
Abstract
Residents who are terminally ill often experience transfers to the emergency department resulting in hospitalizations, which may be potentially avoidable with treatment in the nursing home. This qualitative study explored the perspectives of 15 residents, 10 family members, and 20 nursing home staff regarding end-of-life care and the circumstances prompting resident transfers. Data analysis of participant interviews conducted January to May 2019 in a South Florida nursing home identified four themes related to transfer to the hospital: time left to live, when aggressive treatments would be unavailing, not knowing what the nursing home can do, and transfer decisions are situation-dependent. Study findings underscore the importance of increasing resident and family awareness of treatments available in the nursing home and person-centered advance care planning discussions. Further research should explore the reasons for residents’ and family members’ choice of aggressive therapies and their goals for care at the end of life.
Keywords
Approximately 25% of Americans die in nursing homes (Xing et al., 2013), and 50% of Medicare beneficiaries reside in these facilities in their last six months of life (Aldridge & Bradley, 2017). As many as 38% of nursing home (NH) residents have a hospital stay in their last month of life (Zheng et al., 2015), and about 32% of NH residents die in US hospitals (Allers et al., 2019). NH residents often are transferred to the hospital when an acute change in their condition occurs (Dwyer et al., 2014), and approximately 50% of NH resident hospitalizations at the end of life (EOL) may be potentially avoidable (Xing et al., 2013). These burdensome and often potentially avoidable transfers and hospitalizations (Gozalo et al., 2011; Lemoyne et al., 2019; Xing et al., 2013) may be inappropriate for NH residents who are in their last few months of life (Allers et al., 2019) if there are ample resources to manage the resident’s acute change in condition or provide comfort care in the nursing home (Cardona-Morrell, Kim, et al., 2017; Pulst et al., 2019; Reyniers et al., 2014). Since these end-of-life transfers continue to occur (Lemoyne et al., 2019), a broader understanding of the reasons for these transfers from the perspectives of NH residents and families is critical to improving end-of-life care and reducing these burdensome transfers of NH residents at EOL.
Potentially avoidable transfers, especially for NH residents who are terminally ill, may result in unwanted hospitalizations, increase their distress and risk for hospital-acquired complications and adverse patient events, and exposure to non-beneficial, costly diagnostic testing and interventions (Aldridge & Bradley, 2017; Dwyer et al., 2014; Gozalo et al., 2011; Tanuseputro et al., 2019). Research indicates that up to 81% of residents transferred to emergency departments result in admissions (Dwyer et al., 2014). Circumstances initiating these transfers cited by researchers include a lack of experienced nursing staff (Fosse et al., 2014; Pulst et al., 2019; Wallace et al., 2018) or medical providers and treatment resources on-site (Fosse et al. 2014;.Laging et al., 2015; Reyniers et al., 2014; Wallace et al., 2018), family/resident insistence/preferences or their reluctance to engage in end-of-life discussions (Pulst et al., 2019; Reyniers et al., 2014; Stephens et al., 2015), nursing staff delays in assessing or reporting the resident’s changing health status (Fosse et al., 2014; Wallace et al., 2018), infrequent end-of-life care discussions among providers, residents, and families (Laging et al., 2015; Wallace et al., 2018) about the goals of care (Bern-Klug et al., 2019; Fosse et al., 2014; Nakashima et al., 2017), and absence of advance directives (Fosse et al., 2014) such as do not resuscitate (DNR) and do not hospitalize (DNH) orders (Tanuseputro et al., 2019). Although these recent studies include providers’ (Laging et al., 2015; Reyniers et al., 2014) and family members’ perspectives (Fosse et al., 2014; Pulst et al., 2019; Stephens et al., 2015), the views of NH residents on transfers to the hospital and at EOL are less represented (Lemoyne et al., 2019; Towsley & Hirschman, 2018; Wallace et al., 2018).
NH residents who are nearing the EOL may prefer to remain in the nursing home (Lemoyne et al., 2019) and be cared for by familiar staff who know them (Tappen, 2016; Wallace et al., 2018). They may be incapable of making their own decisions because of their declining health or altered cognition (Su et al., 2020) or prefer to delegate this role to family members or staff providers (Bollig et al., 2016). Family members often are burdened with making difficult end-of-life care decisions and may be unaware of the resident’s preferences (Bollig et al., 2016), or rely on staff for their guidance (Fosse et al., 2014; Pulst et al., 2019; Su et al., 2020). NH residents may also have different perspectives about end-of-life care and transfers to the hospital than their family members or staff providers. Studies that compare the views of
NH residents, family members, and staff are necessary but are still limited (Wallace et al., 2018).
This current study addresses national initiatives targeted at reducing potentially avoidable transfers and hospitalizations of residents (Centers for Medicare & Medicaid, 2019) and improving end-of-life care for the growing number of older adults who will die in nursing homes (Institute of Medicine [IOM], 2015; Xing et al., 2013). The aims of this study were to 1) describe the care resident, family, and nursing home staff prefer for residents approaching the end of their lives if a change in condition occurs, and 2) explore resident, family, and staff understanding of palliative and hospice care, and hospital-based acute care purposes and practices. The results of this study may also inform future research efforts to reduce avoidable hospitalizations at EOL, such as the development of an end-of-life decision guide for NH residents and families since these decision aids are limited (Cardona-Morrell, Benfatti-Olivato, et al., 2017; Xie et al., 2018). This article focuses on participants’ perspectives and preferences, whether the NH resident should remain in the nursing home with hospice care or transfer to the hospital for aggressive therapy.
Study Methodology
This study used a qualitative design with a structured interview guide, which provided a consistent framework and open-ended questions to encourage in-depth dialogue about end-of-life care decisions. Data analysis included data condensation, pattern coding, and thematic interpretation within and across the three participant groups (Miles et al., 2020). The study conducted in a 110 bed Southeast (SE) Florida Rehabilitation and Health Care Center (nursing home) provides skilled long-term (58 beds) and rehabilitative or short-term (52 beds) care. Resident admissions to the long-term care (LTC) unit are primarily transfers from the short-term care (STC) unit in this nursing home.
Ethical Considerations
Before conducting the study, the researchers (authors) received approval from the Institutional Review Board (IRB) at a university and a letter of cooperation from the facility’s administrator. At the time of the interview, participants signed the written consent forms and agreed to be audio-recorded. The researcher followed the informed consent process with each participant as delineated in the IRB protocol. The researchers have no employment, professional, nor business affiliations with the nursing home.
Sample/Participants
The principal investigator/researcher (first author) briefed the nursing home personnel about the study and provided them with a script to use when approaching potential participants to determine their interest in participating in the study. Those who agreed were contacted and screened by the researcher, resulting in an initial purposive sample of 67 participants, 31 NH residents, 13 family members, and 23 staff members. Screening of these potential participants occurred either in-person or by phone (12 family members) to determine their eligibility, interest, and explain the purpose, interview process, and other pertinent study details and set a date/time for the interview if the participant verbally consented. NH residents (aged ≥65 years) were eligible to participate if they were not cognitively impaired as determined by the Mini-Cog Test or Brief Interview for Mental Status [BIMS] (score of ≥13), and were physically and mentally able to engage in dialogue about end-of-life care. Family members (aged ≥18 years) were eligible if they were a relative, spouse, or close friend to a resident and able to engage in dialogue about their resident’s care at EOL. Staff (aged ≥18 years) had to be employed full-time or part-time or medical providers. Out of the 67 potential participants, 46 (16 residents, 10 family members, & 20 staff) met the inclusion criteria and agreed to participate in the study. Of the 16 residents, one was dropped from the study, after the interview, at the request of the family member.
Data Collection
The in-person audio-recorded interviews, conducted from January to May 2019, were structured by the interview guide with similar questions, modified for each participant group. This guide included hypothetical situations and open-ended questions consistent with the research aims. The questions focused on circumstances that may prompt resident transfers to the hospital and participants’ preference for hospital-based or nursing home care/treatment. For this study, EOL is the last few months of life. The questions in the interview guide for NH resident participants are in Table 1. The staff interview guide also includes questions about facility policies or guidelines regarding resident transfers to the hospital and interventions performed for residents who cardiac arrest with do not resuscitate orders (Table 2). The researcher asked additional open-ended questions to encourage further dialogue or clarify ambiguities in participants’ statements. The researchers (authors) decided that the principal investigator would conduct all of the interviews to maintain a consistent approach for data collection and staff collaboration. However, the researchers held regular debriefings to discuss preliminary findings and potential interpretations throughout the study.
Nursing Home Resident Interview Guide.
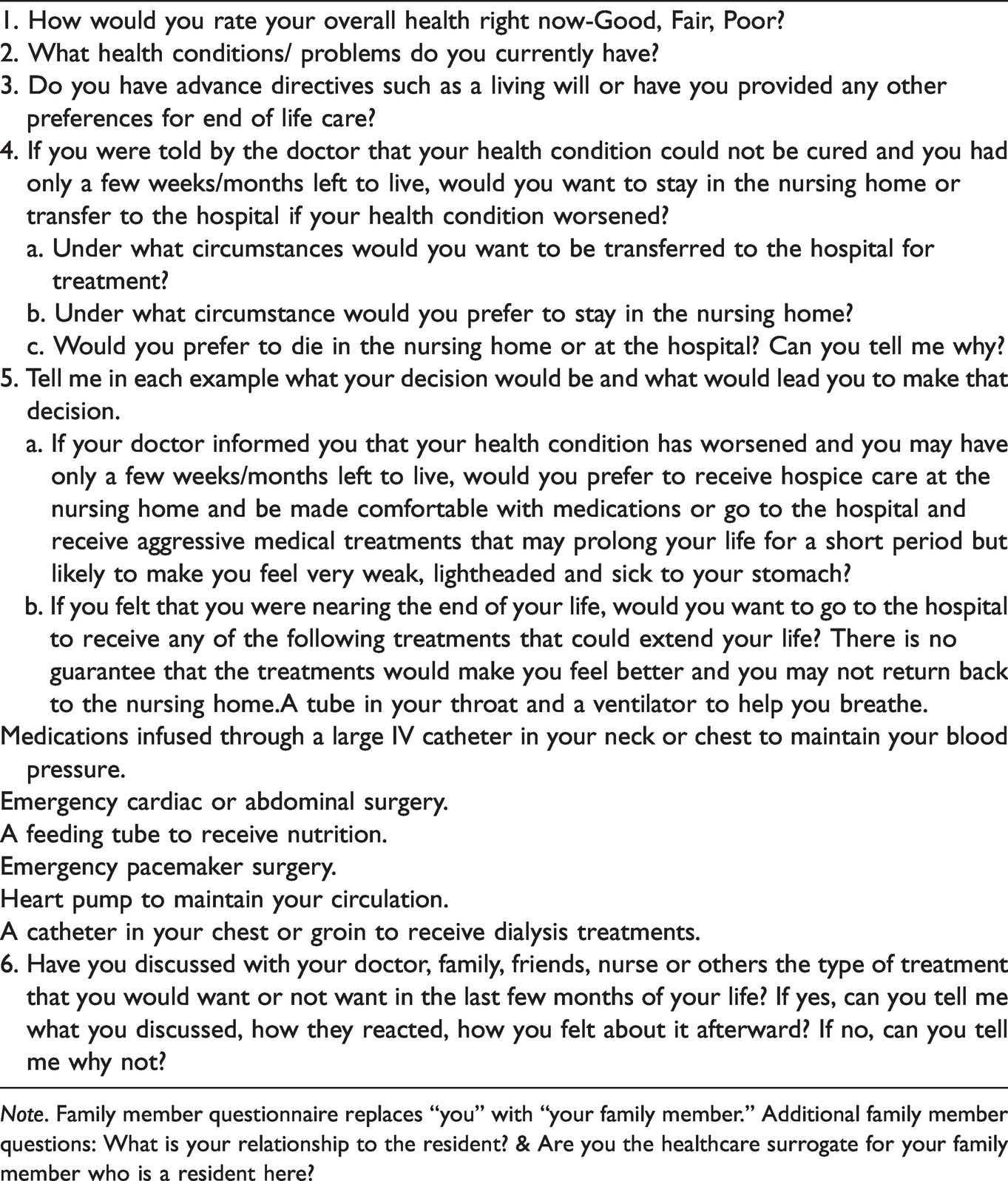
Note. Family member questionnaire replaces “you” with “your family member.” Additional family member questions: What is your relationship to the resident? & Are you the healthcare surrogate for your family member who is a resident here?
Nursing Home Staff Interview Guide.

Interviews for staff and family members took place in a private location in the nursing home, except for one family member who preferred to remain in the resident’s room. Residents were interviewed in their rooms because of immobility-related issues or their preference, except for one short-stay resident who was interviewed privately in the family lounge area. Interview times ranged from 10 to 40 minutes with a mean of 20.5 minutes for NH residents, 21.4 minutes for family members, and 17.4 minutes for staff members. Field notes were written after each interview to record the researcher’s observations. No further recruitment of participants was necessary because data saturation occurred within each of the participant groups, and no new data had emerged (Miles et al., 2020).
Data Analysis
The principal investigator transcribed all of the interviews and checked the transcripts line-by-line to ensure accuracy. Miles et al.’s (2020) method of first (descriptive) cycle and second cycle (pattern) coding guided data analysis. First, the authors read and re-read the transcripts and, using the questions from the interview guide, created matrices to facilitate data condensation and descriptive coding (labeling and categorizing) for each group. The authors initially coded the data independently and met weekly to interpret and condense these preliminary codes into categories, compare and contrast patterns within and across participant groups, seek underlying meanings, and conceptualize overarching themes. Researchers’ biases during coding and interpretations of data were discussed fully and resolved (Miles et al., 2020).
Study Results
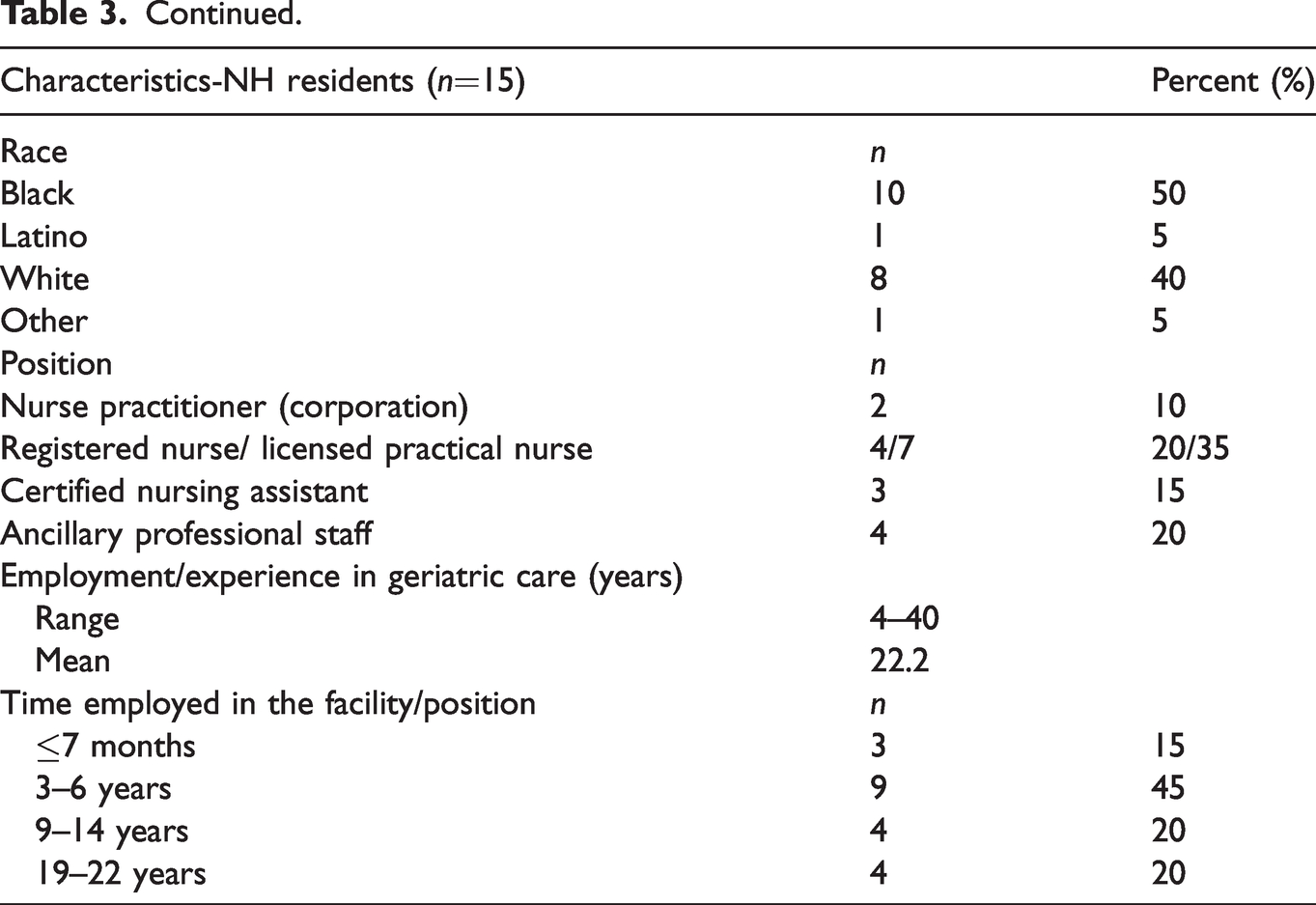
The mean age of residents (5 males; 10 females) was 85.7 years, family members (3 males; 7 females), 61.7 years, and staff members (20 females), 51.1 years (Table 3). Two of the15 residents were STC. Included in this mix were three resident-family dyads, interviewed separately. Residents self-assessed their overall health as good (n = 7), fair (n = 7), and poor (n = 1). Family members rated their relative’s health as good (n = 4) and fair (n = 6). None of the residents were approaching or at EOL as per the nursing staff, notwithstanding any acute catastrophic health event.
Demographics- NH Residents, Family Members, and Staff Members.
Four themes related to the care preferences and perspectives of residents, family members, and staff participants for NH residents nearing or at EOL emerged from their interviews. The themes are time left to live, when aggressive treatments would be unavailing, not knowing what the nursing home can do, and transfer decisions are situation-dependent.
Aggressive therapies, as defined in this study, are the hospital-based treatments listed in the interview guide (Table 1).
For some family members, the difference in time of a few weeks or a week to live compared to a few months changed their minds about transferring their relative to the hospital as this participant expressed, “If it’s something that she has a week to live, and she could be medicated and kept comfortable here…I don’t see a difference between a hospital and here if it’s that cut and dry.” Another family member stated,
If they told me that she only had a little time to live, it depends on what it would be.
Because I would not want her to suffer here in the nursing home if the hospital could make her comfortable. But if the nursing home can give her the same (care) as the hospital, then it’s okay for her to stay here.
However, a few family members expressed that they would still transfer their relative to the hospital because of uncertainties about their relative’s condition, prognosis, or chance of recovery with treatments, as this participant stated.
If she has developed some…bad infection that they cannot treat here, I don’t know if they do IV antibiotics here, then, that’s worth it. You know that’s not extraordinary…you don’t know that she only has a few weeks left to live. Cause if you…treat the symptoms properly, she may have more than a few weeks to live.
When residents were asked their preferences for care if they had only a few weeks to live, except for a few residents who would opt for a transfer to the hospital, their preference was to remain in the nursing home, as one resident related, “If I’ve been told that I only had a few weeks, sedate me as best they could, and I would try to live it out here.” Another resident offered, “I feel comfortable here. The people are nice. I was in the hospital, and I didn’t get that great a treatment in the hospital…if I know this is it, I’d rather be here.”
Staff members indicated that resident and family decisions to transfer to the hospital for aggressive or life-sustaining therapies, regardless of the resident’s remaining time to live or advanced age, depended on the resident and family member preferences for care and what they were comfortable with, and not staff-directed decisions. One staff member offered,
Just because they’re terminally ill, it does not mean that they cannot go to the hospital…it would be on a case by case basis. Some of our residents who are terminally ill may be on hospice, and they may not want any aggressive measures…But then there are some although, they’re terminally ill, they may still want to go and have something done. Especially if it meant it would relieve pain or improve whatever time they have left.
Overall, only a few participants responded yes for aggressive therapies (listed in Table 1) for residents at EOL, except for family members regarding tube feedings and blood pressure medications through a large intravenous (IV) catheter. Half of the family members would opt for a feeding tube for the resident at EOL compared to three residents or four staff who answered the question. Four residents replied yes to intubation and mechanical ventilation compared to only two family members and three staff who would consider this treatment option. However, 4 out of 14 residents and 4 out of 10 family members would want the IV blood pressure medications, while only 2 of 19 staff replied yes.
All family members indicated that they would prefer hospice care over aggressive treatments that might extend their relative’s life but not the quality of their life, although a few were unaware that hospice care was available in the nursing home. This could lead to unnecessary transfers of residents to the hospital as family members said, “It would probably be better for her to be in the hospital and then in the hospital, if it gets real bad, then they always ask to meet with you to send her to hospice,” and, “I wasn’t leaning towards the hospital because of any advanced or aggressive treatments … If the transferring of hospital was necessary, it would be for the more one on one care … that would make her comfortable.” Both family members were unaware of the availability of hospice care in this facility.
In contrast, only nine residents preferred hospice care in the nursing home. Many of the residents seemed familiar with the term hospice care, as this one stated, “They make you die easier as far as drugs and so on.” However, some seemed uncertain about the type and extent of care, and the length of time under hospice care, as this resident explained.
I would (want hospice) … they tell me the last few weeks … or two weeks or one month. But if they say months, it could be 16 months. I don’t think I want to be in hospice that long. No, to starve to death, no … I was told they hold the food back.
Three residents would still go to the hospital for care such as medications, not necessarily for aggressive therapies. One resident who replied no hospice shared his reason, “I had experience with hospice with my mother and father. And hospice, I didn’t like because they kept feeding my mother and father drugs. It just killed their pain, but they didn’t help them at all.” Two other residents were undecided.
Like the family members, most of the staff agreed that hospice care would facilitate comfort for residents at the EOL, but again, the decision would rest upon what the resident and family preferred or as this staff member offered, “If we don’t have any advance directives, unfortunately, we have no choice but to send them to the hospital.” Or another staff member explained, “As a nurse, you may feel that they should definitely be on hospice, but maybe the resident and family are not ready to say quit.”
I think I would rather go to the hospital because I think I’d get a little more care there than I do here in some situations. This place is great. They try their best, but one girl has like eight patients. And you don’t get that much care. You get it as much as they could do. In the hospital sometimes, it’s a little better …
Some residents believed that the hospital could offer more treatments in the last few weeks of life than the nursing home, as this participant expressed.
Well, if it meant I wasn’t gonna live very long here (nursing home), I would be better off in the hospital … they can treat you better in the hospital. They don’t have the provisions here. If I had to be on a bag that hangs up with the medicine. So they can’t do that here … I think it would be the best thing for me. Just to go into the hospital and be treated as it is to lay here and just die.
Some of the family members who would opt to transfer their relatives to the hospital had similar perceptions of hospital care offering, “I think I would trust the hospital a little bit more than … the nursing home … .sometimes it’s the lack of care in the nursing home,” and from another family member, “These people here (nursing home), manage people’s medical conditions on a day to day basis as well as their non-medical needs. At a hospital, all that focus is intensified. There’s more staff … ”
Residents and family members unaware of the nursing home’s capabilities to treat the resident may opt for a transfer to the hospital, as this staff nurse participant explained.
They (family) probably feel like in a nursing home, where we don’t have the technology that the hospital does to save lives, and that the resident has a higher chance of surviving in the hospital which is not true … So they believe that the hospital can save the resident … We can treat them here with about almost the same things … it’s like two standards of care, they don’t believe that nursing homes can provide the care hospitals provide.
Only two family members stated that they would not transfer their relatives to the hospital for care at EOL. Knowing what the nursing home can provide may discourage transfers as this participant expressed, “They have doctors on staff here. And they pretty much can do just about everything they do in a hospital … He likes it here, he’s comfortable, so I want him to be somewhere where he’s familiar with and comfortable with.”
Family member decisions would depend on their relative’s situation when a change in their condition occurred as this participant explained.
But it depends on what the condition is? If it’s heart disease or something like that, like a cardiac event, then I would want her to go to the hospital, but if she started deteriorating mentally and she couldn’t function at all anymore, then I would want her to go to the hospice.
Most, if not, all of the family members expressed that their priority for the resident's care was to promote comfort at EOL, wherever and whatever that involved. As this family member stated, “I wouldn’t want her to be in pain. So whatever that would entail of her not being in pain or suffering … Whether she’s here or at the hospital, I don’t want her suffering.” It was also apparent that family members would make their own decisions regarding their relative’s care except for one participant who would depend on the NH staff, “It depends … If she was unconscious, would you think the hospital is best? I’m sure they would tell me here (nursing home) what would be best for her. I only want what’s best for her. Not for me, but her care.”
Staff explained that acute transfers of residents to the hospital occurred when the resident/family requested transfer, ordered by the physician, the facility was unable to treat or meet the needs of the NH resident, or there was no DNR. Despite the presence of advance directives such as the DNR or living will and hospice care, staff stated that some family members and residents rescind the DNR and hospice choice and opt for transfer to the hospital, as this participant explained.
Ultimately, it is up to the family and what the patient has in his or her living will. If a patient has stated in the living will that under all circumstances they want aggressive treatments, then we will honor that … send them to get aggressive treatment.
Residents, family members, and staff were asked about the presence of advance directives, such as a DNR or living will. All of the family members reported that they are the healthcare surrogate for their NH relative, aware of their relative’s preferences, and 8 of 10 indicated that their relatives had DNR orders in place. Ten of the 15 residents self-reported that they had advance directives/DNR or their family member was aware of their preferences. Staff reports of the presence of advance directives/DNRs for residents varied. Twelve stated that the majority of the long-term residents have DNRs. Only two providers spoke of DNH orders and that transfers do occur even if the resident has a DNH order, as one explained, “Unfortunately, what I learned is that when you say do not hospitalize, they (nurses) still will send the patient out. And sometimes the families can rescind that order.”
Similar to family members, the nursing staff’s goal was to promote the resident’s comfort. Some nursing staff mentioned that transfers occurred in situations such as the resident’s failure to thrive, combativeness, and pain management, as one staff nurse described.
When they are not eating, and we cannot met their needs … sometimes they’re extremely combative, and we can’t handle them. They’re not safe so … we don’t want them to hurt themselves even though it’s the end of life. You still need to be able to help the patient, make him comfortable, and if we cannot meet their needs here, we have to find someplace else to meet them.
Finally, about half of the residents indicated their preference for end-of-life care was to remain in the facility but, they would consider transferring to the hospital if the nursing home “could not help me” or promote their comfort. As this resident related, “It depends if I need treatment or not. For the fact that I need treatment. And I’d have to be more comfortable if they could help me. It depends on what the situation is.” Two residents would not transfer to the hospital under any circumstances, as one remarked, “It’s more comfortable … I’m already here. I don’t have to travel to the hospital to die.”
Discussion
The results of this study indicate that decisions to transfer to the hospital or remain in the nursing home depended on the facility’s ability to treat the resident, resident/family members’ preferences for hospital care, and absence of advance directives, similar to the previously cited literature. This study, however, revealed that residents, like the staff, were more definitive than family members, regarding transfers and end-of-life care with the length of time that a resident has left to live, the resident’s situation, and advanced age (≥90 years) contributing to such decisions. This study also revealed that some resident transfers to the hospital at EOL would occur because of resident and family member’s lack of knowledge about the care that the nursing home could provide. Promoting comfort for the resident at EOL was a priority for all participants, regardless of whether the resident was in the hospital or nursing home, and decisions to transfer depend on the person’s preference and the situation.
Time Left to Live
For some family members and residents, the length of the resident’s remaining time of a few weeks compared to a few months or their advanced age would change their decisions about transfers to the hospital and aggressive therapies. This finding of a perceived shorter life expectancy implies that a family member’s understanding that their relative is dying shifts their priority to comfort, limiting the appropriateness of other hospital-based treatment options for health recovery and are life-sustaining. Bern-Klug et al. (2019) found that family members would prefer peaceful dying and death for their relatives rather than having them endure suffering and potential harm from therapies that would prolong their lives when they realized that their eventual recovery was unlikely. Studies also indicate that NH residents prefer not to be hospitalized at EOL (Lemoyne et al., 2019), which limits their treatment alternatives such as life-sustaining or aggressive therapies. Since research is limited, additional empirical studies should investigate whether the length of time to death expectancy or the NH resident’s age influence decisions regarding transfers to the hospital and the type and extent of care preferred at EOL.
Awareness of Nursing Home Capabilities
Residents’ and family members’ views of the hospital’s ability to provide better care than the nursing home and their lack of awareness of treatment options in the nursing home, including on-site hospice services, contributed to their decisions to transfer for hospital-based care at EOL. These findings support prior research results that end-of-life transfers of residents may be avoidable when advance care planning discussions have occurred and with frequent end-of-life conversations about the resident’s condition and treatment options to facilitate comfort (Bern-Klug et al., 2019; Lemoyne et al., 2019; Nakashima et al., 2017; Stephens et al., 2015). Ongoing provider conversations with NH residents and family members are essential to enable clarification of the nursing home’s ability to treat the resident, resident/family preferences, and goals of care, the resident’s anticipated illness trajectory, and for shared decision-making in the last few months (Cardona-Morrell, Benfatti-Olivato, et al., 2017; Fosse et al., 2014; Pulst et al., 2019; Su et al., 2020). These conversations can prepare family members for making difficult end-of-life decisions as their relative’s condition and cognition decline.
Despite staff and provider recommendations that the resident stays in the nursing home for care (Pulst et al., 2019), families may still insist on transferring when they still have doubts about the nursing home’s ability to care for their relative or implement comfort measures (Pulst et al., 2019; Reyniers et al., 2014; Stephens et al., 2015; Wallace et al., 2018), or their relative’s dismal prognosis (Pulst et al., 2019, Stephens et al., 2015). For some residents and their family members, transfers to the hospital at EOL could be a source of comfort, hope, or reassurance (Reyniers et al., 2014) or as a last attempt to do everything possible to resuscitate the dying resident (Laging et al., 2015; Reyniers et al., 2014; Stephens et al., 2015). Having a conversation with family members can enhance the provider’s understanding of why they are insisting on transferring their relatives to the hospital and appropriately address their concerns. Providers could ask questions such as, tell me the reason you want to transfer, and do you know what would be done differently at the hospital along with an evidence-based resident-family decision guide (Tappen et al., 2020) to clarify the family members’ perspectives.
A resident-family oriented decision aid may be a helpful educational resource to guide NH residents and family members in provider discussions about the resident’s illness trajectory, treatment options, and advance directives (Gonella et al., 2019; Heyland et al., 2015; Laging et al., 2015). It can also support families through the panic and crisis of making decisions about a resident’s end-of-life care (Cohen et al., 2017; Fosse et al., 2014; Pulst et al., 2019; Stephens et al., 2015) as well as serving as a conversation-starting tool for providers. Since family members often make end-of-life care decisions for their NH relative (Su et al., 2020), providers should discuss their understandings of the NH relative's expressed preferences for end-of-life care and hospitalization (Etkind et al., 2018; Pulst et al., 2019).
Transfer Decisions are Situation-dependent
This study’s finding that resident and family decisions regarding transfers at EOL are dependent on the situation suggests that any guidance or decision aid prepared for residents and their family members should cover treatment options that are available in the nursing home and hospital to manage the resident’s health condition at EOL, including comfort measures, palliative care, and hospice care. The information should also include the risks, disadvantages, and expected outcomes of hospital-based treatments and which of these treatments the resident can receive in the nursing home (Cardona-Morrell, Benfatti-Olivato, et al., 2017). Providers can use this information to explain interventions available to treat the resident’s presenting symptoms, consistent with the resident and family member’s goals for care at EOL (Cardona-Morrell, Benfatti-Olivato, et al., 2017; Howard et al., 2017), including expected outcomes of hospice care compared to aggressive treatments as the resident’s condition declines, which may increase residents’ enrollments in hospice care (Reinhardt, 2020).
Similar to prior research (Aeling & Vacha-Haase, 2017; Rodriquez & Boerner, 2019), study findings indicate that residents and family members may have misunderstandings about hospice availability and the care provided that promotes the resident’s physical and emotional comfort (IOM, 2015; Reinhardt, 2020) and the emotional support available to family members (Gonella et al., 2019; IOM, 2015). Although hospice care can reduce residents’ hospital admissions in the last 30 days of life, intensive care unit admissions, aggressive interventions, and in-hospital deaths (Kelley et al., 2013; Zheng et al., 2015), providers should stress that hospice can enhance the quality of the resident’s remaining life and may lengthen the resident’s time left to live (IOM, 2015). Providing reassurance to residents and their family members that hospice care would enhance, not substitute, the care that the resident routinely receives (Aeling & Vacha-Haase, 2017; Gage et al., 2016) may help to allay their concerns about the quality and intensity of nursing home care in meeting the resident’s end-of-life care needs, which study participants expressed. Additionally, providers should explain that under the Medicare Hospice Benefit, the resident can receive 24-hour continuous nursing care in the nursing home for pain and symptom management when acute exacerbations in the resident’s health (periods of crisis) occur (National Hospice and Palliative Care Organization, 2016).
Using an end-of-life decision aid in conversations may enhance the provider’s understanding of the resident’s and family member’s values and care preferences, what is most important at EOL (Gonella et al., 2019; Howard et al., 2017), and their interpretation of appropriate and inappropriate transfers and treatments as the resident’s situation changes in the last few months of life (Cardona-Morrell, Benfatti-Olivato, et al., 2017; Cardona-Morrell, Kim, et al., 2017; Heyland et al., 2015; Xie et al., 2018). These discussions would promote shared decision making and clarify misperceptions about hospital, nursing home, and palliative/hospice care, and the resident’s condition. Knowing the situation and that the same treatments or hospice care could be provided in the nursing home, as this study found, may dissuade some residents and family members from transferring to the hospital and prevent avoidable hospitalizations at EOL. However, further exploration with a larger and more diverse sample of NH residents and family members is necessary to understand more fully their views about hospital-based care and expected outcomes for NH residents at EOL (Reyniers et al., 2014), and the ability of the nursing staff in the nursing home to meet their needs. Additionally, the nursing staff’s perceptions of the inability to meet the resident’s needs, which results in a transfer, should be explored.
Implications for Practice
There are several implications for policy and practice changes to promote resident and family-centered care at EOL and cultivate a climate of trust in nursing home care. First, the nursing home should hold regularly scheduled educational sessions, including printed resources, for residents and family members about nursing home interventions to treat acute changes in the resident’s condition, advance directives, including DNR and DNH orders, and palliative and hospice services, presented by nursing home staff and community hospice partners. These sessions can occur during resident-family social gatherings or care planning meetings routinely offered in nursing homes where family participation is likely.
Second, nursing home providers should have end-of-life person-family- centered care discussions with residents and family members at least twice a year to discuss their care preferences and perspectives, values, and what would matter most at end-of-life. These discussions should be held frequently in the last six months of life as the resident’s condition declines, understanding that the resident or family member may have changed their care preferences depending on the resident’s expected length of remaining time or health situation. Providers can use an evidence-based decision guide to center conversations on the resident’s condition, predicted illness trajectory, and treatment availability and outcomes, as previously discussed. They could ask questions such as, “Which symptom is most concerning for you? and “What can the nursing home do to meet your needs and concerns?” to facilitate a person-centered, family-oriented (IOM, 2015) approach in end-of-life planning discussions. Third, an interprofessional team of nursing home personnel and community hospice partners should evaluate the effectiveness of the nursing home’s processes of end-of-life planning and care based on resident-family evaluations using their suggestions to improve end-of-life care in the nursing home for residents and their family members.
In summary, end-of-life decisions to transfer the resident to the hospital or remain in the nursing home are situation-dependent, challenging, and person-centered, as this study found, meaning providers should have frequent end-of-life discussions with residents and family members to clarify their preferences for care. These conversations are critical to reduce end-of-life transfers to the hospital and help them understand the treatments that the nursing home could provide to promote the resident’s comfort and peaceful dying in a familiar environment (Pulst et al., 2019), as the resident’s health condition declines. This study furthers an understanding of NH residents’ and family members’ perceptions of end-of-life care and their preferences and parallels national initiatives to improve end-of-life care (IOM, 2015) and reduce all-cause hospital readmissions in nursing homes (Qi et al., 2020), especially at the EOL.
Study Limitations
There are several limitations to this study. First, hypothetical situations cannot replace the emotional upheaval of family members when a relative is dying (Gonella et al., 2019; Stephens et al., 2015), and understandably, the prospective views of family members and residents may change when the resident is at EOL, which was apparent in this study and in clinical practice (Cohen et al., 2017; Reyniers et al., 2014; Stephens et al., 2015). However, based on this study’s aims, participants’ views of their preferences for care highlights implications for practice and policy changes such as routine family and resident care planning meetings to educate them about the capabilities of the nursing in meeting the needs of the resident at EOL, the value of advance directives, and to elicit their preferences for care, especially in the last month of life. This study also suggests that hypothetical situations may be a useful tool in provider and resident/family member conversations to explain the resident’s predicted disease trajectory (Dassel et al., 2018) and the treatment options available, and to understand the end-of-life preferences of family members and residents.
This research conducted in one nursing home in SE Florida limits the transferability of findings to other nursing homes. However, this study confirms other research findings that may apply to similar area nursing homes. Lastly, it would have been interesting to compare the circumstances of residents' previous transfers and hospitalizations to family and members' perspectives of these at EOL. Because of this study's aims and focus on EOL, the authors believed that this data was not relevant as it may not reflect participants' perspectives when a resident was in the last few weeks of life, and therefore, not included in data collection.
Conclusion
The results indicate that, although the participants shared the goal of promoting the resident’s comfort at EOL, their decision to remain the nursing home or transfer to the hospital for care depended, to a large extent, on the situation, personal preferences, and uncertainties about the nursing home’s ability to treat the resident and meet their needs, and in some cases, the resident’s age or expected time left to live. The results suggest that frequent provider conversations with residents and family members are necessary to understand their preferences, values, and goals for end-of-life care and prepare them for EOL. Educating residents and families about the treatment resources in the nursing home, including hospice services, may reduce potentially avoidable transfers. This study confirms the need for further research to develop comprehensive end-of-life decision aids for residents and family members to heighten their awareness of the capabilities of the nursing home to meet their goal of promoting comfort and peaceful deaths. Research Approved by Florida Atlantic University Institutional Review Board: November 16, 2018: [1330646-1] Nursing Home Residents, Families, and Staff Perspectives Regarding Care Preferences and Transfers to Acute Care Facilities at End of Life: A Pilot Study
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.