
Abstract
This study aims to determine the meaning of death for nursing students and their attitudes toward dignified death principles. The descriptive study was conducted with nursing students studying at a state university in Turkey. The data were collected using the Personal Information Form, the Personal Meanings of Death Scale (PMDS), and the Assessment Scale of Attitudes toward the Principles of Dying with Dignity (ASAPDD). A positive and low-level significant relationship was determined between the students' age and the scores for the PMDS subdimensions and the ASAPDD. It was found that the students had positive perceptions of death and adopted the principles of a dignified death. It was determined that an increase in the students' perceptions of death positively affected their adoption of the principles of a dignified death.
Death, one of the most real and universal events of life, is the inevitable end for every living creature (Cerit, 2019; Wang et al., 2020). Although it will be experienced by all living beings, death has a different meaning for each individual (Gül et al., 2020). Depending on the age, cultural values, beliefs, and lifestyle of each individual, the perception of death may differ (Bužgová, & Janíková, 2019). In this context, some people think that death is painful and fear death, while others may see death as salvation (Cerit, 2019). The thought of death or dying can sometimes be perceived as an individual's meeting with a loved one or God. This situation can positively affect people's behaviors and lifestyles. However, the thought of death can sometimes emerge as an excessive and pathological fear that can seriously disrupt the life balance and harmony of the individual (Bilge, Embel, & Kaya, 2013).
Because death is a subject surrounded by obscurity, looking after the dying is an important but difficult part of the nursing profession (Österlind et al., 2016). Terminal patients often face many physiological, psychological, and social difficulties because death is inevitable, and they may become dependent on other individuals (Pehlivan et al., 2020). Nurses often have to provide care to patients who are terminally ill or dying in their work environment (Abu-El-Noor & Abu-El-Noor, 2016). This situation causes nurses to encounter death more frequently than other people and to be affected by death (Tüzer et al., 2020). Nurses with high death anxiety may experience emotional difficulties in their work environment. As a result, they may avoid providing care to terminally ill or dying patients. They may try to provide more physical care by ignoring the psychosocial and mental needs of these patients. This may negatively affect the quality of care that nurses provide to patients (Bužgová, & Janíková, 2019; Peters et al., 2013).
Nursing students face experiences of death and dying patients that are similar to those of graduate nurses. Death is a source of great sadness, despair, worry, and fear for nursing students who encounter the reality of death for the first time during their clinical practice (Kim, 2019; Özveren et al., 2020). It is known that students in particular have difficulty accepting the phenomenon of death and coping with its reality. Due to their inexperience in caring for dying patients, they may avoid facing death and not be ready to care for these patients (Bailey & Hewison, 2014; Berndtsson et al., 2019; Jafari et al., 2015). As dying patients want to die in dignity and peace, being taken care of in accordance with ethical standards, student nurses need to recognize their feelings and perceptions of death so that they can meet these patients' needs (Cerit, 2019).
To increase the quality of care and cope with feelings of failure, nursing students who encounter the phenomenon of death must be aware of their attitudes toward dignified death and be able to make sense of death. A dignified death of an individual may involve maintaining autonomy and privacy until the end of their life, avoiding suffering, being with their loved ones, accepting death, and receiving peaceful care in a safe environment (Duru Aşiret et al., 2020; Gurdogan et al., 2017). Since death is inevitable for all living beings, the importance of the concept of human dignity in end-of-life care is indisputable. Providing appropriate care to dying patients and their families by ensuring their dignity is one of nurses' professional roles (Hemati et al., 2016). In 1992, the World Health Organization and the European Medical Association recognized that patients have the right to die with dignity. In 1999, 12 dignified death principles were defined by the Debate of the Age Health and Care Study Group (Duru Aşiret et al., 2020). The American Association of Colleges of Nursing is working to contribute to the quality of care for terminal patients and their families. It has defined dignified death as involving physical comfort, autonomy, readiness, and effective interpersonal relationships, together with the unconditional acceptance of human qualities (Cura, 2020). An individual whose death is approaching deserves a dignified death, and a dignified death is also a fundamental human right (Duru Aşiret et al., 2020). In addition, the principle of individual dignity, which is one of the fundamental values of nursing practice, is a component of the International Coucil of Nurses Code of Ethics. Although dignified death is the main goal of quality end-of-life care (Guo & Jacelon, 2014), nurses' attitudes toward dignified death can positively affect the quality of care (Gurdogan et al., 2017).
Everyone has the right to receive holistic, sensitive, and respectful care. This right has become more important due to the scarcity of time that can be spent with terminally ill patients. While nursing students have to care for terminally ill patients, they may also face their own emotions (Menekli & Fadıloğlu, 2014). Being aware of how students perceive death will affect the quality of care nurses will provide to the terminally ill. In addition, student nurses need to provide effective care by valuing the individual's dignity and uniqueness, knowing that each individual deserves a dignified death just as they deserve a dignified life. Thus, the nurse fulfills the ethical, conscientious, and professional responsibilities expected of her. In this study, the aim was to reveal the meanings of death and the attitudes toward the principles of dignified death in the case of nursing students who will provide care to dying patients during their student years and work life.
Methods
This descriptive study was conducted with students studying at the nursing department of a state universityin Turkey between February 20 and March 10, 2020. A total of 683 students were enrolled in the Nursing Department in the spring semester of the 2019–2020 academic year. The plan was to reach all students without choosing a sample for the study. During the research period, 493 students attending the classes agreed to participate in the study and completed the forms included in the study (participation rate 72.2%). The questionnaires were filled out by participants under direct observation. Students studying nursing in undergraduate departments start hospital practice during the first year's spring semester. During their hospital practice, students care for terminal patients and can witness the deaths of patients. This situation can sometimes be wearing for them. However, the perception of death as a natural process encountered as a result of life helps nursing students to understand death by reducing their experiences of negative situations such as fear and stress concerning death. This helps students provide better quality care to terminal patients by making them understand the necessity of dignity in death, just as in life (Köse et al., 2019; Uysal et al., 2019). For this reason, the study was planned to determine the meanings of death for nursing students and their thoughts regarding dignified death.
Instruments
Data were collected using the following tools: the Personal Information Form, the Personal Meanings of Death Scale (PMDS), and the Assessment Scale of Attitudes toward the Principles of Dying with Dignity (ASAPDD).
Personal Information Form: This form, which was prepared by the researchers in line with the literature, consisted of two parts. In the first part, there were questions about the students' age, gender, and the class they are educated. In the second part, items were included regarding the death status of a close relative, the state of providing care to a terminal patient, finding caring for a dying patient emotionally exhausting, the state of having a deceased patient, and the strongest emotions they had felt after the death of a deceased patient (if they had experienced this).
Personal Meanings of Death Scale (PMDS): This is a scale developed by Cicirelli (1998) to measure meanings attributed to death (Cıcırellı,1998). A Turkish validity and reliability study of the scale was conducted by Koçanoğlu in 2005. The PMDS is a 5-point Likert-type scale consisting of 15 items with three subdimensions: extinction (5 items), life after death (3 items), and motivation/leaving meaningful things behind (7 items). There is no total score obtained from the whole scale. High scores obtained from the subdimensions express the meanings that individuals give to death. In Koçanoğlu’s (2005) study, the Cronbach’s alpha reliability coefficients for the PMDS subdimensions of extinction, motivation/leaving meaningful things behind, and life after death were found to be 0.78, 0.72, and 0.82, respectively (Koçanoğlu, 2005).
Assessment Scale of Attitudes toward the Principles of Dying with Dignity (ASAPDD): This scale was prepared by the Elderly Health and Care Working Group in 1999. It is based on 12 principles included in the Future of Health and Care of the Elderly report. The ASAPDD is a 5-point Likert-type scale with 12 items consisting of positive statements. The total score that can be obtained from the scale varies between 12 and 60. The more the principles of a respectful death are adopted, the higher the score on the scale. The Turkish validity and reliability of the scale were established by Duyan, and the Cronbach's alpha coefficient was found to be 0.89 (Duyan, 2014).
Data Analysis
The IBM SPSS 22.0 (Statistical Package for Social Sciences 22.0) package program was used to analyze the data. In the analysis process, first, the Kolmogorov–Smirnov test was performed for the normality distribution of the variables. As a result of this test, it was determined that the data did not conform to a normal distribution and that non-parametric tests should be used. Therefore, ın the data analysis, descriptive (numbers, percentages, mean values, standard deviation), and comparative statistics (Mann Whitney U Test, Kruskall Wallis test) were used. The correlation between scale scores was evaluated using Pearson's correlation coefficient, with p < 0.05 being considered significant in this study.
Ethical Approval
To conduct the study, written approval was obtained from the Scientific Research Ethics Committee of the Trakya University (TÜTF-BAEK 2020/60, decision number: 03/02) and the relevant institution. The written informed consent of the students was obtained using the Informed Consent Form.
Results
Of the students participating in the study, 82.2% were female, and 66.9% of them stated that they had witnessed the death of a close relative. There was no statistically significant difference between gender and experiencing the death of a close relative in either the PMDS or the ASAPDD scores (Table 1).
Relationship Between Some Characteristics of Students and PMDS and ASAPDD (n = 493).

Note. PMDS= Personal Meanings of Death Scale, ASAPDD= Assessment Scale of Attitudes toward the Principles of Dying with Dignity. *Mann Whitney U Test, ** Kruskall Wallis Test.
Statistically significant values (p < 0.05) are shown in bold.
Of the students, 30% were first-year students. A significant relationship was found between students' classes and the scores for the life-after-death subdimension of the PMDS and the ASAPDD. It was determined that third-grade students received the highest scores for both scales (Table 1).
Of the students, 50.3% stated that they had provided care to a terminal-period patient during their educational lives, and 71.4% of them found caring for the dying patient emotionally exhausting. The ASAPDD scores of the students who cared for terminal patients and found that the care was heavy were higher than those of the other students (Table 1).
Of the students, 48.5% stated that they had patients who had died, and 63.6% of these stated that they experienced the most powerful grief and sadness after their patients' deaths. The ASAPDD scores of the students who had a deceased patient and of the students who felt guilt-failure as their strongest feeling after their patients' deaths were found to be higher than the scores for the other students (Table 1).
The mean age of the students was 20.12 ± 1.80. The students' PMDS subdimension mean scores were 3.45 ± 0.89 for the extinction subdimension, 3.78 ± 0.84 for the life-after-death subdimension, and 3.64 ± 0.72 for the motivation/leaving-meaningful-things-behind subdimension. The mean score for the students' ASAPDD was 46.29 ± 7.64. In addition, a low level of positive correlation was found between the ASAPDD total score average, age, and all subdimensions of the PMDS (Table 2).
Correlation Between Students’ Age and Scale Score Averages and the Relationship Between These Variables.
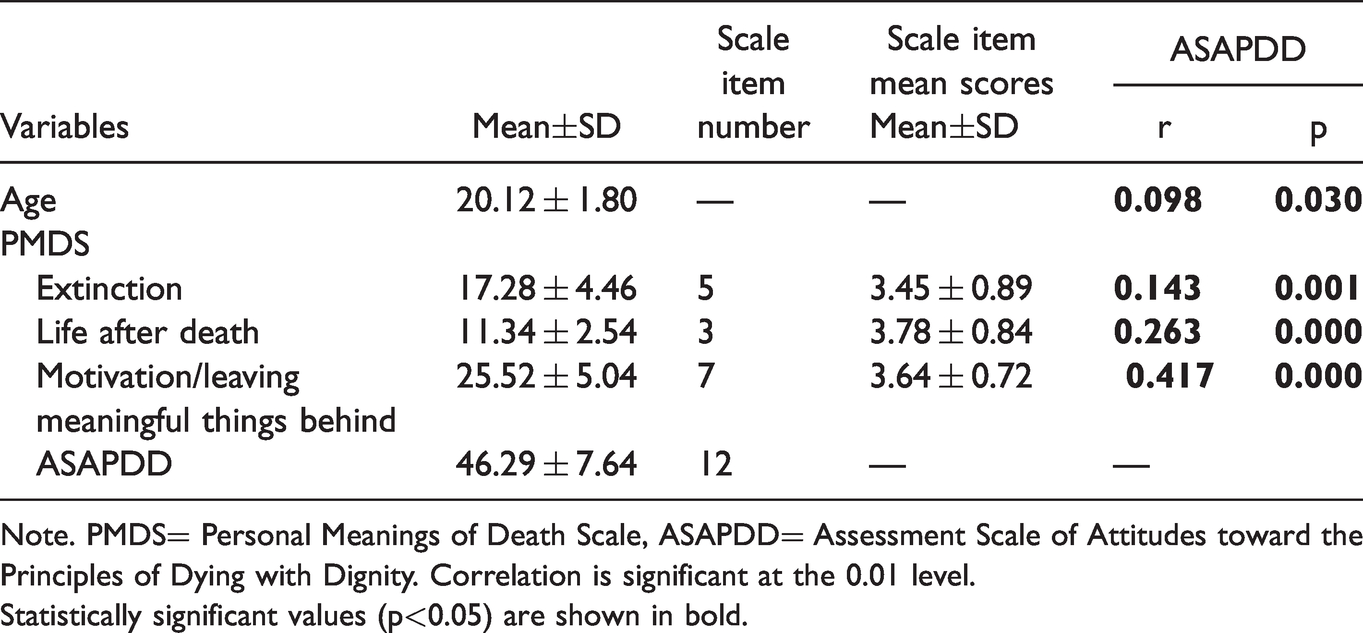
Note. PMDS= Personal Meanings of Death Scale, ASAPDD= Assessment Scale of Attitudes toward the Principles of Dying with Dignity. Correlation is significant at the 0.01 level.Statistically significant values (p<0.05) are shown in bold.
Discussion
The meanings given to death by individuals can be affected by religion, culture, beliefs, traditions, the life periods of the individuals, and their personal experiences (Duyan, 2014; Kavalalı, 2019). It is believed in Muslim societies, including where this study was conducted (Karadag et al., 2019), that death is an undeniable fact that is not extinction but rather gives people eternal life (called the hereafter) (Betriana & Kongsuwan, 2019; Pehlivan et al., 2020). A study reported that most of the nursing students accepted death as the beginning of a new life (Şahin et al., 2016). Similarly, in another study, in which students' perceptions of death were investigated through metaphors, it was determined that students defined death as a new beginning (Teskereci et al., 2020). In this study, the highest score of the students in the life-after-death subdimension of the PMDS was thought to be related to the fact that the study was conducted in a Muslim society and that Muslims believed that there is life after death.
The concept of a dignified death can vary from individual to individual. The ASAPDD scores of the students in this study showed that the nursing students adopted the principles of a dignified death. Similar results were found in the study of Gürdoğan et al. conducted with nurses, which stated that nurses' knowledge of the principles of a dignified death would enable individuals to be prepared for death by taking care of them in a way that befits human dignity (Gurdogan et al., 2017). A study conducted by Aşiret et al. with nursing students determined that the participants had a positive attitude toward good death principles (Duru Aşiret et al., 2020).
Another finding was that there was a significant relationship between the students' classes and the life-after-death subdimension of the PMDS with regard to death meanings and dignified death principles. It was determined that the final-year students received higher scores on both scales than the first-year students. In the study of Cura, it was determined that fourth-grade students showed a more positive attitude toward a dignified death (Cura, 2020). In another study, a positive correlation was reported between nurses' working years and their ASAPDD scores, and it was stated that nurses with more experience had a more positive attitude regarding dignified death (Gurdogan et al., 2017). In addition, the existence of a significant relationship between students' age and ASAPDD scores indicated that these two findings support each other. Studies have reported that as the ages of student nurses and nurses increase, their attitudes toward death change, and they therefore exhibit more positive attitudes while caring for dying patients (Grubb & Arthur, 2016; Hagelin et al., 2016; Lange et al., 2008). In the study conducted by Sharour et al., it was reported that young students' thoughts about dead patients were more negative, while an increase in academic level and experience supported students' positive attitudes (Sharour et al., 2017). The situation in our study, which was found to be similar to that described in other literature, was thought to be due to the fact that the students in our study provided care to more dying/deceased patients as their classes and ages increased, and they thus developed more awareness.
Today, since most deaths occur in hospitals, nurses frequently encounter patients who are dying (Loerzel & Conner, 2016). Students can often provide care to terminal patients in the hospital and witness their patients' deaths, and it is reported that this situation increases death anxiety (Şahin et al., 2016). In the present study, it was determined that almost half of the students provided care to terminal-period patients, and nearly three-quarters of them found this situation wearing. It was also found that these students had higher ASAPDD scores than the other students. There are a limited number of studies on dignified deaths in the literature. In one of these studies, it is stated that end-of-life care is an important predictor for adopting the principles of a dignified death (Dag & Badır, 2017). A different study determined that 41% of the nursing students experienced patients' deaths, but the majority were not ready to care for dying patients and their families (Heise et al., 2018). In line with these findings in the literature, the awareness of the students who cared for terminal patients and who stated that this care was wearing was higher than that of the other students. This suggests that even if the death incident is an unwanted and negative situation, it can be an important lesson for students in learning the principles of a dignified death.
Death puts emotional pressure on nurses. Caring for a dying patient and their family makes a nurse feel emotionally stressed and conflicted (Becker et al., 2017). Nursing students have little experience in caring for dying/deceased patients. It is known that students have difficulties coping with death and do not feel comfortable caring for dying patients (Österlind et al., 2016). In addition, it is stated in the literature that students who care for a terminal patient experience fear, helplessness, guilt, and sadness and feel weak, inadequate, and unprepared in the face of this situation (Berndtsson et al., 2019; Heise et al., 2018; Loerzel & Conner, 2016; Martí-García et al., 2020; Wang et al., 2017). In a qualitative study conducted by Gül et al. (2020) it was determined that the strongest emotions nursing students felt after their death experiences were fear, helplessness, and sadness (Gül et al., 2020). It was reported in the study conducted by Şahin et al. (2016) that most of the students felt sadness after the death of a patient to whom they gave care (Şahin et al., 2016). In this study, it was determined that approximately half of the students had a deceased patient and that the strongest feelings they felt after death were grief and sadness, which is similar to findings in the literature. It was also seen that the students who had a deceased patient and who felt post-death failure, guilt, and anxiety had significantly higher ASAPDD scores, supporting previous study findings. This shows that although caring for terminal patients and having a sense of death made students struggle psychologically, the students gave importance to the preparation of individuals for death by providing quality, dignified, and respectful end-of-life care.
Kübler Ross described death as not a catastrophe and not a destruction but as one of the most constructive, positive, and creative elements of culture and life. This description tells us that death is a process that should be perceived as positive (Cerit, 2019). Accepting death as a positive situation can help the nurse feel better and provide better quality and dignified care (Pehlivan et al., 2020). Studies have found that nurses working in the intensive care unit have a high level of adoption of the principles of dignified death, and it has been reported that nurses have a sensitivity toward human dignity (Çelik, 2019; Köse et al., 2019). In this study, a low level of correlation was found between the motivation/leaving-meaningful-things-behind subdimension of the PMDS, the PMDS life-after-death subdimension, the extinction subdimension, and the ASAPDD scale. In line with these results, it was seen that students could perceive death differently, but nonetheless, all the students were aware of the autonomy, dignity, and uniqueness of the individual during the death process.
Conclusion and Recommendations
As a result, it can be seen that the students attributed different meanings to death, mostly in terms of life after death. Moreover, the fact that the students received the lowest score in the extinction subdimension showed that their perceptions of death were positive. The students' high ASAPDD scores were important in terms of showing that they were aware of the importance of dignity in death and life. It is anticipated that the greater the education that students receive and the more they encounter terminal illness and death, the more they become aware of the principles of a dignified death and provide patient care accordingly. It should be kept in mind that death is devastating for all individuals, and nursing students often witness death in their vocational education for the first time. For this reason, it is recommended that students be supported in the subjects of death and caring for dying patients, allowing them to create positive perceptions of death and adopt the principles of dignified death in their vocational education.
Limitations
The results of this study cannot be generalized because the study was carried out in a single center, the study was based on students' self-reporting, and there were many different factors (religious beliefs, cultural values, social values, family structure, etc.) affecting their views about death.
Footnotes
Acknowledgments
The authors thank all the students who participated in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Before starting the study, approval was obtained from the Trakya University Faculty of Medicine Non-Invasive Clinical Research Ethics Committee.