
Abstract
Science knowledge refers to the depth and breadth of facts acquired within the life, social, and earth sciences, and it has implications for both public and personal health. Drawing from cognitive aging theory, we examine whether levels of science knowledge are associated with age, neuropsychological functioning, and personal health literacy. Fifty-two younger and fifty older healthy adults completed our telephone-based study that included a commonly used test of science knowledge, as well as measures of neuropsychological functioning, health literacy, and relevant descriptives (e.g., mood). Adjusting for other demographics and neuropsychological functioning, older adults had significantly lower science knowledge test scores than younger adults. In the full sample, lower science knowledge showed medium-to-large associations with episodic memory, executive functions, and health literacy, independent of years of education. These results suggest that older adults’ science knowledge falls slightly below that of their younger counterparts and is independently associated with higher order neuropsychological functions and aspects of personal health, which may have implications for accessing, understanding, and using relevant public health information across the lifespan.
Keywords
Introduction
The concept of literacy refers to an individual’s knowledge and competencies in a particular area. While the fundamental reading and writing aspects of linguistic literacy are the most widely studied aspects of literacy (Bartelson, 1986), there are also robust literature on several applied literacies that involve overlapping but separable elements (e.g., health, financial, technological, and legal). Conceptual models of these applied literacies (Berkman et al., 2010) often describe general and domain-relevant lower-order abilities (e.g., word knowledge, semantic memory, and numeracy) that serve a supporting role for related higher-order abilities (e.g., comprehension, integration, and application). Together, these lower- and higher-order abilities help to inform decision-making and behaviors related to that subdomain domain of literacy (Sørensen et al., 2012). Such applied literacy abilities are often contextualized by various antecedents (e.g., social determinants), individual factors (e.g., age, sex, and race/ethnicity), and relevant outcomes (e.g., engagement and utilization, quality of life). The cognitive processes conveyed in these conceptual models of applied literacy have a strong brain basis, which can involve diverse cortical and subcortical networks (Damasio et al., 1976; Petersson et al., 2001). Indeed, several applied literacies are relevant to the daily functioning of older adults and persons with neurocognitive disorders, including financial (Gerstenecker et al., 2017), technological (Woods et al., 2019), and health (Morgan et al., 2015) literacy.
In the current study, we focus on the neuropsychological and personal health aspects of science literacy, and specifically science knowledge. Science knowledge refers to the depth and breadth of facts that one has accumulated and retained from the life, social, and earth sciences (Snow et al., 2016). Science knowledge is a lower-order, fundamental aspect of science literacy that can include factors such as word knowledge (e.g., definition and pronunciation of science terms), content knowledge (e.g., knowing that electrons are smaller than atoms), and numeracy (e.g., understanding percentages). The higher-order, applied aspects of science literacy involve comprehension of the fundamental elements of scientific practice, the social context of scientific processes and their uptake, identifying and judging scientific expertise, and dispositions and habits of mind (Snow et al., 2016). Science literacy has important implications at the individual, community, and societal levels. During the 2019 coronavirus epidemic, for example, individuals were challenged to utilize their science literacy skills to identify reliable and scientifically sound information about the prevention, spread, and treatment of infectious diseases and to make informed decisions about health, fiscal, and social issues (Babicz et al., 2021). Of course, there are many mediators and moderators along the pathway from science knowledge to actual behavior (Suldovsky, 2022), but science knowledge is nevertheless a foundational element of science literacy (Snow et al., 2016). Access to formal education and educational attainment are strongly and positively associated with science knowledge (Pew Research Center, 2015). Men and individuals who identify as white also tend to have higher scores on some measures of science knowledge in the United States (Pew Research Center, 2015, 2019).
The relationship between age and science knowledge is less well understood. Science knowledge can emerge in the early preschool years (Guo et al., 2015) and is thought to develop throughout childhood, alongside academic skills such as math and reading (Wang, 2005). However, the extent to which science knowledge is stable, increases, or decreases with older age remains unclear. We are unaware of any peer-reviewed studies that have systematically examined the effects of age on general science knowledge among adults. Both theory and evidence suggest that crystalized knowledge (e.g., semantic memory) tends to show modest increases with older age (Lindenberger, 2014), despite parallel, age-related decreases in many fluid aspects of cognition (e.g., episodic memory, executive functions, processing speed). For example, vocabulary and general fund of knowledge, as measured by traditional intelligence tests, are higher in older versus younger healthy adults (Wechsler, 2008). Yet two descriptive analyses from the Pew Research Center (2015, 2019) provide mixed evidence for the influence of age on science knowledge in adults. In a 2015 Pew survey, nearly 25% more younger (age <30 years) than older (age >64 years) adults correctly answered questions related to modern science (i.e., technology); however, older adults were slightly better than younger adults on questions about historical science knowledge. In the 2019 Pew survey, older adults had slightly lower general science knowledge scores than younger adults, but these age-related effects dissipated when the models were adjusted for sex, race/ethnicity, and education. Given these mixed and largely descriptive survey findings, we sought to evaluate whether healthy younger and older adults differed in science knowledge.
Given the obvious cognitive basis of science of knowledge, another goal was to evaluate its neuropsychological correlates in older and younger adults. We are unaware of any prior studies of the neuropsychological correlates of science knowledge in adults. We hypothesized that higher levels of science knowledge would be associated with better performance on higher-order measures of cognition, including verbal intelligence, numerical working memory, executive functions, and declarative memory. The bases for these hypotheses arose partly from conceptual models of knowledge and declarative memory, which posit that different aspects of declarative memory are separable (Goodglass et al., 1986) and work in concert to establish robust long-term memory traces (Tulving, 1987). Therefore, we expected that science knowledge would correlate strongly with verbal intelligence (e.g., fund of general knowledge) and other aspects of declarative memory (e.g., verbal recall). Moreover, executive functions and working memory play an important role in the encoding and retrieval of declarative memory (Moscovitch, 1992), including semantic memory (Troyer et al., 1997). In fact, a few studies with children have reported medium-to-large associations between science knowledge and measures of verbal and non-verbal reasoning (Guo et al., 2015). Our hypotheses are also supported by studies showing that these higher-order neuropsychological constructs have medium-to-large associations with aspects of financial (Gerstenecker et al., 2017), technological (Woods et al., 2019) and health (Morrow et al., 2006) literacy.
Our final aim was to evaluate the relationship between science knowledge and health literacy. The relevance of science knowledge to personal and public health has been recognized for decades (Shen, 1975). We aimed to examine whether science knowledge was associated with a few dimensions of personal health literacy. The scientific foundation of many aspects of health is readily apparent, but current models of health literacy (e.g., Sørensen et al., 2012) do not explicitly consider general science knowledge or science literacy. Different aspects of science literacy (e.g., knowledge of specific scientific content and scientific practices) may be important for accessing, digesting, and using information related to health (Snow et al., 2016), which can vary in its scientific rigor (Winker et al., 2000). Moreover, prior studies show that specific health knowledge is positively associated with rigorous health information seeking, general fund of knowledge, and self-efficacy for interacting with health materials (Babicz et al., 2021). As such, we hypothesized that general science knowledge would be positively associated with specific health knowledge and self-efficacy for navigating health-related materials.
Method
Participants
The current study was a planned, secondary analysis of data collected as part of a dissertation project (Matchanova et al., 2023). The parent study was conducted in compliance with our university’s Institutional Review Board and the data were gathered in August and September of 2021. Potential participants were recruited from across the U.S. via word-of-mouth and postings on social media. Interested participants completed an online screening survey, providing written digital, informed consent and affirming that they were: (a) 18–35 years or 50 years or older; (b) at least minimally proficient in English; (c) located in the United States; (d) using at least one social media platform at least one time per week for at least 1.5 hours per week; and (e) not diagnosed with any major neurological (e.g., seizure disorder) or psychiatric (e.g., psychosis) conditions. The study design was cross-sectional and included both between-group and correlational approaches. We used a discrepant age-group classification, which is a common design in cognitive aging research that can enhance power for smaller scale studies. The younger group included adults aged 18–35, which allowed for the enrollment of individuals outside of the traditional college-based youth and thus enriched the range of educational attainment. The sample of older adults included persons as young as age 50, which was done in consideration of growing evidence regarding the importance of understanding cognitive aging in late middle age (Lindenberger, 2014).
Descriptive Data for the Sociodemographic and Psychological Characteristics of the Younger and Older Study Groups.

Note. Bolded p-values < .05. WAIS-IV = Wechsler Adult Intelligence Scale – Fourth edition.
Materials and Procedures
Study participants worked with a trained research assistant via telephone to complete a brief study about COVID-19 information sharing via social media (Matchanova et al., 2023), as well as measures of neuropsychological functioning, general health literacy, and relevant descriptives (e.g., mood).
Science Knowledge
We assessed participants’ factual science knowledge with a 17-item measure (McPhetres et al., 2019) that included widely used general content items from the National Science Board’s Indicators survey (https://ncses.nsf.gov/indicators). Example items include “Electrons are smaller than atoms” and “All radioactivity is man-made.” The internal consistency of this measure was adequate in the full sample (Cronbach’s alpha = .732). Therefore, a total science knowledge score was derived by summing the number of correct items and dividing by 17 to reflect the percentage of accurate responses (sample range = 29%–100%).
Core Neuropsychological Test Battery
The participants completed a telephone-based neuropsychological test battery (Matchanova et al., 2021) with prior evidence of good reliability and validity (e.g., Babicz et al., 2021; Matchanova et al., 2021; Thompson et al., 2023; Thompson et al., 2024). Memory was assessed with the Delayed Recall and Recognition Discrimination Index from the Hopkins Verbal Learning Test-Revised (HVLT-R; Brandt & Benedict, 2001), which is a 12-word supraspan list learning and memory task. Attention was assessed with the Digit Span forward and backward subtests of the Weschler Adult Intelligence Scale—Fourth Edition (WAIS-IV; Wechsler, 2008) and Trial 1 of the HVLT-R. Executive functions were assessed with action (verb) fluency (Piatt et al., 1999; Woods et al., 2005), Category Switching from the Delis-Kaplan Executive Functions Scale (D-KEFS; Delis et al., 2001), and Part B of the Oral Trail Making Test (Mrazik et al., 2010; Ricker & Axelrod, 1994). Raw scores were converted to age-adjusted normative z-scores based on the references cited above. A global composite was constructed by averaging the age-adjusted z-scores derived from these measures (Cronbach’s alpha = .732).
Other Relevant Aspects of Cognition
Estimated Verbal IQ
Participants completed the Information subtest of the WAIS-IV, which assesses general fund of knowledge. Only the 19 items that did not involve the physical sciences were scored for this analysis. A raw total score was generated from those 19 items and was used in this study (sample range = 3–19).
Cognitive Reflection Test
Participants completed a 6-item version of Frederick’s (2005) Cognitive Reflection Test, which assesses the ability to inhibit a reflexive response to basic knowledge and numerical questions (e.g., Who makes Christmas presents at the North Pole?). Correct responses from the six items were summed to generate a total score (sample range = 0–6).
Health Literacy
Participants completed two questionnaires on health literacy. On the Brief Health Literacy Screening Tool (Chew et al., 2008), participants rated the extent to which they agreed with three statements about their health literacy on a five-point scale (Cronbach’s alpha = .739). Higher scores indicate higher perceived health literacy (sample range = 7–15). On the eight-item Electronic Health Literacy Scale (Norman & Skinner, 2006), participants rated their knowledge and perceived skills at finding, evaluating, and applying electronic health information on a five-point scale (Cronbach’s alpha = .884). Higher scores indicate greater perceived efficacy using the internet for health-related purposes (sample range = 8–40). The total scores of these two health literacy measures showed a medium-to-large correlation (r = .43) and were combined into an average sample-based z-score.
Numeracy
Participants completed two measures of numeracy. The seven-item Expanded Numeracy Scale (ENS; Lipkus et al., 2001) queried participants about health-related percentages and proportions (sample range = 0–7). The Arithmetic subtest of the WAIS-IV assesses general mental math abilities (sample range = 8–22). The raw scores from the WAIS-IV Arithmetic and ENS were strongly correlated (r = .55) and were combined into an average sample-based z-score.
Other Study Assessments
Participants completed a questionnaire to gather information about sex, age, race/ethnicity, education, and medical comorbidities. They also completed two measures assessing their current mood, which have also shown evidence of reliability and validity via telephone (Babicz et al., 2021; Matchanova et al., 2023; Thompson et al., 2023, 2024). The 5-item Geriatric Anxiety Inventory-Short Form (Byrne & Pachana, 2011) assessed anxiety symptoms (e.g., “I often feel nervous.”) on a 5-point scale (sample range = 0–5; Cronbach’s alpha = .730). A yes/no version of the 7-item Geriatric Depression Scale (Broekman et al., 2011) was used to assess current symptoms of depression (e.g., helplessness; sample range = 0–5; Cronbach’s alpha = .706).
Data Analysis
All analyses were conducted in JMP Pro 16 (2021, SAS). The primary study aims were tested with a multiple regression, with age group as the predictor variable and the accuracy score from the Science Knowledge Test as the criterion. Due the relatively small sample sizes and concern for over-saturating the models, we adopted the confound approach to determining covariates for the primary regression (Field-Fote, 2019). Specifically, any variable that was significantly associated with both age group and Science Knowledge Test scores at p < .05 was included as a covariate. A series of multiple and logistic regressions with the a priori covariate of education was used to test whether Science Knowledge Test performance was related to and neuropsychological domain scores and health literacy. For these analyses, we limited the risk of Type I error by conducting them in the full study sample and by adjusting the critical alpha to .01.
Results
Determining Covariates
As shown in Table 1, there were age group differences in sex, race/ethnicity, overall neuropsychological functioning, Cognitive Reflections Test score, and medical conditions (ps < .05). Medical conditions were not related to Science Knowledge Test performance (p = .172) and was thus not included as a covariate. The other four variables of sex, race/ethnicity, neuropsychological functioning, and the Cognitive Reflections Test score were all significantly related to Science Knowledge Test performance (ps < .05) and were thus included as covariates in the primary analysis.
Age Group and Science Knowledge
We conducted a multiple regression to predict Science Knowledge Test performance from age group, sex, race/ethnicity, neuropsychological functioning, and the Cognitive Reflections Test score. The full model was significant (F[6,95] = 10.7, p < .0001) and accounted for over one-third of the variance in Science Knowledge Test performance (adj R2 = .37). Age group was a significant contributor to the model, such that older age was associated with lower Science Knowledge Test accuracy (B = −0.07 [-0.14, −0.01]). In addition, Black race (B = −0.12 [-0.20, −0.04]), lower neuropsychological functioning (B = 0.06 [0.01, 0.12]), and lower Cognitive Reflections Test scores (B = 0.04 [0.02, 0.06]) scores were all independently (ps < .05) associated with lower Science Knowledge Test accuracy (Figure 1). Bar Graph Displaying the Science Knowledge Test Performance Scores of Groups of Younger (n = 52) and Older (n = 50) Adults.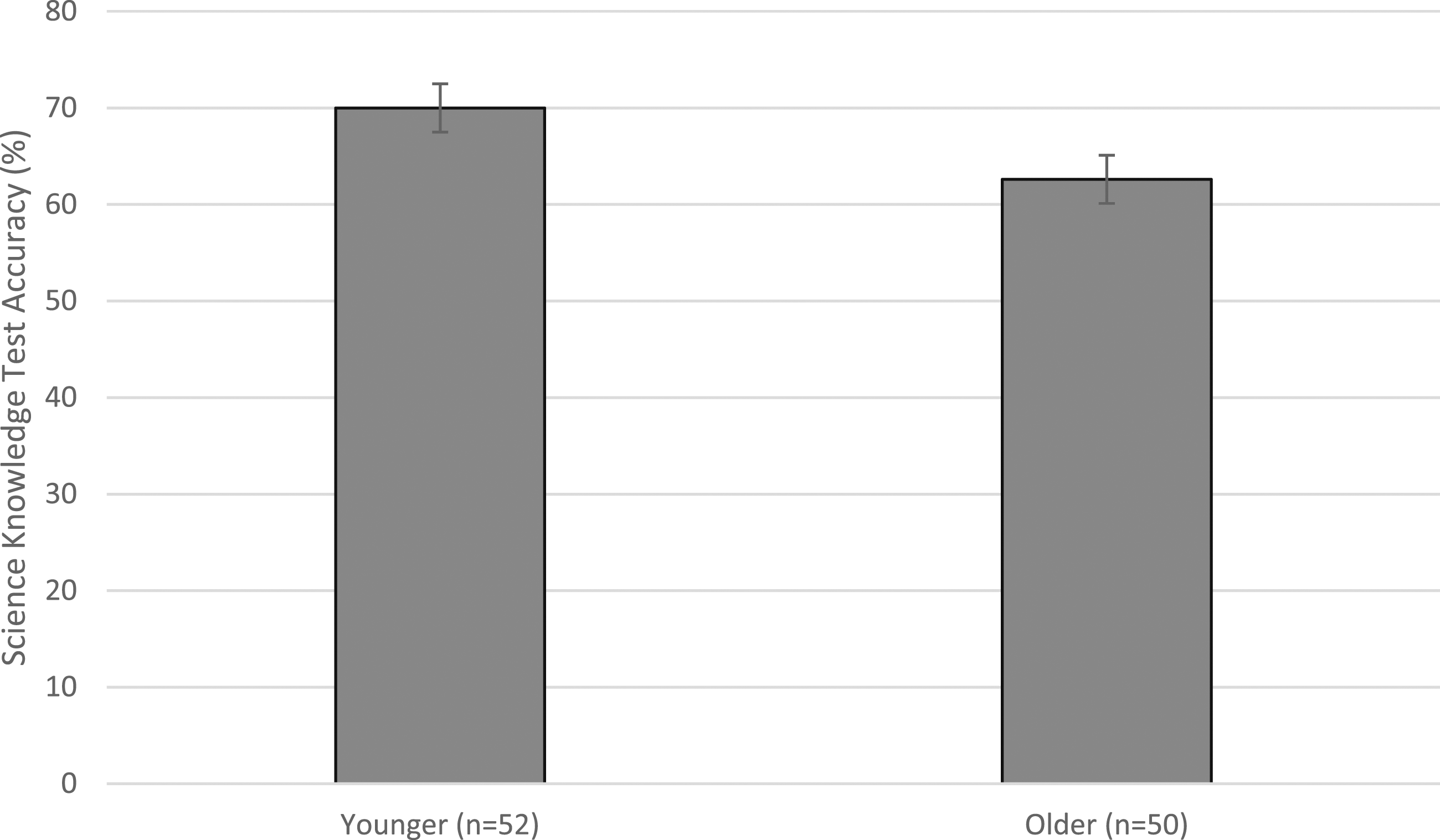
Post hoc Analyses
Given the lack of prior research in this area and the importance of considering sociodemographics and possible moderators (e.g., Nieuwenhoven & Klinge, 2010), we repeated the primary models as stated above while also forcing in education as a covariate. Age remained a significant predictor in that model (p = .0015) and education was not significant (p > .20). In addition, we conducted four post hoc exploratory models that included all the variables described above alongside an interaction term between age group and each of the four covariates. None of the four interaction terms were significant in these models (all ps > .20).
Neuropsychological Correlates of Science Knowledge
Univariate Correlations Between Raw Scores on the Science Knowledge Test and Measures of Cognition in the Full Study Sample and in the Older and Younger Groups Separately.
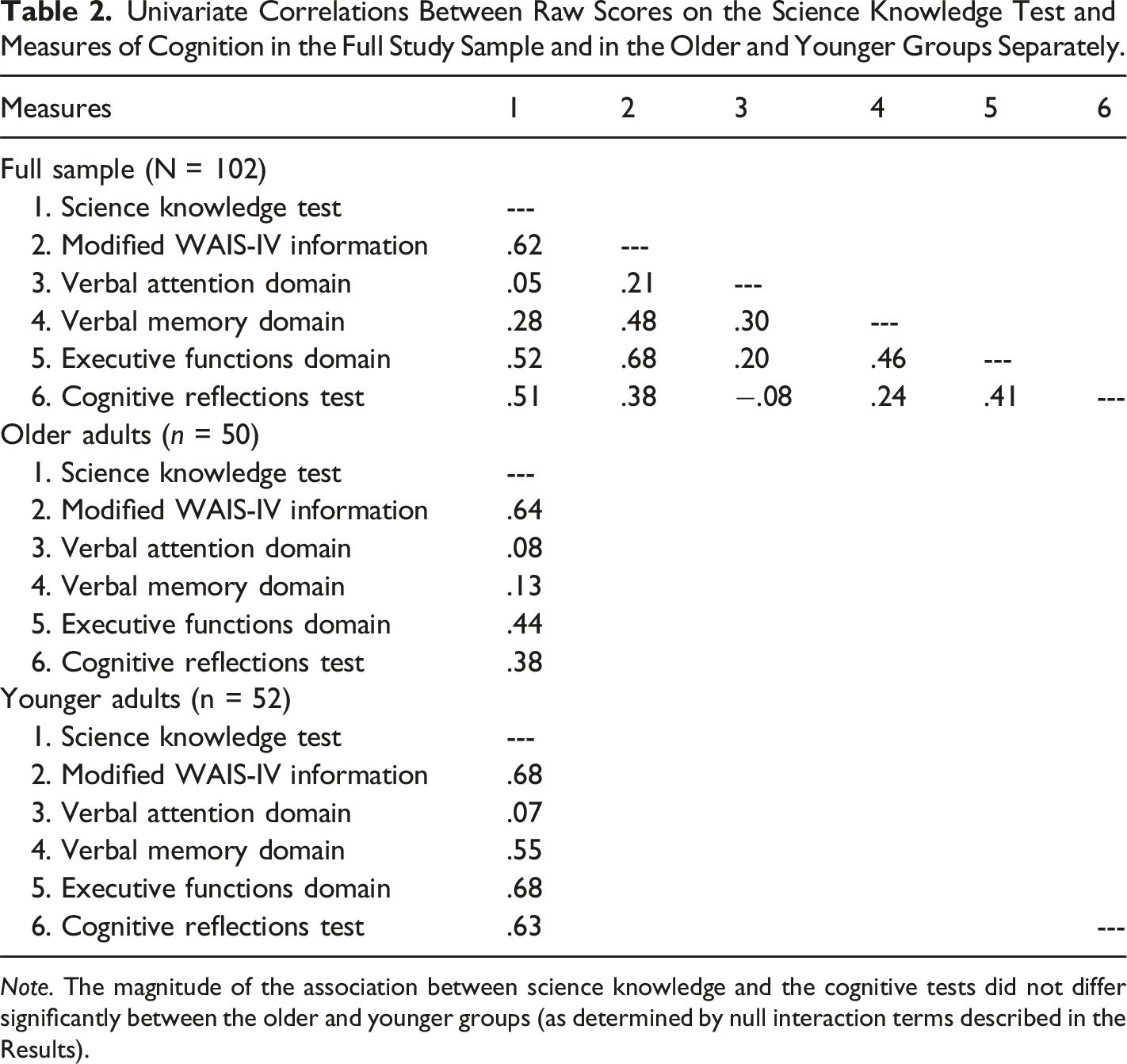
Note. The magnitude of the association between science knowledge and the cognitive tests did not differ significantly between the older and younger groups (as determined by null interaction terms described in the Results).
Health Literacy Correlates of Science Knowledge
At the univariable level, science knowledge correlated with the health literacy composite at r = .28 (r = .32 in the Younger sample and r = .30 in the Older sample) and with the numeracy composite at r = .53 (r = .66 in the Younger sample and r = .40 in the Older sample). A series of regressions were conducted using the Science Knowledge Test as the predictor and education as a covariate. These analyses showed that higher Science Knowledge Test accuracy was independently associated with greater self-efficacy for health literacy (B = 1.2 [0.3, 2.0], p = .004) and better numeracy (B = 2.4 [1.6, 3.2], p < .0001). Note that, the magnitude of the association between Science Knowledge and health literacy did not differ statistically in older versus younger samples all ps > .05 in a series of post hoc models for which an age by health literacy interaction term was entered.
Discussion
Science literacy has clear implications for both personal and public health, but we know little about potential influences of age, neurocognition, and health literacy in this important construct. We found that older adults showed mildly lower science knowledge than their younger counterparts. On average, older adults achieved scores on the science knowledge test that were 5% less accurate than younger adults. Results were consistent with the univariate findings from two previous studies by the Pew Research Center (2015; 2019) but extend that descriptive work by demonstrating the independence of the observed association between older age and lower science knowledge. Specifically, the younger and older groups were comparable in education, general knowledge, mood, and health literacy, which therefore cannot be considered “confounds” (Field-Fote, 2019). Moreover, although the age groups differed in sex, race/ethnicity, and cognition, these variables were included as covariates in the regression in which the age effect was observed. Notably, although some domains of knowledge increase with age (e.g., Lindenberger, 2014), our findings align with studies showing that older adults nevertheless face challenges with aspects of applied literacies, including financial (e.g., Leung et al., 2022) and technological (Woods et al., 2019) literacy. One interpretation of this pattern of differential aging effects on subdomains of knowledge is that older adults may have difficulty keeping pace with the many changes and advancements in these applied areas of literacy. In other words, it is possible that age-related changes in brain structure and function may make it harder for older adults to update their science knowledge.
In support of that interpretation, science knowledge showed medium-to-large associations with measures of delayed verbal memory and aspects of executive functions independent of education in the full sample. Examination of the univariable effect sizes suggested that these effects may have been larger in the younger sample (see Table 2); however, a series of post hoc regressions produced reliably null age group by cognition interaction terms, which indicates more convincingly that the associations did not differ meaningfully across the older and younger adults. Null and small associations were observed for basic verbal attention suggesting that retention of science knowledge is challenging, even for healthy and highly educated individuals (e.g., Custers, 2010). Episodic memory likely plays an important role in both the lower- and higher-order aspects of other applied literacies, including health (e.g., Babicz et al., 2021; Morgan et al., 2015) and technological (Woods et al., 2019) literacy. In fact, memory may work in concert with executive functions to facilitate robust encoding, long-term retention, and use of novel health-related information (Babicz et al., 2021; Moscovitch, 1992). In this case, standard executive functions were measured with speeded tests of cognitive flexibility and generativity from semantic memory stores. Likewise, the Cognitive Reflections Test and numeracy composite can both be interpreted under the umbrella of executive functions. The former requires individuals to inhibit reflexive responses to knowledge-based questions, while the latter involves a strong verbal working memory component. Table 2 further supports this interpretation, showing broadly large univariate correlations between executive functions, Cognitive Reflections Test, and numeracy. The integrity of the pre-frontal and temporal brain networks that support strategic aspects of memory and executive functions are susceptible to modest declines in older adults (e.g., Turner & Spreng, 2012). Thus, older adults may have difficulty quickly learning, organizing, accessing, and generating science-related information. It is also plausible that cohort effects may play a role in the age-related discrepancies in science literacy, whereby younger adults could have more (and more recent) opportunities to update their knowledge (e.g., via technology engagement).
Science and health are often intertwined, particularly with the rise of evidence-based health practice over the past 20 years. However, the role of general science knowledge in personal health and health literacy is not well understood. In this study, science knowledge was associated with several personal health factors; individuals with higher levels of general science knowledge showed better numeracy and reported greater self-perceived health literacy. Medium-to-large effect sizes were observed for the relationships between science knowledge and these aspects of health literacy; moreover, the observed effects were independent of education. Findings align with a handful of studies suggesting that science knowledge and self-efficacy are related (e.g., Davis et al., 2018; Kosobuski et al., 2017) and extend that work to the applied domain of health literacy. One possibility is that general science knowledge may help scaffold the foundational elements of some applied literacies, such as health and technology (Sørensen et al., 2012). In other words, it may be easier for individuals with strong general science knowledge to find, digest, and retain applied health-related information. Future studies may seek to better understand the interplay between science and health literacy, expanding their consideration beyond the lower-order foundational domain of knowledge. Findings also suggest that conceptual models of health literacy might benefit from integrating aspects of science knowledge and literacy.
Limitations and Directions for Further Research
Several limitations to this study deserve consideration in the interpretation and generalization of the findings. This study was a secondary analysis of data that was gathered for another purpose via telephone. As such, the neuropsychological battery was exclusively comprised of verbal measures and did not include tests of many constructs that would be relevant to science knowledge (e.g., novel problem-solving, concept formation, inhibition). Furthermore, the assessment of science literacy was limited to a single measure of science knowledge. Although this measure showed good internal consistency in this sample and has strong evidence of construct validity (see Snow et al., 2016), it only covered a limited dimension of science knowledge and did not assess other aspects of science literacy (e.g., word knowledge and understanding of scientific processes). These results are also tempered by their reliance on a cross-sectional, split-group research design with relatively few individuals aged 65 and older. Longitudinal studies that use a continuous lifespan approach and include larger samples of much older adults are needed to fully understand the developmental trajectory of science literacy. The older adult sample was 80% white and had relatively few individuals with lower levels of education. Moreover, the younger and older study groups were not comparable in sex and race/ethnicity; although we covaried for these demographic factors, such statistical methods are imperfect and are no replacement for careful group matching procedures. Given the importance of race/ethnicity, sex, and education (Pew Research Center, 2015, 2019) in science knowledge in the US, future studies are needed to carefully examine the nature and extent of age-related differences in under-represented racial/ethnic and socioeconomic groups. With these limitations in mind, we interpret our study findings to suggest that older adults may have lower science knowledge, which may correspond with age-related changes in brain structure and function that make it difficult for them to keep pace with scientific advancements and can negatively influence critical aspects of personal health.
Conclusion
Overall, findings from this study suggest that the general science knowledge of older adults falls slightly below that of their younger counterparts, which may reflect difficulties with their age-related organized search and retrieval of information from memory. Indeed, higher levels of science knowledge were associated with the higher order neuropsychological functions of memory and executive functions in both older and younger adults. Finally, science knowledge was independently associated with self-efficacy for navigating one’s personal health and with performance-based numeracy. As such, science knowledge may have implications for accessing, understanding, and using relevant public health information across the lifespan.
Footnotes
Acknowledgements
The authors thank the University of Houston and the study participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Study funding and infrastructure support was provided by the University of Houston.
IRB Compliance
This study was approved by the University of Houston’s Institutional Review Board (IRB STUDY# 00003010). Participants provided written, digital, informed consent.