
Abstract
The aim of this study was to investigate the psychometric properties of the Persian version of the Inventory Complicated Grief (ICG) including reliability, validity and factorial structure. In this cross-sectional study, 332 women and men bereaved at least 6 months from the adult population of Iran. The results showed Cronbach’s alpha was found to be 0.94 for the scales overall score. Inventory Complicated Grief found a positive and significant correlation between the beck depression inventory (BDI) (r = .62, p < .001) and grief experience questionnaire (r = .74, p < .001). Still, he also found that there was a negative correlation between adult hope scale (r = −.44, p < .001). Furthermore, the results of the EFA result showed four factors on this scale. Overall, ICG showed good reliability and validity in Iranian population and it could be applied for assessing their Complicated Grief.
Introduction
The loss of a loved one is among life’s most challenging yet common stressors, resulting in the cascade of emotional, cognitive, and behavioral responses that define grief (Szuhany et al., 2021). Grief refers to the way we respond to bereavement, it can take many different forms, in some form or another, grief is inevitable (Gross, 2018). Grief may be strong or weak, brief or prolonged, immediate or delayed; particular aspects of it may be distorted and symptoms that usually cause little trouble may become major sources of distress (Parkes & Prigerson, 2010). The experience of grief is very personal and multidimensional and has pervasive effects on the bereaved person (S. Mehdipour et al., 2009). Although the meaning of grief is ambiguous in the relevant texts, the concept of grief usually refers to the multiplicity of complicated reactions that occur after the experience of separation and loss, and especially after the loss and death of a loved one. More precisely, grief is the mental feeling caused by the death of a loved one. In a more precise sense, grief refers to the process of dissolving mourning (S. Mehdipour et al., 2009; Sadock et al., 2015). Different types of grief are not mental disorders, and usually, 6 months after the disappearance, most of the symptoms go away. However, in about 10% of people, the symptoms become more severe and complicated over time. Researchers have referred to this condition under various headings such as pathological grief, Traumatic grief, unresolved grief, prolonged grief, and complicated grief (Boelen et al., 2003; Mousavi et al., 2016; H. G. Prigerson et al., 2009; Zisook et al., 1985). Complicated grief usually occurs when a person loses an important person in her/his life and usually suffers from these symptoms for more than 6 months: intense desire and preoccupation with the deceased; anger and bitterness about the death; shock and disbelief; estrangement from others; hallucinations of the deceased; behaviour change, including avoidance or proximity seeking behaviour, Defective daily functioning, difficulty in trusting others in various aspects (Han et al., 2016; Horowitz et al., 1997; H. G. Prigerson et al., 1995b; Shear et al., 2011, 2014). Although Professionals have suggested that these symptoms may indicate major depression disorder, post-traumatic stress disorder, or an anxiety disorder. Researchers have shown symptoms such as prolonged symptoms, having anger and aggression or intense desire for the deceased, having severely disturbing thoughts for a long time and difficulty accepting the reality that Manifested in disbeliefs and a defect in daily functioning and difficulty in trusting others. Consequences indicate that the disorder differs from other disorders (Cozza et al., 2016; Horowitz et al., 1997; Prigerson et al., 1995a, 1995b, 1996, 2000). On the other hand, the common treatments for these disorders have not optimal results in complicated grief (Reynolds III et al., 1999; K. Shear et al., 2005; M. K. Shear et al., 2001, 2014; Zisook et al., 2001). Complicated grief is a significant source of distress and dysfunction and is associated with a wide range of negative mental and physical health consequences (Ott, 2003; H. G. Prigerson et al., 1997). Since studies have shown complicated grief is different from major depression disorder, post-traumatic stress and anxiety disorders (Cozza et al., 2016; Horowitz et al., 1997; Prigerson et al., 1995a, 1995b, 1996, 2000) and effects on mental and physical health (Ott, 2003; H. G. Prigerson et al., 1997), the need for a tool High credibility and validity is essential to help diagnose the disorder. Studies have shown that a provision for a good and complete treatment is a correct diagnosis, one of which is the existence of scales that have optimal psychometric properties. So that the versatile complicated grief scale developed by H. G. Prigerson et al. (1995b) made it possible. Of course, there are various scales for assessing grief (Futterman et al., 2010; Jordan et al., 2005; Kiely et al., 2008; Marwit & Meuser, 2002; H. O. Prigerson & Jacobs, 2001; K. M. Shear et al., 2006). However, because of different reasons such as diagnostic accuracy, poor psychometric properties, the rate of use by therapists and researchers, and attention to dimensions measured by other scales, They are not comparable to the Prigerson Inventory of Complicated Grief, which has all these features (H. G. Prigerson et al., 1995b). Studies have also shown that the symptoms of Persistent Complex Bereavement Disorder (PCBD), introduced as a new disorder in the DSM-5, are consistent with the Prigerson Inventory of Complicated grief (American Psychiatric Associaion, 2013; Ludwikowska-Świeboda & Lachowska, 2019). It is necessary to have a scale that can differentiate between complicated grief and other conditions such as major depressive disorder, anxiety disorders, and post-traumatic stress disorder. H. G. Prigerson et al. (1995b) developed the Complicated Grief Scale to distinguish between normal and complicated grief. This scale has 19 questions that examine the symptoms of complicated grief. Numerous studies that have examined the psychometric properties of this scale in different cultures have shown that this scale has good and desirable psychometric properties (Carmassi et al., 2014; Han et al., 2016; Li & Prigerson, 2016; Lifshitz et al., 2022; Ludwikowska-Świeboda & Lachowska, 2019; Masferrer et al., 2017; Thimm et al., 2019; Tsutsui et al., 2014). According to the author’s knowledge, this scale has been used in two studies in Iran. Researchers have only studied its Cronbach’s alpha coefficient in their research and have not fully examined its validity, reliability, and factor analysis. However, the results show high internal consistency (Aslani et al., 2019; F. Mehdipour et al., 2020). In the main study of H. G. Prigerson et al. (1995b), Cronbach’s alpha was 0.94 and in concurrent validity High correlations with the Beck Depression Inventory (BDI) total score (r = 0.67, p < .001), the Texas Revised Inventory of Grief (TRIG) score (r = .87, p < .001), and the Grief Measurement Scale (GMS) score (r = 0.70, p < .001). According to what has been said so far and the lack of desirable psychometric properties scales based on the cultural and social conditions of the Iranian population in the field of complicated grief, the present study intends the psychometric properties of the Persian version of the complicated grief scale. In addition to providing a reliable scale to Iranian therapists and researchers with desirable psychometric properties, the results of this study also help to develop theoretical knowledge in the field of disorders related to grief. The question of the present study is whether the Persian version of the inventory of complicated grief has desirable psychometric properties?
Method
Participants and Procedure
In this psychometric study, the study population was bereaved adults Persian-speaking. The sample was selected using the convenience sampling method. Considering that Comrey and Lee (1992) suggested a sample size of 300 individuals to study Exploratory Factor Analysis (EFA) and taking into account Myers et al.’s (2011) suggestion of a sample size of 200 individuals for Confirmatory Factor Analysis (CFA), we selected a sample size of 400 bereaved adults. However, 332 individuals (127 male and 205 female) fully completed the scales. The 18-minute online survey, disseminated through social media (WhatsApp, Instagram) and websites, targeted bereaved adults Persian-speaking who had experienced the death of a significant other, either a relative or a close friend: In all participants, the loss had occurred at least 6 months before selected. We collected data between December 2021 and March 2022. Prior to translating the scale into Persian, the authors asked for permission from Dr Holly G. Prigerson. Initially, the questionnaire was translated by two English translators. The following stages were performed according to the intercultural adaptation of self-report measurements (Beaton et al., 2000). Afterward, two translations formed a team, and a single version was set up and translated into English by another translator. Then, the questionnaire was reviewed by experts (two clinical psychologists, two psychiatrists, one doctor in translation) and compared with the original text of the questionnaire. After agreeing (easily and without any problems) on the final English version and the Persian content of the questionnaire, the final Persian version of the questionnaire was prepared. Next, the final questionnaire was piloted on 30 Participants, through interviewing, to ensure its appropriateness for the Iranian culture. Finally, the final version was confirmed for psychometric evaluations. The inclusion criteria were: participants had to be over 18 years of age and have experience of a death of an important person (close family member, friend, other person indicated as important for the respondent) at least 6 months before the study. Exclusion criteria were: any physical condition that would limit the ability of them to take part in the study and incomplete and inconsistent responses to the Questionnaires. A written informed consent that described the objectives and procedures of the study was obtained from all participants and anonymity was assured. Participants were asked to fill out the battery of four self-report measures, Inventory Complicated Grief(ICG), Beck Depression Inventory(BDI), Grief Experience Questionnaire-34(GEQ-34), and Adult Hope Scale(AHS).
Measures
Inventory of Complicated Grief
The ICG is a self-report instrument that can be used to identify CG. The original version consists of 19 items and respondents rate the frequency with which they experience each item on a 5-point scale (0–4), ranging from “never” to “always” (0 = never; 1 = rarely; 2 = sometimes; 3 = often; 4 = always). The authors developed and tested this inventory with 97 elderly bereaved men and women. High correlations with the BDI total score (r = .67, p < .001), the TRIG score (r = .87, p < .001), and the GMS score (r = .70, p < .001), documented concurrent validity. Respondents with ICG scores greater than 25 were in the upper quartile of the sample and reported significantly more impairment in social, general, mental and physical health functioning and reported higher levels of bodily pain than those with ICG scores less than or equal to 25 (H. G. Prigerson et al., 1995b).
Beck Depression Inventory
Beck Depression Inventory, first introduced by Beck and colleagues in 1961, is a 21 items, self-rated inventory with each item rated with a set of four possible answer choices of increasing intensity. When the inventory is scored, a value of 0–three is assigned for each answer and then the total score is compared to a key to determine the depression’s severity (Beck et al., 1961). The reliability and validity of Persian version of BDI has been demonstrated in Iran (Dabson & Mohammadkhani, 2007). According to previous studies on reliability of BDI in Iran and to reduce the chance of a false positive result, we considered a score of 0–15 as normal, 16-30 as mild depression, 31-46 as moderate depression and 47-63 as severe depression (Kaviani et al., 2001)
Grief Experience Questionnaire
GEQ-34 was used to assess the intensity of the grief experience. GEQ was first presented by Bart and Scott and has been widely used for various forms of losses. The reliability rate for this questionnaire was confirmed in a study; its Cronbach’s Alpha was at .90. S. Mehdipour et al. (2009) translated GEQ into Persian and appraised its reliability and validity against GHQ-28 and SCL-25 in undergraduate college students (N = 348) with grief experience. As a result of their study, 34 questions and seven subscales were obtained; Alpha Chronbach for the whole questionnaire was achieved at 0.88. GEQ’ subscales include Rejection, Stigmatization, Search to Find Explanation, Guilt, Somatic Reaction, Personal Appraisal or other people’s judgment in relation to the reason of death, and Shame. In their appraisal of the convergent validity, Mehdipour and colleagues reported a significant positive correlation between GEQ and two subscales of Depression and Somatization of SCL-25 (p > .005) and GHQ-28 (p > .004). Responses are given on a five point Likert scale ranging from Never (1) to Always (2). Internal-consistency reliability was run on scores of this instrument. Results indicated that the standardized Cronbach’s Coefficient Alpha was 0.70.
Adult Hope Scale
The AHS by Snyder was applied to test hope among participants. The scale contains 12 statements – four items are related to agency subscale, four items to pathways subscale, and remaining four are the buffers. Respondents mark their answers on an 8-point scale, where one signifies a completely false statement, and eight describes a completely true statement. The higher the general result (results from two subscales), the greater the hope level. The AHS displays an acceptable internal consistency rate in the original (Cronbach’s α = .74–.84), as well as the Persian version (Cronbach’s α = .82), which is estimated based on research conducted among colleg. The original scale, display correlation with related constructs such as: basic hope, self- esteem, ability to cope with difficult situations, optimism (research among a group of the unemployed, Spearman’s rho = .39), self-efficacy (studies among high school students, Spearman’s rho = .36) (Kermani et al., 2011).
Data analysis
Data was collected using Google Forms. Data were analyzed using SPSS software V. 26 and Amos software V. 26. Descriptive statistics were used to analyze data, and Cronbach’s alpha and test-retest reliability (3-week interval) was used to examine reliability. The correlation between the ICG and the Grief experience questionnaire-34, BDI, and Adult hope scale were analyzed to determine validity. Confirmatory factor analysis was also used to determine to construct validity using Amos software V. 26.
Results
The sample included 332 subjects 205 (61.8%) female, and 127 (38.2) male, with a mean age of 34.62 ± 7.75 years. Also, 49.1% (163) of them were single, 42.5% (149) were married and 8.4% (28) were Divorced. In terms of education level, 74 (22.3%) had diploma, 152 (45.8%) had a bachelor’s degree and 106 (31.9%) had a master’s degree or higher. Average time period since the death of a close person was 16 ± 13.20 months (the time span of this period oscillated between 7 months and 4 years). The bereaved person was the spouse in 29% of cases, a parent in 24%, a child (son/daughter) in 18%, a sibling in 16%, a friend/significant other in 7%, a grandparent in 6% of cases.
Reliability
To assess the reliability of this scale, the reliability of test-retest and internal consistency of questions was used. The results showed that internal consistency by Cronbach’s alpha method for the whole scale was .94 and for the factors of estrangement from others and preoccupation with the deceased, shock and disbelief, yearning and hallucination about the deceased was .93, .86, .85 and 0.81, respectively. The test-retest reliability for the total scale was .81 after a 3-weeks interval (p < .001), and it was .89, .88, .85 and .88 for the Estrangement from others and preoccupation with the deceased, shock and disbelief, Yearning and Hallucinations of the deceased factords, respectively.
Convergent and Divergent Validity
Inventory of complicated grief found a positive and significant correlation between the BDI (r = .62, p < .001) and grief experience questionnaire (r = .74, p < .001). and It was found to indicate convergent validity appropriate for this scale. Also, the inventory of complicated grief had a negative and significant correlation (r = −.44) with the adult hope scale, which indicates the favorable divergent validity of the inventory of complicated grief.
Factorial Structure
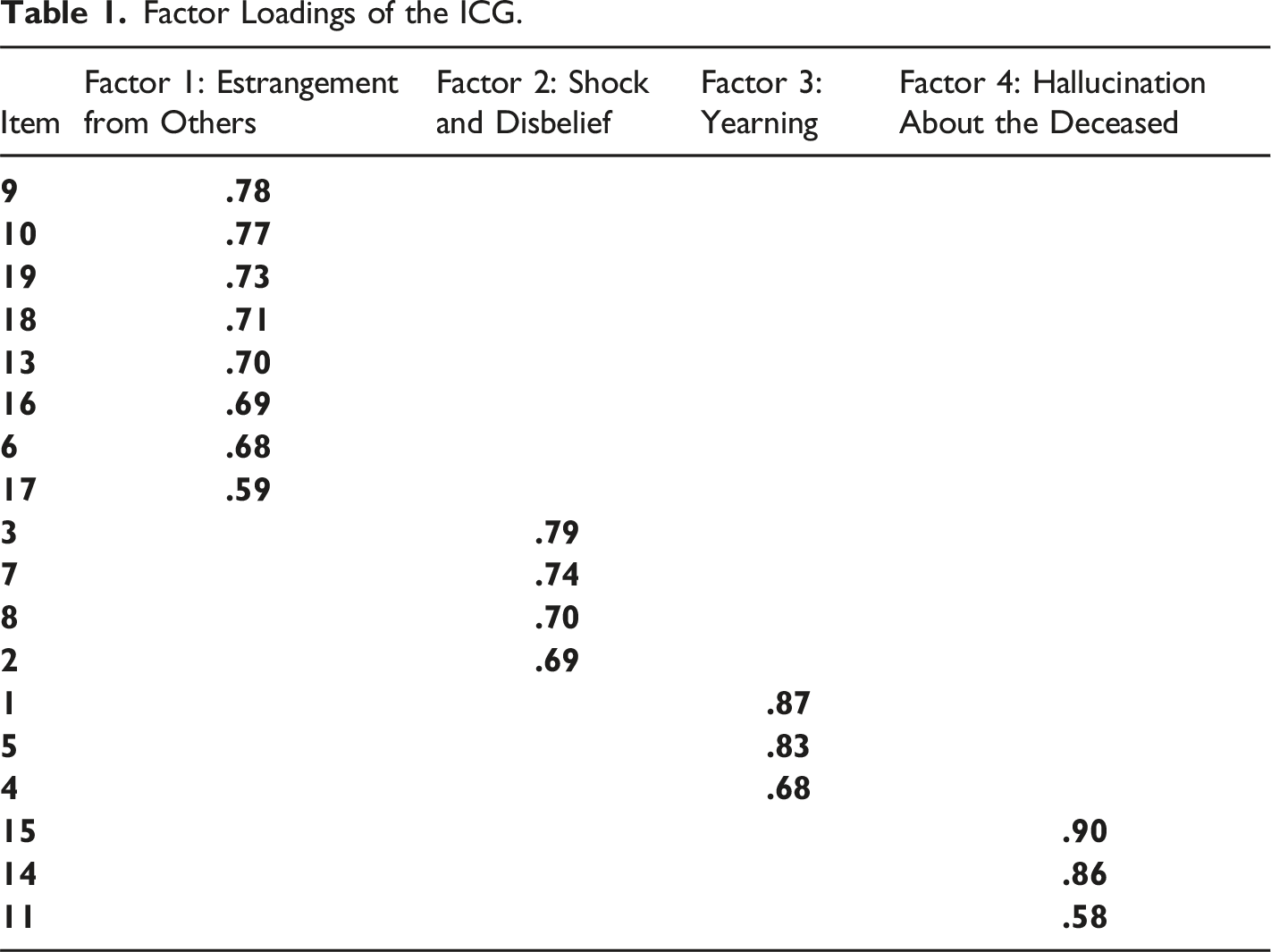
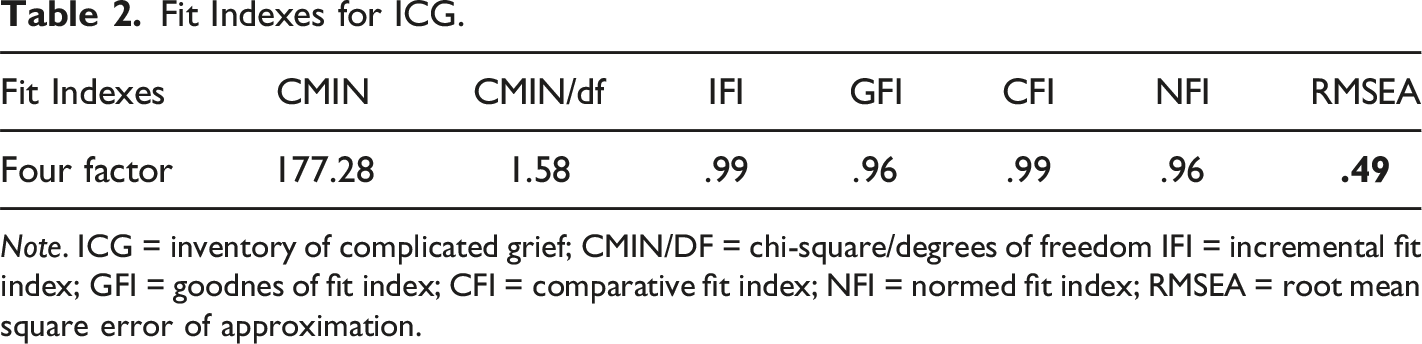
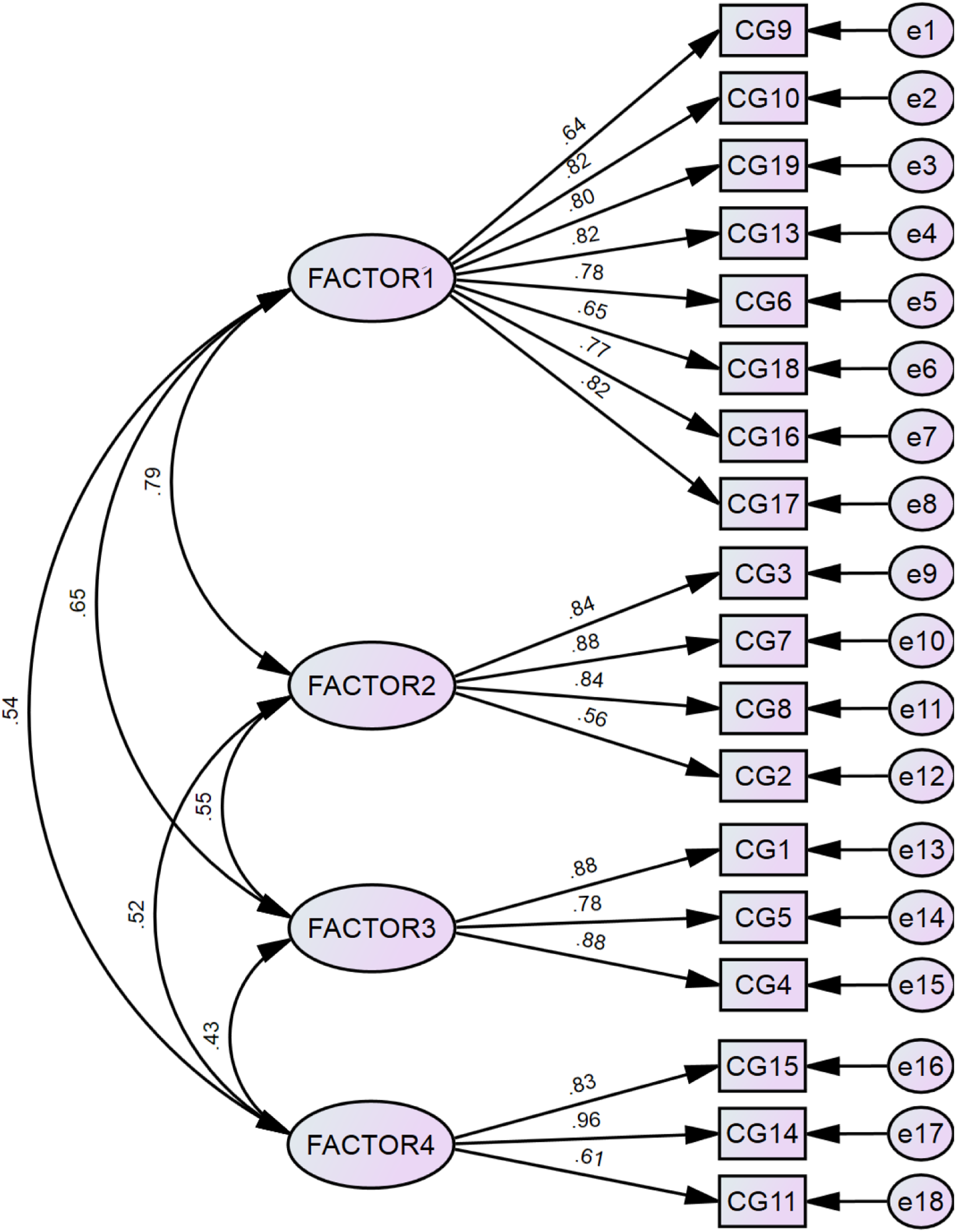
Exploratory and confirmatory factor analysis was used to evaluate the construct validity and factor structure of the inventory of complicated grief. For this purpose, first the adequacy of the sample volume was evaluated by Meyer Alkin’s Kaiser index, which showed the adequacy of the sample volume (KMO = .907). Bartlett’s sphericity test showed that the assumption of zero correlation between the rejected questions and the conditions for performing factor analysis (p <0.0001), df = 171 and Bartlett’s 21.321/3166). Exploratory factor analysis was performed by principal component analysis (PCA) method and varimax rotation, taking into account the specific value of one and the factor load of 0.3. The scree plot showed four factors with eigenvalues greater than 1.0. (Figure 1). In this study, four factors were extracted that explained 71.73% of the variance. Factor 1, labeled the “estrangement from others and preoccupation with the deceased”, had eight terms and had an eigenvalue of 9.012, accounting for 27.285% of the variance. Factor 2 was labeled the “shock and disbelief”, had four terms and had an eigenvalue of 1.508, accounting for 17.268% of the variance. Factor 3, labeled the “yearning”, had three terms and had an eigenvalue of 1.321, accounting for 13.764% of the variance. Factor 4, labeled the “hallucination about the deceased” had three terms and had an eigenvalue of 1.073, accounting for 13.422% of the variance. Table 1 presents the factor loading of inventory of complicated grief items in the present study. The factor load of the 12th item did not reach the standard value of .3 in any of the factors, so the 12th item was removed from the scale. Following the exploratory factor analysis, the inventory of complicated grief also underwent maximum likelihood confirmatory factor. In this study, NFI, CFI, GFI, IFI, CMIN/df, CMIN, RMSEA indices have been used to assess the model fit (Table 2). According to the obtained results and the amount of GFI, IFI, CFI indices which show more than 0.95 and also RMSEA which is less than 0.08 and CMIN/df which is less than three all indicate the appropriate have a model (Figure 2). Scree plot of eigenvalues according to the number of factors. Factor Loadings of the ICG. Fit Indexes for ICG. Note. ICG = inventory of complicated grief; CMIN/DF = chi-square/degrees of freedom IFI = incremental fit index; GFI = goodnes of fit index; CFI = comparative fit index; NFI = normed fit index; RMSEA = root mean square error of approximation. Confirmatory Factor analysis ICG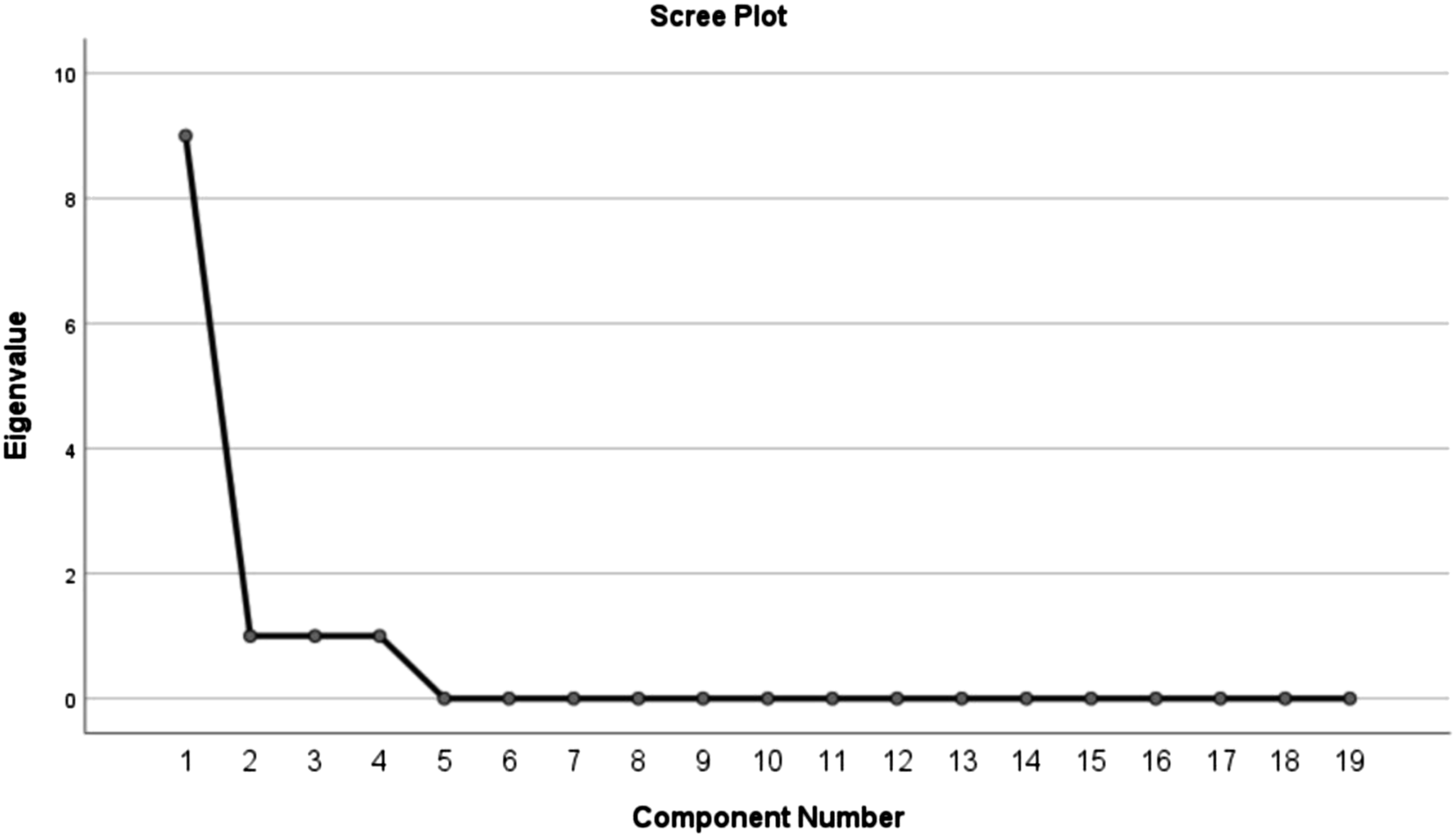
Discussion
The purpose of this study was to investigate the psychometric properties of the Persian version of the Inventory of Complicated Grief so that researchers have access to a valid scale for examining complicated grief in the Iranian population. For this purpose, this scale examined factor structure, convergent and divergent validity, internal consistency, and test-retest reliability. The findings showed high internal consistency between the scale and the subscales, so Cronbach’s alpha coefficient for the 18-item scale was .94. For the subscales of Estrangement from others and preoccupation with the deceased, shock and disbelief, Yearning and Hallucinations of the deceased were .93, .86, .85, .81, respectively. The Cronbach’s alpha coefficient for the whole scale equals the original version .94 (H. G. Prigerson et al., 1995b) and the Italian version .94 (Ludwikowska-Świeboda & Lachowska, 2019). As can be seen, the obtained Cronbach’s alpha is similar to the other versions (Ludwikowska-Świeboda & Lachowska, 2019; H. G. Prigerson et al., 1995b). The test-retest reliability method was used to obtain the stability of the scores over time. The results showed that the correlation coefficient between the two performances over a 3-week interval was .81, which was significant (p < .01). As a result, the Persian version of the Inventory of Complicated grief has good test-retest reliability; this result is slightly higher than the original version, equal to .80 (H. G. Prigerson et al., 1995b). The results of factor analysis showed that the data follow the four-factor model, which contradicts the results of the original Italian and South Korean versions of this scale, which indicates that this scale is one-factor (Han et al., 2016; Lifshitz et al., 2022; H. G. Prigerson et al., 1995b). On the other hand, the results align with the Spanish, Norwegian, Hebrew versions and the study of Simon et al. The results showed that the scale was multifactorial (Lifshitz et al., 2022; Masferrer et al., 2017; Simon et al., 2011; Thimm et al., 2019). Generally, the results showed that the 18-item Persian version of the inventory of complicated grief includes four factors: Estrangement from others and preoccupation with the deceased, shock and disbelief, Yearning and Hallucinations of the deceased. The Grief Experience Questionnaire and BDI were used to evaluate the convergent validity in this study. The results showed that the inventory of complicated grief had a positive and significant correlation with the experience of grief and the BDI. This moderate to the high correlation of the total score of the inventory of complicated grief with the symptoms of grief and depression is consistent with previous findings (Ludwikowska-Świeboda & Lachowska, 2019). Also indicates that complicated grief overlaps with depression but is distinct from the disorder; this finding is consistent with other studies (Spuij et al., 2012; Thimm et al., 2019). The examination of the inventory of complicated grief factors showed that detachment is associated with symptoms of depression and anxiety. This finding follows research showing that loneliness is an important link between bereavement and depression. This finding is consistent with research showing that loneliness is an important link between grief and depression (Fried et al., 2015; Thimm et al., 2019). In general, the symptoms that distinguish complicated grief from a major depressive disorder and post-traumatic stress disorder are difficulties accepting death, intense longing for the deceased, being angry and angry about the death of an important person, and feeling meaningless in life without the deceased (Salloum et al., 2017; Spuij et al., 2012). Adult hope scale was used to assess divergent validity. According to the results, hope was negatively correlated with complicated grief, indicating that people with lower hope experience more severe symptoms of complicated grief. Studies have shown that the higher a person’s level of optimism, hope, and belief in self-efficacy, the milder the symptoms of complicated grief. Therefore, having positive beliefs about the future can help adjust to absence. Feeling efficient in the face of daily challenges without a deceased and having a positive outlook on the future makes it possible to discover new goals in life and hope. Commitment to their realization can help the bereaved person to focus less on a lasting loss (Ludwikowska-Świeboda & Lachowska, 2019). High levels of hope in young people are better associated with mental health (Salloum et al., 2017). The study results by Vale et al. Showed that high levels of hope might act as a psychological power and protect inappropriate internalized behaviours in youth and life dissatisfaction from stressful events (Valle et al., 2006). Several studies have supported the protective role of hope (Salloum et al., 2017). In another study, the results showed that low levels of hope were associated with higher levels of psychological distress or poor social and emotional functioning in a sample of non-clinical youth (Gilman et al., 2006; Salloum et al., 2017). Finally, as with other studies, this study has its limitations. First, the sampling was done in an accessible manner, which weakens the generalizability of the findings. Second, the study was conducted using self-report questionnaires and online (WhatsApp, Instagram), which may have led to a bias of respondents. Third, only self-report scales were used to measure convergent validity so that the results may be affected by the effect of the method. Since this study was performed on the general population, it is suggested that clinical samples be used to achieve the cut-off points of this scale in the Iranian population in future studies.
Conclusion
Despite the widespread use of the complicated grief scale in clinical and research settings in other countries and the lack of studies related to the validation of this scale in Iran (to the best of our knowledge), the present study was undertaken. In conclusion, the findings of this study showed that the Persian version of the Inventory of Complicated Grief has good reliability and validity and can be used for studies evaluating complicated grief in the Iranian population.
Footnotes
Acknowledgments
The authors appreciate all the people who helped us with the planning of the study and the data collection and the men and women who voluntarily participated in this study.
Ethical Considerations
The Proposal of the study was approved by the Student Research Committee, Iran University Of Medical Sciences. Also the Research Ethics Committee of the IUMS (IR.IUMS.REC.1400.782) was approved the study. The authors also obtained the informed consent of participants to take part in this study before filling out demographic information. All participants were told that participation is voluntary. In addition, all participants were ensured about the confidentiality of their information.
Availability of Data and Materials
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study benefited from the support of the Student Research Committee of the Iran University of Medical Sciences by grant No 0-1-15-20739.