
Abstract
This study aimed to determine the needs of end-of-life cancer patients’ and their nurses’ perspectives and experiences regarding end of life period. A qualitative descriptive phenomenological study design was adopted comprising face-to-face, semi-structured interviews with patients and their nurses. Content analysis was conducted using the ‘Induction’ approach. 15 patients and 15 nurses participated in study. This study emerged three categories, nine themes for patients, and seven themes for nurses. Categories were determined according to the Donabedian model. The interviews revealed that although the nurses wanted to provide the necessary care, they could not accomplish it because of excessive workload, inadequately informed patients, and less than desired knowledge and education levels of the nurses and healthcare team. Improved care coordination and partnership working are essential for supporting both patient and their nurses at the end of life.
Cancer is a leading cause of death worldwide by the uncontrolled proliferation of cells. The incidence of cancer worldwide is 19.3 million, of which 10 million have died from cancer (GLOBACAN, 2018). Also, there will be about 27.5 million new cases of cancer by 2040, and 16.3 million adults and elderly individuals will die of cancer (American Cancer Society, 2019). In our country, 20% of deaths are caused by cancer. Furthermore, according to 2008 data, this rate is estimated to reach 37% with approximately 22 million new cancer cases occurring annually by 2030 (Turkey Cancer Statistical, 2019). This condition increases the cancer patients’ need for palliative care and end-of-life care, a subunit of palliative care.
The World Health Organization (WHO, 2018) defined palliative care as “an approach that improves the quality-of-life of patients and their relatives facing problems associated with life-threatening illness, through the prevention and relief of suffering by means of early and effective identification, assessments, and treatment of pain and other problems, physical, psychosocial, and spiritual”.
Internationally, nurses constitute the largest group of healthcare providers. Nurses spend more time with patients and their families than other healthcare professionals because they face serious illnesses. Because of expert nursing care, it reduces the distress and burden of patients and their families facing death, as well as the need for support for their unique physical, social, psychological, and spiritual needs (Wu et al., 2016). The palliative care nurse basically aims to improve the quality of life of the patient and his family who are in the process of illness and death, and the family who is left behind in the grieving process after death. For this, the nurse has important roles such as education, treatment, coordination, care and counseling. In fulfilling these roles, the nurse should meet the needs of the patient and their family and respect their privacy (Hagan et al., 2018). Besides, nurses’ values, attitudes, beliefs, educations and opinions affect the decisions and behaviors towards care given to the patients. The patients’ opinions and satisfaction regarding their received care are among the indicators of the quality-of-care provided. The patients’ views regarding nursing care quality are also an important component in improving hospital services, and can change patient compliance and treatment outcomes (Chan et al., 2016). Therefore, it is important to know the opinions of nurses and patients about care. It is thought that nurses with positive opinions will accurately determine the care needs of end-of-life patients, and care priorities will match the patient’s (Lu et al., 2014). In a study investigating patients’ appropriate and inappropriate care needs, patients indicated that their care needs werenot fully met because inappropriate care needs were prioritized (Bolt et al., 2016). In related studies, it was found that the wounds and odors in the mouth adversely affect the patient’s nutrition, since oral care is not given adequate priority. It was also found that symptom management was facilitated with the detection of early-stage oral morbidity, and the quality-of-life was also increased (Kvalheim et al., 2016). Other studies found that due to the lack of communication and information, psychosocial and emotional care needs of the patients were not prioritized, and physical symptom management did not satisfy the patients (Nedjat-Haiem et al., 2017). After the literature review, this study was planned because of the paucity of studies on the overlap from perspectives of patients and nurses on end-of-life cancer care.
Purpose and Theorical Framework
The aim of this study is to determine the needs of end-of-life cancer patients’ and their nurses’ perspectives and experiences regarding the end-of-life period.
The Donabedian Model constitutes the theoretical framework of the research. This model, developed by Avedis Donabedian in the 1960s, is generally used in defining the quality of care by determining the current needs in health. According to Donabedian, quality care can be almost anything anyone wants it to be (Donabedian, 1988, 2002). A Donabedian model assumes the existence of three essential factors in assessing quality – structure, process and outcome – and possibly a causal relationship between them (Figure 1). For Donabedian, structure is defined as the places where medical care takes place and the instrumentalities of each product and may include the features of the system, the service provider or the patient. Process refers to the set of activities that take place, on the one hand, between professionals and, on the other, between professionals and patients. It includes technical and interpersonal aspects. Outcomes are the consequences for the health and well-being of individuals and society and include clinical outcomes, quality of life and satisfaction with the care provided (Donabedian, 2002). Donabedian Model components and their relationship.
In literature such as retrospective studies, experimental studies and quasi-experimental studies are used in the collection and evaluation of data by Donabedian model. In the results of the studies conducted with these methods, it is stated that the opinions of the patients, their relatives and health personnel should be taken (Kamal et al., 2014; Nakazawa et al., 2016; Voyce et al., 2015). The Donabedian model was used as the theoretical framework of the research, as it renders the sub-dimensions, outputs and interrelationships of the needs that determine the quality of end-of-life care for the patient and the nurse.
Method
Design
Based on the descriptive phenomenological approach, a qualitative research design, this research was conducted using a semi-structured interview guide (Merriam, 2015). This method was developed by Husserl. Husserl thought that the studies should reflect a phenomenon or experience on daily life. Because this method argues that it is the way a person experiences the life he lives and at the same time the reality he has lived. While defending this method, Husserl argues that thoughts should be in epoche and bracketing should be in order to be free from prejudices of people and to be transparent (Husserl, 2003, 2006). This method was chosen because it aims to reveal the “essence” or “basic structure” of any phenomenon under investigation. The Consolidated Criteria for Reporting Qualitative Research (COREQ) was used as the qualitative research guide (Tong et al., 2007).
Participants and Recruitment
The study population consisted of inpatients with cancer at the end-of-life and their nurses in an oncology hospital. The sample was selected by the typical sampling method, which is a purposeful sampling method used to collect qualitative data. This sampling method aims to have an idea and to reveal the experiences clearly by examining a phenomenon or event in depth (Gill, 2020). The sample size was based on data saturation indicated by the repetition of information (Merriam, 2015). The study comprised a total of 30 participants, including 15 patients whom met the inclusion criteria and 15 nurses who were primarily interested in these patients. The patients who were diagnosed with cancer, informed about diagnosis, 18 years and older, at the end-of-life, Karnofsky Performance Scale Score <50 (this scale was used to recruit patients at the end-of-life. Those with score ≤50 (Evans & McCarthy, 1985) were selected), no cognitive and psychiatric problems, Turkish speaker, voluntary and the nurses who were primary caregiver of participant patient, 18 years and older, voluntary were included in study. Our purpose in choosing these criteria is to accurately identify the end-of-life patient and to reach cancer patients in this group.
Afterward, doctors and nurses of patients were interviewed to ascertain the patients’ suitability for the interview. Written consent was obtained from patients and their nurses who met the inclusion criteria.
Data Collection
The patients and their nurses were interviewed face-to-face by KT as part of a Masters project. The researcher took a qualitative research course and a training in confronting death and communicating with a dying patient as part of the master’s course. In addition, the researcher worked as a nurse in the general internal medicine and oncology service for about 2 years. Necessary measures were taken to ensure that participants felt comfortable and were able to make eye contact with the researcher in the interview setting. Interviews with the patients were conducted in the patients’ rooms. One-on-one interviews with the nurses were conducted either in the nurse room or in a private storage room. The interviews were recorded on tape. Written and oral consent was obtained from participants before recording the interviews. Each interview lasted 20–40 min. The researcher conducted six pilot interviews (3 patients, three nurses) in September 2017 to assess her interviewing skills and to get used to recording. The pilot interviews were not included in the study. Data were collected between September 2017 and February 2018.
Descriptive form for the patient: Consisted of a total of
Descriptive form for the nurse: Consisted of a total of
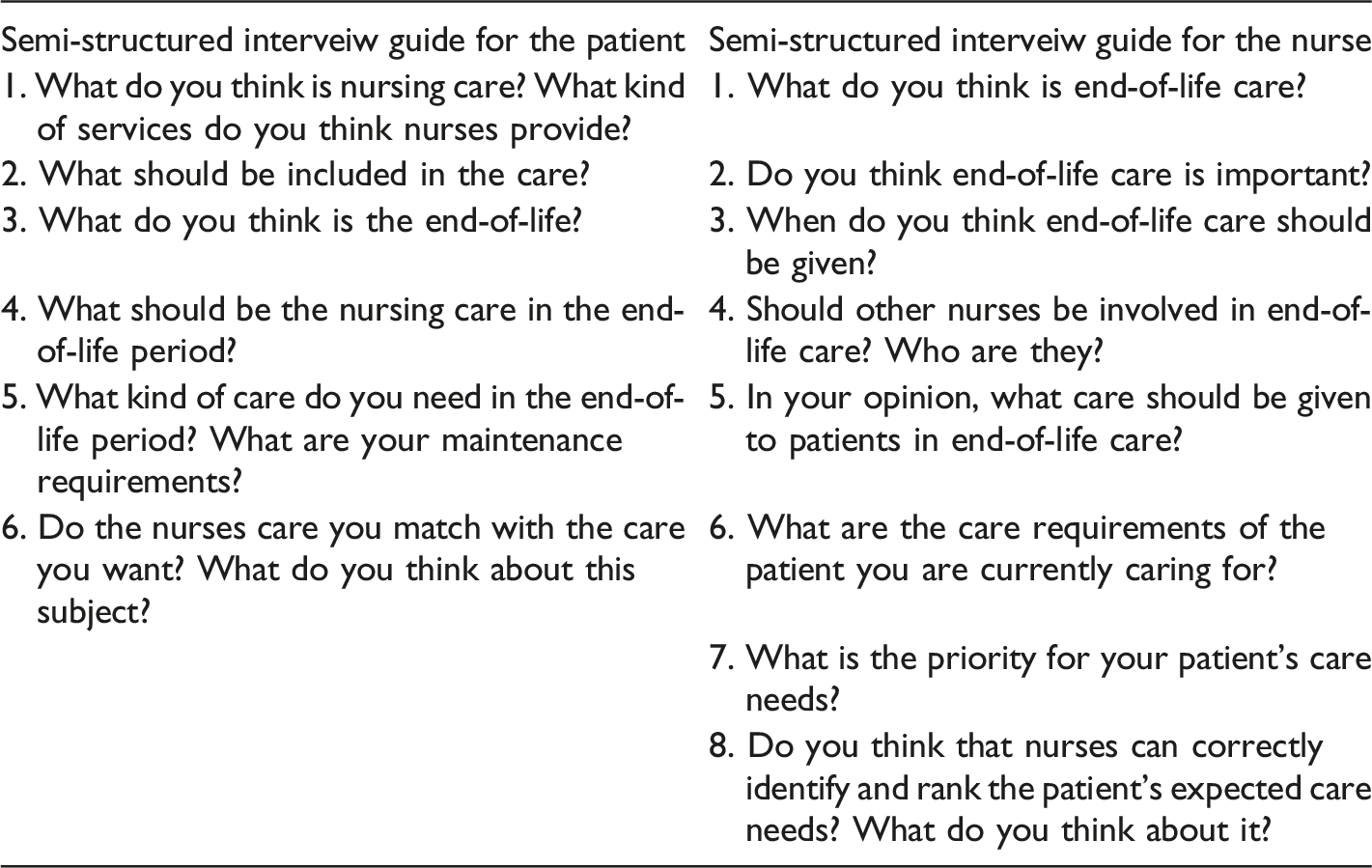
Semi-Structured Interview Guides
Ethical Approval
Ethical approval and written permission were obtained from the Non-Invasive Clinical Research Ethics Committee of University (16969557-1089, Decision No: GO 17/595-02, Date: 12.07.2017), medical directory and study participants. Written permission was obtained from the Hacettepe University Oncology Hospital to conduct the research. Additionally, oral and written consent was obtained from participants according to the guidelines presented in the Declaration of Helsinki.
Data Analysis
Research data were analyzed using content analysis with an inductive approach. In this analysis method, the collected data was first conceptualized, arranged logically according to the concepts obtained, and the themes explaining the data were determined (Merriam, 2015).
Steps of data analysis: 1. The tapes were transcribed and read carefully multiple times by both researchers. 2. The tapes were replayed to check the transcripts. 3. The content of the interview text was open coded (identification of statements with similar meanings), and the identified statements were coded by naming them. 4. The named codes were divided into themes and sub-themes in terms of their similarities and differences. 5. Three different specialists were consulted to verify data analysis and ensure the validity and reliability of the findings. Data were evaluated by experts from different departments to prevent professional blindness. 6. The steps of data analysis were re-examined by the researchers.
Trustworthiness
Regarding the credibility of the study, descriptive data, peer review, and external audits were used to achieve the purpose of the study. Peer interrogators in peer review questioned the researchers on research methods and analysis to ensure that the researchers remained honest and avoided bias. In the external audit review, the main and sub-themes extracted in the analysis were evaluated by three different experts. Themes were reorganized based on these experts’ opinions.
Results
The findings were grouped into two categories: socio-demographic characteristics and themes-related data.
Socio-demographic Characteristics
Socio-demographic Characteristics of the Patients (n = 15).

Ca = Cancer; HCC = Hepatocellular Carcinoma.
Socio-demographic Characteristics of Nurses (n = 15).
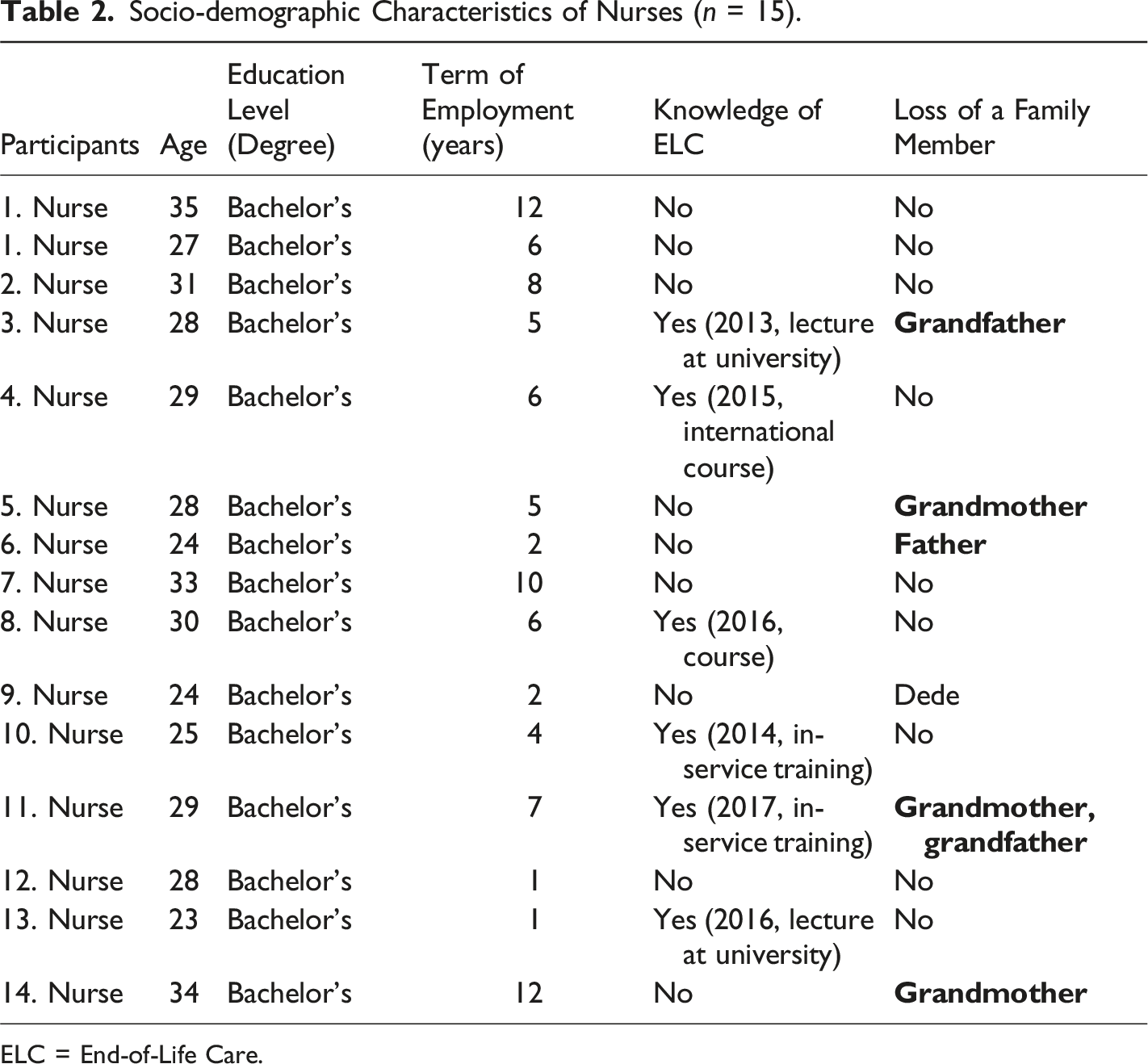
ELC = End-of-Life Care.
Themes-related Data
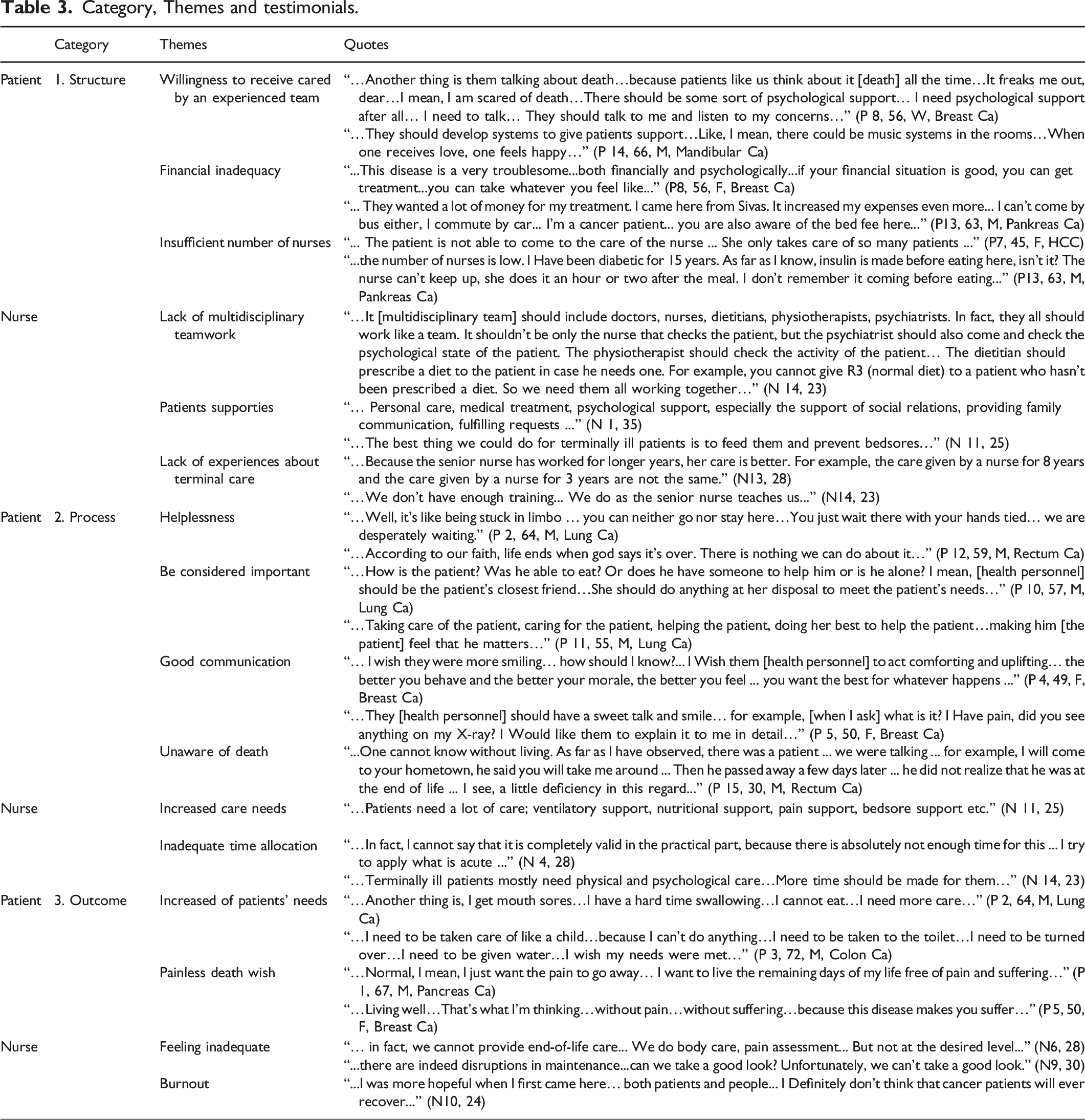
Category, Themes and testimonials.
Categories and Themes for Patients
Semi-structed interviews with patients revealed three categories, nine themes and quetos regarding their views on ELC (Table 3). The categories and themes were Structure (willingness to receive cared by an experienced team, financial inadequacy, insufficient number of nurses), Process (helplessness, be considered important, good communication, unware of death) and Outcome (increased of patients’ needs, painless death wish).
Category 1: Structure
Theme 1: Willingness to Receive Cared by an Experienced Team
End-of-life patients stated that healthcare professionals should receive training and the system of caring for patients should be developed. It seems that patients want a competent healthcare team who can care for patients whose death is imminent.
Theme 2: Financial Inadequacy
In this theme, patients stated that they had difficulty in sustaining their material life due to the chronic process of cancer disease and meeting what they wanted in their last period.
Theme 3: Insufficient Number of Nurses
The patients stated that the number of nurses was not sufficient and their care was not done as they wanted.
Category 2: Process
Theme 4: Helplessness
Patients stated that they could neither live nor die, that death could happen at any time and that there was nothing they could do but wait for death. Patients generally stated that they felt helpless and could do nothing.
Theme 5: Be Considered Important
End-of-life patients stated that they expect more attention from health personnel because they need attention.
Theme 6: Good Communication
End-of-life patients stated that nurses should be more friendly, talk to them and be in constant communication with them, and thus they will feel better.
Theme 7: Unaware of Death
Patients stated that they could not get enough information from their nurses and doctors about their condition. For this reason, it was determined that patients could not prepare for death and they could not say goodbye to their relatives.
Category 3: Outcome
Theme 8: Increased of Patients’ Needs
During the end-of-life period, patients’ needs increased. They need more physical and psychological care, and they expect these needs to be met.
Theme 9: Painless Death Wish
Patients generally stated that they wanted to die comfortably without suffering, and to spend their remaining time without pain.
As a result of semi-structured interviews with end-of-life cancer patients, patients generally stated that they could not get the care they wanted, the care provided changed from nurse to nurse, that nurses tried to provide care as much as they could, but the current end-of-life care system and training were not sufficient. Patients also stated that their physical care needs such as wound care, treatment application and follow-up were met. However, they emphasized that psychospiritual care needs such as talking about death, fear of death and anxiety, and social and environmental care needs such as being in the hospital and sick room constantly and fulfilling their last wishes were not met.
Main Themes and Sub-Themes for Nurses
Semi-structed interviews with nurses revealed three categories, seven themes and quetos regarding their views on ELC (Table 3). The categoies and themes were Structure (Lack of Multidisciplinary Teamwork, Patients supporties, and Lack of experiences about terminal care), Process (Increased Care Needs and Inadequate Time Allocation) and Outcome (Feeling Inadequate and Burnout,).
Category 1: Structure
Theme 1: Lack of Multidisciplinary Teamwork
The nurses generally emphasized the importance of team members cooperating with each other to meet the needs of the patients and to cope with problems.
Theme 2: Patients supporties
Nurses stated that patients should be supported especially in terms of physical and psychological care.
Theme 3: Lack of experiences about terminal care
In this theme, nurses stated that their experiences on the end-of-life period was not sufficient and that they provided care from their seniors as far as they could see.
Category 2: Process
Theme 4: Increased Care Needs
Nurses stated that physical and psychological care needs of patients at the end-of-life increase and that meeting physical care needs in particular is of primary importance to patients.
Theme 5: Inadequate Time Allocation
Nurses stated that all the care (psychological, social, spiritual ...) needed by the patients should be given, but they could meet their acute care (physical) because they could not have enough time.
Category 3: Outcome
Theme 6: Feeling Inadequate
In this theme, nurses stated that they could not provide adequate and desired level of care to end-of-life cancer patients.
Theme 7: Burnout
Nurses stated that they experienced burnout due to the transformation of empathy into sympathy over time and their inexperienced work in the service.
Additionally, the interviews revealed that although the nurses wanted to provide the necessary care, they could not accomplish it because of excessive workload, lack of cooperation among the multidisciplinary team, the patients were not adequately informed, and the education and knowledge levels of the existing nurses and health care team were not at the desired level.
As a result of semi-structured interviews with nurses, nurses generally could not provide end-of-life care for their patients, they gave priority to physical care for their patients, they could not find enough time for other care, and the cooperation of the multidisciplinary team was insufficient. In addition, there was no difference in care between nurses who received and did not receive end-of-life care training. Nurses who received end-of-life care training were aware that there should be a holistic approach in care and that only acute intervention should not be made. The nurses who did not receive end-of-life care training stated that they were worried about the care they provided and the end-of-life care process.
Discussion
The aim of this study is to determine the needs of end-of-life cancer patients’ and their nurses’ perspectives and experiences regarding the end-of-life period.
The Donebedian model, which is used to determine the quality of service and care in health, constitutes the theoretical framework of the research. The models used in the research conceptually reveal the results for determining the needs of patients and people, making the process more comfortable, and developing professional practices based on a holistic view. In addition, models become tools to remind us of different components of care that we ignore or forget (Alligood, 2013; Bayat, 2017; Voyce et al., 2015). The end-of-life care needs, which are the findings of the research, are presented as components and outputs through the Donabedian model. The needs were identified in this way provided guidance for improving care and ensuring a good death process.
People have cultural differences due to different societies, environments, life, and beliefs. Due to these cultural differences, individuals' end-of-life views also differ. End-of-life period generally is perceived negatively. Although there is a belief in life after death in our Turkish culture and Islam, it is observed that the fear of death is dominant. The health personnel working with patients and their relatives have difficulty in talking about death. The reason for this is that the patients and health personnel with a negative perception of death do not feel comfortable and competent in this regard.
Patients receiving end-of-life care are still alive, living, and need care. Kim and Seo’s (2016) qualitative study with 11 nurses found that when nurses made patients feel that they existed, patients felt better and could cope better with the fear of death. In our study, patients emphasized the importance of receiving care and attention while expressing their thoughts, and the nurses emphasized the importance of providing time and physical and psychological support to the patients. Although the nurses were aware of the importance of giving more time to the patient and providing psychological support, they stated that they could only provide physical care because of the excessive workload. It is important problem of the nurses’ inability to provide high-quality care to the patients because the excessive workload is prevalent worldwide, and not only in our country. However, end-of-life cancer patients need more care and special attention compared to other patient groups. Therefore, the health and hospital policies of the countries should be rearranged according to end-of-life patient care.
Globally, the most frightening situation for end-of-life patients is suffering, while the perception of quality death involves painless death, peace, and comfort. Failure to provide a quality death process in the post-life period harms human dignity and leads to ethical problems (Hold, 2017). In our study, patients and nurses stated that for quality death and care, the experienced multidisciplinary team should reserve sufficient time and provide psychological and physical care support.
The health workers have difficulty in communicating with end-of-life patients due to the notion of dragging the patient to despair, assuming that the patient will be harmed and that they are not ready for the end-of-life period. The multidisciplinary team should communicate with each other to provide quality care and good death process. Walzack et al. (2014) reported that patients and doctors improved their quality of life by using nurse-based communication support systems in a randomized controlled study. However, Mitchell et al. (2011) reported that the patients who did not receive end-of-life care support had more psychological problems than those who did. To provide quality care to end-of-life patients, the healthcare team should have sufficient knowledge and professional experience of end-of-life (Coffey et al., 2016). The healthcare team members who are inadequate in terms of education can cause inadequacy in physical care, psychological support, information, communication, providing end-of-life care, and determining the priorities of the end-of-life patient (Kim & Seo, 2016). In our study, it was determined that the patients had limited communication with the health personnel and family, they could not talk about death, and some patients remained hungry for a long time. On the other hand, it was also determined that the nurses' average years of professional experience were low. The nurses could not determine the patients’ care priorities, did not provide adequate care, did not provide adequate information to the patient, continued aggressive treatment practices, and tried to provide end-of-life care according to their own experiences. The reason for this situation is thought to be the negative perception of death in our culture, the lack of education among nurses about end-of-life care, and difficulty in communicating with end-of-life patients. Additionally, it is undeniable that nurses do not allocate sufficient time to the patients due to the high workload, and that may result from not having a palliative care understanding in a system aiming to treat.
Strengths and Limitations
The strength of this research is that semi-structed interviews of individuals were conducted to obtain their sincere opinions, ideas, and feelings. Additionally, it was ensured that the interviews were conducted in a informal conversation so that individuals could express themselves freely.
The study had some limitations. It was observed that the nurses’ and physicians’ definitions of end-of-life patients were different and inadequate. For this reason, since the end-of-life care patients interviewed could not be detected beforehand, the duration of the interview was shortened because of fatigue and hoarseness. It was also difficult to find patients who needed to express themselves because of the lack of palliative care service in the affiliated hospital and the fact that the patient rooms were usually for two persons.
Conclusion
When the results of the study are considered, death is seen as an inevitable end from the patients and their nurses. Nurses stay away from meeting the needs of patients due to reasons such as not being able to face the facts and not being able to talk about death. In this case, it can prevent patients from feeling lonely and insignificant and from expressing their feelings. As a result, patients may exhibit either aggressive and aggressive or depressive and introverted behaviors. According to the results, it was found that the patients’ expectations were not met by the nurses. This was known by the nurses, but they could not provide the care they wanted to give because of the workload and lack of information. We think that our study will contribute to the quality care of cancer patients in the end-of-life period, eliminate deficiencies, and improve the current order. Unfortunately, our country is not in a very good position concerning end-of-life care and is at the initial level. Therefore, better support and guidelines are needed to provide the desired end-of-life care and the basis for implementation. In this study, the opinions of patients and nurses about the care provided were taken in order to eliminate the lack of care at the end of life and to increase the quality of care provided. This study is a valuable resource as a qualitative study that illuminates the perceptions of patients and nurses at the end-of-life period and care through interviews. We will plan the necessary training and cooperate to improve the quality of care provided by the end-of-life healthcare team. In addition, it is recommended to train the healthcare team, to include this training in the undergraduate education programs, to conduct academic studies such as national congresses, symposiums, and panels, to provide in-service training within institutions, and to provide various academic consultancy. It is also necessary to establish associations for the end-of-life period, to develop the aims and objectives of the established associations, to increase the association members, to raise the awareness of the society through these associations, to establish separate care units for end-of-life care, and to establish different projects. A sufficient number of experienced staff should be provided. The multidisciplinary team should have end-of-life care experience. Ministerial support should be provided in the establishment of these units.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Kübra TERZİ RN, PhD(c), Research AsisstantHacettepe University, Sıhhıye Campus, Nursing Faculty Internal Medicine Nursing Department Altındağ/Ankara-TURKEY, phone: +90(312) 305 15 80-177, Fax: +90(312) 312 70 85, e-mail:
Sevgisun KAPUCU, RN, PhD, Professor DoctorHacettepe University, Sıhhıye Campus, Nursing Faculty Internal Medicine Nursing Department Altındağ/Ankara-TURKEY, phone: +90(312) 305 15 80-124, Fax: +90(312) 312 70 85, e-mail: