
Abstract
This study investigated death literacy within a United States (U.S.) community using the Death Literacy Index (DLI). Aims: (1) establish benchmark DLI and subscale scores, (2) examine demographic variability, end-of-life (EOL) experience, and spirituality, (3) assess psychometric properties of DLI. A cross-sectional survey using the DLI was conducted with a community convenience sample. The sample (n = 367) was 75% White, 70% female, with a mean age of 53 years. The overall DLI score was 4.87 (scaled 0–10), with the highest subscale score in Support Groups (6.04) and the lowest in Doing Hands-On Care (3.75). Higher scores are associated with older age, being widowed, Medicare, EOL experience, and spirituality. Factor analysis and confirmatory factor analysis via structural equation modeling supported the 6-factor model with good fit statistics. Strong internal consistency and subscale reliability confirmed the DLI as a reliable instrument for measuring death literacy in the U.S.
In a report by the Lancet Commission on the Value of Death, Sallnow et al. (2022) highlight the growing complexity surrounding death in contemporary society. Until the mid-twentieth century, responsibility for death care largely rested with families and faith communities (Sallnow et al., 2022). Advances in health technology have contributed to a societal emphasis on prolonging life, often at significant cost (Lofland, 2019). This increased medicalization of end-of-life (EOL) care has left the community with limited experience, knowledge, and skills in navigating EOL care in the current U.S. healthcare system. As a result, patients and families often react to treatment imperatives rather than proactively planning for a preferred EOL experience.
Addressing the challenges of EOL care is both significant and timely, particularly as the U.S. population ages and the financial burden of EOL care continues to rise. According to reports, Medicare costs incurred in the last year of life account for between 13% (Aldridge & Kelley, 2015) and 21% (Duncan et al., 2019) of expenses. For 2022, this translates to an estimated $123 billion to $198 billion (Center for Medicaid and Medicare Services, 2022). These figures raise concerns about the long-term sustainability of current EOL care models.
Two primary services support EOL care: hospice and palliative care. Hospice care, available in the U.S. since the 1970s, aims to provide a dignified death while minimizing suffering and unnecessary medical interventions. Despite its benefits, hospice remains underutilized, largely due to a misalignment between hospice regulations and the evolving clinical needs of individuals with chronic illness at the EOL (Fine, 2018). Palliative care teams have expanded in hospital settings, supporting patients and families in goals of care conversations and care navigation. Unfortunately, access to community-based palliative care remains inconsistent and is often inadequately reimbursed in the U.S. (Kamal et al., 2013). The role of health insurance is unique to the U.S. and bears exploration. Health insurance varies based on age, income, and employment status, perhaps impacting access to EOL care.
Researchers have increasingly explored public health approaches aimed at improving EOL care. Peeler et al. (2023) conducted a scoping review of public health palliative care interventions and found that community-based efforts can address residents’ practical needs, enhance individual knowledge and skills, and strengthen the overall community. EOL care needs are community-specific, depending on the local context, demographics, and social capital (Peeler et al., 2023). These findings suggest that proactive community engagement can foster the development of EOL care systems that are more effective, meaningful, and cost-efficient, while also addressing the current over-medicalization of the EOL experience.
Leonard et al. (2022) developed a Death Literacy Index (DLI) as a tool to measure community-level knowledge and skills related to EOL care and decision-making. Death literacy has been defined as a “set of knowledge and skills that make it possible to gain access to, understand, and act upon EOL and death care options” (Noonan et al., 2016, p. 32). Noonan and colleagues propose that this form of literacy is primarily acquired through personal and community-based experiences with death and dying.
The DLI has been adapted and validated across multiple international contexts, including Australia (Leonard et al., 2022), Turkey (Semerci et al., 2024), China (Che et al., 2023; Li et al., 2023), the United Kingdom (Graham-Wisener et al., 2022), and Sweden (Johansson et al., 2023). Across these studies, consistent factors associated with higher death literacy include older age, widowhood, religiosity, retirement status, strong social connections, and having children. Notably, all studies emphasize the critical role of direct experience with EOL care as a key determinant of higher death literacy.
Despite its international application, the DLI has not yet been used or evaluated in the U.S. This study seeks to address this gap by using the DLI within a U.S. community and contributing to the broader understanding of death literacy in the American context. The purpose of this study was to assess death literacy in a U.S. community using the DLI. Prior research has demonstrated that the DLI exhibits strong validity and reliability across diverse cultural settings (Che et al., 2023; Graham-Wisener et al., 2022; Johansson et al., 2025; Leonard et al., 2020; Semerci et al., 2024). The unique challenges related to healthcare access in the United States—particularly in the absence of a universal healthcare system—will be addressed.
The aims of this study were as follows: (1) To obtain benchmark DLI total and subscale scores for a U.S. community. (2) To examine variability in DLI scores across demographic characteristics, health insurance type, experience with death and EOL care, and religious/spiritual background. (3) To evaluate the psychometric properties of the DLI within a U.S. context.
Methods
This study employed a cross-sectional research design to collect data through an anonymous online survey. The survey was accessed via a Quick Response (QR) code, with paper versions available upon request. Participants were recruited from a diverse cross-section of the Santa Clarita Valley, a suburban community of Los Angeles County. The demographic characteristics of Santa Clarita include a population of 228,673, with a racial mix of 44% White, 34% Latino, 12% Asian, and 4% Black residents. Other features include a $123,001 median household income, 7.5% poverty rate, 64.8% employment, 41.8% Bachelor’s degree or higher, and 5.4% without health insurance (Survey Census Bureau and American Community, 2022).
Inclusion criteria required participants to be at least 18 years of age, have a primary residence in one of nine identified zip codes, and be able to read English. A convenience sampling approach was used, incorporating local advertising, community presentations (Senior Center, Churches, Chamber of Commerce), direct recruitment by the investigator, and snowball sampling techniques. Participation was voluntary, and completion of the anonymous survey implied informed consent. Data collection occurred over a nine-week period, from January 14 to March 17, 2025. Participants were offered the option to enter a gift card drawing as an incentive. To preserve anonymity, any identifying information was separated from survey responses immediately upon submission. Sampling targets were informed by local census data to set data collection goals concerning age, gender, and race to ensure a valid cross-section of the target community (Census Bureau and American Community Survey, 2022). A target sample size of 350 was determined to achieve a confidence level of 95% with a 5% margin of error.
Measures
The survey instrument consisted of three sections: (1) demographic and health insurance information, (2) questions related to end-of-life (EOL) experience and spirituality, and (3) the Death Literacy Index (DLI).
The demographic section included two open-ended questions (zip code and age) and seven multiple-choice questions covering gender, marital status, education level, race/ethnicity, income level, parental status, and health insurance coverage. The inclusion of the health insurance variable makes a unique contribution as prior research has primarily occurred in countries with national health programs (Che et al., 2023; Graham-Wisener et al., 2022; Johansson et al., 2023; Leonard et al., 2020; Semerci et al., 2024).
Five additional yes/no questions assessed participants’ experience with EOL care and spiritual characteristics. These included whether participants had experienced the death of a close friend or family member due to a prolonged illness, had professional or volunteer experience in EOL care, or had personally provided care for someone at the EOL. Previous studies have shown that experience with EOL care is linked to higher death literacy, demonstrating known group validity (Graham-Wisener et al., 2022; Johansson et al., 2023; Leonard et al., 2022). Additional items addressed the presence of a spiritual or religious background and current spiritual or religious practice. These variables have also been associated with higher death literacy (Graham-Wisener et al., 2022; Johansson et al., 2023; Leonard et al., 2022).
The 29-item Death Literacy Index (DLI) developed by Leonard et al. (2020) was used without modification. The DLI comprises four domains: Practical Knowledge, Experiential Knowledge, Factual Knowledge, and Community Knowledge. The Practical Knowledge domain includes two sections: Talking Support and Doing Hands-On Care. The Community Knowledge includes two sections: Accessing Help and Support Groups.
Responses were gathered using a five-point Likert scale, ranging from 1 (e.g., “not true of me,” “not able,” or “strongly disagree”) to 5 (e.g., “very true of me,” “very able,” or “strongly agree”). Thus, higher numerical scores indicate greater levels of death literacy. The instrument yields a total score (mean of all items) and subscale scores (mean of items in each domain). Prior studies have demonstrated strong internal consistency, with Cronbach’s alpha values ranging from 0.90 to 0.95 across different populations (Che et al., 2023; Johansson et al., 2023; Leonard et al., 2020; Semerci et al., 2024).
The final survey combined all sections into a 43-item instrument. According to Qualtrics, the estimated completion time ranged from six to eight minutes. The survey was designed with required responses to minimize missing data, and a “prefer not to answer” option was included for sensitive demographic questions.
Statistical Analysis
Survey data were exported from Qualtrics and analyzed using SPSS V30.0 (SPSS Inc., Chicago, IL). Descriptive statistics were used to summarize demographic characteristics and responses to the experience/spirituality questions.
DLI responses, originally measured on a 1–5 scale, were rescaled to a 0–10 scale to align with prior studies. The total DLI score was calculated as the mean of all 29 items, while subscale scores were computed as the mean of their respective items. Analysis of Variance (ANOVA) was conducted to examine differences in the DLI total and subscale scores across various demographic variables and experience/spirituality factors. Statistical significance was set at an alpha level of p < 0.05.
Age was categorized into groups consistent with the Census Bureau (18–24, 25–29, 30–39, 40–49, 50–59, 60–69, 70–79, 80+) (Census Bureau and American Community Survey, 2022). Health insurance responses, which allowed multiple selections, were reclassified into three categories: (1) low-income coverage, (2) Medicare, and (3) private insurance only (e.g., Preferred Provider Organization or Health Maintenance Organization plans).
Results
Sociodemographic Characteristics of Participants
Sociodemographic Characteristics of the Sample (n = 367)
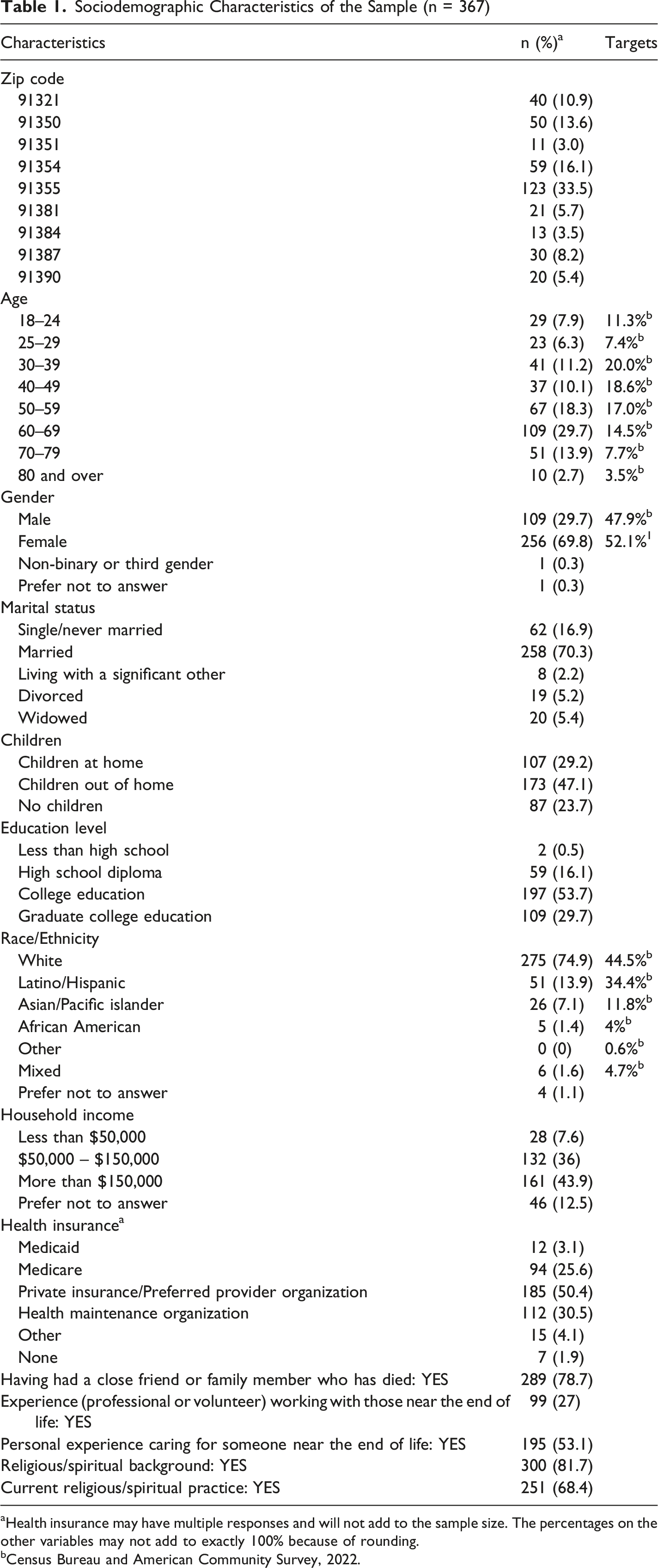
aHealth insurance may have multiple responses and will not add to the sample size. The percentages on the other variables may not add to exactly 100% because of rounding.
bCensus Bureau and American Community Survey, 2022.
Participants represented all nine targeted zip codes in the community of interest. The mean age was 53.4 years, with 65% of the participants aged of 50 or older. The sample was predominantly female (70%) and married (70%). A large portion of participants reported having a college or graduate degree (83%). Although multiple racial groups were represented, most participants identified as White (75%). Annual incomes exceeding $50,000 or over were reported by 80% of the sample. Health insurance coverage varied, with 50% reporting private insurance coverage.
With respect to EOL experience and spirituality, 79% of participants reported having experienced the death of a close friend or family member due to prolonged illness. Professional or volunteer experience in EOL care was reported by 27% of participants, while 53% indicated personal experience caring for someone at the EOL. Additionally, 82% of participants reported a spiritual background, and 68% indicated an active spiritual practice.
Aim 1 Analysis: Benchmark Death Literacy Index Scores
Mean Scores for the DLI and Subscales (Scaled 0-10)
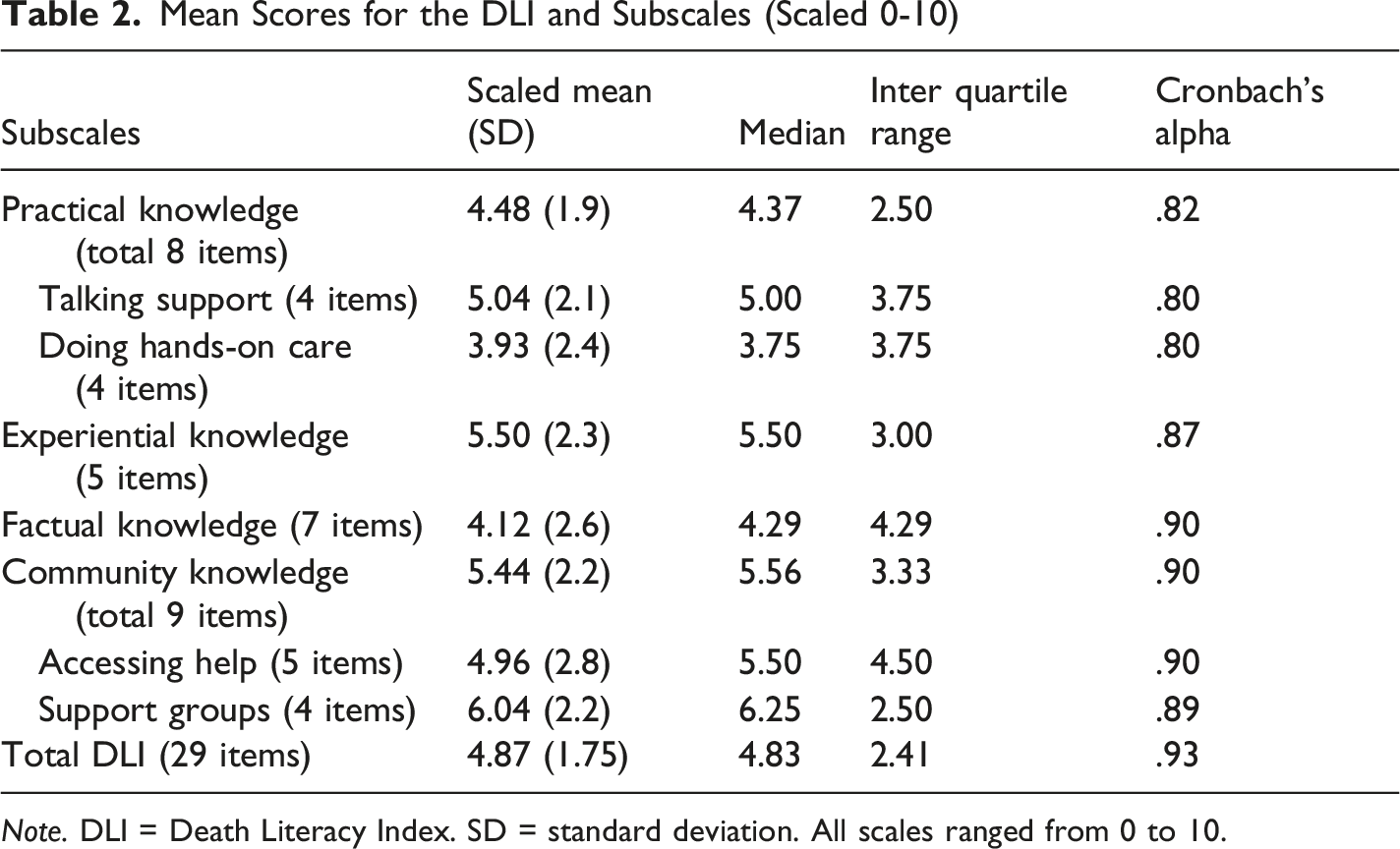
Note. DLI = Death Literacy Index. SD = standard deviation. All scales ranged from 0 to 10.
Among the subscales, the highest mean score was observed for the Support Groups subscale (mean = 6.04), which assesses awareness of available support resources for individuals who are dying, their caregivers, and those experiencing grief. The highest-scoring individual item reflected awareness of grief support groups (mean = 7.00).
Other relatively high-scoring individual items included the ability to talk to a doctor about support at home for a dying person (mean = 6.12). Upon further analysis, higher scores on this item were significantly associated with being White (p = .004) and having a higher level of education p = .002). Another individual item associated with high death literacy was the experience of grief or loss, which led individuals to re-evaluate what is important (mean = 6.32). Further analysis revealed that higher scores were associated with those reporting a spiritual background (p = .002). In addition, the ability to access emotional support had one of the highest mean scores (mean = 6.05). This higher score was associated with reporting a spiritual background (p = .003) and reporting a current spiritual practice (p = .009).
In contrast, the lowest mean score was observed in the Doing Hands-On Care subscale (mean = 3.93). Items within this subscale assess ease or difficulty with practical care giving skills, such as feeding, bathing, or lifting a person. The lowest-scoring individual item was reporting difficulty bathing a person (mean = 3.02), followed by lifting a person (mean = 3.47). Additional low-scoring items included knowing the law about dying at home (mean = 3.57), access to palliative care (mean = 3.62), ability to navigate the healthcare system (mean = 3.72), and talking about grief with a child (mean = 3.92).
International Death Literacy Index Scaled Mean Score Comparisons
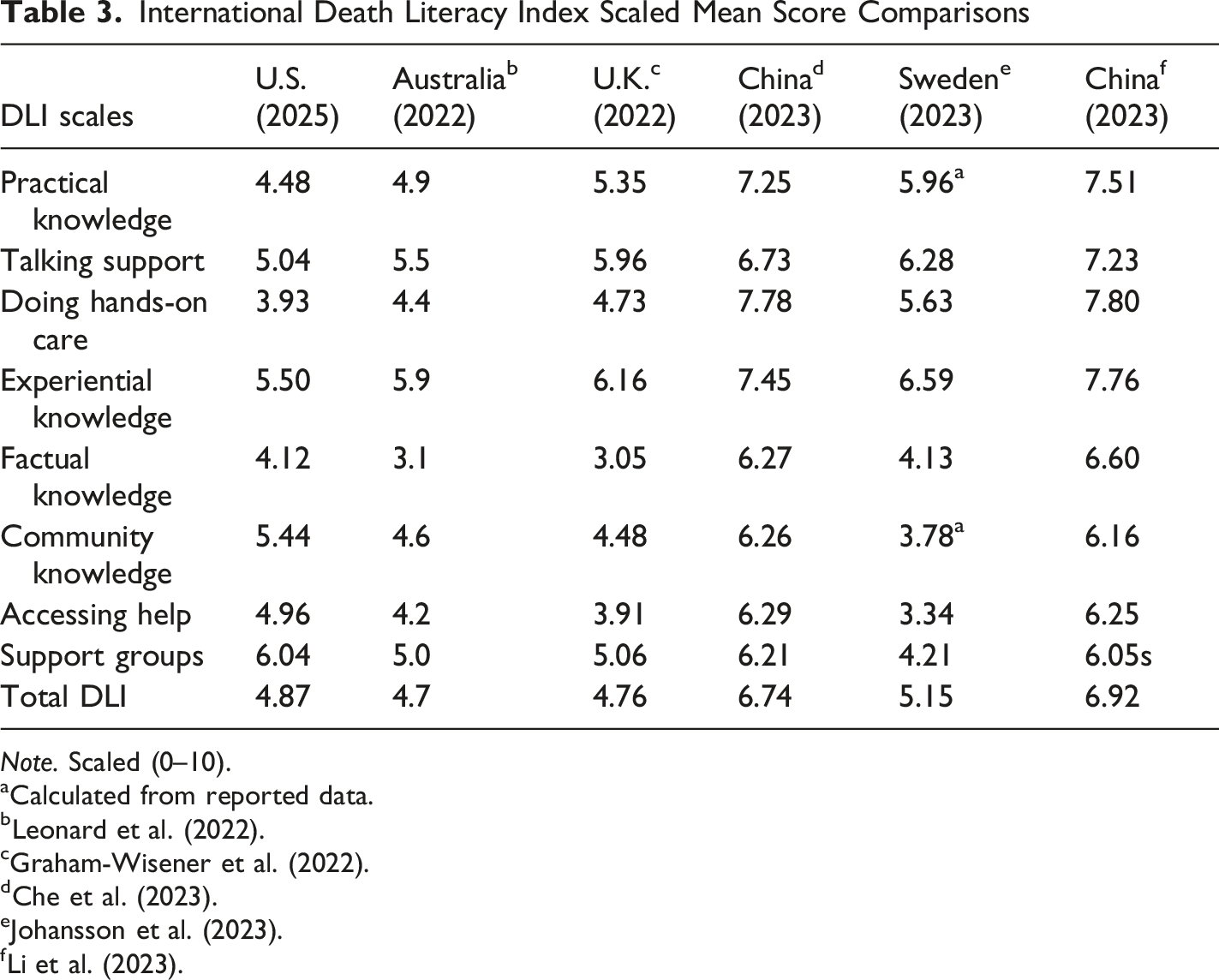
Note. Scaled (0–10).
aCalculated from reported data.
Aim 2: Variation in Death Literacy by Demographic, Experiential, and Spiritual Factors
Significant ANOVA Results by Demographics, Experience, and Spirituality
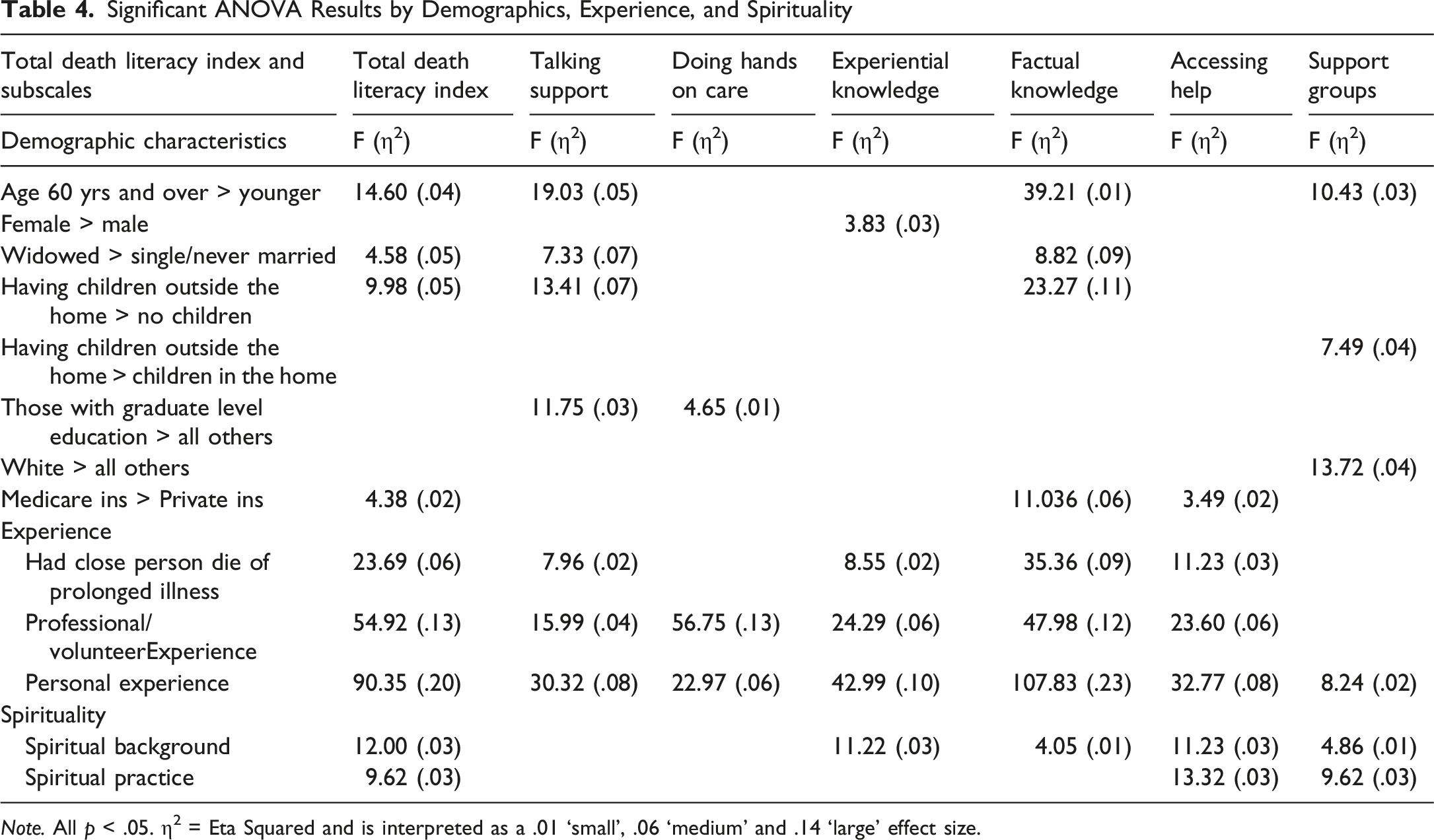
Note. All p < .05. η2 = Eta Squared and is interpreted as a .01 ‘small’, .06 ‘medium’ and .14 ‘large’ effect size.
No significant differences in DLI scores were observed across zip codes. Gender differences were limited, with women scoring significantly higher than men on the Experiential Knowledge subscale, but not on the total DLI score or other subscales. However, age was significantly associated with death literacy. Participants aged 60 years and older demonstrated higher total DLI scores and higher scores in several subscales, including Talking Support, Factual Knowledge, and Support Groups, compared to participants under age 60.
Marital status was also associated with death literacy. Widowed participants had significantly higher total DLI scores, as well as higher scores in the Talking Support and Factual Knowledge subscales, compared to participants who were single or never married. Similarly, participants with children living outside the home demonstrated higher total DLI scores and higher scores in multiple subscales compared to those without children or with children living at home.
Educational attainment was associated with higher death literacy, particularly among participants with graduate-level education, who scored significantly higher in the Talking Support and Doing Hands-On Care subscales.
When race/ethnicity was analyzed as a dichotomous variable (White vs. all other groups), White participants demonstrated significantly higher scores in the Support Groups subscale. No significant differences were observed in total DLI scores or other subscales.
Income level was not significantly associated with DLI scores. However, health insurance status revealed meaningful differences. Participants with Medicare coverage (government insurance for those ≥65 years and/or disabled) scored significantly higher than those with private insurance on the total DLI score, as well as on the Factual Knowledge and Accessing Help subscales.
End-of-Life Experience and Spiritual Factors
Experience with EOL care emerged as a strong predictor of death literacy. Participants who reported having experienced the death of a close friend or family member, professional or volunteer involvement in EOL care, or personal caregiving experience all demonstrated significantly higher DLI scores compared to those without such experiences. The strongest effect was observed among participants with personal caregiving experience.
Spirituality was also associated with higher death literacy. Participants who reported a spiritual background or a current spiritual practice demonstrated significantly higher total DLI scores compared to those who did not. These differences were particularly evident in the Accessing Help and Support Groups subscales, although effect sizes were modest.
DLI Reliability and Validity
The DLI demonstrated strong reliability and validity within this U.S. sample. Internal consistency was high, with a Cronbach’s alpha of 0.93 for the total scale and acceptable reliability across subscales.
Construct validity was supported by the normal distribution of scores and the absence of floor or ceiling effects. Known-group validity was confirmed, as participants with EOL experience consistently scored higher than those without such experience.
Structural validity was assessed via factor analysis using a principal components analysis with varimax rotation. A six-factor model converged in seven iterations with good fit statistics: x2/df = 2.54, p < .001, RMSEA = .065, CFI = .091, TLI = .899. Structural equation modeling using maximum likelihood estimation was used to assess the fit of the model shown in the path diagram for the model (Figure 1). Structural equation modeling for the six-factor model (Leonard et al., 2022)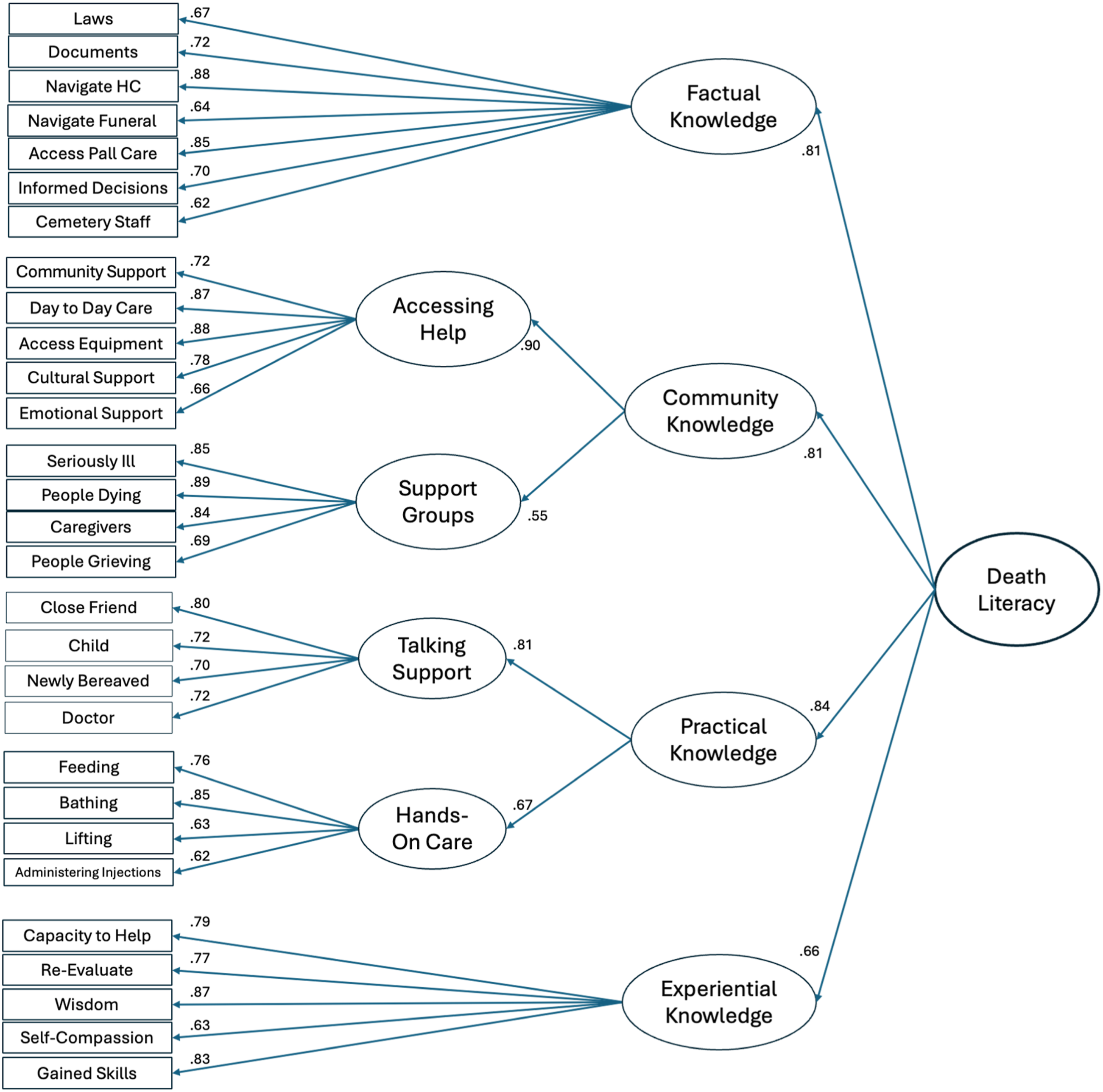
Discussion
The findings of this study provide important insights into death literacy within a suburban U.S. community. Consistent with prior international research, overall DLI scores demonstrated relatively limited variation across many demographic variables, including gender, race, education, and income. However, meaningful differences emerged within specific subscales and population subgroups, highlighting important nuances in how death literacy is distributed.
Participants aged 60 years and older, widowed individuals, those with children living outside the home, and individuals enrolled in Medicare exhibited significantly higher total DLI scores. A common characteristic among these groups is older age and increased exposure to EOL care. These groups also demonstrated higher scores in the Factual Knowledge and Talking Support subscales, suggesting strengths in both understanding EOL processes and communicating about them.
At the subscale level, Support Groups emerged as a relative strength within the community, with the highest mean score among all domains. Awareness of grief support groups was notably high; however, knowledge of caregiver-specific support groups was comparatively lower, which is concerning given the well-documented burden experienced by caregivers. The sample scored high in accessing emotional support for themselves, which may not necessarily come from caregiver support groups.
Spirituality appeared to play a meaningful role in death literacy, particularly in accessing emotional support and interpreting experiences of grief and loss. Participants with a spiritual background or current spiritual practice demonstrated higher scores in relevant subscales, suggesting that faith-based communities may serve as important sources of support and knowledge. These findings underscore the importance of considering spirituality in efforts to improve death literacy at the community level.
Being comfortable speaking with a doctor about support at home for EOL care received a notably high score across the entire sample. This finding is encouraging, suggesting that community members are willing to talk about EOL care with their physicians. However, further analysis revealed some disparities based on race and educational levels. This finding highlights areas for advocacy and the importance of raising community death literacy, as this demographic may not seek information from the primary doctor, relying on personal support systems.
Despite these strengths, notable gaps were identified. The lowest scores were observed in the Doing Hands-On Care subscale, indicating limited confidence in performing practical caregiving tasks such as bathing, lifting, and administering care. These findings suggest that a lack of hands-on caregiving skills may represent a significant barrier to providing EOL care in the home setting. Given that hospice care in the United States often relies on family members to provide direct care, targeted education and training in these skills may be beneficial. The community Last Aid curriculum might be an avenue of intervention (Mills et al., 2020).
Similarly, relatively low scores in the Factual Knowledge subscale highlight gaps in understanding key aspects of EOL care, including legal considerations, access to palliative care, and navigation of the healthcare system. Knowing the law regarding dying at home had the lowest score within this subscale, a finding that aligns with other studies (Johansson et al., 2023). In the U.S., most palliative care is provided in hospital settings, while community-based palliative care remains inconsistent and poorly reimbursed, possibly contributing to the low score for knowing how to access palliative care. These findings likely reflect the complexity and fragmentation of the U.S. healthcare system, where access to services is often inconsistent and difficult to navigate.
Experience with EOL care emerged as the most significant predictor of death literacy. Participants with personal caregiving experience demonstrated the highest levels of death literacy across nearly all subscales, with particularly strong effects observed in total DLI scores, Factual Knowledge, and Experiential Knowledge. Consistent with previous studies, EOL experience stands out as the most crucial characteristic associated with death literacy (Graham-Wisener et al., 2022; Johansson et al., 2023; Leonard et al., 2020, 2022; Li et al., 2023). These findings reinforce the importance of experiential learning in developing death literacy.
Professional and volunteer experience also contributed to higher scores, although to a lesser extent in certain domains. This group had no significant difference from the rest of the sample in the Support Groups subscale. Although significant, they also demonstrated only small effect sizes in the Talking Support and Community Knowledge subscales. These findings indicate potential areas for professional development.
The inclusion of health insurance as a variable provided additional insight into structural influences on death literacy. Participants with Medicare coverage demonstrated higher DLI scores than those with private insurance, particularly in areas related to factual knowledge and access to care. This may reflect increased interaction with healthcare systems among older adults, as well as greater exposure to EOL-related services. Further examination of this finding is indicated.
Limitations
Several limitations should be considered when interpreting these findings. The study was conducted within a suburban community in Los Angeles County, which may limit generalizability to other regions with different demographic or healthcare characteristics.
Data collection occurred during a period of significant external events, including regional wildfire activity and changes in federal immigration policy. These events may have influenced participation rates, particularly among certain demographic groups. Notably, the sample underrepresented Latino participants relative to the community population.
The sample was also skewed toward older, female, and highly educated individuals, which may have influenced the overall DLI scores. Recruitment strategies that involved engagement with faith communities may have contributed to the high proportion of participants reporting spiritual backgrounds and practices.
Additionally, the survey was administered in English and required literacy, thereby excluding non-English-speaking individuals and those with limited reading ability. These factors should be considered when interpreting and generalizing the results.
Despite these limitations, the study has several strengths, including a relatively large sample size, complete data collection with no missing responses, and the introduction of health insurance as a novel variable relevant to the U.S. context. Importantly, this study represents the first application of the DLI within the United States, providing valuable benchmark data for future research.
Conclusion
This study identified key factors associated with higher death literacy in a U.S. community, with experience in end-of-life care emerging as the most significant predictor. While the community demonstrated strengths in awareness of support resources and access to emotional support, important gaps were identified in practical caregiving skills and factual knowledge related to EOL care. The findings highlight the need for targeted interventions aimed at improving hands-on caregiving skills, increasing knowledge of EOL care options, and enhancing navigation of the healthcare system. Community-based education programs and professional training initiatives may be effective strategies for addressing these gaps. The death literacy strengths in this community point towards avenues of harnessing EOL experience and support to care for others, prompting a grass-roots approach to improving care.
By applying the DLI in a U.S. context, this study contributes to the growing body of knowledge on death literacy and provides a foundation for future research. Continued investigation is needed to better understand variations in death literacy across different populations and to identify effective approaches for strengthening community capacity to support end-of-life care. Ultimately, improving death literacy has the potential to enhance the quality, accessibility, and person-centered EOL care in the United States.
Footnotes
Ethical Considerations
Ethical approval was obtained from the University of California, Los Angeles Office of Human Research Protection Institutional Review Board (IRB), including a waiver of signed consent. Voluntary completion of the anonymous survey implied consent.
Author Contributions
K. Nelson: Conceptualization, Methodology, Formal Analysis, Writing-Original Draft. E. Brauer: Methodology, Review and Editing, Final Approval. ML. Brecht: Methodology, Analysis and Interpretation, Review and Editing, Final Approval. E. Economou: Methodology, Review and Editing, Final Approval. B. Bates-Jensen: Conceptualization, Methodology, Analysis and Interpretation, Review and Editing, Supervision, Final Approval.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.