
Abstract
Both hand and finger sensory perception and motor abilities are essential for the development of skilled gestures and efficient bimanual coordination. While finger dexterity and finger sensory perception can be impaired in children with cerebral palsy (CP), the relationship between these two functions in this population is not clearly established. The common assumption that CP children with better sensory function also demonstrate better motor outcomes has been recently challenged. To study these questions further, we assessed both finger dexterity and finger gnosia, the ability to perceive one’s own fingers by touch, in groups of 11 children with unilateral (i.e., hemiplegic CP) and 11 children with bilateral spastic CP (i.e., diplegic CP) and compared them with typical children. In our sample, children with hemiplegia exhibited finger dexterity deficit in both hands and finger gnosia deficit only in their paretic hand. In contrast, children with diplegia exhibited finger gnosia deficits in both hands and finger dexterity deficit only in their dominant hand. Thus, our results indicated that children with spastic hemiplegia and diplegia present different sensory and motor profiles and suggest that these two subgroups of CP should be considered separately in future experimental and clinical research. We discuss the implications of our results for rehabilitation.
Introduction
Cerebral palsy (CP) is classically defined as a disorder of posture and movement caused by early lesions in the developing brain (Rosenbaum et al., 2007). It is the most prevalent childhood physical disability, affecting 2–3 per 1,000 live births (see Surveillance of Cerebral Palsy in Europe, 2002 for a survey in Europe and Van Naarden-Braun et al., 2016 for statistics in the United States). In the vast majority of individuals suffering from unilateral or bilateral CP, impairment is evident in both fine motor ability, also labeled dexterity, and sensory functioning, including tactile discrimination, (Auld, Boyd, Moseley, Ware, & Johnston, 2012), proprioception, and stereognosis (Arnould, Penta, & Thonnard, 2007). These various forms of sensory deficits have been less extensively studied than motor impairments in previous CP research (Forssberg, 2014; Gordon, Bleyenheuft, & Steenbergen, 2013; Majnemer, Bourbonnais, & Frak, 2008); and this is regrettable as both intact sensory perception and motor capacities are essential for the development and production of skilled motor gestures (Augurelle, Smith, Lejeune, & Thonnard, 2003; Eliasson & Burtner, 2008; Flanagan, Bowman, & Johansson, 2006) and bimanual coordination (Gordon, Charles, & Steenbergen, 2006). An improved understanding of the interrelationship between tactile sensory perception and dexterity in children affected by CP is important. This study sought to gain further knowledge and understanding in this area by determining the degree to which fine motor impairments are associated with sensory deficits in children with CP.
Although it is commonly assumed that children with CP who show better sensory function also show better motor outcomes (e.g., Majnemer et al., 2008; Tachdjian & Minear, 1958), Bleyenheuft and Gordon (2013) have recently challenged this assumption, noting as evidence, the conflicting results of several previous studies of correlations between these skills among children with CP. While a relationship has clearly been established between stereognosis and motor function in the case of unilateral cerebral palsy (e.g., Arnould et al., 2007; Auld et al., 2012; Krumlinde-Sundholm & Eliasson, 2002), inconsistent results have been reported for such other commonly assessed sensory modalities as tactile perception (i.e., light touch), tactile discrimination and proprioception (e.g., Arnould et al., 2007; Auld et al., 2012; Bleyenheuft & Thonnard, 2011; Krumlinde-Sundholm & Eliasson, 2002). One explanation of these inconsistencies may be that, both in children with CP and in normally developing children, the correlation usually found between fine motor and sensory measures varies with other variables, including the children’s age (Bleyenheuft, Wilmotte, & Thonnard, 2010; Richards & Persinger, 2004) or, perhaps, a third factor such as the child’s general level of cognitive or maturational development. Bleyenheuft and Gordon concluded that the presumed strong relationship between sensory and motor abilities in this population may be overstated. If this is the case, impairment in these two sets of skills may be independent.
In this study, we examined two separate groups of school-age children with CP—namely diplegic CP and hemiplegic CP. Hemiplegic CP, also called unilateral CP, is the predominant form of CP, and it is characterized by elevated muscle tone (spasticity) on one side of the body, usually most affecting the arm. In contrast, diplegic CP is characterized by increased muscle tone in both legs and, to a lesser extent, in the upper limbs. While these two subgroups of children with CP are often studied jointly (e.g., Arnould, Bleyenheuft, & Thonnard, 2014; Asano & Morioka, 2018; Majnemer et al., 2008), their distinct patterns of motor deficits (Beckung & Hagberg, 2002) and neuropsychological profiles (Bottcher, 2010) suggest, in accordance with Bleyenheuft and Gordon (2013), that more attention should be paid to their potential differences. A unilateral brain lesion in hemiplegic CP, most commonly caused by a periventricular venous infarction or a perinatal arterial ischemic stroke, usually affects both ascending sensory and descending motor pathways (Staudt, 2010), whereas brain lesions in spastic diplegic CP are usually located along the periventricular white matter and lead to direct bilateral involvement of lower limb corticospinal tracts with frequently associated disrupted sensory tracts (Hoon et al., 2009). For both groups of children, we assessed sensory functions through finger sense or finger gnosia, which involves both tactile perception and mental representation of finger position. In view of recent research emphasizing the importance of body representation in CP (Fontes, Cruz, Souto, Moura, & Haase, 2017), assessing sensory abilities through finger gnosia seemed particularly meaningful, because it constitutes a higher level cognitive sensory test than do more basic tactile tasks. Concerning finger dexterity assessment, we used the classic Nine-hole Peg Test (Smith, Hong, & Presson, 2000). As mentioned earlier, our main purpose was to determine whether finger dexterity and finger sense could be dissociated in children with the two main forms of CP. Based on previous literature, we predicted that children with hemiplegia would suffer from both dexterity impairment because of their motor deficits and sensory dysfunction of their paretic hand (e.g., Arnould et al., 2007; Bleyenheuft & Thonnard, 2011; Thevenot et al., 2014; Wingert, Burton, Sinclair, Brunstrom, & Damiano, 2008). As for their nonparetic hand, we expected dexterity impairments (Duque et al., 2003) but preserved finger sensitivity (Fontes et al., 2017; Thevenot et al., 2014). Among children with diplegia, we expected their dexterity to be less affected than gross motor functions (Carnahan, Arner, & Hägglund, 2007), but there are reports of slight finger dexterity impairment in their nondominant hands (Arner, Eliasson, Nicklasson, Sommerstein, & Hägglund, 2008; Arnould et al., 2007). As for sensitivity, Wingert et al. (2008) found that children with diplegia present impairments in both hands with greater nondominant hand deficits. To sum up, we predicted that children with hemiplegia would suffer from both sensory and dexterity impairments in their paretic hand but only from dexterity deficits in their nonparetic hand. 1 We predicted that children with diplegia would show both dexterity and sensory impairments, but we made no precise predictions for which hand, as prior literature provides too little guidance in that regard.
Method
Participants
Children’s Mean Ages and Scores on the General Cognitive Tests.
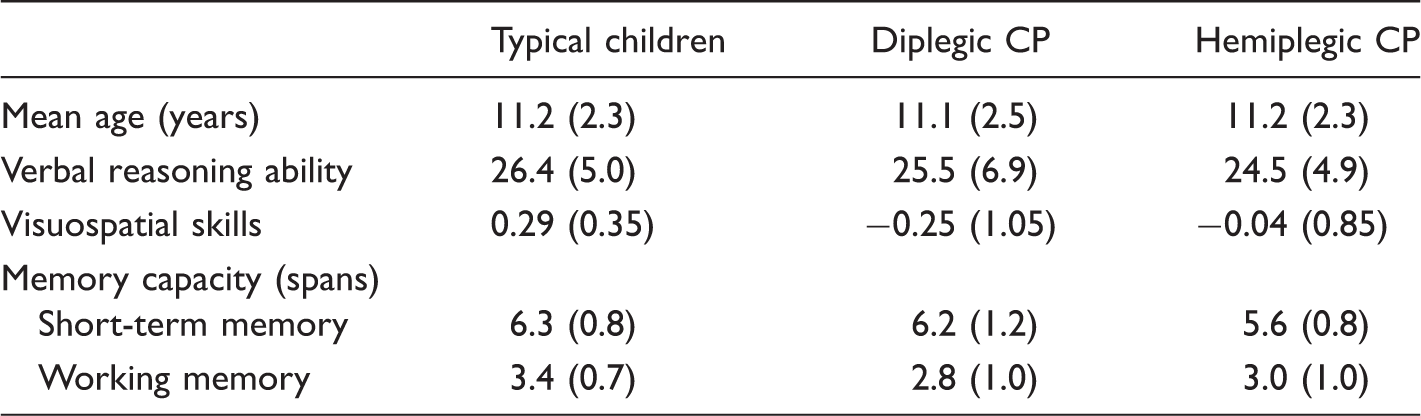
Note. Verbal reasoning abilities were measured with the subtest Similarity of the WISC-IV and we obtained raw scores out of 46. Visuospatial skills were measured with a test in which participants had to match a target picture with a similar picture and Z scores were calculated by combining participants’ accuracy and response time deviations from the mean of the whole population. Memory capacity was measured with a digit span forward (i.e., short-term memory) and a digit span backward (i.e., working memory) and the span corresponded to the maximum of digit recalled in a series. Standard deviations are in brackets. CP = cerebral palsy.
We recruited children with CP from an outpatient pediatric neuro-orthopedic clinic and from a motor and educational home-care service; they were classified from Level I (only impairments in speed, balance, and coordination) to III (use of handheld mobility indoors and wheeled mobility for long distance outdoors) on the Gross Motor Function Classification System (GMFCS; Palisano et al., 1997). All children were able to perceive light touch with no difficulties and were following a normal school curriculum. For all participants, we obtained informed consents from the children’s parents before testing; the study was approved by the local Ethics Committee. Each child was also asked whether they wanted to take part in the study and was free to discontinue participation at any time. We assured children and their parents of the children’s anonymity and confidentiality.
Instruments and Procedure
General cognitive skills
Verbal reasoning abilities were measured with the Similarities subtest of the Wechsler (2003) intelligence scale for children—Fourth Edition (WISC-IV). For short-term and working memory capacity assessments, we used the forward and backward spans of the Digit Span subtest of the WISC-IV, respectively. Finally, to assess visuospatial skills, we designed a task using the DMDX software (Forster & Forster, 2003) in which children had to match a target picture with an identical picture from among four choices.
Finger dexterity
Finger dexterity was assessed (always with the dominant hand first) with the Nine-hole Peg Test in which children must place nine pegs in nine holes onto a pegboard as quickly as possible (Smith et al., 2000). The experimenter recorded execution times with a stopwatch, and asked children to stop the task after 120 seconds. After this limit, a penalty of 10 seconds was assigned for each unplaced peg. Total time to complete the task, including penalties, constituted the score for this task, used for all subsequent data analyses.
Finger sense
Finger sense was assessed using a finger gnosia test in which children must identify which of their fingertips was touched by the experimenter. In our adaptation of the test, children wore fingerless gloves with different colors on the three central fingers of each glove. This adaptation allowed children to answer verbally by color naming, eliminating a confounding traditional requirement for a motor pointing response or the need for children to have any finger naming vocabulary. Children were asked to place their hands palm down through a lateral aperture of a covered box to prevent them from being able to visualize their fingers being touched. The cover of the box was rapidly opened after touching to enable children to see and name the color(s) corresponding to the touched finger(s). The experimenter touched either one finger in isolation or two fingers simultaneously or sequentially. To avoid anchoring effects, we tested only the three central fingers, which are known to be less sensitive than the outside digits (Gerstmann, 1940; Reeve & Humberstone, 2011). The child’s dominant hand was always assessed first. The percentage of correct responses for each hand was used as the score on this task for all subsequent data analyses.
Results
Participants’ Execution Times (in Seconds) in the Finger Dexterity Test and Scores in the Finger Sense Task as Well as Results of ANOVAs.
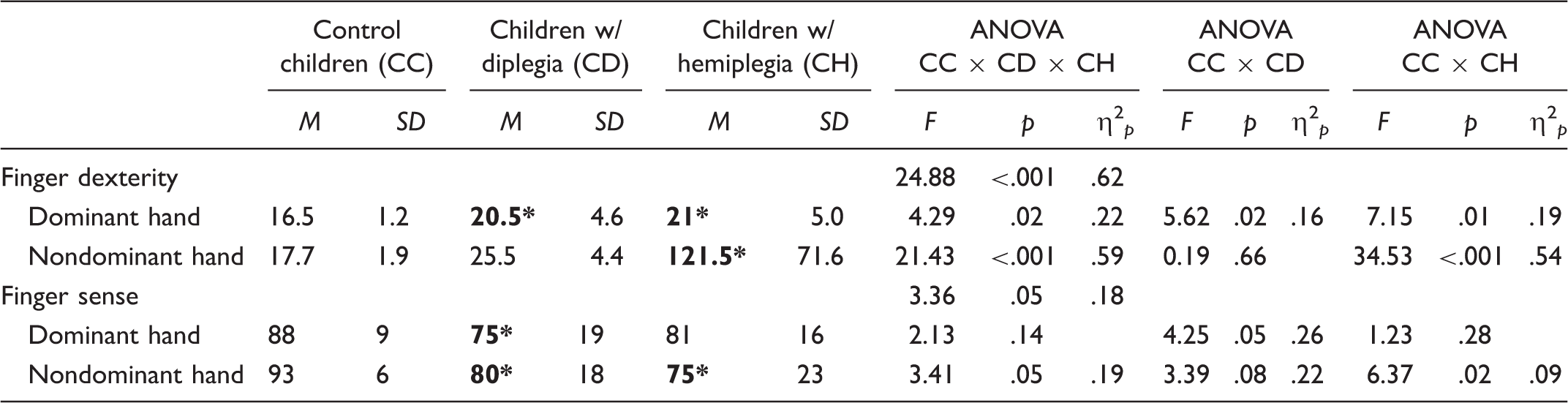
Note. ANOVA = analysis of variance; M = mean; SD = standard deviation; F = F statistic of ANOVA; p = level of significance; η2 p = partial eta squared (only provided for significant p values). Values in boldface reflect impaired performance in children with CP compared with control children (i.e., significant differences between CC and CD or CH).
Finger Dexterity
The ANOVA showed that the main effect for Group was significant, F(2, 30) = 24.88, p < .001, η2
p
= .62. Planned comparisons revealed a significant difference in execution times on the Nine-hole Peg Test between HG (70.1 seconds) and CG (17.1 seconds), F(1, 30) = 41.33, p < .001, η2
p
= .58. However, DG were not significantly slower (23 seconds) than CG. There was also a main effect for Hand, F(1, 30) = 21.95, p < .001, η2
p
= .42, with quicker execution times when the dominant hand was used (19.3 seconds) compared with the nondominant hand (54.9 seconds). We also found a significant interaction between Hand and Group, F(2, 30) = 18.30, p < .001, η2
p
= .55. Planned comparisons showed that HG differed from CG in both dominant and nondominant hand use—16.5 versus 21 seconds for the dominant hand, F(1, 30) = 7.15, p = .01, η2
p
= .19 and 17.7 versus 121.5 seconds for the nondominant hand, F(1, 30) = 34.53, p < .001, η2
p
= .54, for CG and HG, respectively. In contrast, DG differed from CG only for the dominant hand (20.5 seconds), F(1, 30) = 5.62, p = .02, η2
p
= .16 (see Figure 1a) but not for the nondominant hand (25.5 seconds), F(1, 30) = 0.19, p = .66 (see Figure 1b).
Box plot showing mean execution times in the Nine-hole Peg Test on the dominant hand (a) and nondominant hand (b) and mean percentages of correct answers in the Finger Gnosia Test on the dominant hand (c) and nondominant hand (d). Values are median (central thick lines), 25%, and 75% quartile ranges around the median (box height), and upper and lower limits (whiskers). *p < .05. **p < .01. ***p < .001. CP = cerebral palsy.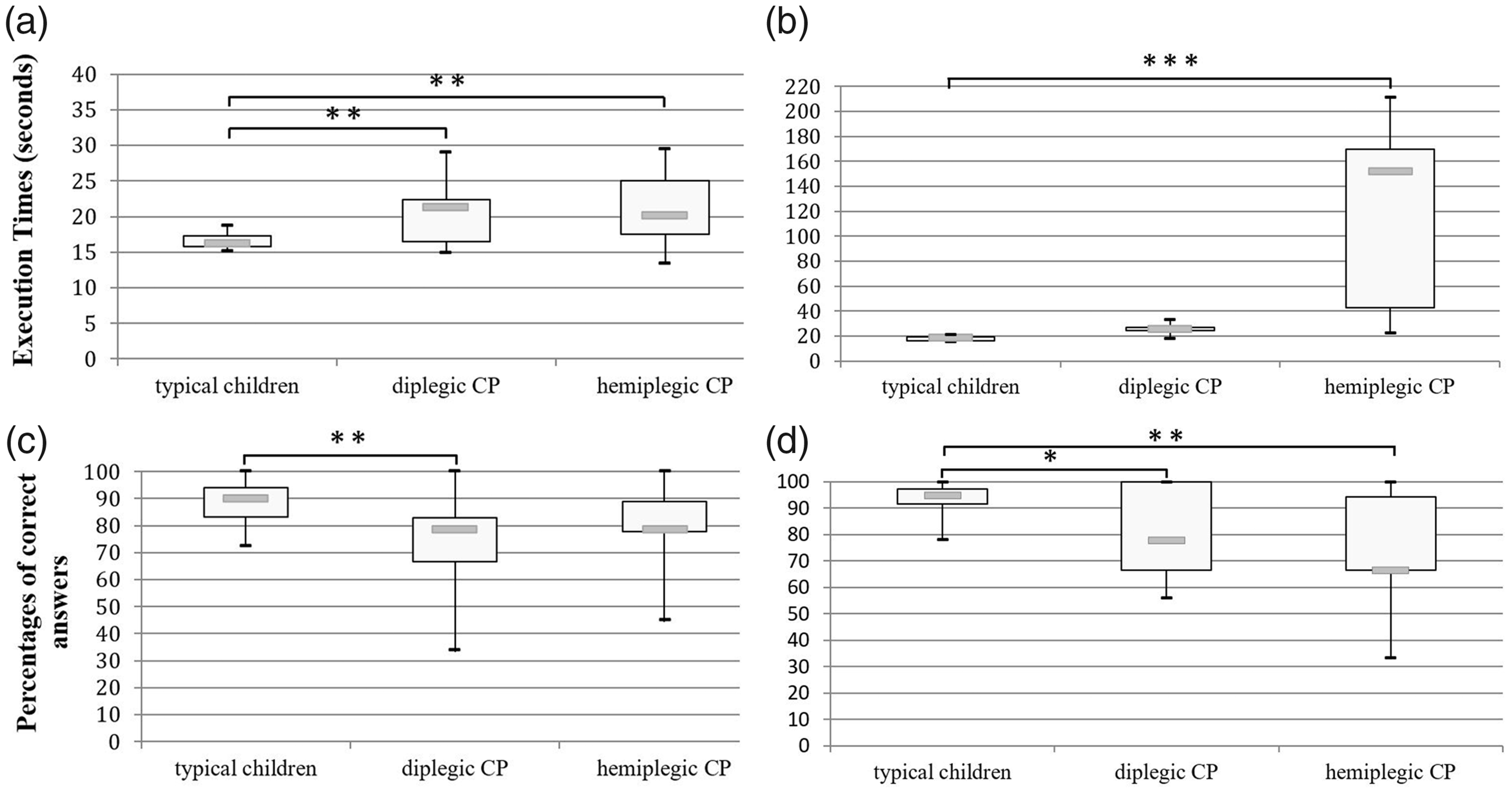
Finger Sense or Finger Gnosia
Again the ANOVA revealed a statistically significant main effect of Group, F(2, 30) = 3.36, p = .05, η2 p = .18. Planned comparisons revealed that CG were more accurate in the finger gnosia task (91%) than both DG (77%), F(1, 30) = 5.23, p = .03, η2 p = .15, and HG (78%), F(1, 30) = 4.84, p = .04, η2 p = .14. For this measure, we found no significant main effect of Hand, F(1, 30) = 0.26, p = .62, and there was no significant interaction between Group and Hand, F(2, 30) = 1.60, p = .22. Nevertheless, and because we predicted that only the nondominant hand (i.e., paretic hand) should suffer from finger sense deficit in HG, we performed a series of planned comparisons on the data. We found, consistent with our prediction, that HG were less accurate than control children only when using the nondominant hand (i.e., paretic hand; 75% vs. 93%), F(1, 30) = 6.37, p = .02, η2 p = .09, whereas there was no difference between the two groups of children for the dominant hand (i.e., nonparetic), (81% vs. 88%), F(1, 30) = 1.23, p = .28. In contrast, finger gnosia was impaired for both hands in DG (75% and 80% for the dominant and the nondominant hand) relative to CG, F(1, 30) = 4.25, p = .05, η2 p = .26, and F(1, 30) = 3.39, p = .08, η2 p = .22 for the dominant and the nondominant hand, respectively (see Table 1 and Figure 1c and 1d).
Discussion
In this research, our main purpose was to determine whether finger dexterity and finger sense could be dissociated in children with the two main forms of CP, namely hemiplegic and diplegic CP. In accordance with our predictions (Filho, Souza, Nunes, Braga, & Dellatolas, 2005; Fontes et al., 2017), our results showed that children with hemiplegia presented dexterity impairment in both hands but finger sense deficit was evident only in their paretic hand. A different pattern emerged for children with diplegic CP who presented finger sense deficits for both hands but finger dexterity impairment was evident only in their dominant hand, when compared with typically developing children.
Therefore, we observed a double dissociation between finger sense and finger dexterity. Finger gnosia can be intact among these children even when dexterity is impaired, and inversely, finger dexterity can be intact when finger gnosia is impaired. These results support Bleyenheuft and Gordon’s (2013) conclusion, challenging the common assumption that children with CP who show good sensory function are apt to show good motor outcomes. As these authors suggested, the children’s age had not been systematically covaried in previous studies, leading to an incorrectly assumed correspondence between finger sensory skills and finger dexterity among children with CP.
Our observation of a dissociation between finger sense and dexterity is relevant clinically because it has been well documented that sensorimotor integration is related to precision grip and grasping (Bleyenheuft & Gordon, 2013, 2014; Gordon et al., 2006, 2013). Consequently, if sensory or dexterity functioning of either hand is impaired in children with CP, difficulties in gripping and gesture execution can be expected. Thus, these results may encourage therapists to more systematically assess sensory deficits in these children, including finger sense, and to train sensory perception during interventions (Walmsley et al., 2018). As indicated by the bilateral finger gnosia deficit in children with diplegic CP, our results also make clear that this kind of assessment should not be limited to those children with CP who have obvious upper limb sensorimotor deficits. More generally and in order to get a full and realistic picture of these children’s abilities, comprehensive neuropsychological testing ought to go beyond classical psychometric cognitive measures to include dexterity and somatosensory assessment.
In addition to unimanual intensive practice, our results also support the idea that bimanual training, classically used in children with hemiplegic CP (Gordon et al., 2008; Gordon, Schneider, Chinnan, & Charles, 2007) can also be useful for children with diplegic CP (Saussez, Van Laethem, & Bleyenheuft, 2018). Because of interhemispheric influences, children have not only the ability to transfer motor programs from the less affected to the more affected hand (Gordon et al., 2006), but might also be able to improve their sensory abilities. As for children with hemiplegic CP, these results suggest that neurorehabilitation programs might capitalize on preserved abilities concerning finger sensitivity of their nonparetic “spared” hand. Indeed, children with better sensory abilities have been shown to exhibit larger functional gains after short-term motor training than children with less developed sensory abilities (Robert, Guberek, Sveistrup, & Levin, 2013). Intensive motor training of the nonparetic hand is, therefore, likely to be very efficient; and bimanual training could be envisioned after satisfactory improvement of the nonparetic hand motor functions. Such remediation programs focusing on the “healthy side” could be especially important because preserved dexterity of the nonparetic hand in school-aged unilateral CP children is related to their cognitive performance (Thébault et al., 2018).
By way of study limitations, before firmer conclusions and more precise and concrete remediation programs can be conceived and tested based on these preliminary results, it is important to note that finger gnosia relies on complex and specific brain pathways within the parietal lobes, meaning that finger gnosia might not be strictly identical to other cortical sensory abilities such as stereognosis, graphaesthesia, or two-point discriminations. Therefore, it will be important for future research to determine whether our results are generalizable to these additional aspects of finger sensitivity. Second, our clinical samples were small in number and of limited type, further affecting generalizability. Replications with larger and more diverse samples are needed. While the purpose of this article was not to explain the anatomical basis of the different clinical profiles we obtained, future research might address those questions through further explorations of brain structure and neurophysiology.