
Abstract
Hospice bereavement programs in the United States lack standardized guidelines, resulting in service disparities and underutilization. While many hospice bereavement programs focus on pathologizing grief, humanistic approaches remain underexplored. The purpose of this study was to assess the current structure and challenges of hospice bereavement programs and to gather coordinators’ recommendations to inform the development of a foundational minimum standards for supporting healthy grieving. This quantitative study gathered data through online surveys from bereavement coordinators in California. By aligning these findings with standards from the Center for Medicare and Medicaid Services and the National Hospice and Palliative Care Organization standards, the Humanistically Universalizing Grief (HUG) model was developed, which provides core principles and advisory guidelines for hospice bereavement care. The HUG model offers a structured yet adaptable framework to improve program consistency, accessibility, and equity, ensuring bereavement care is comprehensive, sustainable, and responsive to the diverse needs of grieving individuals.
Introduction
Bereavement support is a core component of hospice care in the United States; however, its structure and delivery remain poorly defined. Medicare defines bereavement counseling as “emotional, psychosocial, and spiritual support and services provided before and after the death of the patient to assist with issues related to grief, loss, and adjustment” (National Alliance for Care at Home, 2022, p. 1). Under the Medicare Hospice Benefit, hospice agencies are required to offer bereavement services to family members for at least one year following a patient’s death (Code of Federal Regulations, 2026; Kaiser Permanente, 2024; U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation [HHS-ASPE], 2023). Despite this mandate, federal regulations do not specify which services should be provided, nor how bereavement care should be delivered.
In the absence of clearly defined standards, hospice bereavement care is characterized by substantial variability and inconsistency. Prior research has documented wide variation in the types of services offered, the timing of service delivery, the populations served, as well as in the professional qualifications of those providing care (Bartley et al., 2025; Becker & Cagle, 2021, 2023; Dean et al., 2014; Ghesquiere et al., 2015; Giang et al., 2025; Lichtenthal et al., 2024). Despite the National Hospice and Palliative Care Organization (NHPCO) publishing draft bereavement standards in 2022, no state or federal policies currently mandate specific bereavement program components. Consequently, hospice bereavement services vary widely from minimal offerings like informational brochures to comprehensive programs that include individual and family counseling qualified mental health professionals (Becker & Cagle, 2021).
The lack of formalized standards reflects a broader pattern of limited attention to bereavement care within service delivery. As highlighted by the Lancet Commission on the Value of Death (2022), bereavement has historically received insufficient recognition in policy and practice. Additionally, the lack of federal specified mandates for hospice services creates disparities in service implementation and outcome goals for bereaved family members (HHS-ASPE, 2023). A study of over 600 agencies across the United States highlighted this issue, finding that bereavement support most often consisted of mailing written materials to families with no formal follow-up communication (Becker & Cagle, 2023). While individual counseling was offered in some circumstances, it had low utilization (Becker & Cagle, 2021). The evidence highlights a deficit in both the standardization of hospice bereavement programs and the inclusion of grief normalization approaches.
This is underscored by a systematic review of 44 bereavement program evaluation reports published between 2000 and 2018 (Wilson et al., 2021). The authors pinpointed evaluation methods and concluded that formal bereavement program evaluations were ad hoc and inconsistent, failing to yield the quality of information needed to retain, enhance, or expand bereavement programs. Furthermore, only 12 out of the 44 studies were conducted in the United States, with none including hospice settings. This suggests that evaluations have been conducted at a rate of only one per year over the past 18 years.
Another systematic review examined how services met their responsibilities for ensuring continuity of support for families after a patient’s death (Jurgens et al., 2025). Researchers concluded, “No articles provided a robust evidence base for their model of care, which is an area worthy of much greater attention” (2025, p. 10). Additionally, their study highlighted the need for clearly defining the primary purpose of services and ensuring bereaved needs align with national standards.
In 2023, the United States Congress directed The Agency for Healthcare Research and Quality (AHRQ) to establish an evidence base for what constitutes high-quality bereavement and grief services. However, AHRQ ultimately determined that there remains, “important gaps in our knowledge of various aspects of bereavement care” concluding that “more work is needed to understand for whom, and in what ways, could the identification, assessment, and treatment of grief be most appropriate and effective…” (2025, p. 58). Giang et al. (2025) statewide assessment of bereavement services also indicated that due to rising mortality rates in the States, “bereavement represents a significant public health concern, “and that “little is known about the availability and distribution of bereavement services…” (p. 1). Globally, the review from the UK’s Commission on Bereavement (2022), also highlighted unequal access to appropriate formal support, noting that some groups are especially poorly supported. It also described social, organizational, and structural factors that negatively influence people’s experiences of bereavement and limit their ability to access help. All these gaps underscore the need for greater clarity, consistency, and empirical examination of hospice bereavement programs.
U.S. Evaluation of Hospice Bereavement Services
The Hospice industry’s gold standard evaluation tool is the Consumer Assessment of Healthcare Providers and Systems (CAHPS) Hospice Survey. The CHAPS survey is a 47-item questionnaire to rate and measure the experiences of patients who died on hospice care, as well as the understandings of their primary caregivers. The Centers for Medicare & Medicaid Services (CMS) established the CAHPS Hospice Survey with contributions from many stakeholders, including other government departments, industry stakeholders, consumer groups, and other vital individuals and establishments that partner in hospice care. However, only one section of the questionnaire is focused on emotional support and consists of the following two questions; (1) While your family member was in hospice care, how much emotional support did you get from the hospice team? (2) In the weeks after your family member died, how much emotional support did you get from the hospice team?
Only one of the above questions is directed towards post-death emotional support and it does not specifically indicate whether the support is provided through a hospice bereavement program. The CAHPS hospice survey response rate for the public reporting period spanning the fourth quarter of 2023 through the third quarter of 2024 was 28%, which is consistent with response rates reported in prior patient experience research (CAHPS Hospice Survey, 2025; Casarett et al., 2010; Klein et al., 2011). Parast et al. (2018) observed that the caregivers of descendants from racial/ethnic minority groups, as well as those whose hospice services were covered by Medicaid, had lower CAHPS survey response rates.
Currently, the CAHPS survey, the discipline’s gold standard measure of hospice care, has several notable limitations: (1) the survey is voluntary and relies solely on self-reported data from bereaved caregivers, (2) national response rates are low, with some agencies reporting even lower rates, limiting the statistical reliability and generalizability of the findings, (3) Of the 47 survey items, only two address emotional support, representing just 4% of the overall content (4) people of color are significantly underrepresented among respondents.
There is currently no standardized data collected across hospice agencies regarding bereavement program services. Beyond the limited number of U.S. based hospice bereavement program evaluation studies, little is known about (1) participation rates in hospice bereavement programs, (2) the types of services offered, (3) program structure and design, (4) participant outcomes, and (5) programmatic limitations. As noted earlier, the screening tools and surveys commonly used in hospice settings tend to adopt a pathologizing lens on grief and often fail to account for the cultural and environmental factors that shape grief behaviors and responses.
The aim of this study was to examine the current structure and challenges of hospice bereavement programs and to elicit bereavement coordinators’ recommendations for future standards, with the ultimate goal of informing the development of foundational minimum standards grounded in humanistic frameworks that support culturally, spiritually, and somatically affirming approaches to healthy grieving.
Hospices Utilizing Pathologized Frameworks for Grief Within the United States
Within hospice programs in the United States, CMS mandates bereavement services be provided to family members for one-year following a patient’s death. In 2022, 1.72 million patients received hospice care in the United States (National Alliance for Care at Home, 2024). This figure does not account for all the bereaved family members who are also eligible for bereavement services under the hospice requirements. Although the Medicare Hospice Benefit mandates hospices to provide grief support to families, it does not specify what services should be offered or how they should be delivered (Becker & Cagle, 2023). CMS’s regulations further state, “An initial bereavement assessment of the needs of the patient’s family and other individuals focusing on the social, spiritual, and cultural factors that may impact their ability to cope with the patient’s death. Information gathered from the initial bereavement assessment must be incorporated into the plan of care and considered in the bereavement plan of care” (Code of Federal Regulations, 2026, p. 385).
Given this lack of specificity, many hospice programs rely on various established evidenced-based screening tools, such as the Bereavement Risk Assessment Tool (BRAT) and Bereavement Risk Index (BRI) (Lawler et al., 2020) to identify symptoms of Prolonged Grief Disorder (PGD) and meet this requirement. However, these measures fail to assess the full psychosocial factors shaping the grief experience, thus limiting the scope and responsiveness of care provided.
In a national survey of 591 U.S. hospice agencies, Ghesquiere et al. (2015) found that nearly all of the agencies used screening tools to identify PGD, underscoring the predominant reliance on diagnostic-focused assessment to guide bereavement care. However, these screening tools have limited function in assessing the whole person and providing a comprehensive biopsychosocial assessment. Not all individuals experiencing grief will meet criteria for PGD and even when they do, it would fall outside the scope of practice of hospice care. Additionally, a diagnosis of Prolonged Grief Disorder requires that the loss occurred 12 months prior (American Psychiatric Association, 2022).
Given that hospice programs are required to offer bereavement support for one year after the death of a patient’s loved one, evaluating for prolonged grief disorder (PGD) during this timeframe would be considered premature. Assessments and hospice bereavement services should be comprehensive, considering individuals’ natural emotional, neurobiological and physical responses to loss, as well as cultural contexts that shape grief. To date, however, no research has examined grief assessments in hospice bereavement programs primarily through a humanistic lens.
Literature Review
Importance of Humanizing Grief
Humanizing grief invites consideration of whether bereavement may be better understood as a natural, multidimensional human response to loss, rather than primarily as a condition requiring resolution or normalization through intervention. Contemporary clinical and public-health literature consistently frames grief as a universal response to the death of a loved one, encompassing emotional pain, yearning, and fluctuating awareness of loss that are expected for most individuals and not inherently pathological (National Center for Biotechnology Information [NCBI], 2025; Phillips et al., 2025).
Empirical research across diverse populations further demonstrates that grief is characterized by sadness, longing, and meaning-related distress that unfold over time and reflect the enduring significance of attachment and relationship, rather than dysfunction (Bonanno et al., 2002; Bowlby, 1980; Neimeyer, 2001; Nielsen et al., 2025; Redican, 2026; Wortman & Silver, 2001a). Longitudinal and scoping studies emphasize that while grief trajectories vary considerably, the emotional experience of bereavement remains embedded in ordinary human life and persists precisely because meaningful bonds do not end with death (Bonanno and Papa, 2003; Freud, 1917/1957; Klass et al., 1996; Raine and Kamal, 2025; Stroebe et al., 2017). Within hospice care, this perspective underscores the importance of bereavement services that validate grief as a legitimate and meaningful response to loss, rather than framing it as a condition requiring resolution or correction.
Grief is also embodied, with physical responses that are widely documented as part of the normal grieving process. Clinical and public-health sources describe fatigue, sleep disturbance, appetite changes, chest tightness, headaches, gastrointestinal discomfort, and generalized bodily pain as common and expected following bereavement (Bonanno et al., 2002; Bowlby, 1980; NCBI, 2025; Raphael, 1983; Stroebe et al., 2007). Empirical studies show that bereaved individuals frequently report somatic symptoms that correlate with grief intensity without indicating underlying medical pathology (Lindemann, 1944; Parkes, 1972; Sillis et al., 2022; Stroebe et al., 2007).
Longitudinal research further demonstrates that symptoms such as insomnia, bodily tension, and fatigue commonly diminish over time as individuals adapt to loss (Mancini et al., 2011; Nielsen et al., 2025; Nordström et al., 2024; Ott et al., 2007; Wortman & Silver, 1989). Psychosomatic research suggests that these physical manifestations reflect transient dysregulation of stress-response systems and autonomic arousal that accompany emotional distress, rather than illness or disorder (Cohen et al., 2007; Lenzo et al., 2025; McEwen, 1998; Thayer & Lane, 2000). Importantly, contemporary grief frameworks emphasize normative grief responses and should not be automatically medicalized (Cunningham et al., 2025; Hilberdink et al., 2023; Horowitz et al., 1997; Wakefield, 2012; Wortman & Silver, 2001b).
From a neurobiological perspective, grief represents the brain’s normal response to the loss of an attachment figure—someone whose presence had been repeatedly expected and relied upon (Bowlby, 1982; Friston et al., 2017; O’Connor & Seeley, 2022; Panksepp, 1998). The brain operates as a predictive system, continuously generating expectations about relationships, routines, and emotional safety based on prior experience (Parr et al., 2022). When death occurs, the brain must reconcile a profound mismatch between long-standing neural predictions (e.g., “this person will be here”) and the new reality of permanent absence, producing prediction-error signals that contribute to the emotional, cognitive, and physiological features of grief (Friston, 2010; O’Connor & Seeley, 2022; Panksepp, 1998; Ratcliffe & Velasco, 2024).
Neuroimaging studies show that reminders of the deceased activate brain networks involved in autobiographical memory, emotional salience, and cognitive regulation, reflecting the brain’s effort to integrate loss into existing self-referential frameworks (Evstigneev et al., 2025; Michel et al., 2023; Ochsner & Gross, 2005; O’Connor et al., 2010; Svoboda et al., 2006). These neural patterns are typical during bereavement and generally evolve over time, with persistent alterations observed primarily among individuals experiencing prolonged or impairing grief (O’Connor, 2022; Seeley et al., 2022).
Grief also unfolds within cultural contexts that shape how loss is understood, expressed, and supported—an especially salient consideration in hospice bereavement care. Cultural norms influence whether grief is expressed publicly or privately, which emotions are emphasized or restrained, and which mourning practices (e.g., prayer, memorial rituals, food sharing, ancestor veneration, or continuing spiritual bonds) are considered meaningful and healing (Dein, 2024; Durkheim, 1912/1995; Freud, 1917/1957; Malinowski, 1925; Phan et al., 2025; Van Gennep, 1909/1960). Within hospice settings, these frameworks affect how families interpret bereavement outreach such as condolence calls, support groups, and memorial services, and whether such services are perceived as supportive or misaligned with family values (Aeschlimann et al., 2024; Killikelly et al., 2023).
Research further highlights that culturally grounded idioms of distress, migration histories, religious worldviews, and collective family roles shape both grief trajectories and willingness to engage with formal bereavement services (Killikelly et al., 2023; Kleinman, 1995; Le et al., 2025; Neimeyer et al., 2014; Rosenblatt, 2008; Sue et al., 1991). Consequently, hospice bereavement care increasingly emphasizes cultural humility, prioritizing responsiveness, flexibility, and partnership over standardized assumptions about grief expression or recovery timelines (HHS-ASPE, 2023; Madni et al., 2022, p. 57).The Agency for Healthcare Research and Quality’s (AHRQ) systematic review on bereavement care stated, “The grief experience is highly influenced by the sociocultural contexts in which people live; necessitating culturally-tailored approaches to grief assessment and intervention” (2025, p. 57).
To clarify the conceptual foundations underlying this review, the following guided frameworks are provided to show grief as a normal emotional, physical, neurobiological, and cultural process, rather than a pathological condition.
Natural emotional responses to loss: The experience of grief as an emotion reminds us of the profound significance and irreplaceable nature of others, and it is deeply ingrained in our existence. It suggests, in an intellectual sense, that true loss cannot be recovered. Truly, following a time of grieving, numerous individuals who have experienced loss are able to find joy and fulfilment in their lives. However, it is important to acknowledge that the loss itself cannot be undone. (Mammen & Mironenko, 2015)
Natural physical responses to loss: Grief inscribes itself on the body – in a process, referred to as impression – and is simultaneously expressed by the body in various social and material contexts. In other words, grief is a cognitive emotion that informs the embodied person about something in the world, and it is a communicative emotion that conveys significant information to others. (Brinkmann, 2019 p. 291)
Influences of neurobiology to loss: Stanislas Dehaene states, based on what we know, virtually all the brain’s regions can participate in both conscious and unconscious thought” (Dehaene, 2014, p. 53). This suggests that individuals who have experienced loss may continue to have thoughts, memories, and emotions related to their grief for an extended period of time, possibly even years. Additional emotions linked to the loss, like frustration, remorse, anxiety, and sadness, can occasionally arise unexpectedly in reaction to seemingly insignificant triggers (Holinger, 2020).
Cultural influences (communal, social, institutional, interpersonal): In order to comprehend how a member of a particular culture handles loss, it is necessary to not only identify that culture but also evaluate the congruence between their own bereavement process and the expectations that their culture appears to have for bereaved individuals. (Shapiro, 1996)
Grief is both an emotion that is felt and imprinted upon the body, as well as something that is expressed via the body in social environments (Køster, 2022; Pearce, 2020). The body is simultaneously physiological, ecological, phenomenological, social, and cultural (Fuchs, 2018). Grief, like other emotions, entails an appraisal of the situation one is in (in the case of loss) resulting in a cognitive component (Bonanno & Papa, 2003), but it also has a social and communication component as bodies convey grief through unique postures, gestures, gazes, and comportments (Keck et al., 2022; Lopez et al., 2017).
To examine these concepts in practice, the present study utilized a quantitative survey approach to assess bereavement coordination and minimum standards within hospice settings.
Method
Study Design
This quantitative study utilized a pragmatic epistemological framework, which conceptualizes knowledge in terms of its practical utility and real-world consequences. Pragmatism emphasizes the value of ideas and interpretations based on their capacity to inform action and decision-making, making it particularly appropriate for applied research examining hospice bereavement practices through an online survey methodology (Johnson, 2016). Consistent with this orientation, the present study seeks to generate findings that are not only empirically informative but also relevant to the delivery and refinement of hospice bereavement services. In alignment with this framework, the study is guided by the following research question: How do current hospice bereavement programs vary in structure, delivery, and utilization due to the absence of standardized guidelines?
Drawing on classical pragmatist thought, meaning is understood as arising from experience and as inherently shaped by contextual conditions (Peirce, 1903). In the context of an online survey, participants’ responses are embedded within specific professional, organizational, and digital environments, and attending to these contexts strengthens the interpretation of the data. Pragmatism further supports analytic flexibility and openness to multiple perspectives, which is essential given the geographic diversity and varied professional experiences of hospice bereavement coordinators. This epistemological stance enables the integration of heterogeneous viewpoints while maintaining a focus on the practical implications of the findings for hospice bereavement care.
Sample
A non-probability purposive convenience sampling strategy was used, in which participants were selected based on accessibility and relevance to the study population, consistent with common practice in exploratory social science research (Jager et al., 2017). Snowball sampling was also employed, whereby contacting or participating coordinators referred other eligible colleagues for potential inclusion. Bereavement coordinators employed by CMS-certified hospice agencies across California were eligible for inclusion. The 2020 publicly available Medicare Acute Care and Hospice dataset (Center for Medicare & Medicaid Services) was used to identify eligible agencies. To enhance sample heterogeneity, agencies with varying hospice census sizes, annual Medicare reimbursement levels, and ownership types were targeted. This study employed a small sample to ensure focus on hospice bereavement programs and services and obtain relevant data for future bereavement program research.
Respondent Demographics
Hospice Bereavement Coordinators and Hospice Program Demographics

aData is presented as frequency and percentage of total n = 23.
Data Collection
Seventy hospice agencies were contacted to invite bereavement coordinators to participate in the online survey. The target sample size was 20 bereavement coordinators. Inclusion criteria required participants to be currently serving as hospice bereavement coordinators within California. Exclusion criteria included non-active coordinators, non–English-speaking individuals, and those affiliated with agencies outside California. A web-based survey was used due to its advantage of being cost-effective, relatively quick to implement, and efficient in collecting data from multiple participants.
The sampling frame for this survey included 70 potential respondents, representing the number of cold calls made. The online survey was open from November 2023 to February 2024. Of the 70 individuals contacted, 27 initiated the survey, and 23 completed it. This yielded a response rate of 39% and a completion rate of 85%.
Procedures
After receiving Institutional Review Board approval from Loma Linda University (IRB# 5230412), 70 hospice agencies were contacted via phone to speak with their designated bereavement coordinator to (1) introduce the study (2) determine their interest in participating and (3) obtain permission to collect their contact information (email addresses) for survey distribution. Interested participants were then emailed a hyperlink to the online survey. The first page of the survey consisted of the informed consent form outlining the study’s objectives and instructions for participation. Access to the online survey was open for 60 days. Reminder emails were sent on days 15 and 30 to participants who had not completed the survey.
Instrument
This exploratory quantitative web-based survey was used to collect information from hospice bereavement coordinators. A 19-item web-based survey was developed and was intended to gather hospice bereavement program data to formulate advisory guidelines that consider various agencies’ unique characteristics (i.e., population served, staffing, resource allocations, geographic locations etc.) This online survey was created with Qualtrics software and had three sections (1) demographics (2) characteristics of bereavement program and (3) bereavement program recommendations.
The first section gathered demographics with four multiple choice questions related to the hospice agencies and bereavement coordinators (i.e., hospice last three digits of zip code, years at agency, degree level etc.) The second section consisted of ten multiple choice questions directed at current bereavement program characteristics and aspects (i.e., staffing, development of hospice program, barriers, bereavement services offered etc.) The third section had four multiple choice questions and one open-ended question that focuses on bereavement coordinator’s hospice bereavement program recommendations (i.e., importance of national standards, what services should be a standard etc.) One final question allowed respondents to provide additional responses not captured within predefined categories.
Data Analysis
Content analysis was employed as a systematic approach to examine patterns and distributions within structured survey data. This method is appropriate for closed-ended responses, as it facilitates the organization and quantification of categorical and ordinal data. Accordingly, descriptive statistics were generated, including frequencies and percentages for demographic, multiple-response, and ranking items, and means for scaled responses. Content analysis was also used for the single open-ended question at the end of the survey.
Results
The results from this quantitative study describe the organizational characteristics, staffing patterns, and service practices of hospice bereavement programs in California. Analyses focused on identifying commonalities and variations in bereavement program structures, the range of services provided, and bereavement coordinators’ perspectives on program evaluation and standardization. Findings are organized into three primary domains: bereavement program staffing, bereavement program services, and bereavement coordinators’ recommendations for standardization.
Bereavement Program Staffing
Approximately 70% of the respondents reported that the social work profession plays a significant role in hospice bereavement programs. Approximately 61% of the respondents used volunteers for services. 43% of the agencies involved in the study identified using interns, MFTs (Marriage and Family Therapists), LMFTs (Licensed Marriage and Family Therapists), and trainees (see Table 1). Lastly, the average full-time equivalent (FTE) for bereavement staffing was 3.22 FTEs per agency. The smallest agency having .600 FTEs and the highest agency with 12.2 FTEs.
Bereavement Program Services
Nearly 90% of the respondents stated that their agency supports over 200 bereaved family members annually. This substantial number highlights the significant demand for bereavement services in the community and highlights the importance of agencies in meeting this demand. The top three most commonly utilized bereavement services reported by all hospice programs (100%) were 1-on-1 support groups, condolence phone calls, and condolence cards (see Table 1). The top three culturally affirming approaches identified by over 75% of the respondents included multilingual resources, grief resources, and staff trainings.
Bereavement Coordinators’ Recommendations for Standardization
The findings highlighted that nearly 70% of respondents used program evaluations for bereavement assistance such as postal, internet, and post-counseling satisfaction surveys. Additionally, a significant percentage of respondents (41%) advocated for annual evaluations of hospice bereavement programs as a national norm. However, 32% of respondents expressed the need for flexibility in the timeline of these evaluations, highlighting the importance of considering individual agency needs. Furthermore, a majority of respondents over 80% expressed support for establishing nationwide hospice bereavement standards (see Figure 1). Participants’ who believe national hospice bereavement standards are needed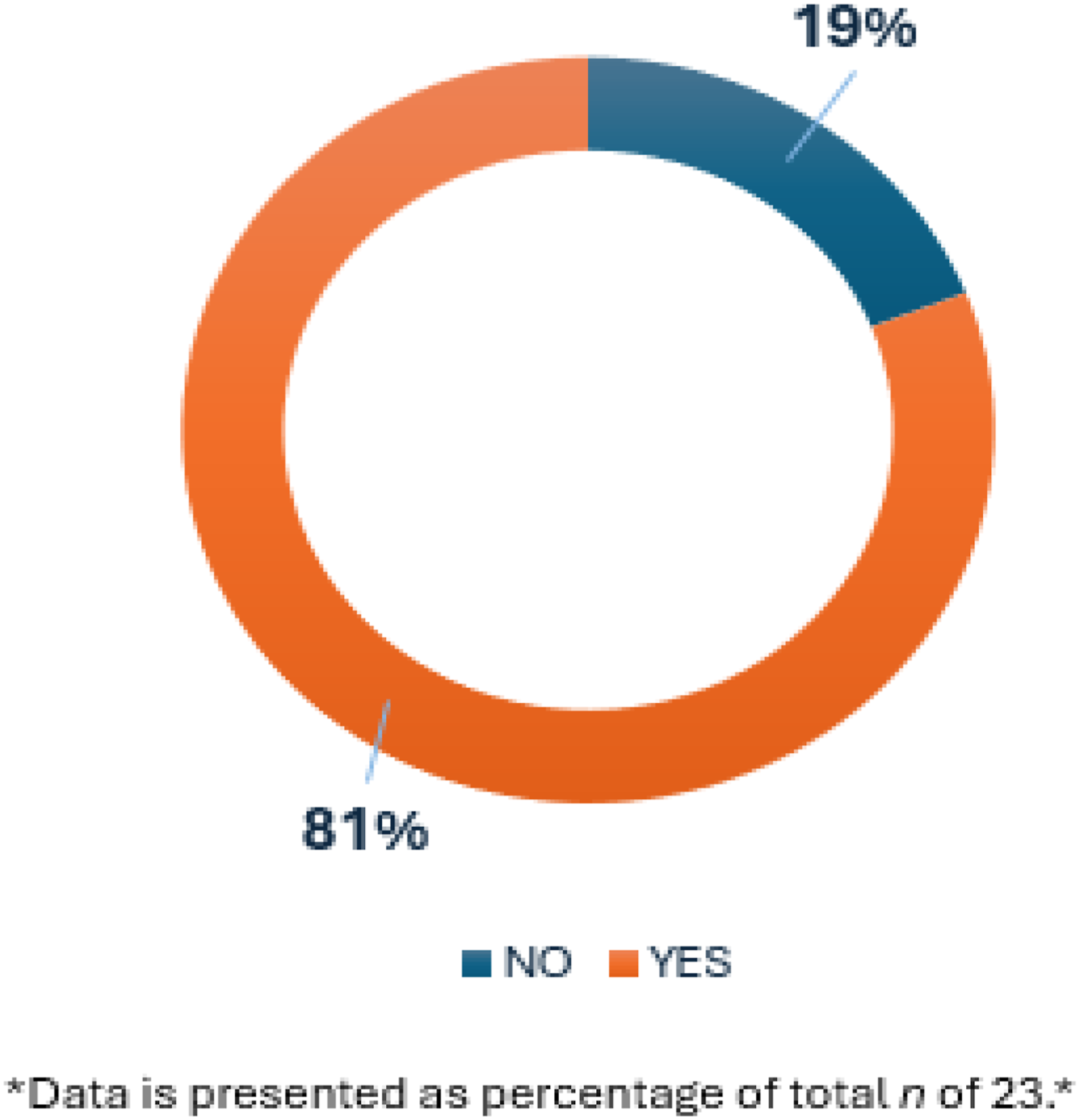
91% of respondents felt that Medicare should reimburse for hospice bereavement services (see Figure 2). Bereavement coordinators indicated that If CMS were to establish specific national standards, the four most important services to provide to bereaved individuals would be (1) Condolence phone calls (2) grief groups (3) 1-on-1 grief support (telephone or home visits) and (4) resources (electronic or mailed.) Participants’ who believe Medicare should reimburse for hospice bereavement services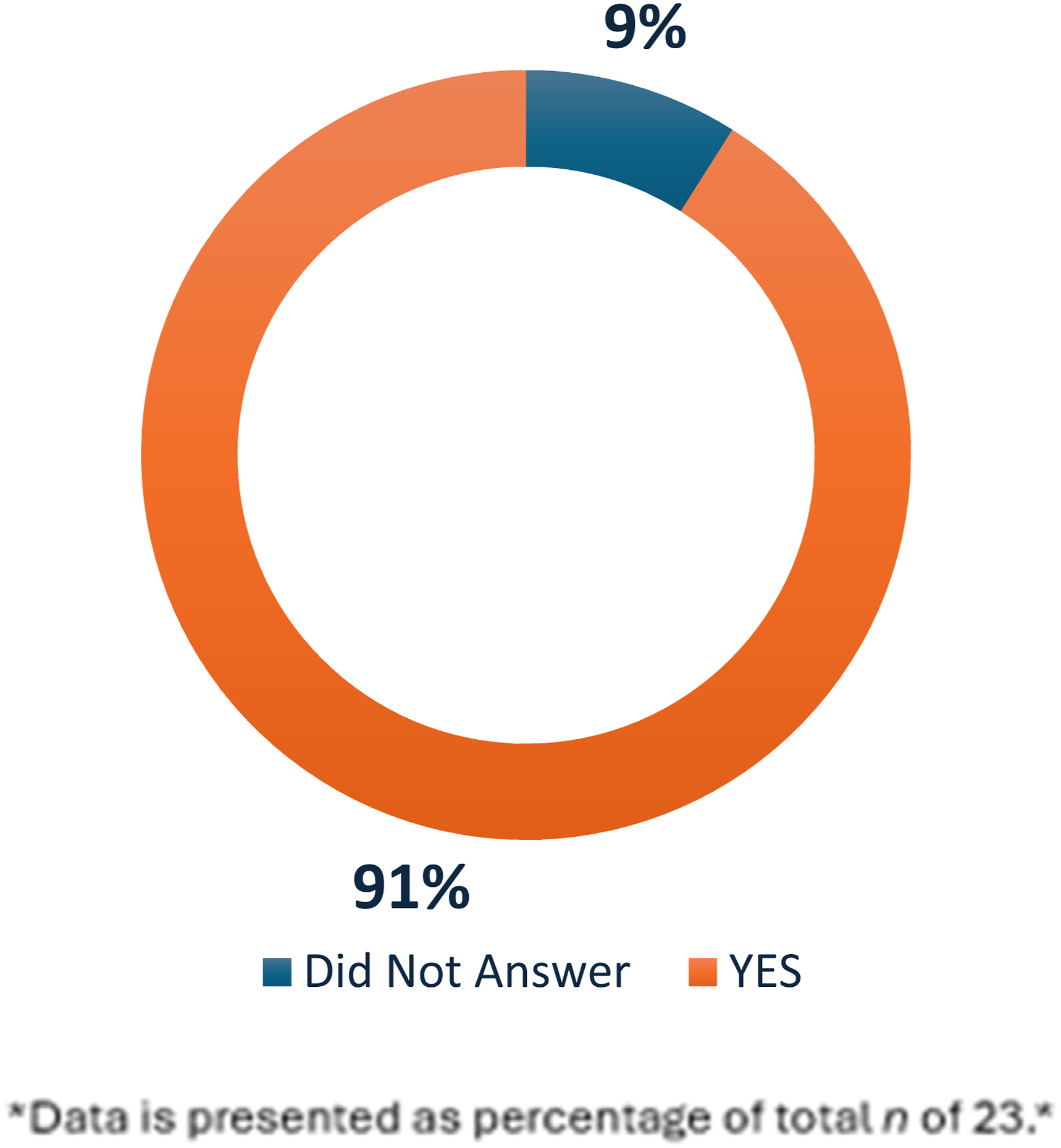
Another noteworthy finding is the wide variance of bereavement staffing across agencies. The results show a range of as little as .600–12.2 full-time equivalents (FTEs) for each agency. For example, one agency servicing less than 100 bereaved per year had 1.0 FTE in comparison to another agency serving over 200 bereaved with only less than 1.0 FTE. The range of agencies serving 200+ bereaved (83%) had a staffing variance between as little as .600 to as high as 12.2 FTEs. These findings suggest a need to consider minimum staffing allocation standards alongside the minimum bereavement service standard for best bereavement service outcomes.
The findings collectively suggest a wide spectrum of hospice bereavement program structures and staffing allocations among participating California agencies. Although certain program elements, such as individualized grief support, group facilitation, and condolence outreach, were nearly universal, the data revealed substantial differences in program evaluation practices, staffing resources, and the scope of available bereavement services.
The findings reveal both consistency and variability across hospice bereavement programs in California. While coordinators expressed strong agreement on the importance of core services, such as condolence outreach, grief groups, and individualized support, the results also highlighted substantial disparities in staffing levels, program evaluation practices, and funding structures. These patterns suggest that although hospice agencies share a commitment to bereavement care, the discipline lacks unified standards and sufficient systemic support to ensure equitable service delivery. The following discussion interprets these findings in the context of current hospice practices and introduces the development of the Humanistically Universalizing Grief (HUG) model as a framework for addressing these identified gaps.
Discussion
Findings from the bereavement coordinator survey revealed substantial variation in bereavement program design and delivery, alongside strong consensus regarding the need for national standards and Medicare reimbursement. These findings underscore a growing professional recognition that bereavement care is an essential component of hospice services rather than an ancillary function. The following sections interpret these findings, outline key challenges, and present the development of the Humanistically Universalizing Grief (HUG) model as a framework with regulatory considerations for advancing standardized and humanistic hospice bereavement care.
A Call for Uniform Standards vs. Operational Flexibility
The strong survey support (80%) for national bereavement standards suggests a unified recognition that hospice bereavement programs lack consistency, and coordinators see value in structured guidelines. However, the fact that 32% of respondents favor flexibility in evaluation timelines implies that rigid implementation of national standards could be impractical given diverse operational constraints. This highlights the need for a hybrid model, using a core set of baseline standards with adaptable components that agencies can tailor based on population size, staffing resources, and regional considerations.
Medicare Reimbursement: A Systemic Shift in Perception
The overwhelming majority (91%) of bereavement coordinators believe Medicare should reimburse hospice bereavement services, reflecting a shift in how bereavement care is perceived within healthcare policy. Historically, bereavement support has been considered a supplementary service, but this data suggests that professionals in the field see it as an essential component of end-of-life care. If reimbursement were to be implemented, it would redefine bereavement care as an integrated part of the healthcare continuum, potentially leading to more specialized staffing, enhanced program structures, and increased accessibility for grieving families who might otherwise receive limited or unknown support.
Staffing Disparities: A Risk to Program Efficacy
The high variability in staffing allocation (0.600 to 12.2 FTEs per agency) exposes a fundamental flaw in how bereavement services are structured. Agencies with low staffing levels but high caseloads likely struggle to provide personalized grief support, potentially leading to delays in service delivery or reduced effectiveness of interventions. If staffing standards were implemented alongside service guidelines, agencies could be better equipped to meet demand without compromising care quality. This issue isn’t merely an operational concern, it directly impacts the mental and emotional well-being of bereaved family members, highlighting the potential crisis in service accessibility.
Priority Services: A Shift Toward Accessibility and Versatility
The identification of condolence calls, grief groups, one-on-one support, and resource distribution as the top four bereavement services suggests that coordinators favor a mix of structured group support and individualized outreach. These findings echo the primary findings of previous studies (Barry et al., 2012; Becker & Cagle, 2023; Demmer, 2003; Foliart et al., 2001). Notably, phone-based and mailed/electronic resources are listed as critical services, which speaks to the increasing role of remote accessibility in grief care. This reflects broader healthcare trends where telehealth and digital interventions are becoming essential tools for delivering care to underserved or geographically isolated populations. Hospice agencies may need to expand virtual bereavement programs, ensuring grieving individuals receive consistent and accessible support even when in-person services are unavailable.
These findings point toward a critical juncture in hospice bereavement care. The strong consensus on the need for national standards and Medicare reimbursement suggests that the field is ready for formalized recognition, while the staffing disparities highlight an operational gap that must be addressed before any policy implementation. The data does not suggest that a rigid, one-size-fits-all approach is feasible, but rather that a structured framework with adaptable elements is necessary. If policymakers and healthcare leaders act on these insights, hospice bereavement care could shift from an inconsistent, underfunded services to a recognized and resourced element of end-of-life care, ensuring that bereaved individuals receive meaningful and equitable support nationwide.
Development Process for the HUG Model, Advisory Guidelines & Core Principles
The HUG model, advisory guidelines and core principles were developed using several methods: (1) A comprehensive literature review that focused on (i) Grief as a humanistic experience (ii) Limitations of pathologizing grief (iii)Variability and underutilization of hospice bereavement services. (2) An online survey given to current hospice bereavement coordinators. (3) Abiding by the current CMS regulations and standards of the National Alliance for Care at Home, formally National Hospice and Palliative Care Organization (NHPCO) for hospice bereavement services.
Regulatory Considerations
These guidelines abide by the Centers for Medicare & Medicaid Services (2026) regulatory standards for Hospice agencies within the United States. These guidelines meet the four elements of the bereavement counseling sector for hospice that include: (i) Have an organized program for the provision of bereavement services furnished under the supervision of a qualified professional with experience or education in grief or loss counseling. (ii) Make bereavement services available to the family and other individuals up to 1 year following the death of the patient. (iii) Ensure that bereavement services reflect the needs of the bereaved. (iv) Develop a bereavement plan of care that notes the kind of bereavement services to be offered and the frequency of service delivery.
Lastly, these guidelines align with the national guidelines that have be developed by the National Hospice and Palliative Care Organization (NHPCO) for bereavement care in hospice (2022), which include: (i) Identify family members in need of bereavement support, prior to and following the death of the patient. (ii) Assess patient and family strengths, bereavement risk, concerns and needs related to grief and loss from start of hospice care through the end of bereavement care. (iii) Empower families to recognize and develop skills to manage grief by exploring ways they have effectively coped in the past and identifying areas of strength and resilience, assisting families in identifying current social and spiritual resources for support. (iv) Refer family members who need services for mental health or other needs that are outside the scope of the hospice bereavement program to quality resources in the community.
The findings from the bereavement coordinators’ survey emphasize key challenges and opportunities in hospice bereavement care, particularly the need for uniform national standards, Medicare reimbursement, adequate staffing, and priority service offerings.
Finalized HUG Model, Advisory Guidelines & Core Principles
The final version of the HUG model, advisory guidelines and core principles were developed in addressing the lack of foundational guidance for hospice bereavement services with a humanistic lens. The development process was comprehensive and drew from the latest research, results from the bereavement coordinator survey and abiding by the current CMS regulations and standards of the National Hospice and Palliative Care Organization (NHPCO) for hospice bereavement services.
The core principles of Humanistically Universalizing Grief (HUG) conceptualize grief as a natural, universal human experience. These principles emphasize that grief is an adaptive, embodied, and deeply personal process that varies across individuals, cultures, and contexts, while also shaping identity, relationships, and meaning (Appendix A.) These principles are derived from a comprehensive review of the literature on the normalization of grief.
The 20 HUG foundational program guidelines were developed to provide hospice agencies with a standardizable set of foundational and minimum elements for bereavement care. Grounded in a humanistic understanding of grief as a normal and diverse experience, these guidelines aim to ensure consistent, accessible, and culturally responsive support across hospice programs in the United States (Appendix B.)
Finally, the HUG agency model operationalizes a humanistic approach to bereavement care by illustrating how individuals engage with a continuum of supportive services. Centered on four core service types based on practice patterns, the model also incorporates flexible, community-responsive offerings to ensure care remains accessible, individualized, and contextually relevant (Appendix C.)
Bridging Research Gaps
The HUG model, advisory guidelines and core principles address the longstanding absence of formalized standards in U.S. hospice bereavement programs. This study identified four critical research gaps now embedded within the HUG framework.
First, the web-based bereavement coordinator survey indicated strong endorsement of national hospice bereavement standards and Medicare reimbursement (80%), reinforcing the necessity of formalized guidelines, aligning with congressional efforts to define high-quality bereavement care (AHRQ, 2025). Second, the framework integrates a humanistic, non-pathologizing approach to grief, as survey responses indicated no reliance on medicalized grief models in program development. Third, the HUG bereavement program model incorporates core foundational services, mirroring previous survey results (Barry et al., 2012; Becker & Cagle, 2023; Demmer, 2003; Foliart et al., 2001) that identified condolence phone calls, grief groups, one-on-one grief support, and accessible resources as essential. Lastly, program evaluation remains a priority with over 90% of coordinators advocating for structured assessment to support funding and resource allocation. These elements establish a comprehensive, evidence-informed framework, offering a standardized yet adaptable model for hospice bereavement care.
Limitations
Several limitations should be considered when interpreting the findings of this exploratory quantitative study. First, the sample size was relatively small (n = 23); however, this was consistent with the exploratory aim of the study, which sought to generate preliminary insights into hospice bereavement programs rather than draw definitive or generalizable conclusions (Babbie, 2020). While the focused sample allowed for initial examination of key issues, including program variation, staffing, and service delivery, it may have limited the breadth of perspectives represented. In addition, most respondents were affiliated with hospice agencies serving more than 200 bereaved individuals annually, which may have contributed to the underrepresentation of smaller hospice bereavement programs and constrained the ability to capture variation across agency types. Furthermore, respondents were drawn from only 11 of California’s 58 counties, limiting the geographic diversity of the sample and potentially reducing the applicability of the findings to hospice agencies operating in rural, underserved, or differently resourced regions.
Implications for Further Research
The findings of this exploratory study underscore the need for future research with broader scope and increased methodological depth. Subsequent studies should aim to include larger and more diverse samples of hospice agencies across a wider range of counties and regions, both within California and nationally, to enhance representativeness and generalizability. Given the substantial variation observed in staffing levels, service delivery models, and program structures, future research should examine how these differences influence bereavement care quality, accessibility, and outcomes.
In addition, mixed-methods approaches or longitudinal designs may provide deeper insight into how bereavement programs evolve over time and how national standards or reimbursement mechanisms, if implemented, might affect practice. Furthermore, empirical evaluation of proposed frameworks and guidelines, including their feasibility, implementation, and effectiveness across diverse hospice contexts, is needed to inform evidence-based policy and program development. Lastly, while the guidelines informing this study are grounded in theory and experiential knowledge, further research is needed to evaluate their implementation, feasibility, and effectiveness in diverse hospice contexts.
Conclusion
This was the first study of its kind to survey hospice bereavement coordinators that focused on recommendations for national standards for hospice bereavement programs, with an emphasis on non-pathologizing grief approaches. It was the intent of this study to establish foundational data that can be used to develop national standards and regulations for hospice bereavement programs in the United States. Along with providing a rooted humanistic framework within hospice bereavement programs.
Supplemental Material
Supplemental Material - Humanistically Universalizing Grief (HUG): Advisory Guidelines for National Hospice Bereavement Programs Standards Within the United States
Supplemental Material for Humanistically Universalizing Grief (HUG): Advisory Guidelines for National Hospice Bereavement Programs Standards Within the United States by Jared Garcia, Lynn M. Raine, Larry Ortiz, Mary Akstin in OMEGA - Journal of Death and Dying
Footnotes
Acknowledgments
The authors thank the hospice bereavement coordinators who generously shared their time and expertise by participating in this study.
Ethical Considerations
This study was reviewed and approved by the Loma Linda University Institutional Review Board.
Consent to Participate
Informed consent was obtained electronically from all participants prior to participation in the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.