
Abstract
The aim of this study was to investigate the relationship between religious orientation, coping strategies and suicidal behaviour among secondary school adolescents and college students. A total of 196 participants (73 adolescents and 123 adults college students) completed the online survey consisting of the Religious-Orientation Scale-Revised, Brief COPE and Suicidal Behaviours Questionnaire-Revised. Adolescents in secondary school had higher odds of suicidal thoughts and behaviour than college students (OR 4.40, 95% CI: 1.133, 17.094, p = 0.032). Individuals who employed an avoidant coping strategy had higher odds of suicidal thoughts and behaviour after adjusting for other relevant variables, which indicated that when a person engages in avoidant coping strategy, it is most likely that they have a higher odds of suicidal thoughts and behaviour (OR 1.118, 95% CI: 1.050, 1.189, p < 0.001). There is an urgent need to initiate psychological interventions to reduce suicide behaviour risk among Malaysian secondary school adolescents.
Introduction
Suicide has become the second most common cause of death for people aged 15 to 29 years old (World Health Organization [WHO], 2019). Every year, an approximate of 800,000 people die of suicide (WHO, 2019). Suicide occurs throughout the world and in all cultures (WHO, 2019). The rates of suicide among males are higher compared to females based on data by WHO (2018). According to data by WHO (2019), it was also found that the rate of suicide was 55% higher than deaths from war and homicide. In Malaysia, it was observed that there was an increase in suicidality prevalence among adolescents from 2012 to 2017 whereby there was an increase of 2.1% for suicidal ideation and 0.5% increase in suicide planning and attempt (Institute of Public Health [IPH], 2017). Chan et al. (2018) found that the highest suicide rates among races were the Indians and the least was the Malays. Based on the statistics in 2017, Wilayah Persekutuan Kuala Lumpur had the highest prevalence for suicidal ideation accounting for 13.2% followed by Selangor for suicidal planning, 9.5% and Perak, 9.3% for suicidal attempt (IPH, 2017).
Suicide refers to an action or behaviour that is intentionally done to oneself that leads to death (Silverman & Maris, 1995). Suicidal thoughts and behaviour encompasses suicidal ideation, planning, attempt (Nock et al., 2008) and death by suicide (Castle & Kreipe, 2007). Suicidal ideation refers to an individual having thoughts, considering or having plans about taking one own’s life (Klonsky et al., 2016). Suicidal planning refers to creating a specific plan on which how one would die (Nock et al., 2008). Suicide attempts on the other hand refers to a person carrying out an act that would potentially injure themselves with the intention of killing themselves (Centers for Disease Control and Prevention [CDC], 2019).
As the risk of suicidal thoughts and behaviour is able to be reduced with the help of protective factors, there are a few factors that could be further investigated. Religion (Huang & Wang, 2019; Jacob et al., 2019; Lester, 2017) and coping strategies (Mirkovic et al., 2015; Primananda & Keliat, 2019) have been found to be protective factors against suicide. Religion is a set of beliefs and practices that are related to the gods (Durkheim, 1976). Religion provides an individual the way of life by guiding them based on a set of beliefs (Yasein & Moghal, 2017). Religious orientation refers to types of motivation an individual has when engaging in religious practices, and could be categorised into extrinsic and intrinsic religious orientation (Allport & Ross, 1967). It has been found that individuals with intrinsic religious orientation tend to hold true to their beliefs, values and practices, believes in God and may see pain or problems as a will from God such as to teach the individual to persevere (Stack, 1983). On the other hand, those with extrinsic religious orientation may see religion as a way to achieve their goals such as getting social recognition or to fit in (Yasein & Moghal, 2017). This might explain how having intrinsic religious orientation might lead to better outcomes compared to extrinsic orientation. Studies have shown that individuals who have intrinsic religious orientation have lower suicidal behaviour than those with extrinsic religious orientation (Lester, 2017; Lester & Walker, 2017; Lew et al., 2018 ; Malihe & Motahare, 2016).
However, there are also contradicting views on religious orientation and suicidal behaviour. Lester and Walker (2017) found that there was a negative relationship between intrinsic religious orientation and suicidal ideation in European American women but not for men and both genders of African American. Besides, Lawrence et al. (2016) found that intrinsic religious orientation such as praying and being affiliated to that particular religion is not a protective factor for suicidal ideation. Dueñas et al. (2020) found that there was no correlation between religious orientation and suicidal behaviour. They also found that religiosity was a protective factor among older adults and not for adolescents. Similarly, Wu et al. (2015) found out that religious orientation was not a protective factor against suicidal behaviour among adolescents but was a protective factor among adults.
Coping strategy, on the other hand, has been found to be a protective factor as it can safeguard a person from the risk of suicidal behaviour (Mirkovic et al., 2015; Primananda & Keliat, 2019) depending on the type of coping strategy that they use. There are many types of coping strategies and the types employed vary from individual to individual (Carver, 1997). Some may engage in adaptive coping strategies such as actively trying to find a solution to the problem (Heffer & Willoughby, 2017) whereas some engage in maladaptive coping strategies such as engaging in suicidal behaviours when things are mentally stressful for them (Huang & Wang, 2019; Michel & Gysin-Maillart, 2015). It was found that engaging in approach coping such as active coping and planning and emotional coping such as getting emotional support or acceptance were associated with lower risks of suicidal behaviours (Campos et al., 2017; Cheung et al., 2018; Heffer & Willoughby, 2017; Ong & Thompson, 2019; Tang et al., 2015). On the other hand, those who engaged in avoidant coping such as denial, emotional eating, and ineffective coping such as behavioural or mental disengagement were associated with higher risks of suicidal behaviours (Ong & Thompson, 2019).
Complicating matters, suicide is a crime in Malaysia, according to Section 309 of the Penal Code (Attorney General’s Chamber, 2006), and is a capital sin in Islam, the national and majority religion of Malaysia. As Islam forbids their adherents from suiciding (Chan et al., 2018), it is assumed that the rate of suicide will be low. However, the number of suicide cases among adolescents in Malaysia is on the rise. Therefore, this study aimed to examine if religious orientation and coping strategy were predictive of suicidal behaviour. In addition, we examined whether there were significant differences between males vs. females, and secondary school vs. college students, in their level of suicidal behaviours.
Methods
Study Design and Sampling Method
This study was a cross-sectional quantitative study. Participants were recruited through purposive sampling as this study required secondary school and college students who were studying in either Kuala Lumpur or Selangor, Malaysia. In this study, an online survey was used to collect data.
Sample and Location
The sample size for this study was calculated based on the formula, ’50 + 8m’ whereby ‘m’ referred to the number of variables (Tabachnick & Fidell, 2013). A total of 114 participants were needed whereby a minimum of 57 participants were needed from secondary schools and college respectively. A total of 196 participants was recruited whereby 73 participants were from secondary school and 123 from college which fulfilled the requirement of a minimum participants of 57 from each category. This study focused on adolescents and young adults from Wilayah Persekutuan Kuala Lumpur and Selangor as based on the survey by the Institute for Public Health (IPH,2017), Wilayah Persekutuan Kuala Lumpur had the highest number of adolescents with suicidal ideation accounting for 13.2% whereas Selangor had the highest in suicide planning (9.5%).
Data Collection
A link to the questionnaire was posted on Facebook to disseminate the questionnaire to individuals who fit the inclusion criteria for the study. Before answering the questionnaire, participants were asked to read the informed consent that contained the purpose, benefits, risks for participating in this study and their rights as a participant and then agreeing to it. The questionnaire contained the demographic questionnaire, the religious-orientation revised (ROS-R) scale, Brief COPE scale and Suicide Behaviour Questionnaire-Revised.
Pilot Study
A total of 30 participants were recruited for the pilot test. According to Johanson and Brooks (2010), a total participant of 30 from the targeted population for the pilot study is sufficient. It is also said that the minimal recommendation for a pilot study is 30 participants (Johanson & Brooks, 2010). The pilot study was done to address certain issues such as revising certain questionnaire to ensure it is understood by the targeted participants and to know if this study can be done without difficulty (Johanson & Brooks, 2010).
Instrumentation
Demographic Questionnaire
Participants were asked to fill up the demographic questionnaire pertaining their name, age, date of birth, gender, state, ethnicity, religion, perceived academic results, family income, stating either college or secondary school student and number of siblings.
Religious Orientation-Revised (ROS-R)
Religious orientation was measured using the Religious Orientation-Revised (ROS-R) or Revised Intrinsic/Extrinsic Religious Orientation Scale (Gorsuch & McPherson, 1989). The ROS-R measured two types of religious orientation which were intrinsic and extrinsic. The ROS-R contained 14 items whereby 8 items measured intrinsic religious orientation whereas 3 items measured social and personal external religious orientation respectively (Tiliopoulos et al., 2007). Examples of the items were ‘I enjoy reading about my religion’ and ‘It doesn't much matter what 1 believe as long as I am good’. Questions were answered based on a 5-point Likert scale whereby 1 indicated ‘strongly disagree’ and 5 indicated ‘strongly agree’ (Tiliopoulos et al., 2007). The scores for intrinsic religious orientation ranged from 8 to 40 whereas for extrinsic religious orientation, it ranged from 3 to 30 (Tiliopoulos et al., 2007). The ROS-R had an internal consistency reliability of .83 for intrinsic religious orientation and .65 for extrinsic religious orientation (Gorsuch & McPherson, 1989).
Brief COPE
Coping strategy was determined using Brief COPE by Carver (1997). The Brief Cope contained 28 items and these items were classified into two groups which were avoidant and approach coping (Eisenberg et al., 2012). Questions were answered based on a 4-point Likert-scale whereby 1 indicated ‘I haven’t been doing this at all’ and 4 indicates ‘I’ve been doing this a lot’ (Carver, 1997). Some of the items were ‘I’ve been criticising myself’ and ‘I’ve been giving up trying to deal with it’. The scores on the subscales were calculated based on the manual and the scores were categorised into the types of coping strategy an individual has. The coping strategy were categorised into either avoidant or approach coping strategy except for religion and humour (Eisenberg et al., 2012). The scale had an internal consistency reliability ranging from .50 to .90.
Suicide Behaviours Questionnaire-Revised (SBQ-R)
The Suicide Behaviours Questionnaire-Revised (SBQ-R) (Osman et al., 2001) was used to determine suicidal behaviour. The SBQ-R had 4 items whereby each item measured different dimensions of suicidal behaviour such as frequency of suicide attempt, lifetime and self-reported suicidal ideation or attempt and threat of suicide attempt (Osman et al., 2001). Examples of the items were ‘Have you ever thought about or attempted to kill yourself?’ and ‘How often have you thought about killing yourself in the past year?’. Each question had a scale and different responses corresponded to a different value. A cut off score that was recommended to be used by Osman et al. (2001) was ≥7 to indicate the presence of suicide behaviour risk. The SBQ-R scale score had an internal consistency reliability of Cronbach’s alpha = .80.
Data Analysis
IBM Statistical Package for Social Science (SPSS) Version 22 (Armonk, NY: IBM Corp) was used to analyse all of the data. Descriptive data was used to analyse participant’s information. As the data was non-parametric, Spearman’s correlation was conducted to test the correlation between religious orientation, coping strategy and suicidal behaviour. Mann-Whitney U test was done to examine if there is a significant difference between gender on suicidal behaviour and also between adolescents and adults on suicidal behaviour. Finally, a binary logistic regression was conducted. Logistic regression was used to test the odds ratios of factors predicting suicide risk (religious orientation, coping strategy, age, gender, religion and education level) based on the dichotomised SBQ-R based on the cut-off score of ≥7 as the dependent variable.
Results
Pilot Test
The questionnaire was tested on 30 participants and there were no comments from the participants regarding the questionnaire. Internal consistency was conducted using SPSS and it was found that all 4 instruments had a high reliability. The ROS-R, Brief COPE and SBQ-R had an acceptable reliability (refer to Table 1). According to Taber (2018), a Cronbach’s alpha with the value of those above .70 is considered acceptable. The Cronbach’s alpha ranging from .93–.94 are considered excellent and those ranging from .84 to .90 are considered reliable (Taber, 2018).
Internal Reliability Consistency for Pilot Test and Actual Study.

Note. ROS-R = Religious Orientation Scale- Revised, SBQ-R = Suicidal Behaviours Questionnaire- Revised.
Demographic Information
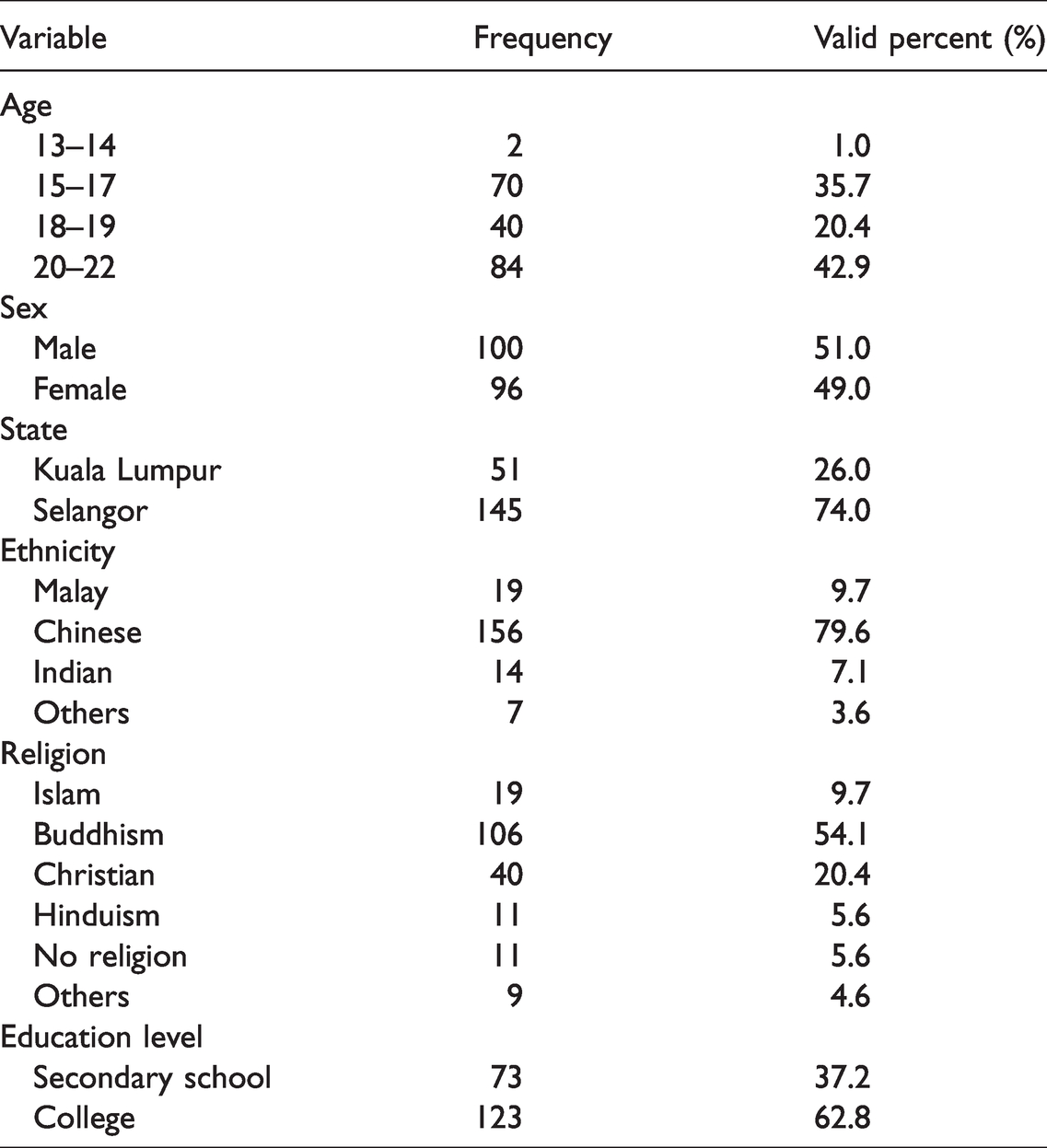
A total of 196 participants had participated in the study. Descriptive analysis of the participants and also the scoring of the scales were conducted and can be seen in Tables 2 and 3. The participants’ age ranges from 13–22 years old (M = 18.62, SD = 1.87). Seventy-three participants were from secondary school whereas 123 participants were in college. There were more participants in the age group of 20–22 (42.90%), followed by 15–17 (35.70%), 18–19 (20.40%) and the least were 13–14 years old (1.0%). More males (51.0%) compared to females (49.0%) had participated in the study and most of the participants were from Selangor. Among the participants, most of them were Chinese, Malay, Indian and followed by other ethnicities such as Punjabi. Most of the participants were Buddhist, followed by Christian, Islam, Hindu, no religion and other religion (refer to Table 2).
Participants’ Profile (N = 196).
Spearman’s Correlation for Religious Orientation (Intrinsic and Extrinsic), Coping (Avoidant and Approach) and Suicidal Behaviours.
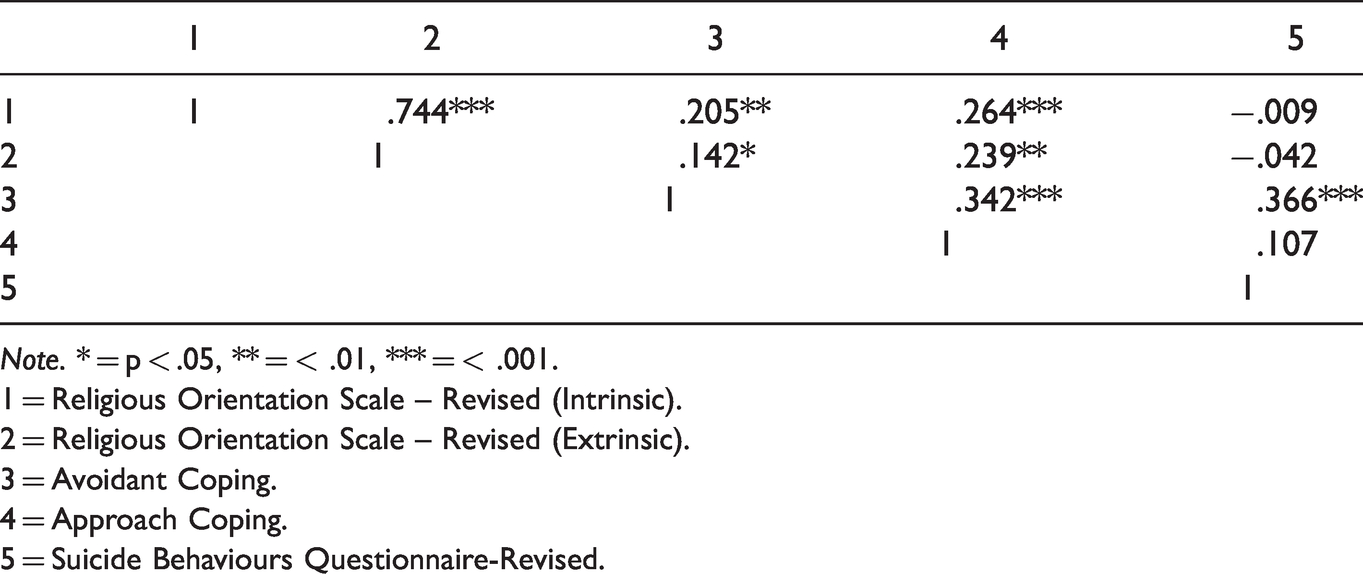
Note. * = p < .05, ** = < .01, *** = < .001.
1 = Religious Orientation Scale – Revised (Intrinsic).
2 = Religious Orientation Scale – Revised (Extrinsic).
3 = Avoidant Coping.
4 = Approach Coping.
5 = Suicide Behaviours Questionnaire-Revised.
In order to test the correlation between religious orientation, coping and suicidal behaviour, Spearman’s rank correlation analysis was conducted. The scores on the ROS-R (intrinsic and extrinsic), Brief COPE (approach and avoidance) and SBQ-R were correlated as presented in Table 3. There was non-significant correlation between intrinsic religious orientation and suicidal behaviour, r = −.01, p = .898 and extrinsic religious orientation and suicidal behaviour, r = −.042, p = .555. However, there was a significant positive correlation between avoidant coping strategy and suicidal behaviour, r = .37, p < .001 but not for approach coping strategy, r = .11, p = .135.
The Mann-Whitney U test showed that there was no significant difference in suicidal behaviour of males (Md = 4.5, n = 100) and females (Md = 6.00, n = 96), U = 4298, z = −1.30, p = .195. In addition, the Mann-Whitney U test showed that there was a significant difference in suicidal behaviour of adolescents (Md = 6, n = 73) and adults (Md = 4, n = 123), U = 3623, z = −2.31, p = .021. The results revealed that secondary school adolescents had significantly higher median scores for suicidal behaviour than adults in college.
The model of the binary logistic regression conducted on factors predicting suicidal behaviours was significant, χ2(14) = 38.18, p < .001, explaining 24.1% (Nagelkerke R2) of variance in suicidal behaviour and have classified correctly 61.7% of cases. The Hosmer and Lemeshow test suggested that the model was a good fit as it has a p-value of more than .05 which was p = .563. Results of the binary logistic regression analysis are shown in Table 4. The regression results indicated that adolescents in secondary school had a higher risk of suicidal behaviour compared to college students (OR 4.40, 95% CI: 1.133, 17.094, p = 0.032). In addition, those employing avoidant coping style also had elevated risk of suicidal behaviour (OR 1.118, 95% CI: 1.050, 1.189, p < 0.001).
Logistic Regression of Factors Associated With Suicidality (Suicidal Behaviours Questionnaire-Revised).

Note. B = intercept; OR = odds ratio; CI = confidence interval; *Reference group.
Discussion
It was found that religious orientation did not have a correlation with suicidal behaviour and was not a significant predictor of suicidal behaviour, which was not consistent with studies done by Malihe and Motahare(2016), Lester (2017) and Lew et al. (2018). However, the results found in this study were consistent with past studies done by Dueñas et al. (2020), Cole-Lewis et al. (2016), Lester and Walker (2017) and Wu et al. (2015).
One of the reasons can be due to age difference (Cole-Lewis et al., 2016; Dueñas et al., 2020; Wu et al., 2015). It was suggested that as people grow older with increasing issues with their social life, physical health and mental health, they tend to seek support or comfort on religious practices (Cole-Lewis et al., 2016; Wu et al., 2015). Religion becomes a coping strategy and it also becomes part of their identity (Wu et al., 2015). According to Malone and Dadswell (2018), they had found that older adults mentioned that religion becomes part of their coping strategy and that it gave them a sense of peace especially when they have an illness. This would explain the low levels of religious orientation among adolescents (Cole-Lewis et al., 2016). However, according to Cole-Lewis et al. (2016), adolescents tend to seek support from others through social connectedness such as from families or friends. Not only that, it was found that most adolescents have said that religion was not important to them and that they were not religious compared to their older counterparts (Hackett et al., 2018). For example, adolescents may attend religious functions not because of their own free will but because of the encouragement from their family (Cole-Lewis et al., 2016).
Besides, avoidant coping strategy was also examined as a risk factor for suicidal behaviour. There was a correlation between avoidant coping strategy and suicidal behaviour, which was also a significant predictor of suicidal behaviour. These results were in line with past studies done by Campos et al. (2017), Cheung et al. (2018), Heffer and Willoughby (2017), Ong and Thompson (2019), and Tang et al. (2015). The results from these researchers indicated that as a person engages in avoidant coping strategy, they would have a higher chance of engaging in suicidal behaviour. As adolescents go through vast changes in terms of their physical image, their relationship with family and friends, their school context and academic demands (Santrock, 2017), they might have a hard time managing these changes and a hard time choosing the appropriate coping strategy to cope with stress that comes along with these changes (Herres, 2015). When adolescents are overwhelmed by the stress and unable to cope effectively, they might engage in avoidant coping strategy (Capella & Adan, 2017; Young & Limbers, 2017). Although engaging in avoidant coping strategy is said help reduce an individual’s stress, it does not solve the problem (Lazarus & Folkman, 1984).
The link between avoidant coping strategy and suicidal behaviour can be explained by the stress generation model that mentioned that an individual has the ability to change its environment by playing the active role and not the passive role (Hammen, 2006). When a person avoids the stressors, it may actually make the situation worse and add additional stressors to it (Anniko, 2018) which may lead to suicidal behaviour. Thought suppression can also explain the link between avoidant coping strategy and suicidal behaviour (Wenzlaff & Wegner, 2000). By suppressing one’s thoughts about the stressors, it was found to have counterintuitive findings whereby a person would actively think about the stressors. This suggests that when one tries to avoid the stressors by not thinking about it, it may lead to the person actively thinking about it. If active approaches were not taken to deal with the stressors, there might be consequences on that individual such as psychologically, emotionally and cognitively (Anniko, 2018).
Furthermore, there was no significant difference between gender in suicidal behaviour which was consistent with Malihe and Motahare(2016) and Uddin et al. (2019). This can be due to the greater level of gender equality among young people in Malaysia. According to WHO (2018), it is generally known that the rates of suicide among males are higher compared to females. In today’s society, the awareness of gender equality on both genders and gender norms are on the rise (Gupta et al., 2019) and this can be seen with the effort made by the United Nations whereby they had come up with a blueprint of Sustainable Development Goals which included the gender equality (United Nations, 2020). According to River (2018), it was found that most of the male participants seek help from therapist of counsellors when in distress which lowers the risk of suicidal behaviour. River (2018) also found that most of the male participants who seek help from medical professionals mentioned that they had ‘nothing to lose’ and a minority of male participants did not seek for help as it does not follow the gender norm whereby seeking help would be seen as ‘not manly’. Therefore, this situation may be changing in the younger generation. However, what River (2018) had found was based on Western countries and that most males are still reluctant to seek help which was consistent with what Heath et al. (2016) and Yin et al. (2019) had found. They found that majority of males in Eastern countries were less likely to seek help regarding their mental health. Therefore, more studies need to be conducted in Eastern countries.
Not only that, it was found that there was a significant difference between adolescents and adults on suicidal behaviour whereby adolescents had a higher level of suicidal behaviour compared to adults. This difference was maintained after adjusting for other demographic and risk factors, whereby adolescents remained 4.4 times more likely to have suicidal behaviour risk compared to college students. This may be because adolescents are at the age where they would experience changes that are drastic in terms of their physical appearance, social lives such as having to transition from middle school to high school and forming relationships with others, trying to understand themselves, in other words, finding their own identity and trying to find their sense of belongingness in order to fit in (Santrock, 2017). These drastic changes that occur could be detrimental to adolescents as they can produce stress or pressure (Huang & Wang, 2019). Some of the factors that had contributed to the rise of suicidal behaviour in adolescents compared to adults are academic stress (Kok et al., 2015), relationship issues (Kok & Low, 2019) and also bullying (Hinduja & Patchin, 2019).
In a society where academics are heavily emphasised, there is no doubt that adolescents feel stressed and this could possibly lead to suicide (Kok et al., 2015). According to Kwak and Ickovics (2019), the stress from academics is due to the competitiveness of the school environment and the expectations from others in order for them to excel. According to Kok et al. (2015), they found that parents in Malaysia had placed a great value of emphasis on the importance of education where they would send their children for extra classes in order for them to excel in their examinations. Not only that, adolescents would also spend most of their time either in school or extra classes as most of the time they were needed to stay back for extra curriculum activities and also being sent to extra classes by parents (Kok et al., 2015). According to Reddy et al. (2017), adolescents’ self-esteem would drop and this would lead to suicidal behaviour when the fear of failing is always being reinforced by both parents and teachers. Relationship issues can be another explanation to the increase of suicidal behaviour in adolescents compared to adults (Kok & Low, 2019). Another explanation that may have contributed to the rise of suicidal behaviour in adolescents is bullying (Hinduja & Patchin, 2019). Kok et al. (2015) further found that adolescents had mentioned that they were lonely whereby they had nobody to confide their problems to which also act as a stressor that contributed to suicide.
However, these factors were not part of this study and need to be investigated in future studies. In addition, this study has a few limitations, including the lack of generalisability inherent in cross-sectional studies employing purposive sampling. In addition, we did not investigate other aspects related to religious belief, such as the level of religiosity. Finally, individuals may have different interpretations regarding their religion’s teachings about suicidality, and exploring this was not within the scope of the study. There is an urgent need to intervene with adolescents in secondary schools who are suffering from a higher risk of suicidal behaviours, and yet may not have recourse to the help they need to overcome their suicidality.
Conclusion
To conclude, this study was conducted to examine if there was a relationship between religious orientation, coping strategy and suicidal behaviour. The results showed that adolescents in secondary school had more than four times the risk of suicidal behaviour compared to college students. This might indicate that adolescents are more prone to suicidal behaviour. It was also found there was no difference between males and females in suicidal behaviour which could indicate that both genders have the capability of engaging in suicidal behaviour. Not only that, there was no correlation between religious orientation and suicidal behaviour but there was a correlation between avoidant coping strategy and suicidal behaviour. This could indicate that being religious does not protect a person from suicidal behaviour whereas engaging in avoidant coping strategy would predict that a person has a higher chance of engaging in suicidal behaviour.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.