience and self-esteem for suicide attitudes should attempt to remedy the limitations of the current study, such as improved sampling strategies to obtain a more representative U.S. population, utilization of both explicit and implicit measures of self-esteem, and the development of more effective research forums that allow for greater experimental control. Replication studies would also do well to measure other attitudinal and behavioral responses to suicide, particularly ones that consider more nuanced cases of suicide beyond attitudes toward a “typical” person who dies by suicide that provide no context. Since the purpose of this study was to test only the core assumptions of TMT (i.e., the effect of mortality salience and self-esteem), future research should also develop and test hypotheses regarding the potential for other factors to impact the MS effect beyond what has been previously examined in the TMT literature, such as previous history of suicide exposure. Additionally, it would be important to examine the MS hypothesis on suicide attitudes in samples outside the U.S., as our belief systems and worldviews are almost entirely dependent on the culture by which they were formed (Sullivan & Greenberg, 2013). That is, it is possible that the MS effect on reactions to suicide would be vastly different in cultures. In any case, the present findings that mortality salience and low self-esteem are indeed relevant to our attitudes toward suicide is highly valuable for our understanding of how stigma operates and the potential role of high self-esteem in mitigating negative reactions to this public health crisis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the University of Kentucky College of Social Work.