
Abstract
The study aimed at finding the risk factors associated with adult mortality (15–59 years) due to external causes (accidents, suicide, poisoning, homicide, and violence). Using National Family Health Survey data-4 consisting of 1,756,867 sample, we applied a Robust Poisson Regression Model to determine the potential risk factors. Findings suggest that the highest proportion of deaths due to external causes was in the age group 20–24 years. The prevalence of these deaths was higher among older adults (age 50 years and above). The risk was more among males (Incident Rate Ratio (IRR) for females is: 0.29, p < 0.001), rural residents (IRR: 1.16, p < 0.001), exposed to mass-media (IRR: 1.08, p < 0.05), residing in female-headed households, in households having a member with higher education. This risk decreased for large families (IRR: 0.89, p < .001). A need to strengthen awareness and mentorship programs for young-adults and middle-aged people to control such avoidable deaths is recommended.
Keywords
Mortality is an important component of demographic change and a critical measure of a population’s health and public health systems (Mathers & Boerma, 2010; McKerrow & Mulaudzi, 2010). The occurrence of death can be naturally, un-naturally, or as the result of a combination of both. Deaths due to external causes or non-medical causes which are against the order of nature comprise of the injury due to either trauma, physical or chemical agents, or other means of violence. These are primarily categorized into accidental, poisoning, due to violence, homicide, or suicide (Sjögren et al., 2000). These deaths can be unintentional (such as transport-related, falls, drowning, fires and burns, venoms, and poisons) or intentional (suicides and assaults). Traffic collisions, drowning, poisoning, falls or burns, and violence from assault are the commonest form of external causes of deaths. Road traffic and drowning are the leading causes of death among external causes of death.
Reducing mortality due to external causes as mentioned in the third Sustainable Development Goal (SDG) which focused on ensuring healthy lives and promoting wellbeing. Deaths due to external causes are gaining momentum and creating a huge life loss among adults. This group constitutes the work-force and is very crucial for the development of any society as they are biologically reproductive, economically productive, and can take responsibility to support the children and elderly population (Feachem, 1992). Premature deaths among adults are affecting society when families are devastated by the early death of adult members of the family as the premature death of the principal income earner often inflicts serious financial hardship to the family (Saikia & Bhat, 2008). Damage to this section will inevitably have a substantial impact on the socio-economic development of a country and also it leads to a slowdown in overall national development (Herzer & Nagel, 2019).
An understanding of levels, patterns, and trends of adult mortality due to external causes along with the determinants is an important part of any demographic inquiry. With society going through a transition in quick succession, a host of problems have crept in causing serious concern amongst the conscious section. Every death including un-natural causes, whether suicidal, accidental, or homicidal, represents a tragic waste of precious human life and resources. Data on deaths by external causes in a particular geographical area indicates the nature of such communities, and the health standards and legislation policies (Arun et al., 2010). Usually, demographers continue to place a great deal of focus on demographic and social factors associated with adult mortality (Rogers et al., 2002) as cultural and socio-economic factors of a country are usually related to the causation of deaths due to external causes. (Palmiere et al., 2010). Despite the scanty of literature focusing on determinants of adult mortality, theoretically one should expect that some key issues need to be addressed to move socio-economic mortality studies of adults in India beyond gender, regional and spatial differential to a more inclusive perspective. To understand the avoidable deaths, the present paper aims is to study various socio-economic, demographic, and behavioral factors influencing adult mortality due to external causes (accidents, suicides, homicides poisoning, murder, and others).
Data and Methodology
This study aimed to find the determinants of adult mortality (age 15–59) using the fourth National Family Health Survey (NFHS-4) data that was conducted in 2015–16 covering 640 districts, 29 States, and 7 Union Territories of India. The survey followed a multi-stage sampling design in both the urban and rural areas and provided national, state, and district-level estimates of most demographic and health indicators. For the first time, information on deaths due to external causes was collected in this fourth round of NFHS. Further information about survey and methodology is given elsewhere (International Institute for Population Sciences & ICF, 2017).
As NFHS-4 asked only one question on external causes of death, so to get the break-up of different external causes of deaths among adults, the present study also extracted data from National Crime Records Bureau (NCRB) for the year 2015 The National Crime Records Bureau (NCRB) is a government agency responsible for collecting and analysing data based on crime as defined by the Indian Penal Code (IPC) and special and local laws. NCRB (established in 1986) was set up to function as a repository of information on criminals and crimes to assist the investigators in linking crime to the perpetrators. Its mission is to empower the Indian police force to uphold the law, protect people, and provide leadership and excellence in crime analysis. NCRB compiles and publishes national as well as state-wise crime data annually. NCRB provides age- and sex-wise data on deaths due to natural accidents, unnatural accidents, suicide, homicide, murder, dowry deaths for different years.
Statistical Analysis
Bivariate and Multivariate analysis were used for analysis. In the multivariate analysis, the Robust Poisson regression model was used for examining the factors associated with deaths due to external causes among adults in India. When Poisson regression is applied to binomial data, the error for the estimated relative risk will be overestimated (Zocchetti et al.,1995). However, this problem may be rectified by using a robust error variance procedure or the Robust Poisson regression method (Royall, 1986). Although Poisson regression was used when outcomes were measured in counts it can be used in binary outcome when the outcome is rare but measured in large samples (Saikia & Ram, 2010; Zou, 2004). Robust Poisson regression models are valid, unbiased, and is a better alternative to the logistic regression method in case of binary dependent variable in large samples (Huang, 2019; Saikia & Ram, 2010; Zou, 2004).In 2,01,485 articles that focussed especially on Binary outcomes, used Robust Poisson regression models (Huang, 2019). The whole analysis was carried out in Stata 16.0.
Information on 73,966 deaths since January 2012 was extracted from 6,01,509 households, which was combined with the person file. Further, some of the individual’s characteristics including consumption of alcohol were brought to this file from the individual men and women files. As the analysis was restricted to adults aged 15–59 years, the sample was 17,56,867 persons with 4,103 deaths due to external reasons.
Outcome Variable
In NFHS4, information was asked on whether any usual member of the sampled household died due to external causes since January 2012 and this was the first most time in the history of NFHS. Age at death and sex of deceased was asked for each death that occurred in the household. This information about the deceased person was collected from the head of the household. The outcome variable was defined and coded as- If the death occurred due to accidents, suicides, poisoning, homicide, or violence, that death was coded as death due to external causes (‘1’), the survived persons were coded as (‘0’) and the don’t know cases as (‘8’). The “don’t know” cases were taken as “no” and analysis was done accordingly.
Independent Variables
In this study, the individual characteristics such as - age, age-square, sex of the individual (died or survived); household characteristics including age and sex of the household head, place (rural, urban) of residence, number of members in the family, wealth index (poor, middle, rich), the region of residence (north, central, east, northeast, west, south) owning a car by the household; household’s access to mass media (no exposure, or at least one source of mass media), and information of family members such as - educational qualification of the person acquiring the highest completed education (illiterate, primary, secondary, higher), and drinking alcohol were taken as independent variables.
Here, 5 wealth quantiles were clubbed into three viz. “poorest and poorer” as “poor”, middle as middle and “richer and richest” as “rich”. Information on having either two or four wheeler was created. “Two wheeler” refers to motorcycle or scooter (0” as “no” and “1” as “yes”) and four wheeler refers to car or truck (0” as “no” and “1” as “yes”).
The 29 States and the 7 UTs of India were clubbed into 6 geographic regions. The ‘north’ region included Jammu & Kashmir, Himachal Pradesh, Punjab, Haryana, Chandigarh, Delhi, Uttarakhand, and Rajasthan. The ‘central’ region included Uttar Pradesh, Madhya Pradesh and Chhattisgarh. Bihar, Jharkhand, West Bengal, Odisha, and Andaman & Nicobar comprised the ‘east’ region. The ‘northeast’ region included Assam, Arunachal Pradesh, Meghalaya, Manipur, Mizoram, Nagaland, and Tripura. Gujarat, Dadra & Nagar Haveli, Daman & Diu, Maharashtra, and Goa comprised the ‘west’ region. The ‘south’ region included Andhra Pradesh, Telangana, Karnataka, Kerala, Lakshadweep, Puducherry, and Tamil Nadu.
As most of the individual characteristics of the deceased were not available in data, so proxy variables from members of the households were considered based on available literature on the possible linkages with adult mortality. According to Saikia and Ram (2010), the behaviours of household members should be taken as either a proxy for the dead person's behaviour or to examine the resultant impact of these behaviours on the dead person. For example, some previous studies revealed that like smoking, drinking behaviour spread through close and distant social relationships because smoking habits depended on the habits of one's spouse, siblings and friends (Christakis & Fowler, 2008). Several other studies showed that drinking initiation in adolescence was associated with siblings and parental behaviour (Conrad et al., 1992; Tyas & Pederson, 1998). According to Osler et al. (2001), there was a family resemblance in smoking as well as drinking behaviour, especially within the same generation.
The educational level of the deceased and the other members was approximated by the highest level of the person of the family who attained the highest education. Similarly, alcohol consumption of any household member was conserved as a proxy variable for risk behaviour for externally caused death.
Results
The distribution of total deaths as well as external causes of deaths from the NFHS-4 and NCRB is shown in Figure 1. About 22.1 percent deaths out of total deaths occurred due to any external cause in 2015–16. The figure shows that among all external causes, deaths due to unnatural accidents were the maximum (62.5 percent), followed by, suicides (26.2 percent). The proportion of deaths due to homicides (0.8 percent) and due to dowry (1.7 percent) was the least reported in the same year (2015).

Distribution of Total Deaths And External Causes of Deaths Among Indian Adults (15–59 Years).
The percentage share of deaths due to external causes to all deaths occurred among adults (15–59) in India and its states are shown in Figure 2. Overall, 22.1 percent of Indian adult’s (15–59 years) deaths were attributed to external causes. The percentage of deaths due to external causes to total deaths was maximum for Manipur (30 percent), followed by. Kerala (28.7 percent), West Bengal (27.1 percent). The proportion was least for Dadra and Nagar Haveli (7.7 percent) and Lakshadweep (3.9 percent).
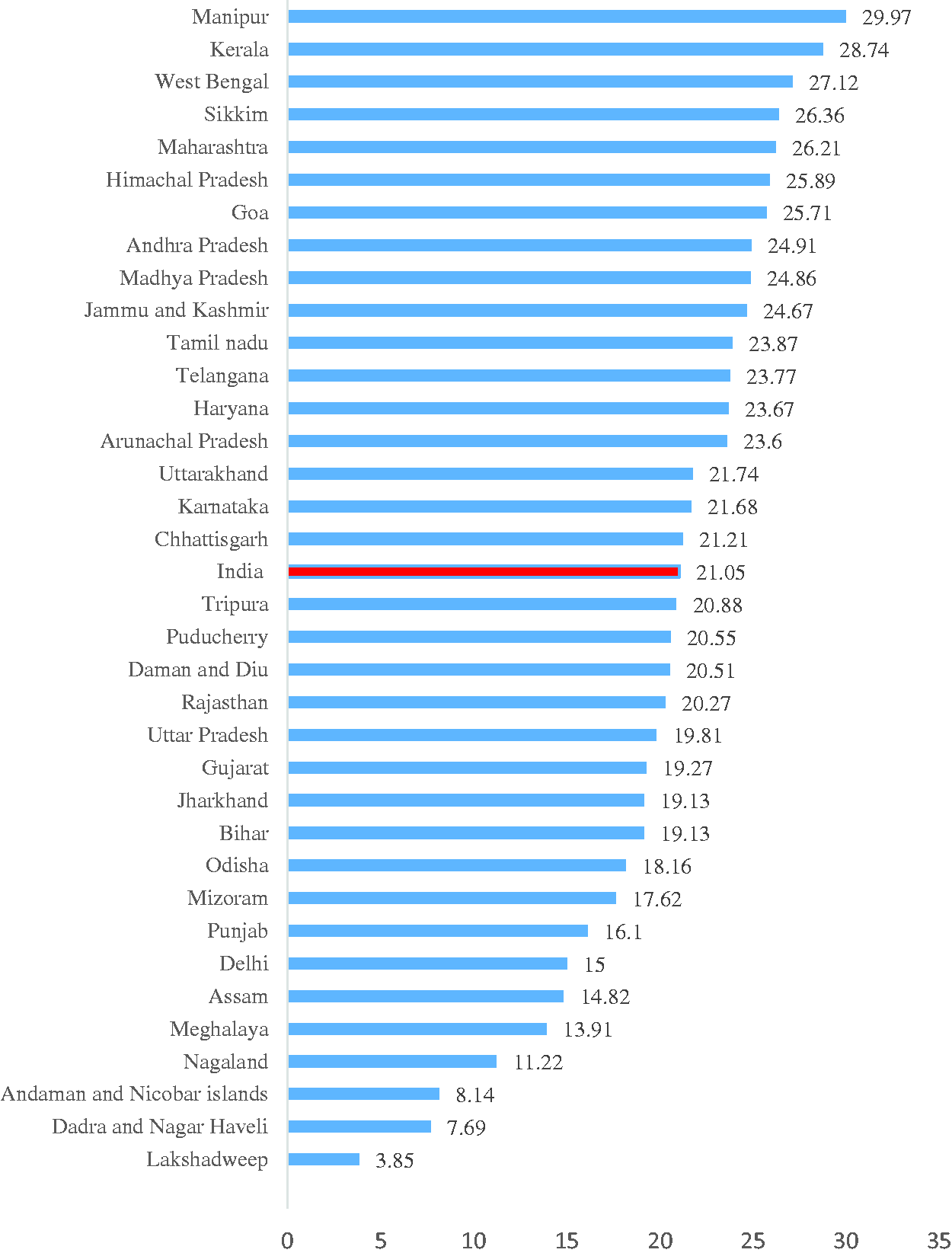
Percentage Distribution of Deaths due to External Causes Among Adults in Indian States.
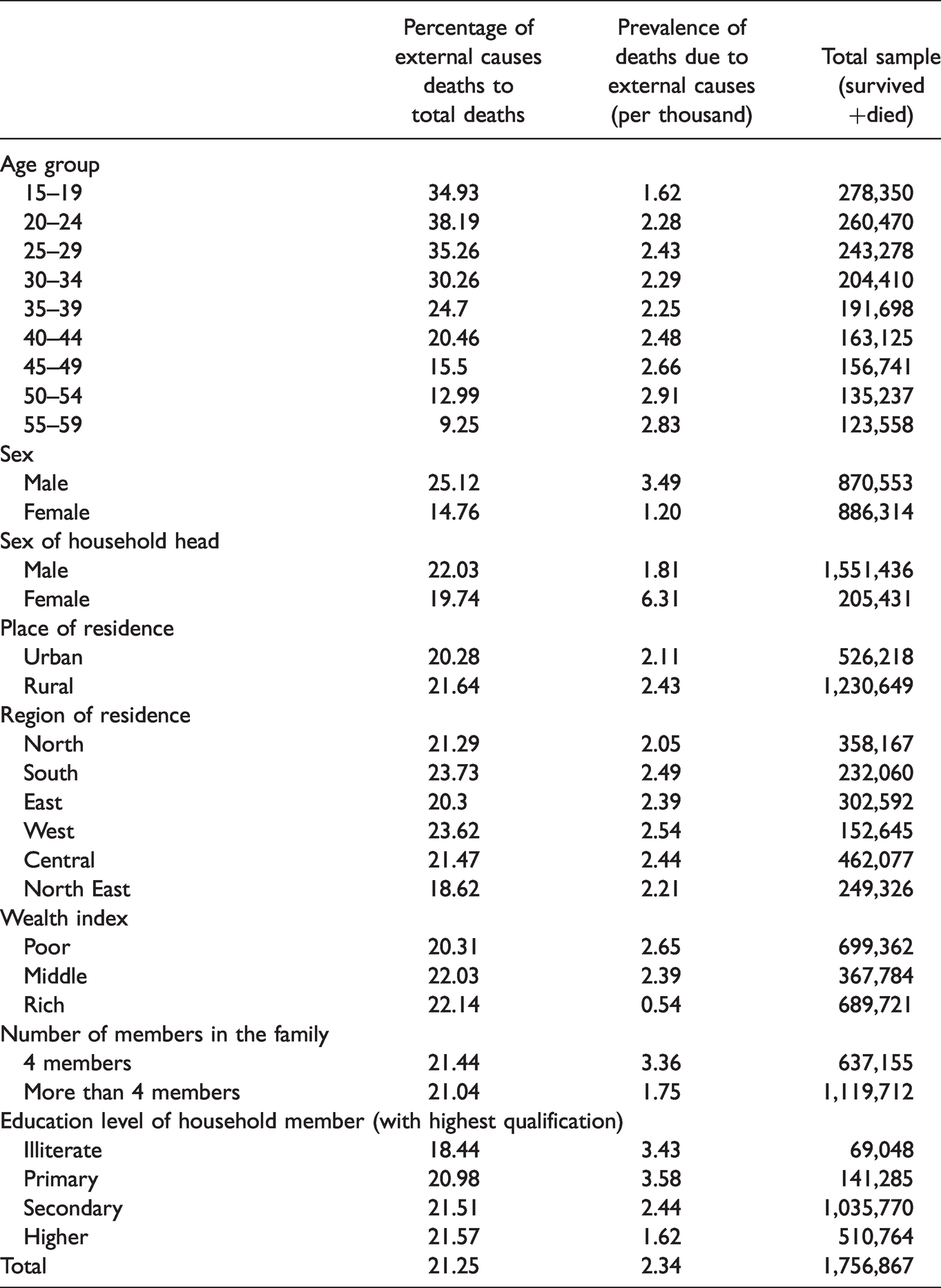
The deaths due to external causes among adults in India by socio-economic and demographic characteristics were shown in Table 1. The deaths due to external causes varied considerably with the age of the deceased. The table showed that with increasing age, the percentage of deaths due to external causes decreased. Here, 38.19 percent and 35.26 percent of the total deaths occurred due to external causes to people in the age group 20–24 years and 25–29 years respectively and then decreased to 9.25 percent in the age group 55–59. Although the percentage decreased 55–59 and 50–54 age group showed the prevalence of 3 deaths per thousand which were the highest prevalence of deaths due to external causes among all ages. The study also found that deaths attributable to external reasons varied by sex of the deceased. Almost 25.12 percent of the deaths among males occurred due to external reasons with the prevalence of almost 4 deaths per thousand compared to only 14.76 percent of the deaths among the females with a prevalence of almost one death per thousand. The percentage of deaths due to external causes was high in male headed households (22.03 percent) than the female headed households (19.74 percent) but the prevalence was found to be maximum in female-headed households (6 per thousand). The percentage and prevalence of Deaths due to external reasons were also high in the Southern (23.73 percent) and Western (23.62 percent) with a prevalence of approximately three deaths per thousand in both the regions and minimum in the case of North-Eastern (18.62 percent) and Eastern region (20.3 percent) with same prevalence 2 deaths per thousand population for both North Eastern and Eastern region. These deaths were slightly higher in rural (21.64 percent) than in urban areas (almost 20.28 percent) with almost the same prevalence of two deaths per thousand population. In case of wealth index, the prevalence of deaths attributable to external causes was minimum in case of people belonging to rich wealth quantile (less than 1 death per thousand population). The prevalence of deaths due to external causes was lowest among people living in highly educated households (less than 1 deaths per thousand people). Though the proportion was almost the same for persons living in smaller families (4 or fewer members) (21.44 percent) and larger families (more than 4 members) (21.04 percent), the prevalence of deaths due to external causes were more in persons belonging to smaller families (almost 4 deaths per thousand) than the larger families (almost two deaths per thousand population).
The Total Number, Prevalence Percentage of Deaths due to External Causes to Total Deaths in India Among Adults (15–59) by Different Socioeconomic and Demographic Characteristics.
The result of the robust Poisson regression analysis to find the socio-economic and demographic factors associated with the deaths due to external causes among adults was presented in Table 2. The present study found that with age the risk of deaths due to external causes was increasing but the relationship between age and risk of deaths due to external causes was not linear (clear from the variable age square with incidence rate ratio (IRR), 0.99, p < .05). Females were significantly 0.29 (p < .001) times less likely to die due to external causes than males. Adults belonging to female-headed households and rural areas were having significantly more risks (3.46 times and 1.14 times respectively) of deaths due to external causes. The risk of these deaths decreased with the increase in the number of family members. Here, the incident rate ratio was 0.89 (p <.001). People belonging to the Central and Western region and of India were having respectively 1.23 (p < .001) and 1.13 (p < 0.1) times higher risk and North Eastern region were having 0.12 times lower risk of deaths due to external causes than Northern residents. People belonging to households with at least one member having higher education (0.67, p <.001), were less likely to die from external causes than the households with illiterate members. The study also found that the risk of deaths due to external causes was significantly higher among persons from the household having access to at least one mass media source.
Robust Poisson Regression Results Showing the Risk Factors of Deaths due to External Among Adults in India.
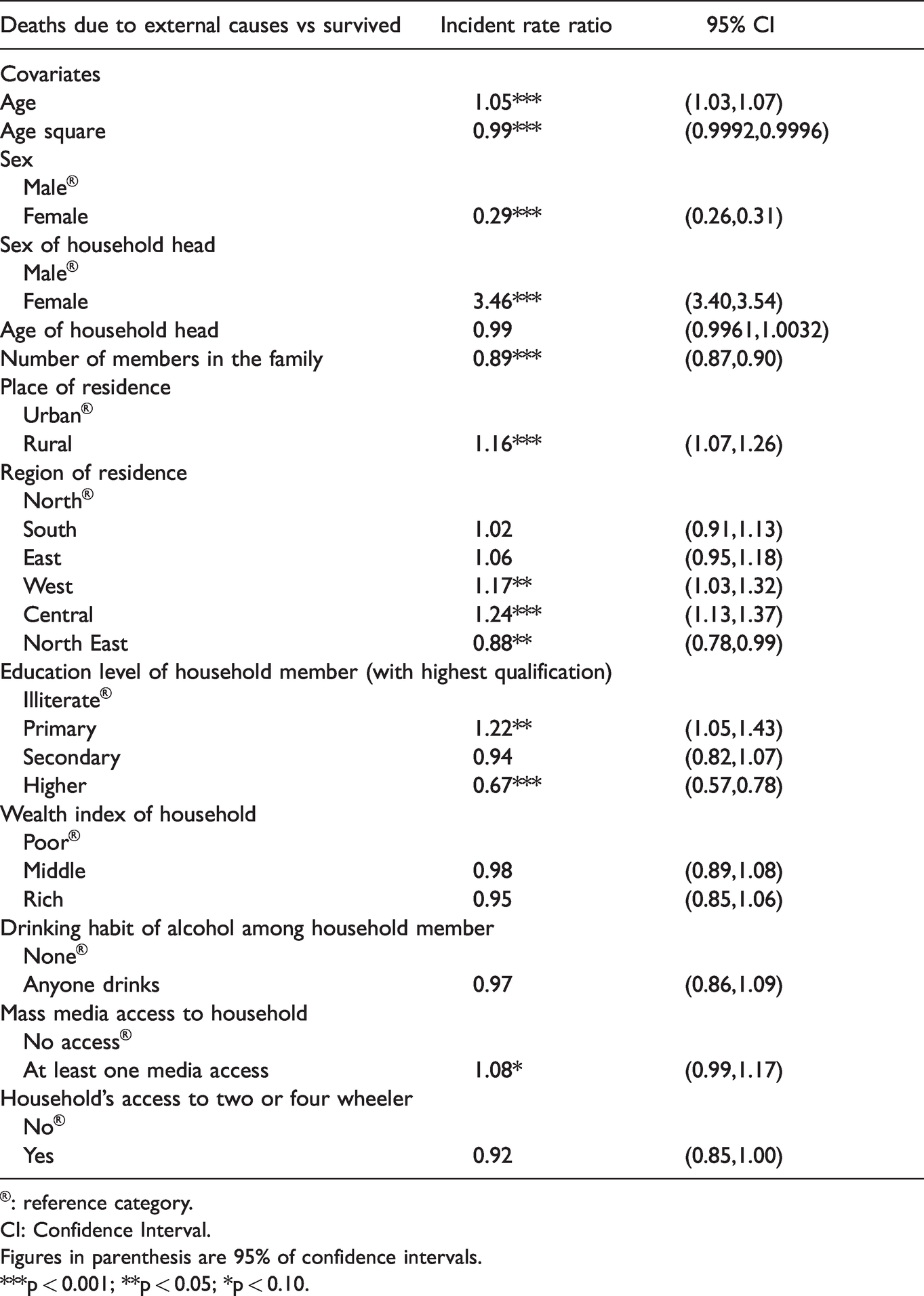
®: reference category.
CI: Confidence Interval.
Figures in parenthesis are 95% of confidence intervals.
***p < 0.001; **p < 0.05; *p < 0.10.
Discussion
The present study finds that the prevalence, as well as the risk of death during adulthood, are significantly higher among males. The studies of Sorenson (2011), Dannenberg et al. (1994) and Schnitzer and Runyan (1995), Moniruzzaman and Andersson (2008) signify that men are more likely to die of illness than women. Men's higher unintentional injury, suicide, and homicide mortality rates are being observed in all age groups in low, middle, and high-income countries. Men are more likely to be in circumstances that increase their exposure to injury risk (Sorenson, 2011). Some of the circumstances or situational factors result in extended exposure. Wilsnack et al. (2000) and Turner et al. (2004) found that gender and risk-taking are very closely linked and in the case of males it is positively associated with the injury. More than biological sex, the level of masculinity and the level of internalization of gender roles explain gender differences in risk-taking among adolescents as well as premature deaths (Granié, 2009). On the other hand, in the Indian context, women’s deaths particularly due to violence might remain underreported or misreported as the information was collected from the head of the household. Further, as died women might not be reported by the respondent owing to the overall lack of social importance given to the female gender in the Indian context. This study reveals that the higher risk of deaths due to external causes among youth aged 20–24 and then decreases with age. Several studies found youth at more risk of accidents, injuries (Peshin et al., 2014; Singh et al., 2018; Srivastava et al., 2005; MCCD report,2013) Singh et al. (2018) showed that deaths due to external causes are more among people belonging to the age groups 12–19 years and 20–34 years. Peshin et al. (2014) found the highest incidence of deaths due to poisoning occurred among people aged 18–35 years. Another study by Srivastava et al. (2005) reported the highest incidence of poisoning in the age group 14–40 years. MCCD report for the year 2013 also suggests that youth and adolescents (15–24 and 25–34) are more vulnerable to injuries and poisoning-related deaths.
This present study suggests a positive relationship between prevalence and risk of deaths attributable to external causes and female household-headship status. According to Kitulwatte et al. (2017), a study on the pattern of unnatural deaths due to external causes are also associated with family disputes, family pressures, and family position. Most of the Indian families are headed by men and in many households, adult women become head after the death of elder men. So, the higher risk of adult death in the female-headed households is because the head of these households might have changed after the adult’s death. Besides this, there are several reasons that members from female-headed households are vulnerable to external causes of death. Prior studies (Buvinić & Gupta, 1997) found that female headship and poverty were strongly positively associated in India. The authors found that female-headed households, despite their smaller size in comparison with other types of households, often carry a higher dependency burden than other households and the main earners of female-headed families were mostly women, who have lower average earnings than men. Since catering to individual demands and taking proper care are often not possible, they might feel neglected and subjugated which might lead to suicidal tendencies among them. Mental, emotional, and economic stress become the very plausible side-effects of the overburdened responsibilities they have to carry. On a societal ground, female-headed households are not much respected or looked upon by society as the male-headed households in India. This is also one of the major reasons that they also develop mental stress in their fight to get accustomed to it. Often children and youth who belong to female-headed families have to pursue a course that reduces financial burden and how fast they can be bread-earners for the family. The same thing happens if they have some unconventional dreams or career paths they wish to pursue, but due to financial constraints, they are not able to pursue them. These types of regrets and stress can remain for the entire life of a child born and brought up in such families. The amalgamation of all these factors can trigger suicidal tendencies in the minds of children of such families.
The lower prevalence and the risk of deaths due to external causes among the large size families is another important finding of this paper. Living with other family members can promote compliance with group norms, encourage health practices and reduce stress through emotional reassurance or a helpful appraisal of difficult situations. Also, family members can exercise some measure of social control, for example, by discouraging behaviours such as smoking, drug abuse, excessive alcohol consumption, and promoting behaviours such as maintaining regular exercise and sufficient rest (Antonucci, 1990; Saikia & Ram, 2010).
This study shows a significant association between household wealth and the prevalence of adult mortality due to external causes but the relationship is not significant with the risk of deaths due to external causes. Individuals from affluent families are generally not exposed to extremely hazardous and laborious work such as working in construction sites, factories, where the chances of meeting with external accidents are significantly high. Also, since financial security is mostly with the rich section, so they are less prevalent for getting stressed due to financial factors and also die from external causes as compared to the poor or middle class. The present study further implies that rural residents are more prone to die due to external causes. Both crude and age-adjusted injury death rates were higher in rural areas than in urban areas and it was true for both developing and developed countries (Hu et al., 2010; Jiang et al.,2011; Moshiro et al., 2005; Ostry, 2009) like Australia (Mitchell & Chong, 2010), Ireland (Boland et al., 2005), Canada (Ostry, 2009). According to Hu et al. (2010), intentional suffocation, drowning, transportation incidents, and suicide not only were the major causes of deaths due to external causes but also play a key role in explaining the urban‐rural disparities in fatal injuries. The present study finds that people belonging to the Central and Western region of India are having significantly higher risk k of deaths due to external causes than Northern residents. Singh et al. (2018) found that deaths due to non-medical reasons for people in the age group 12 years and above were high in the eastern, western, and southern regions of India compared with the northern regions.
It was found from the present study that people belonging to households with at least one member having a higher education are less likely to die from external causes than the households with illiterate members. Education, being one of the three basic indicators for measuring the socioeconomic status of an individual, and it has significant importance for mortality differentials (Kitagawa & Hauser, 1973; Saikia & Ram, 2010; Schwarz, 2005). A study by Perez and Turra (2008) reveals that the risk of adult deaths in the lowest educational group is about twice as high in Brazil as in the highest educational group. Educated people are generally more informed and conscious about how to avoid external injuries (like obeying traffic rules), hence the risk is less for them.
The present study also results in a greater risk of external deaths with at least one mode of usage of mass media. As the age of the internet and electronic devices are blooming, using them has almost become an integral part of our lives. It is often seen that usage of mobile, internet and related stuff in the streets is leading to accidents and resulting in unnatural deaths. Similarly, the impact of movies, television serials, and television series create a massive impact in the minds of young people which goes a long way in influencing their decisions in important aspects of life. Judicious usage of all these resources is mostly absent which leads to the magnification of the negative impact it is creating. It is almost like a double-edged sword- if one knows how to use both sides efficiently, then it’s a great weapon to have, but it has also got the potential to significantly harm him if used wrongly. Cybercrime is also on the rise. There is a lot of data available on the internet, and thanks to mobile networks, internet data has become very cheap in recent times. The misuse of this internet data is on the rise. Cybersecurity, though has gone through massive up-gradation in recent times, is still liable when used by people not aware of its whereabouts. As a result, people receive online threats and there is always a possibility of personal data and confidentiality getting breached. Bank frauds are a common thing nowadays, and things like this affect people’s minds the most in a negative way. This social media and internet age has got so intricately associated with lives that even the sudden fake news of some information leaking or a fraud in this sector has enough potential to turn lives in the wrong way. People, who experience this, often get so stressed, that it leads to suicidal tendencies and hugely negative thoughts in their minds. In a conclusion, anything going in the wrong direction in life can attack the fragile minds and can lead them to head towards a potential disaster. This research rejects the proposition that the drinking behaviour (drinking alcohol) of household members might have led to a higher risk of external deaths among adults. Further, the research found no significant association with owning a motor vehicle by the household.
Apart from the new findings discussed above, the study could not assess the determinants of different causes- accidents, violence, poisoning, homicide, poisoning separately as NFHS data did not include separate questions on these causes. Further, adult mortality particularly due to the external causes is under and misreported reported Rukmini, 2016).
So the prevalence that the study estimated will be at a lower level. There can be an issue with data quality (under/miss reporting) in domestic violence deaths, specifically of women. Thirdly, except for age and sex, this data did not provide any information about the deceased. The assumption was made about his/her socio-economic and lifestyle behaviours from the other members of the households. This assumption might be incorrect in many cases. Nevertheless, the findings with the limited information based on the first time asked question in the large scale survey have been presented and discussed with the literature support.
Conclusion
The present study has documented the prevalence and the determinants including socio-economic, demographic, and behavioural factors of adult mortality due to external causes that constitute around 21.25% of total deaths among adults (15–59 years) in India. The prevalence of deaths due to external causes is more among men, people living in female-headed and poor households, generally from rural areas, are from Western and Southern regions of India, with no education and having four or more family members. It is found that the determinants of externally caused adult mortality are many and diverse. The study finds that the risk of deaths due to external causes is more among men, persons belonging to rural areas, living in the central and western region of India. Further, it is higher among persons living in smaller family size households and the households that is having access to at least one mass media. Another crucial finding is that risk of deaths due to external causes is higher among persons belonging to a less educated family.
The association of these factors with adult mortality due to external causes remains considerable even after controlling for the other variables. Socio-economic status like the educational qualification of household members has a close association with adult deaths. The educational composition of households is also a key factor influencing adult mortality, the improvement of which can substantially reduce premature adult deaths in India. About social factors, family structure is associated with adult mortality, substantially by intervening in certain socio-economic sectors. Mass media access is also linked with adult mortality due to external causes, they should be used properly to reduce the deaths due to external causes.
The complete elimination of these deaths due to external causes is not possible but it can be minimized. According to Smith et al. (2009), to effectively optimize premature mortality due to external causes, ongoing national efforts need to be strengthened and supplemented with effective innovative actions. Some of these actions can include premature death as a performance measure at the national and provincial levels and setting appropriate targets, which offers policymakers a major opportunity for securing health system improvement and accountability. Deaths due to external causes among adults are also associated with stress. For them, free counseling services can be arranged according to their convenience. It is suggested that like National Health Policy, the Mental Health policy should be implemented and brought into action to bring about a change in the scenario. There is a need for regular monitoring of deaths due to non-medical reasons in India and its states to better guide the national and state policies related to health and health behaviour. Also, stringent laws need to be exercised to capture the correct data of deaths due to external causes. It is a matter of great concern that about 62.5% of all deaths due to external causes are attributed to unnatural accidents. Hence, a proper investigation should be done to unearth the exact reasons behind this and appropriate steps should be taken by the government and the concerned authorities to reduce them. Most of the sources underreport the actual data and due to the absence of adequate laws, there are instances where deaths due to domestic crimes like homicide or torture are likely to be hidden to avoid police harassment and social isolation, specifically in rural areas. Efforts should be made to collect the data as accurately as possible because it is only when the actual data is available, policies can be implemented efficiently, thus positively affecting millions of lives and improving the efficiency of the system as a whole.
Footnotes
Acknowledgments
We thank the reviewers from the journal for giving their useful comments for the improvement of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.