
Abstract
Hyperactive and hypoactive children show attentional deficits. An effort was made to modify their approaches to a vigilance task by varying the feedback received for correct detections and false alarms. It was expected that hyperactive children would do better when receiving knowledge of false alarms; hypoactive children would do better when receiving knowledge of correct responses. 20 hyperactive and 20 hypoactive children, ages 6 to 10 yr., were each tested under three conditions with a vigilance task: (a) feedback for correct responses (KR+), (b) feedback for false alarms (KR -), (c) no feedback (NKR). Feedback was given by a tone. For the total error score, hyperactive subjects committed more errors than hypoactive ones under KR+ and fewer errors under KR -. Hypoactive children committed fewer errors under KR+ than no knowledge. Partial support for the hypothesis was obtained. Hyperactive children generally do better when given knowledge of errors; they become more cautious in responding. Hypoactive children do best when given information regarding correct responses; they become less inhibited in responding.
During the past decade a great deal of clinical interest has focused on children defined as hyperactive. Hyperactivity is seen as manifested by attentional deficits, impulsivity, and motoric restlessness. Less attention has been directed to the hypoactive children who, while at the opposite end of the activity level spectrum, also show evidences of attentional deficits. The present study attempted to determine under laboratory conditions the contingencies through which the attention deficit of the hyperactivity and hypo-activity syndromes could be modified.
The study focused on behavioral approaches to the modification of attentional deficits. Numerous studies have reported the use of behavioral strategies to help hyperactive children in particular, all of which show some degree of success in reducing hyperactive behavior, usually defined in terms of increased in-seat behavior (Christensen & Sprague, 1973; Edelson & Sprague, 1974; Meichenbaum & Goodman, 1971; Palkes, Stewart, & Kahana, 1968).
We could find no studies in which techniques for reducing attentional deficits were compared using samples of hyperactive and hypoactive children. Dykman, Ackerman, Clements, and Peters (1971) hypothesized that hyperactive learning-disabled children were weak in inhibition, habituated slowly to novel stimuli, and showed considerable spontaneous recovery of extinguished responses. It was further thought that hypoactive children were strong in inhibition, habituated rapidly to novel stimuli, and extinguished rapidly. It may be argued that, if a hyperactive child is to be helped to focus attention, the basic task becomes one of helping him to inhibit responses; on the other hand, the hypoactive child must be encouraged or taught to be less inhibited in responding.
An experimental vehicle for studying attentional deficits or hyperactive-hypoactive behaviors utilizing a basic vigilance task has been investigated by Anderson, Halcomb, and Doyle (1973). The vigilance task is quite simple, and the only requirement for achieving a performance at a near perfect level is maintaining attention on the task. The observer-subject has to be alert almost continuously to detect and report all signals. Detection failures can be identified with failures in attention. It was demonstrated by Anderson, et al. (1973) that their computer-controlled vigilance task could differentiate between learning disabled children and normal controls. Moreover, the task showed different performance patterns between hyperactive, normoactive, and hypoactive children. Sykes, Douglas, and Morgenstern (1973), and Sykes, Douglas, Weiss, and Minde (1971) have also studied the performance of hyperactive children on a continuous performance task which is a type of vigilance task. Their results were similar to those reported in the studies from Texas Tech (Anderson, et al., 1973; Anderson, Halcomb, Ozolins, & Hopson, 1974; Anderson, Halcomb, Gordon, & Ozolins, 1974; Doyle, Anderson, & Halcomb, 1976).
In the present study the vigilance task was used to provide a test of the observation that hyperactive children need to develop caution in responding to a task demanding close, sustained attention while hypoactive children need to be less inhibited in their responses to the same type of task. Studies of vigilance task with normal adult populations have suggested that knowledge of results of false alarms (KR-) has led to a more cautious performance while knowledge of results of correct detections (KR+) has led to an increased tendency to respond. Thus, the hypotheses of the present study may be stated clinically as follows: hyperactive children will make fewer random errors and more correct responses to a vigilance task when given knowledge of their random errors (false alarms). The hyperactive children will respond to knowledge of correct responses by increasing their already high level of motoric activity; in short, they will make an excessive number of responses, thereby increasing the false alarm rate. On the other hand, hypoactive children will better their performance (increase correct detections) when given knowledge of their correct detections. Providing a hypoactive child with a knowledge of errors will tend to increase an already excessive level of inhibition and yield a subsequent reduction in correct detections.
Method
Subjects
The subjects were children ranging in age from 6 yr., 0 mo. to 10 yr., 10 mo. who were enrolled in resource rooms of a public school system and two private schools in a metropolitan area. Children were placed in the classes for learning disabled based on appraisals from psychologists and educational diagnosticians. The criteria established by the Texas Education Agency for placement of children in the program were utilized.
Out of a total population of 131 children whose parents responded affirmatively to a request for participation in the research, 43 were categorized as hyperactive and 32 as hypoactive. Twenty hyperactive and 20 hypoactive children were then drawn at random from the population of subjects. Judgments of activity level were obtained by categorizing the children into one of three levels of activity: hyperactive, normoactive, or hypoactive. Ratings of activity level were obtained from both the parents and the school by simply asking if it was felt that the child in question was in general much more active, about the same, or not at all as active as other children of the same age. If there was disagreement between parents and school ratings concerning the child's activity level, a third ranking was obtained by observing the child through a one-way mirror during the first experimental session. The child was then classified into the category decided, upon by two out of the three observers. Children on medication were not ranked or included in the study. The ranking procedures in general followed the methods outlined in a previous study by Doyle, Anderson, and Halcomb (1976).
Apparatus
The basic vigilance/distractibility task has been described in detail by Anderson, et al. (1973). The subject's task was to monitor a visual display for 30 min. to detect periodic signals against a background of regularly occurring events. The display console was housed in a booth approximately 1.20 m X 120 m. The booth was carpeted, air-conditioned, and had indirect lighting. A pleasant, carpeted waiting room served as an entry way where the child's parents could sit and wait while the session was in progress.
The child was instructed to observe two flashing lights which appeared on a panel in front of him. The lights flashed in combinations of red-red, green-green, or red-green (green-red) at the rate of one flash/2 sec. with a .2-sec. duration. A response button mounted in a bicycle handle-bar grip was connected to the display console by a wire .51 m long. The subject could hold the grip in either hand and was not required to maintain a certain position in order to make a response.
During the 30-min. session, a total of 840 red-red, or green-green combinations were presented; 60 red-green (green-red) signals were interspersed among the 840 events. The red-green combinations were presented on a variable-ratio 15 schedule, with a total of 10 red-green combinations appearing every 5 min.
A 70-dB, 1K-Hz, or 18K-H2 tone served as knowledge of results. The auditory tone had a duration of 0.5 sec. and was generated by a BR Foringer Audio Oscillator connected to a speaker housed out of sight beneath the display console. A second speaker, similarly housed, was connected to a Sony Cassette recorder. The entire sequence of flashing lights and the knowledge of results presentations were controlled by a Digital Equipment Corporation PDP-8/e Digital Computer. The equipment was set up to provide three conditions: (1) Knowledge of correct response (KR+)—tone followed each correct detection, (2) Knowledge of errors (KR-)—tone followed each false alarm, and (3) No information (NKR)—no tone following either a correct detection or false alarm. The primary dependent variables were: (a) total number of correct detections for the 30-min. session; (b) total number of false alarms for the 30-min. session; and (c) total errors—total correct detections missed plus total false alarms.
A correct detection was defined as pressing the response button to the red-green (green-red) stimulus combination. False alarms were defined as responses to the red-red or green-green light combinations.
Design
A split-plot analysis of variance design was used. The between-subjects variable was the two differing activity levels (hyperactive and hypoactive). The within-subjects variables were three different types of KR and six 5-min. intervals; all cells contained 20 subjects. The sequence of administration of the repeated treatment levels (knowledge of results) in combination with one level of the nonrepeated treatment (activity level) was randomized independently for each block. The frequencies of the auditory knowledge of results were counterbalanced between subjects.
Procedure
Each child was exposed to the three conditions of feedback regarding performance in three sessions spaced 1 wk. apart. Previous research has demonstrated that performance on the vigilance task is not affected by practice. A 5-min. practice session was conducted prior to the 30-min. experimental session. At the outset of this session, instructions were standardized and relayed via an audio cassette tape recording into a loud-speaker in the chamber. A 30-min. white noise recording was played during the experimental session to mask distracting noise outside the booth.
No attempt was made to keep a child in the booth against his will, and the run was terminated if a youngster wish to leave. All of the hypoactive children completed the three experimental sessions. Four hyperactive children either quit in the middle of a session or did not appear for future sessions. Their data were not used, and four other children were drawn at random from the available population of hyperactive children.
Results
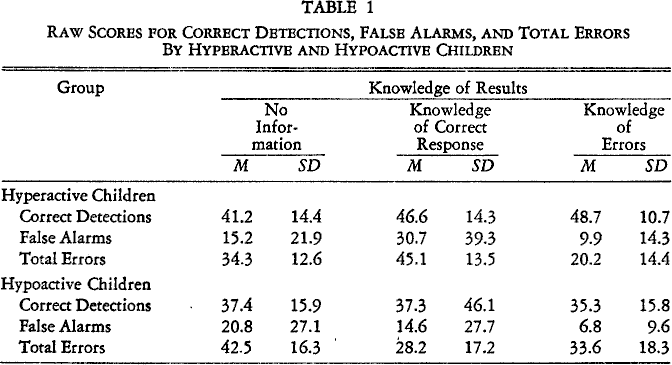
The dependent variables, correct detections, false alarms, and total errors, were examined across the three conditions using raw data (Table 1).
Raw Scores for Correct Detections, False Alarms, and Total Errors By Hyperactive and Hypoactive Children
Correct Detections
The analysis yielded significant effects for the different types of feedback (F = 5.86, df = 2/76, p < .01; Fig. 1). An analysis of the simple main effects indicated that hyperactive children obtained significantly more correct detections than did hypoactives under knowledge of errors (F = 11.70, df = 1/114, p < .01). Within-groups, the analysis pointed to significant differences for both hyperactive (F = 3.314, df = 2/76, p < .01) and hypoactive (F = 8.373, df = 2/76, p < .01) children across the differing types of feedback. The Tukey HSD statistic showed that hyperactive children obtained significantly fewer correct detections under no information than they did either under knowledge of correct detections (q = 3.61, df = 3/76, p < .05) or knowledge of errors (q = 3.98, df = 3/76, p < .01). Hypoactive children obtained significantly more correct detections under knowledge of correct detections than they did either under no information (q = 5.83, df = 3/76, p < .01) or knowledge of errors (q = 7.89, df = 3/76, p < .05).

Vigilance performance as correct detections related to type of feedback
False Alarms
A test for homogeneity of variance of the false alarms data gave a significant F test. The data could not be transformed into a homogeneous distribution; consequently, Friedman's two-way analysis of variance (a median test) was used on the data in addition to the F statistic, as a check for the influence of extreme scores. Friedman's two-way analysis of variance showed a significant effect of feedback on the total amount of false alarms committed by hyperactive children (r2 = 9,10, df = 2, p < .01), but not by hypoactive ones (r2 = 4.47, df = 2). Specifically, for hyperactive children, the Wilcoxon matched-pairs signed-ranks test showed significantly more false alarms under knowledge of correct detections than under either no information (T = 27.5 N = 17, p < .02) or knowledge of errors (T = 24.8, N = 18, p < .05). Between groups, the Mann-Whitney U test indicated a significant difference between the amount of false alarms committed by hyper- and hypoactive children under knowledge of correct detections (r2 = 2.52, p < .01). The total false alarms results also were analyzed by the F ratio.
No significant differences were found for activity level (power = .65). A significant treatment effect (F = 6.31, df = 2/76, p < .01) and interaction between treatment and activity level (F = 3.27, df = 2/76, p < .05) were found (Fig. 2). An analysis of the simple main effect indicated that hyperactive children committed significantly more false alarms than hypoactives under knowledge of correct detections. Within groups, the analysis pointed to significant differences for both hyperactive (F = 13.52, df = 2/76, p < .01) and hypoactive (F = 5.64, df = 2/76, p < .01) children across the differing types of feedback. The Tukey HSD statistic showed that hyperactive children committed significantly more false alarms under knowledge of correct detections than either no information (q = 5.277, df = 3/76, p < .01) or knowledge of error (q = 7.076, df = 3/76, p < .01). Hypoactive children committed significantly fewer false alarms under knowledge of errors than they did under no information (q = 4.725, df = 3/76, p < .05).
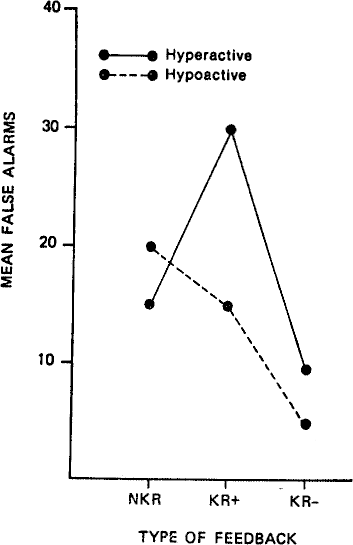
Vigilance performance as false alarms related to type of feedback
Thus, the only difference between the parametric and nonparametric analysis was the parametric finding of significantly fewer false alarms by hypoactive children under knowledge of errors. The influence of extreme false alarm scores on the parametric analysis must be considered in interpreting this apparent contradiction.
Total Errors
To obtain an over-all index of performance efficiency, correct detection and false alarm scores were combined into a single error score. For example, if a child obtained 50 correct detections and 10 false alarms, he was given an error score of 20 (10 missed correct detections and 10 false alarms). No significant difference was found for activity level. A significant treatment effect (F = 4.41, df = 2/76, p < .01) and interaction between treatment and activity level (F = 6.46, df = 2/76, p < .01) were found (Fig. 3). An analysis of the simple main effect indicated that hyperactive children committed significantly more errors under knowledge of correct responses than did hypoactives (F = 3.91, df = 1/114, p < .05). Within groups, the analysis pointed to significant differences for both hyperactive (F = 7.43, df = 2/76, p < .01) and hypoactive (F = 3.45, df = 2/76, p < .01) children across the differing types of knowledge of results. The Tukey HSD statistic showed that hyperactive children committed significantly more errors under knowledge of correct responses than under no information (q = 3.42, df = 3/76, p < .05) and significantly fewer errors under knowledge of errors than no information (q = 4.43, df = 3/76, p < .01). The difference between knowledge of correct responses and knowledge of errors performance for hyperactive youngsters also was significant (q = 7.76, df = 3/76, p < .01).

Vigilance performance as total errors related to type of feedback
The Tukey HSD showed hypoactive children committed significantly fewer errors under knowledge of correct responses than they did under no information (q = 5.13, df = 3/76, p < .01). Errors under knowledge of errors also were significantly fewer than under no information (q = 3.71, df = 3/76, p < .01). Total errors committed by hypoactive children did not differ significantly between knowledge of correct responses and knowledge of errors (q = 1.42, df = 3/76).
Discussion
The results provided partial support for the hypotheses. Under the knowledge of error condition, that is, when hyperactive children were given feedback concerning errors (false alarms), the correct-detection rate showed a slight increase over knowledge of correct responses and there was a statistically significant decrease in false alarms. When performance was examined in terms of Total Errors committed, the hyperactive children showed significant differential responding under the various knowledge of results conditions. Total Error rate increased significantly under the knowledge of correct detection condition and decreased significantly under knowledge of errors when compared to no feedback.
When feedback was given regarding correct detections, the hyperactive children showed a significant increase in correct detections over the no-feedback condition. Both the hyperactive and hypoactive children showed an increase in correct detections when given positive feedback and their correct detection rates were similar.
The hypoactive children showed a significant increase in Correct Detections under the knowledge of correct detection as expected; when given feedback regarding random responses (false alarms) their correct detection rate dropped. This was in marked contrast to the correct detection rate of the hyperactives under knowledge of errors. The over-all false-alarm score showed a downward trend; highest rates were under the no-information condition and lowest rates under knowledge of errors. Finally, the total errors made when knowledge of correct responses and knowledge of errors were provided were not markedly different from each other although they improved over the condition of no feedback.
These data can be examined for clinical implications and from the theoretical perspective. Clinically, there is a strong indication that providing hyperactive children with a contingency perceived as positively reinforcing may have the inadvertent effect of increasing random responding. Not only may one get an increase in the desired behavior, but there may also be an increase in extraneous, random responding. In essence, there may be an increase in the behavior which teachers and parents particularly define as unproductive and evidence of motoric restlessness. On the other hand, feedback regarding errors, particularly the random moves, may have the effect of increasing the child's attentiveness. We are very cautious about identifying this type of feedback with an aversive condition or equating it with telling a child when he is wrong. The social connotations of this are subtle indeed.
Clinically, hypoactive children tend to do best when they are given positive feedback. Telling the hypoactive child when he is incorrect apparently increases caution which results in lower correct detection. Thus, the hypoactive children appear to need a lot of positive feedback. Feeding them information about errors may have the undesired effect of increasing their already cautious, slow responding approach to a problem.
There is a tendency among clinicians particularly to consider all children with attentional deficits as “hyperactive.” It is apparent that children with attentional deficits and distractibility are not a homogeneous group. Treating these children as if they respond uniformly is likely to lead to failure of treatment and frustration of clinicians.