
Abstract
Considerable effort has gone into studying bereavement in children, adults and the elderly, but few studies have investigated the effects of bereavement or grief interventions in young adults. Even fewer studies have reported on the effect of interventions for young adults with grief complications. The present study seeks to help fill this gap by describing a Danish treatment program specially developed for young adults with complicated grief reactions. The dual process model of coping with bereavement, psychodynamic theory, and a narrative approach provide the foundation for the treatment. In addition, it utilizes an eclectic use of techniques and a group treatment modality that involves providing individual therapy within a group context. The core elements of the treatment are discussed and then exemplified in two case studies.
Keywords
Introduction
The Danish National Center for Grief is a non-profit organization that provides specialized grief therapy free of charge to bereaved children and young people, ages 6 through 27 years, in three outpatient clinics in the cities of Copenhagen, Aarhus and Odense. The center has been in existence for over 20 years, and is funded through governmental and private funds. This paper describes the center’s group therapy program for parentally bereaved young adults, ages 20 through 27 years, which incorporates the dual process model of coping with bereavement (Stroebe & Schut, 1999), psychodynamic theory as applied to grief therapy (Rubin, 1999), and a narrative approach (R. A. Neimeyer, 2000). We review theoretical rationale, discuss therapeutic tools used, and provide two case examples for illustration. A recent study of the effect of this treatment method found statistically significant treatment effects, in terms of reduction in symptoms of prolonged grief, posttraumatic stress, and depression. The effect was assessed by comparing pre- and post-scores on outcome measures of clients who received therapy and clients who were on the waiting list prior to receiving treatment. The results of this intervention study will be presented in a separate publication.
At this point it is well-established that losing a parent early in life (0–18 years of age) is associated with increased vulnerability and risk of adverse effects both in the short- and long-term (Bergman et al., 2017; Luecken & Roubinov, 2012; Rostila & Saarela, 2011). For example, bereaved children have been found to be at increased risk for mental health problems (Lundberg et al., 2018; Nickerson et al., 2013), increased mortality risk during childhood, adolescence and into early adulthood (Li et al., 2014; Rostila & Saarela, 2011) and increased long-term suicide risk (Guldin et al., 2015). The loss of a loved one during adulthood (age 18 and older) has also been found to be associated with increased risk of mental and physical health problems and mortality, including death by suicide (Guldin et al., 2017; Stroebe et al., 2007). Studies that have investigated the consequences of bereavement specifically during young adulthood (approximately ages 18 to 25) have found bereavement to be associated with increased mental health problems, including low self-esteem and low life satisfaction (Lundberg et al., 2018; Mash et al., 2014). It has been found that bereavement in young adulthood may be associated with academic difficulties, and disruption in developmental, occupational, and social tasks (Hardison et al., 2005; Janowiak et al., 1995).
In part to try to medicate the long-term adverse effects of bereavement, there has been a growing interest in developing and evaluating psychological interventions for bereaved people, especially for those with what has been called complicated, prolonged, persistent complex or pathological grief (Lenferink et al., 2019). Recent systematic reviews and meta-analyses have found support for psychological intervention for bereaved adults with prolonged or persistent grief responses (Johannsen et al., 2019; Maass et al., 2020; Wagner et al., 2020). Most grief interventions and effect studies today have focused on a broad age group of adults aged 18 years or older. Grief therapy specifically targeting parentally bereaved young adults has largely been ignored (Mash et al., 2014). This is potentially problematic, as it seems possible that a bereaved 25 year-old might have a different experience with the loss and thus different treatment needs compared to those bereaved at for example 55 or 82 years of age.
The Danish National Center for Grief offers a treatment program specifically developed for bereaved young adults (age 20 through 27 years). It was developed with their developmental needs in mind and an understanding of the challenges they face, as they work to transition from childhood to adulthood (e.g., in terms of identity formation, social needs, and finding their path in life). The purpose of this paper is to describe the intervention. We first describe the targeted client population. Then we describe the structure and content of the therapy, followed by a discussion of the treatment’s underlying theoretical foundations and essential therapeutic tools. We end by providing two clinical case examples for illustration.
Description of the Client Population and Enrollment Procedure
On an annual basis, approximately 180 parentally bereaved young adults between the ages of 20 and 27 years receive outpatient psychotherapy at the Danish National Center for Grief with. They have lost one or both parents due to physical illness, accidents or suicide, and struggle to cope with their losses. They are typically self-referred or referred by their general practitioner, a social worker, or a guidance counselor.
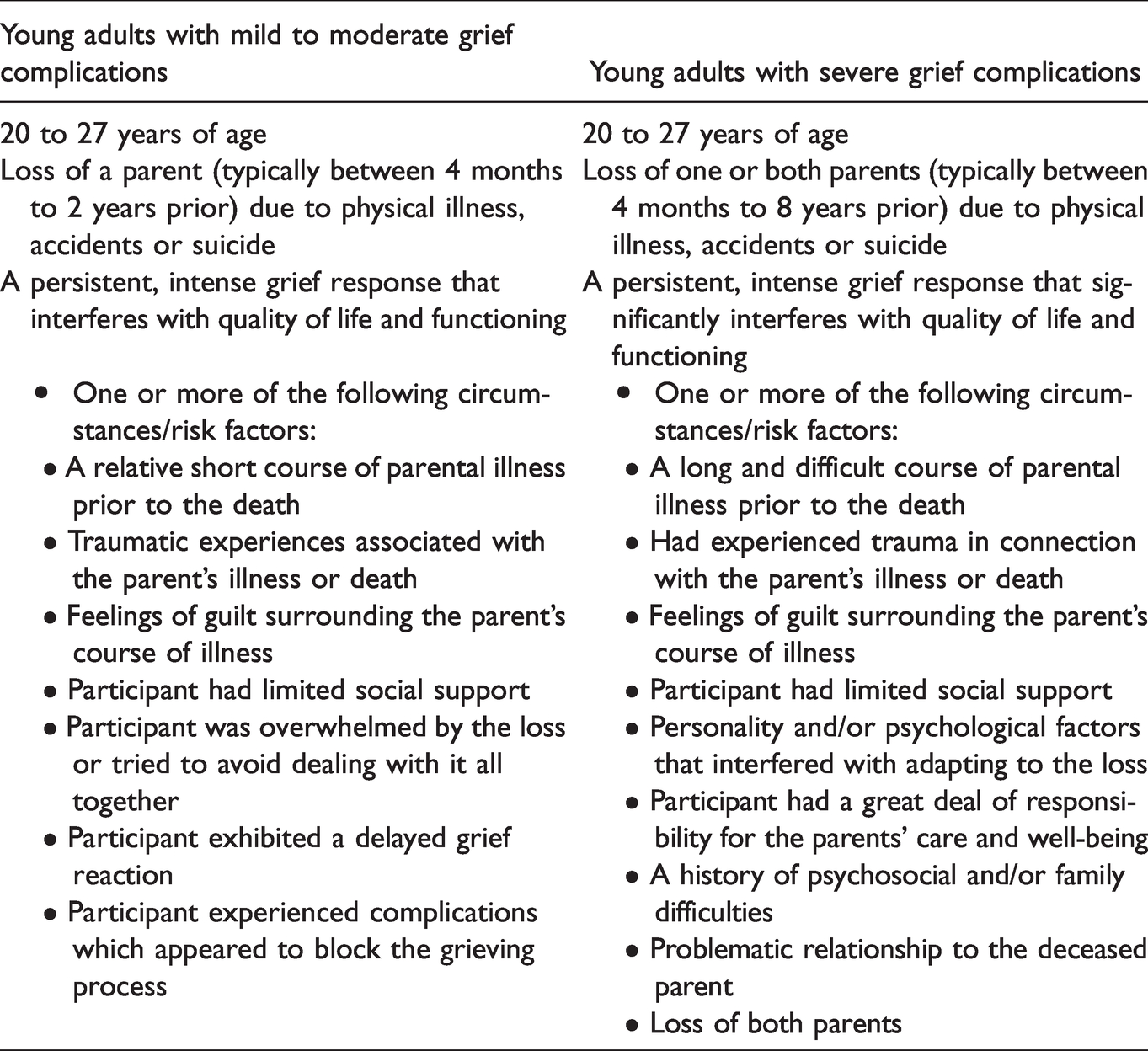
Eligibility for the treatment is determined through an initial telephone screening and a subsequent clinical interview, both completed by a psychologist. During the telephone screening, a preliminary determination is made as to the client’s potential eligibility, level of clinical need, and motivation for treatment. Those who proceed to the subsequent clinical assessment participate in a semi-structured interview. The timing of the clinical assessment is such that at least three months have passed since the death. The interview format has been developed by psychologists at the clinic to assess the client’s symptomatology, level of functioning, background history, social network, and more. While the clinical interview incorporates assessment of elements consistent with the diagnostic criteria for Prolonged Grief Disorder (PGD) and Persistent Complex Bereavement Disorder (PCBD; (Lenferink et al., 2019), it also addresses known risk- and protective factors related to complicated grief (Burke & Neimeyer, 2013), attachment patterns, and developmental maturity level. It is not a requirement that the young adult meet criteria for PGD or PCBD. Rather, it is sufficient that, based on the clinical evaluation, there is evidence that the client experience grief complications, ranging from mild to severe. Eligible clients are subsequently divided in to two groups: those with mild to moderate grief complications, and those with severe grief complications. See description of the two groups in Table 1.
Eligibility Criteria.
Clients with mild to moderate grief complications are enrolled in a time-limited group therapy program; those with severe grief complications are offered an open-ended group therapy program (see next section of the paper). Typically, the clients start therapy within a few months of the clinical interview, with a maximum wait time of six months. Once clients have started therapy, the dropout rate is low.
Some young adults are found ineligible for the group therapy programs, as they meet predetermined ineligibility criteria. These are listed below (see Table 2.)
Ineligibility Criteria.

Clients deemed not eligible because of the deceased parents’ problems with alcohol and substance abuse, are eligible for another of the center’s treatment programs, specifically developed for that population (Bache & Guldberg, 2012). Young adults, who are assessed not to be experiencing grief complications, are referred to the center’s peer support group. Finally, young adults with difficulties that may prevent them from benefitting from the program, such as young adults with server psychopathology, are referred to appropriate community resources.
The Structure of the Treatment Program
In this section we describe two treatment programs: 1) a time-limited, 18-session group for young adults with mild to moderate grief complications, and 2) an open-ended group for young adults who experience severe grief complications. Both groups consist of 8 clients, are led by one or two psychologists, and meet once a week for 2½ hours. Each session includes 2 hours of therapy, followed by 30 minutes of unstructured conversation, without the psychologists present. The unstructured time at the end of the session serves to help the participants transition from therapy to their everyday life outside of group, thereby facilitating the movement between loss-oriented and restoration-oriented processes in accordance with the dual process model of coping with bereavement (Stroebe & Schut, 1999).
The therapeutic approach in both the time-limited and open-ended group is the same, that is, it is grief-specific and developed specifically for parentally bereaved young adults. The approach is sensitive to the developmental challenges facing this age group, i.e., challenges such as seeking to develop an independent existence while transitioning from childhood to adulthood, and to how the loss of a parent can further complicate this life phase. The dual process model for coping with bereavement (Stroebe & Schut, 1999) and psychodynamic therapy (e.g., Rubin, 1999) provide the core underlying theoretical foundation. However, a range of therapeutic techniques are employed, e.g., narrative, existential, and cognitive behavioral approaches, and psychoeducation, allowing for a targeted approach to each client’s individual needs.
Individual Therapy in a Group Setting
The therapy modality can be described as individual therapy in a group setting. The group setting helps provide an atmosphere of support, understanding, and witnessing (Brok et al., 2014; Lin, 2001). As a result of the bereavement, young adults can feel alienated from their non-bereaved peers (Nielsen & Winther-Lundqvist, 2019), and many may therefore be motivated to participate in group therapy, which offers the opportunity to meet peers in similar situations. This can reduce feelings of loneliness and of being different, while facilitating a sense of recognition, belonging and normalcy. At the same time, our group approach provides an unavoidable confrontation with (or exposure to) the reality of loss and grief. Each individual must not only share and relate to his or her own personal loss history, but is also confronted with the narratives and challenges of the others in the group. To be able to share complex problems and acknowledge and share difficult feelings, while in the presence of others, becomes a strong and necessary answer to the otherwise difficult problem of struggling with the painful and difficult feelings associated with grief in isolation. In our opinion, the group setting is an effective tool in addressing common problems associated with grief complications, that is, avoidance of the reality of the loss and the painful feelings associated with grief, and the feeling of being alone with one’s grief (Boelen & Eisma, 2015; Shear, 2015).
Within in each session, clients work one-on-one with one of the psychologists for approximately 15 minutes. When one client is working, the other clients listen and silently reflect on what is discussed, and on how it might, or might not, be relevant to their own experience and grief. The individual therapy component of the therapy allows for individualized, focused interventions targeted to each client’s needs. It is possible to pay special attention to topics of particular importance to the individual. It also serves to strengthen the therapeutic alliance and develop a sense of safety. At times, topics are discussed more broadly among all the group members, and there is an opportunity to share experiences and offer support and understanding.
This structure of providing individual therapy in a group setting is designed to offer the best of both worlds, that is, a targeted, individual approach to address each client’s unique situation, but doing so in the context of supporting peers, with whom they can easily relate and feel less alone in their grief.
Time-Limited vs. Open-Ended Group
The group for the young adults experiencing mild to moderate grief complications consists of 18 sessions. It follows a manualized protocol and has a theme-based structure. The themes are: 1. Establishing the group, 2. Setting goals for treatment, 3. The deceased parent, 4. Timeline of the parent’s illness, 5. The death, 6. Current social network and family relationships, 7. Continuing bonds, and 8. Saying goodbye to the group. The number of sessions used per theme varies from group to group, depending on what themes seem most relevant for the particular group.
The treatment program for bereaved young adults with severe grief complications is continuous and open-ended. Each client remains in the group for as long as deemed necessary by the client and the psychologist. There is a rolling enrollment, where a new client joins the group, once a current client has completed his or her treatment. This group does not follow a theme-based structure, but the themes of therapy mirror those of the time-limited group, and the treatment approach is essentially the same. The main differences between the two treatment groups thus have to do with the pace and dose of treatment, and the fact that the participants in the open-ended group typically do not work on the same theme at the same time. At this time, a protocol has not yet been developed for the open-ended group.
The Goals of Therapy
The main goals of therapy are typically, through increased insight and awareness and via strengthened coping skills and resources, to help the clients: accept, adjust to and integrate the death in the client's life narrative learn to acknowledge, accept and manage the difficult feelings of grief develop adaptive coping skills that can help promote well-being and healthy adjustment develop a flexible oscillation between the loss- and restorative processes of grief explore, understand and come to terms with the past relationship with the deceased develop a continuing bond to the deceased promote positive personal development encourage healthy social relationships find meaning, purpose in life and hope for the future
Thus, we strive to facilitate that parentally bereaved young adults are able to adjust to, cope with and integrate their loss into their lives in ways that enables continued development, effective functioning, and having a meaningful life.
The Theoretical Foundation
The Dual Process Model: Grief as a Dynamic and Complex Process
The grief specific theoretical foundation for the treatment rests on the dual process model (Stroebe & Schut, 1999, 2010). In accordance with this model, the psychologists embrace the notion that grief, at its core, is a dynamic and complex process. The grieving person needs to address both loss-oriented and restoration processes to be able to adjust to and integrate the loss into his or her life. That is, the bereaved person needs to, on the one hand, confront and experience the difficult painful feelings associated with the loss; learn to accept that the deceased is in fact dead; and establish a new and different kind of continued bond to the deceased – the loss-oriented work (Stroebe & Schut, 1999). At the same time, the bereaved person must find a way to embrace and adjust to the everyday life changes associated with the loss. That includes, among other things, learning new things; finding solutions to practical challenges; establish new roles, identity and relationships independent of the deceased; and continuing their personal development – the restoration work (Stroebe & Schut, 1999). The dual process model proposes that, ideally, the bereaved person oscillates between the two processes. It provides a dosing mechanism that facilitates confronting the various processes and challenges in manageable portions, so that the overall adjustment can take place little by little. In the course of our therapy, this process of adaptive adjusting to loss is explicitly explained to the clients through psychoeducation. In our experience, this tends to increase the clients’ understanding of their own experiences, as well as point out where they may have gotten stuck in the grieving process. It also seems helpful when our clients learn that grief has no expiration date, but that their grief will become more manageable over time.
The fact that grieving takes place in a cultural context with norms and expectations for how one grieves, and that this impacts the bereaved persons’ experience, is also explicitly addressed in the course of our treatment. Obviously, the client’s personal context, the bereaved young adult’s personality, attachment pattern, coping strategies, defense mechanisms, as well as familial and social circumstances also influence their work with both loss and restoration processes (Guldin, 2019).
Within this understanding of the grief process, psychologists work flexibly with the clients, using therapy techniques from various therapeutic approaches (see details in a later section) in order to, among other things, encourage acceptance of the death, promote effective regulation of emotions, facilitate the creating of a continued bond with the deceased while also helping the client find his or her identity separate from the deceased, and, finally, help the client be able to function better in life and establish relationship with supportive others.
Psychodynamic Therapy: Grief as a Relational Issue
A cornerstone of psychodynamic grief therapy has to do with increasing the client’s awareness of experiences, feelings, emotions and thoughts, that previously were outside of the client’s awareness, which, in turn, is thought to promote healing (Rubin, 1999). When someone loses a significant other, coping with the loss means having to adjust to the separation from an important person, and finding a way to manage past, sometimes unconscious, and unresolved conflicts and feelings associated with the deceased. In psychodynamic grief therapy, the psychologist becomes an object for transference of the client’s experiences and feelings (Chessick, 1983; Rubin, 1999). That is, the transference is in part based on the client’s experiences with the psychologist, and in part based in past experiences with the, now lost, significant other. In our experience, when the dominating person in the bereaved young person’s life is the deceased, transference observations and interpretations about the relationship between the client and the deceased offer great meaning and potential for the client’s therapeutic process and progress. This line of inquiry also becomes important when focusing on the role the deceased will continue to play in the bereaved person’s life going forward, i.e., the continued bond. In our program, the psychologist’s job therefore becomes to help the client investigate the reactions and feelings associated with deceased person, rather than in relation to the psychologist.
In addition to working with transference and countertransference, psychodynamic grief therapy also works with resistance, in part by focusing on addressing defense mechanisms and underlying conflicts (Worden, 2018). In our experience, this is relevant in relation to the deceased, the remaining parent, and difficult episodes during the parent’s illness, but also the client’s own past feelings and actions. Frequently, this work is centered around the feelings of shame and anger. For example, a young person can develop strong feelings of shame associated with having felt unable to handle frightening and emotionally overwhelming situations with a seriously ill or dying parent appropriately. In response, the young person may defensively dissociate from these experiences, subsequently storing these in the unconscious. As such, they are difficult to access and hence integrate in the narrative of the young person’s life. Anger is another feeling that can signal a defensive stance. Misplaced anger can defend against feelings of powerlessness, which the young person may have experienced in the context of living with a dying parent or following the death. In those cases, the sense of powerlessness can be expressed by directing the anger at other people, situations or perhaps the self, and can lead to overreactions to small infractions or other difficulties in the young person’s life. In our experience, by assessing and investigating these feelings and the associated reactions, it can be possible to uncover unconscious elements and conflicts – some that have to so with the deceased, some with other people, and some self-directed. By making the unconscious conscious, our clients experience a greater sense of awareness and insight, which can facilitate the grieving process.
Within our groups, the work of an individual client can arouse reactions and associations in the other group members. Accordingly, topics of relevance for other group members are discussed and further investigated in the group, allowing for sharing of feelings and for normalizing the client’s experience. In this context, some of our clients are able to let go of conflicts and the associated disruptive feelings all together, seemingly because of having expressed, externalized, and shared those with the supportive group members.
Existential Focus: Revisiting Narratives and Identity
The death of a loved one can for some result in an existential crisis, which is overwhelming and seemingly impossible to overcome (R. Neimeyer, 2005). The loss can activate strong feelings of meaninglessness, unfairness and powerlessness, which makes it hard to see a meaningful and safe way forward in life (Yalom, 1980). Some feel a sense of betrayal, perhaps even violation, and abandonment (Burke and Neimeyer, 2012). Also, in our experience, the death of a loved one can heighten the bereaved person’s own fear dying or fear that other important people in their lives might die. In this existential chaos, it is difficult finding a way to manage and recreate a happy and meaningful life (R. Neimeyer, 2005). To achieve this, it can be helpful to encourage the client to tell, create, or re-create meaningful narratives or life stories, incorporating the death of the parent (Neimeyer, 2000; Neimeyer & Lyddon, 1999; White & Epston, 1990). According to Neimeyer (2000), focusing on narratives and life stories can help facilitate meaning making. This in turn can help facilitate acceptance of and adjustment to the death. It allows for the necessary work to learn to reflect on the past and on the relationship to the deceased. Further, it can become possible to embrace the emotional pain of grief, while also focusing on the present life and maintaining a positive and hopeful outlook for the future, in spite of the loss. It is also possible to work on future narratives, e.g. hope and dreams for the future, and explore how the deceased can continue to play a role, also referred to as continuing bonds (Klass et al., 1996).
Our young adult clients often report that they felt like they lost a part of their own identity when their parent died. In addition, they experience feeling knocked down by life, which created a sense of insecurity, vulnerability, and lack of competence, further undermining their identity. Issues around identity can meaningfully be addressed through working with the client’s narratives of the loss and integrating these in the life story (Neimeyer, 2000; Neimeyer & Lyddon, 1999; White & Epston, 1990). In revisiting and reworking the narratives, it becomes possible for the client to reshape or re-conceptualize his or her identity, perhaps into one that is more preferred and functional. Some of this work involves revising traumatic and unpleasant experiences, learning to face and contain difficult feelings and experiences, and to integrate them in to the greater narrative. Likewise, exploring the relationship to the deceased, potential role reversals, expectations the client had of both the parent and him- or herself can be relevant. Finally, being able to consider the whole parent, both the good and the bad, results in a more nuanced and coherent narrative of the parent and, by extension, the parent-child relationship. This can help reshape the client’s narrative and influence his or her self-perceived identity.
Therapeutic Tools Used
In this section, we discuss a selection of the specific therapeutic techniques used in the groups. These techniques are, among other things, used to facilitate discussion, bring attention and awareness to important experiences and feelings, decrease avoidance, and increase meaning making.
Goal Setting
At the beginning of treatment, each client works with one of the psychologists to establish realistic treatment goals, in the context of the group. It involves paying attention to the client’s current difficulties and talking about how the client would like to feel and function differently, when therapy ends. Descriptions of current problems and specific desirable goals are explicitly formulated and written down, using the client’s own words. The goals are revisited throughout the treatment to guide the process and ensure that therapy stays on track. The psychologist may ask” What is difficult for you right now, in connection with having lost your parent?”, “By the end of therapy, how would you like things to have changed?” or “When you finish therapy, how would you like to feel differently?” to help facilitate the clients’ goal setting. While clients have individual goals, they often overlap thematically with those of others in the group. Common themes have to do with wanting to feel less sad, overwhelmed, and alone; being able to accept the death; being able talk about the deceased more easily; being able to recall positive memories; and being better able to deal with feelings such as anger, regret and self-blame.
Timeline
Clients are asked to create a timeline of their experience with their parent’s illness and death, highlighting times the clients found particularly difficult. Revisiting the course of illness, and/or the experience of the death, and documenting it as well as possible can help create a coherent narrative (Neimeyer, 2000). When reviewing the timeline in the process of therapy, it provides an opportunity to verbalize, consider and re-consider experiences, feelings, and actions. It can reveal connections and explanations, which were not previously apparent. In other words, it can help the client gain insight and develop alternative interpretations of his or her experience. Within the safety of the therapeutic environment, it may bridge gaps in the narrative, as the client gets an opportunity to explore previously avoided situations and feelings. It is not uncommon for our clients to be able to recall details and memories previously repressed, and while perhaps difficult in the moment, it is often followed by relief and appreciation because this helps the client integrate a more complete representation of what happened. Considering what the client went through and dealt with and documenting the course of illness on a timeline, we have noticed, can also foster a sense of agency, self-compassion and feeling proud of oneself. It is important, we believe, to maintain the focus on what the client rather than the ill parent went through, because diverting attention from the bereaved to the deceased can be avoidance in the service of defending against unwanted feelings.
Working With Letters
Letter-writing, inspired by Davidsen-Nielsen and Leick (2009), Pennebaker (1997) and; Pennebaker and Chung (2011), is the central technique used to facilitate the therapeutic process. The use of letters provides structure both to the general therapeutic process and to each client’s individual therapy. Letters are typically addressed to the deceased parents, but can also be addressed to important other people. They are written down in a journal or book, and serve both as the catalyst for the individual work and as a record of the therapy process and progress. Most weeks, each client receives an assignment to write a letter, covering a certain topic derived from that week’s session. The letters can help the client deconstruct the otherwise complex loss experience and their grief reactions. They also provide an opportunity to reflect upon, clarify, and reinterpret important experiences, feelings, and actions, and thereby potentially construct new, more helpful narratives where needed. Typically, letters will focus on issues that contribute to or maintain grief complications, for example, failure to accept the loss, traumatic memories, feelings of guilt, etc. The letters are read aloud and discussed in the following session. The act of reading the letters aloud is seen as a way to share, externalize and bring to light, what the client is experiencing and struggling with. While it may require a few sessions for some clients to get comfortable writing and sharing their letters, as it is unfamiliar in the beginning, they typically end up finding both the writing and the reading aloud worthwhile and helpful.
Periodically and especially towards the end of therapy, the clients are asked to go back through and review their letters. This highlights the progression of therapy and the grief experience. Their book of letters also become a repository of stories and memories, and can come to symbolize a connection to the deceased.
Photos of the Deceased
In addition to letter-writing, our treatment program involves working with photos. Clients introduce their deceased parent to the group in part by sharing and passing around a photo of their parent. Moreover, they are instructed to look at a photo of the deceased parent before writing their letters at home, as well as prior to reading their letters aloud in the group setting. In our experience, this often helps the client feel more connected to the parent. In addition, we find that working with photos can help stimulate feelings, thoughts, and memories that can be important for the therapeutic work. For some of our clients, it becomes a so far avoided confrontation with the parent’s death and the difficult feelings associated with grief. However, those of our clients, who are afraid to look at pictures of their deceased parent, typically find themselves quickly desensitized to looking at the pictures, and, in time, rather than being a source of sadness and despair, looking at photos become a source of comfort and feeling connected. Furthermore, the act of sharing photos with others in the group personalizes the parent and facilitates conversation about the parent and the relationship.
Emotion Regulation
The clients in the group often experience high levels of emotional distress and difficulty regulating their feelings, as the autonomic nervous system as well as the endocrine systems can become dysregulated following bereavement (O’Connor, 2012). Some clients report that they cannot control their overwhelming feelings. Other talk about having experienced embarrassing “break downs” in front of others, causing a fear that it will happen again. Others think that if they were to allow themselves to “feel grief”, they would not be able to handle it, fearing that they would not be able to recover, or perhaps even go crazy. Consequently, some clients try to shut down their feelings all together, which leads to an emotional numbness that also includes shutting down even positive feelings. Others try to cope and manage their discomfort through drug and alcohol misuse, gambling, and through acting out behavior, as observed in Rostila and Saarela (2011). The emotional distress felt by the young adults with grief complications is often accompanied by poor sleep, trouble concentrating and decision-making, low energy, physical discomfort, and restlessness. Hence, it becomes a therapeutic goal to help the clients learn more helpful, adaptive ways to regulate their feelings, so they neither engage in complete avoidance nor feel completely overwhelmed by their emotions. Interventions can include psychoeducation about the connections between thoughts, feelings, and actions, and about the fleeting nature of feelings. We work with the clients to help them learn to accept and acknowledge feelings rather than to fight and try to avoid them, to monitor feelings, and develop a more nuanced feeling vocabulary. We also employ mindfulness exercises, and strategies such as breathing, relaxation, and grounding exercises for regulation of physical reactions and sensations.
Gaining Insight
Promoting greater insight, for example insight associated with experiences, feelings, relational patterns, and their impacts on the client, and thus coming to understand and break down defense mechanisms that previously obscured this insight, is an essential part of our therapeutic work. For example, a young woman preoccupied by how she felt that her boyfriend had let her down when her mother was dying, may in fact be defending against having to think about the very difficult and frightening manner in which the mother died. This insight may, within the content of the supportive therapeutic environment, make it possible for her to confront the difficult and overwhelming feelings and experiences associated with the death, and thus help her address important elements in her grief. Consequently, she can stop ruminating about the boyfriend’s actions and perceived lack of support.
Promoting greater insight can also involve helping the client recognize patterns of interactions with others, which may have a negative impact on the client’s coping. For example, it can be patterns of always prioritizing the needs of others rather than own needs, taking on the identity of a victim who is continuously wronged, or having a habit of rejecting the advice of others. It is our experience, that these types of unhelpful patterns can, once brought to the awareness of the client, be addressed, explored and often changed in the course of therapy for more adaptive and helpful patterns of interactions. Reaching a higher degree of insight creates greater understanding, clarity and meaning, and the client leans to embrace a more flexible and exploring cognitive approach. For example, our clients may be encouraged to think back on otherwise avoided experiences and try to remember and talk about both positive and negative memories involving the deceased. This, in turn, may potentially help gain a more complete, balanced and coherent narrative, which can help promote understanding, meaning, and integration. In our experience, cognitive work also plays an important role when working with feelings of guilt, shame and anger. By investigating the way, the client thinks about and interprets the experiences that have led to the current painful feelings of guilt, shame and anger, it is possible to explore other, perhaps more helpful and balanced ways to think about and interpret what happened, which will influence the client’s feelings about these past situations. In addition, it becomes possible to explore ways to accept and perhaps forgive actions and choices, that, left unexplored, likely would have continued to play a disruptive function in the young adult’s life.
The Good Enough Psychologist
While knowledge of theory and therapeutic techniques are important when conducting therapy with young adults experiencing grief complications, so are the qualities of the psychologist and the therapeutic alliance. Winnicott (1986) described the often cited concept of the “good enough parent.” Similarly, the “good enough psychologist” could be considered. Non-specific factors, such as the perceived personal warmth and empathy of the psychologist, the client’s expectations of and engagement in the therapy process, and the alignment of client’s and psychologist’s goals for therapy, contribute to the therapeutic alliance and the likelihood of successful treatment outcome (Hougaard, 2009). In the groups, we strive to provide a safe and transparent environment. The psychologists take responsibility for maintaining the therapeutic frame and process, with a predictable structure and rituals, contrary to the client's often chaotic and unpredictable everyday life. In some situations, transference come into play, with the psychologist representing the nurturing, educating, and structure-providing parent, allowing for mirroring as well as work on attachment patterns and strategies.
The good enough psychologist strives to provide a secure base in the group and within the therapeutic relationship (Bowlby, 1988; Holmes, 2001). From a safe haven position, the client can – accompanied by the psychologist and the group – explore difficult and painful experiences related to the parent’s terminal illness and death or associated with a sudden and traumatic death. This exploration in the presence of supportive others (psychologist and group) can be essential for the client’s progression in therapy.
The psychologists do not help the clients get rid of their grief, but rather attempt to help the young people connect to the grief and learn to live with it. They challenge and encourage the clients to confront the pain that previously had been repressed, and support their efforts to find ways to manage intensive and potentially disruptive feelings while maintaining a day-to-day life.
The good enough psychologist cannot and shall not attempt to replace the deceased parent. But the psychologist aims perhaps for a while, and in a limited way, to serve as a substitute in terms of providing aspects of an attachment relationship, which the young person is lacking, while attempting to rebuild his or her life, find an inner base, experimenting with how to share very difficult and painful experiences with others.
Challenges Associated With the Method
In this section, we highlight some of the challenges associated with our treatment method. First, time-management can be challenging for the psychologists leading the groups. Typically, each client brings a letter to each session, which they will read aloud and discuss with one of the psychologists. To keep the momentum and flow going in the session, and to make sure each client has sufficient time to work one-on-one with one of the psychologists, the psychologists must track the time spent with each client carefully. For the individual work to be meaningful, the psychologist must also relatively quickly determine the relevant topic on which to focus that particular session. This can prove challenging.
Another challenging aspect can be reaching a good balance between the individual work and therapeutically using the group as a whole. That is, deciding when to prioritize bringing a topic up for discussion in the group in order to, for example, normalize a client’s experience, solicit feedback from peers, or facilitate sharing of support. This, in turn, can help build group cohesion and trust. Thus, the psychologist is working to balance the needs of the individual with those of the group. As above, this can be trying, but the fact that there are two psychologists is particularly helpful here. While one is working individually with a client in the group, the other can have a broader focus and initiate a group discussion when deemed helpful.
A third type of challenge can occur in the time-limited group which follows a set order of themes. At times, a client may be experiencing a non-grief-related stressor, for example a difficult break-up or difficulties at work or at school. This can make it difficult for the client to engage in grief work. In the open-ended group this can be accommodated, but this is more difficult in the time-limited group, where therapy centers around a progression through relevant, ordered themes. In that situation, the psychologist must determine how best to help the client address the acute issues while keeping the grief work on track as much as possible. This requires flexibility, creativity and good clinical judgement on behalf of the psychologist.
A final example of a challenge has to do with the method itself. For some clients it emotionally very difficult to tolerate exposure to painful memories, thoughts, and feelings; but such exposure plays an important role in the therapy. Here the psychologist’s empathy, tolerance of emotions, timing and sense of “dosing” of the exposure are important. The fact that the exposure takes place in a group context may add to the client’s experienced vulnerability, and it may also impact the other group members. Consequently, the psychologist must find a way to work therapeutically with both the individual and the group.
Case Illustrations
We now present two cases to illustrate some of the elements discussed above. The cases have been anonymized.
Case Illustration: William
William was 21 years old when he was encouraged by a social worker to seek grief therapy. He had lost his father 1½ year ago, suddenly due to a heart attack. Since his father’s death, William had been very angry and explosive. He had had many conflicts with his mother, friends, and strangers. When he was out partying with friends, he drank too much, became provocative, and acted out. This often resulted in him ending up in fights. To his friends it seemed that he almost looked for an opportunity to fight and that he enjoyed hurting others and even getting hurt himself. William did not work or attend school. His nights and days were reversed. Typically, he slept during the day and stayed up all night playing videogames. When he was not with his friends, he played computer games or gambled on-line.
William attended the open-ended, time unlimited therapy group. The goal of therapy was to help William gain an understanding of this own reactions following the death of this father. The aim was also for him to understand and work through the meaning of having lost a father, with whom he had had an ambivalent relationship. Understanding the impact of the fact that the father died suddenly was also explored.
William was an only child. When William was a child, his father worked long hours and was often away from the family. When William was a young child, his father had been his hero. William did anything possible to get his father’s attention. During his teenage years, William’s relationship with his father became conflictual. William was angry with his father, in part because he realized that he had never really been there for him, and yet the father wanted to control him. William was also angry with his father for treating William’s mother poorly.
In therapy, William’s anger associated with his conflictual relationship with his father became a prominent focus. Within the secure therapeutic alliance between William and the psychologist, the psychologist became the object of transference. Potential contributing sources of the anger were explored and it became clear that much of it was rooted in the feeling that the father had been largely unavailable, and William actually doubted if his father had ever loved him. The therapy also explored the way William, through his self-destructive behavior after his father’s death, seemed to direct his anger at himself. The letter-writing assignments became a vehicle for William to address his father, to explore, observe, and consider the relationship he had had with his father, and the meaning of his death. He came to understanding that his anger masked feelings of guilt for having been so angry at his father that he wished the father would die; he also struggled with feelings of guilt for having distanced himself from his father for years.
For William, writing and working with the letters was about finding a way to integrate the more vital parts of his lived experience with his father and learn to understand his own ambivalence towards his father, whom he both loved and hated. He came to the realization that many feelings were wrapped up in his grief. For William it became important to work with the loss and to renegotiate his relationship with his father, who had let him down. With renegotiations and reinterpretations of the relationship it became possible for William to reconnect with his father. This made possible new narratives, where anger and guilt did not overshadow other feelings associated with his grief. It became possible for William to focus on aspects of his father and their relationship that were meaningful and important to him, and to carry those with him in his life going forward. The group served an important containing role in William’s therapy. It became a safe place for him, where his experience of loss slowly unfolded. Being listened to, understood and mirrored, meant that William became able to focus on his future with greater hope and enthusiasm.
Case Illustration: Lisa
Lisa was 24 years old, when she contacted the clinic about a year after her mother’s death. She was referred by a social worker. The mother died from cancer, following about 6 months of illness. Initially, Lisa presented with low mood and flat affect. Her nights and days were turned around. She was socially isolated, did not have the energy to look for a job, and had stopped doing things she used to enjoy doing. She was trying to avoid all thoughts and feelings related to her mother’s illness and death. Lisa’s grief response was intense, complicated, and marked by signs of depression. She was assigned to the open-ended, time unlimited group.
During the course of treatment, it became apparent that Lisa grew up in a dysfunctional family. Her parents had a conflictual relationship. Lisa was close with her mother, but had an insecure attachment to her father. Following the mother’s death, Lisa did not feel supported by other family members, and she withdrew from them.
In the group, Lisa initially had difficulty expressing her feelings and talking about her mother’s illness and death. For a long time, Lisa insisted that she did not remember anything from the time just before her mother died. When she tried to talk about it, she got anxious and felt that her thoughts just went “blank.” Instead, the group became a place where she listened to the others’ experiences and worked to increase her capacity to tolerate and contain the thoughts and feelings those arouse in her. She slowly gained the courage to talk about her own experienced associated with her mother’s illness and death, and it became possible for her to confront the experiences and reactions she had repressed since her mother’s death. It was especially experiences of watching her mother suffer and the physical deterioration of her body that had been too overwhelming and frightening to think and talk about.
As Lisa became able to open up more in therapy, it became apparent that Lisa’s own actions surrounding her mother’s death contributed a great deal to her grief complications. Shortly, before the mother died, Lisa left the hospital in a state of anxiety and despair. She jumped on a train to a neighboring city. While being on the train, she was contacted by the hospital and told that her mother was likely to die shortly, but she did not turn around. She experienced this as a panicky escape, and the beginning of a relentless drive to be constantly moving. Lisa spent the next days partying, drinking, and engaging in promiscuous behavior. Lisa did make it back for her mother’s funeral, but left for the next 6 months, traveling, moving from place to place, and from job to job. Once she returned home, she was unable to restart her life, and thus the referral for therapy.
As part of therapy, Lisa wrote letters to her mother where she became able to investigate and develop her narrative of her mother’s illness and death. This happened in measured portions in order not to be overwhelmed. Little by little, she confessed what had happened. She wrote about her intense feelings of shame and regret, and that she felt she let her mother down. She also described feeling as though she had been controlled by something, that had led her to behave in ways she considered completely unacceptable and shameful.
For the first time, she experienced that it was possible to talk about these perceived shameful acts. The group was able to contain what she was expressing, and, through feedback, help her see that her actions in part reflected the great love she had for her mother, but also the need to protect, or take care of, herself. After a while, Lisa was able to accept and experience her feelings, while also experiencing her grief. It became possible for her to acknowledge the tremendous loss she felt, but also to share positive memories – which she had not previously been able to.
The course of therapy for these two clients drew on many of the core elements discussed previously in this article. For example, they both benefited from the targeted individual work but also importantly from the supportive and containing role of the group; the psychodynamic understanding of how clients dissociated strong feelings (e.g. anger and shame) and relied on defense mechanisms that turn out not to be helpful in the long run; and finally the appreciation that in the face of the death of a significant person, a great number of feelings and reactions, sometimes contradictory ones, coexist and must be dealt with in the grief process. In William’s case he had to figure out how to grieve the loss of a father, with whom he had had an ambivalent relationship. In Lisa’s case, she had to come to understand that her reactions, which she perceived as unacceptable and selfish, in part reflected a great underlying love for her mother.
Conclusion
In this article, we have described a treatment approach to working with parentally bereaved young adults who have experienced complications in their grieving process. Young adulthood can be a challenging period in a person’s life, because it represents a transitional phase between childhood and adulthood, between dependency and independence. Young adults are often not quite settled in their adult lives. They do not yet feel completely confident in their abilities and path in life. They may have limited experience handling crises, and may not yet have established their own social support network separate from their family. Young persons, who, in addition to these typical developmental challenges, have to deal with a loss of a parent, are often significantly challenged in their coping with the loss. While the treatment described here is a treatment for grief complications, it is our experience that the benefit is broader. This is reflected in the following quote from a 21-year-old woman after finishing treatment. She noted: I have learned many different and important things from the group. If I have to pick one, it will be that I have changed how I think about myself. In the past, I have been very self-critical. In particular, as it relates to what I did when my mother was ill. Now, I am more tolerant, and I don’t see those actions as a sign that I am a bad person, but they have to do with the situation I was in, and what I had to deal with. And I understand that my actions were okay. That means, that I also accept and trust my own feelings more – I no longer worry about if they are “right” or “warranted.” Now I say that that is how I feel now, and that is okay.
Footnotes
Acknowledgements
We would like to thank and acknowledge our colleagues and fellow therapist within the Danish National Center for Grief for their review and comments on earlier drafts of the manuscripts.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The therapy program for bereaved young adults within the Danish National Center for Grief has been supported by the following: Velux Fonden, Helsefonden, The Danish Ministry for Children and Social Affairs, Ole Kirks Fond.