
Abstract
The purpose of this study is to investigate the characteristics of law enforcement officers in the United States who died from COVID-19 in 2020–2021. Data were drawn from the Officer Down Memorial Page (ODMP) website. Results reveal that 729 law enforcement officers died from COVID-19 between 2020 and 2021, with the majority of these deaths occurring in the southern region of the United States. Additionally, a larger percentage of COVD-19 deaths were reported for officers who were male, White, and older compared to officers of color, younger officers, and female officers.
Keywords
Introduction
In March 2020, the World Health Organization (WHO) announced that COVID-19 infections had reached pandemic levels and individuals were advised to isolate as a means of mitigating its spread and severity. At the time of this announcement, COVID-19, a virus causing mild and acute respiratory distress, was thought to be spread from person to person through close contact (Moreland et al., 2020). On March 13, 2020, the Trump administration declared a nationwide emergency, and 2 days later, states began to implement shutdowns and other strategies to prevent the spread of the COVID-19 pandemic. These strategies included closing borders and schools, curfews, and banning crowds. At the time of the declaration, more than 1600 COVID-19 cases and 41 deaths had been confirmed in the US (CNN, 2020). Because each state and territory have the authority to implement its own policies, there was great variability in the types and timing of COVID-19 policies and restrictions. For example, in the beginning phases of the pandemic New York City and the state of Louisiana shut down their public-school systems, the state of Ohio called for the closing of restaurants and bars, the state of Washington restricted the size of public gatherings, and California issued a stay-at-home order. Between March and May 2020, 42 states and territories had implemented mandatory stay at home orders while others implemented advisory stay at home orders (CDC, 2022b; Cloud et al., 2020; Moreland et al., 2020). The timing of re-openings also varied, with the state of Alaska being the first state to lift stay-at-home orders on 24 April 2020 (Cloud et al., 2020).
Despite these COVID-19 reduction strategies, frontline workers in essential businesses and services, such as law enforcement officers (LEOs), were still required to report to work in person, which made them susceptible to workplace outbreaks and placed them at the highest risk of work-related exposure to COVID-19 due to the inability to adequately distance themselves from others (Gaitens et al., 2021; Lancet, 2020). In fact, the risk of severe COVID-19 for non-healthcare essential workers was found to be more than double that of non-essential workers (Mutambudzi et al., 2021). To minimize the spread of COVID-19, law enforcement agencies did seek creative ways to practice social and physical distancing, such as allowing some employees (e.g., command staff, detectives) to work from home (Police Executive Research Forum, 2021), but these practices were inconsistent. Thus, the proportion of LEOs who were able to fully work from home during stay at home orders is unknown.
Accordingly, several studies have focused on the differential risks and effects of COVID-19 among essential workers. Most of these studies have disproportionately focused on the healthcare workforce (Demirjian et al., 2020; Hennein et al., 2021; Pearman and HughesSmith, 2020; Shechter et al., 2020) or on racial/ethnic disparities in the essential workforce (Roberts et al., 2020; Rogers et al., 2022). A few studies have specifically focused on the increased stress experienced by LEOs and other essential workers due to COVID-19 (Cai et al., 2020; Frenkel et al., 2021; Newiss et al., 2022; Tehrani, 2022). To date, only one study has examined the characteristics of LEOs who died from COVID-19. Violanti et al., (2022) used data from the National Law Enforcement Officer Memorial Fund to determine the proportionate mortality and national rate of death from COVID-19 among LEOs in 2020. Findings revealed that, in 2020, the majority of law enforcement deaths (over 60%) were the result of COVID-19. More specifically, they found that LEOs who died from COVID-19 were more likely to be male, White, 50 years or older, and had 10 or more years of experience (Violanti et al., 2022). Although this study provided useful insight into LEO deaths resulting from COVID-19, the findings of this study are limited because data are restricted to COVID-19 deaths in 2020 and does not include individuals serving as volunteer/auxiliary officers and deputies who may have been granted arrest powers during the COVID-19 pandemic. Thus, the purpose of this study is to investigate the number and characteristics of LEOs who died from COVID-19 in 2020 and 2021 utilizing line of duty death statistics collected by the Officer Down Memorial Page (OMDP), a non-profit organization that records annual statistics of LEOs killed in the line of duty. Additionally, the present study examines the number of days between COVID-19 infection and death. It is important to study these patterns because LEOs are a critical component of public infrastructure tasked with maintaining public order, enforcing laws, and managing public safety (Bureau of Justice Statistics, 2022). These duties require interactions with the public and place officers at the highest risk of exposure as frontline essential workers (Centers for Disease Control and Prevention, 2022a). And while worker shortages have become exacerbated due to the pandemic (Frogner and Dill, 2022; Ochieng, et al., 2022), a shortage of LEOs “to protect and serve” could be detrimental to public order and safety.
Law enforcement involves many work-related hazards, including the risk of injury and exposure to disease. These hazards are likely one explanation for the shorter life expectancy of police officers compared to the general population (Violanti et al., 2013), although line of duty deaths have declined substantially in that past 50 years (White et al., 2019). But changes in patterns of crime, particularly during the lockdown period in the early months of the pandemic, may have altered the occupational risks associated with law enforcement and exacerbated the likelihood of officers contracting COVID-19. Generally, crime decreased during the lockdown period, with a return to pre-pandemic levels after this restriction was lifted (Abrams, 2021; Boman and Gallupe, 2020; Campedelli et al., 2021). The literature on calls for service during lockdown are inconsistent. At least one study noted an increase in calls for service (Dai et al., 2021), but others found no significant change in the number of service calls during the lockdown period (Ashby, 2020; Jennings and Perez, 2020). These studies and others did find that reports of certain types of crimes, such as domestic violence, increased during lockdown (Ashby, 2020; Bullinger et al., 2021; Hsu and Henke, 2021; Jennings and Perez, 2020; Leslie and Wilson, 2020; McCrary and Sanga, 2021; Mohler et al., 2020; Piquero et al., 2021; Sharma and Borah, 2022). Thus, law enforcement officers responding to these domestic situations may have been at an increased risk of COVID-19 exposure due to close interactions with unmasked, infected individuals.
Another change in crime reporting concerned calls for LEOs to respond to violations of COVID-19 policies for protective and preventive behaviors (e.g., stay at home orders; face mask requirement; public gathering restrictions; Mills et al., 2021; White and Fradella, 2020). Responding to these calls may have increased an officer’s risk of COVID-19 exposure, as some responding officers were coughed or spit on by civilians. However, these protective and preventive policies varied by state, as did law enforcement’s response to these violations. For example, in Texas, stay at home orders were advisory, but not mandated. As a result, violations of these orders may have been less likely to involve law enforcement. But in states like California and New York, stay at home orders were mandatory for all persons not deemed to be essential workers, so violations may have been more likely to be reported to and investigated by law enforcement. In states like Florida, Georgia and Pennsylvania, a mixture of both mandatory and advisory stay at home orders were implemented (Moreland et al., 2020), indicating the complexity of these policies and the inconsistent response of law enforcement across jurisdictions. Similarly, face masks policies varied by state—some states required masks, some recommended masks, and 15 states had no mask policy (Fischer et al., 2021)—resulting in discrepancies in types of service calls and risk of infection. The politicization of the pandemic also added to the disparate response by law enforcement to such policy violations (Jackson et al., 2021). As states began to relax their social and physical distancing restrictions and individuals within the United States were able to attend larger public gatherings (e.g., protests and demonstrations, political rallies, sporting events), LEOs were attending these events as part of their job duties. However, there is some evidence that these public gatherings, specifically protests, also altered patterns of crime, as they were associated with increases in certain types of crime, primarily violent crimes (Koppel et al., 2021; Rosenfeld et al., 2021).
The usual patterns of crime may also factor into the risk of exposure faced by LEOs. Crime data show that most arrests are of young, White males, although Black and Hispanic males are disproportionately arrested (Federal Bureau of Investigation, 2020b). Similarly, young, White males were also less likely to comply with pandemic protective and preventive behaviors (Bish and Michie, 2010; Gette et al., 2021; Green et al., 2021), thus potentially increasing officer risk of infection. There is also an association between crime and low income, minority communities (Sampson and Raudenbush, 2001; Sun et al., 2004). Although crime reports and arrests declined during the initial period of the pandemic, there is variability in this pattern by place, to the extent that some areas and neighborhoods with higher rates of crime either maintained or increased their previous levels. These places also tended to be disproportionately clustered in low income, minority neighborhoods (Andresen and Hodgkinson, 2021; Drake et al., 2022; Campedelli et al., 2020; Moise and Piquero, 2021). For officers responding to reports of crime in these areas, there may have been a heightened risk of infection. Such an assumption is plausible because COVID-19 tended to disproportionately affect disadvantaged neighborhoods (Pierce et al., 2021; Samuels-Kalow et al., 2021).
Another work-related risk affecting LEOs is exposure to stressful and traumatic events. Extensive research has shown that exposure to stressful and traumatic events could negatively affect physical health outcomes (Thoits, 2010). For LEOs in the United States and worldwide, sources of stress during the pandemic involved concerns over infection (both self and their families) along with a lack of communication from management (e.g., police chiefs; Charman and Bennett, 2022; De Camargo, 2022; Frenkel et al., 2021; Grover et al., 2020; Newiss et al., 2021). More specifically, De Camargo’s (2022) research utilizing police officer interviews found that officers in the United Kingdom reported increased levels of anxiety surrounding fears of their families and themselves contracting the virus. Combining these work-related risks with the additional stressors of the pandemic may have intensified the mental health challenges experienced by officers, as well as shaped their susceptibility of infection.
Method
Data and Measures
Data were drawn from the Officer Down Memorial Page’s (ODMP) website. ODMP is a non-profit organization that collects data on law enforcement officials who have died while on duty. Specifically, this website honors these individuals and provides an opportunity for citizens (e.g., friends and family) and other officers to memorialize their sacrifices (Officer Down Memorial Page, 2021). Criteria for inclusion includes any law enforcement officer in the United States and its territories whose death was the result of the following: a felony murder, accidental, natural, health-related (including COVID-19), previous work-related injuries, and off-duty LEOs working in an official law enforcement capacity. Submissions for the ODMP database are reviewed by a member of its Board of Directors. If the member is unable to decide, the submission is reviewed by the majority of the full board whose decisions are final unless there is sufficient reason for re-review. Any previous submissions found to not meet ODMP’s criteria are removed from the website.
It has been estimated that, since 1776, more than 25,000 law enforcement officials have died while on duty, according to Officer Down Memorial Page (2021). The ODMP defines law enforcement officer as those employed with a municipal, city, county, state, or federal agency and who have the power of arrest; correctional and detention officers engaged in the custody and security of offenders; and military police officers (Officer Down Memorial Page, 2021). Data were restricted to the reported law enforcement officer deaths due to COVID-19 between January 1, 2020, and December 31, 2021. Demographic characteristics of LEOs obtained included race/ethnicity, sex, age, years of service, state, military service and branch, days between contraction and death, and organization type. Month and day of week of death were also obtained and aggregated by season (winter, spring, summer, and autumn/fall). State of death was also aggregated into Census Bureau regions (northeast, Midwest, south, and west).
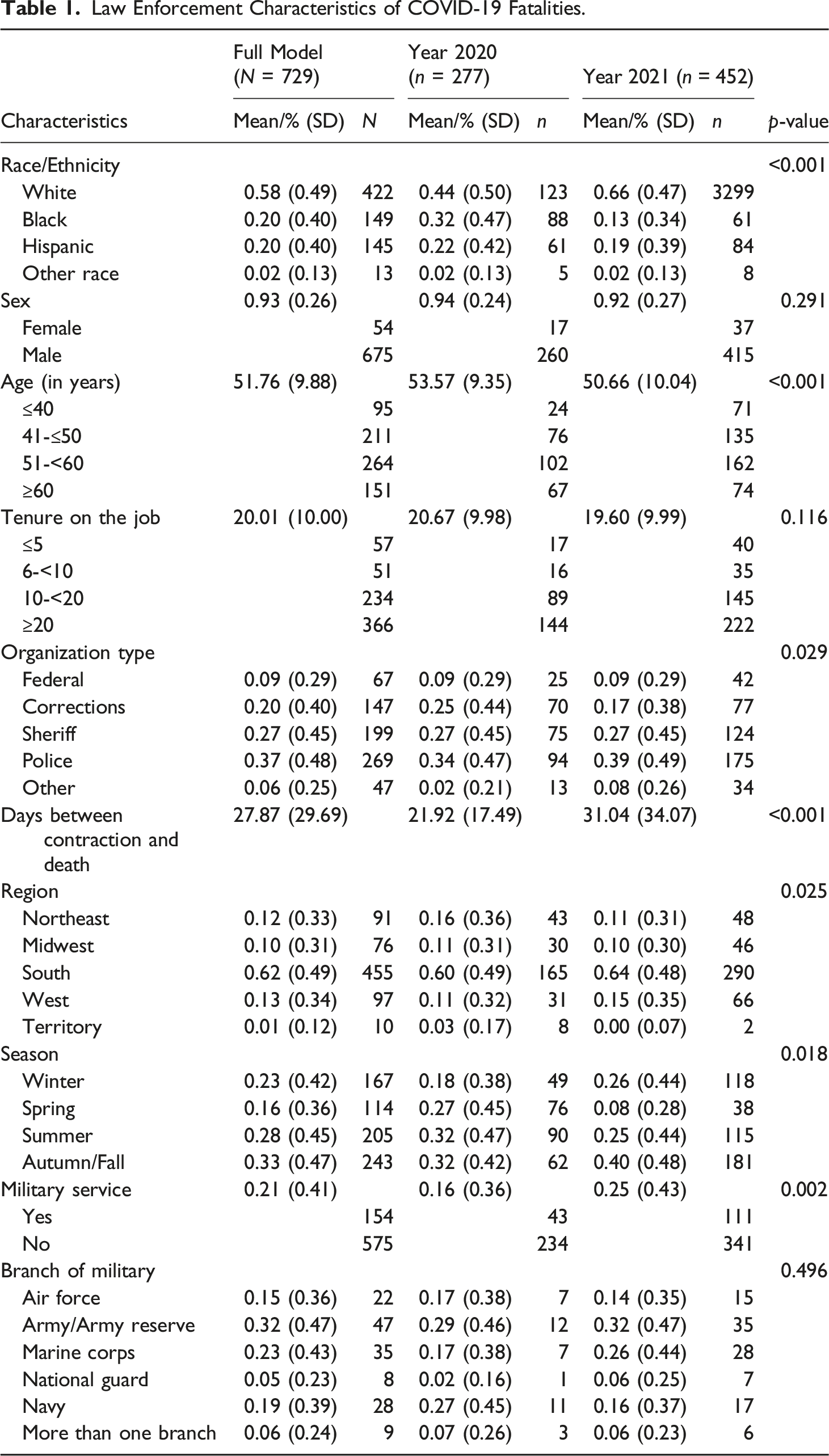
Law Enforcement Characteristics of COVID-19 Fatalities.
Results
COVID-19 deaths among LEOs accounted for 54% of reported line of duty deaths in 2020 and 48% in 2021. Table 1 shows the number and share of officer COVID-19 deaths for 2020 and 2021, as well as how these statistics varied by several characteristics. More than 700 law enforcement officials died from COVID-19 in 2020 and 2021, with a larger share (62%) occurring in 2021. Male officers accounted for about 93% of these deaths overall. The share of COVID-19 deaths among female officers more than doubled, from 17 deaths in 2020 to 37 deaths in 2021; however, COVID-19 deaths among male officers increased more than 250%, from 260 deaths in 2020 to 415 deaths in 2021.
More than half of the total deaths occurred among White officers (58%) relative to other racial/ethnic groups (p < 0.001). However, there are some marked differences in deaths by race/ethnicity by year. White officers accounted for 44% of deaths in 2020, but the number of deaths nearly doubled and the share increased to about two thirds in 2021. Conversely, Black officers accounted for about one third of deaths in 2020, but the share dropped to 13% in 2021. The number and share of deaths among Hispanic officers and those officers of some other race remained relatively constant over the 2-year period.
The mean age of those officers who died from COVID-19 during the 2-year period was nearly 52 years of age. The mean age was slightly older in 2020 at more than 53 years of age but declined to 50.66 years in 2021 (p < 0.001). Tenure on the job averaged 20.01 years, but also varied by year at 20.67 years in 2020 and 19.60 years in 2021. The average number of days between contraction and death for the 2-year period was about 28 days (p < 0.001). In 2020, this average was shorter at 21.92 days, but increased by nearly 10 days in 2021.
There were also differences in the share of officer deaths based on type of organization employed (p < 0.05). More than 80% of COVID-19 deaths occurred among officers employed in correctional, sheriff, and police organizations. The largest decline in the share of officer deaths—8 percentage points—is found among those employed in corrections, which accounted for 25% of deaths in 2020 but 17% in 2021. Law enforcement officers working in policing represented 37% of COVID-19 deaths, with the share of deaths increasing 5 percentage points in 2021.
Deaths also varied by month and season (p < 0.05), similar to total COVID-19 deaths (see Figure 1). For both years, officer COVID-19 deaths tended to follow the national trends, with monthly differences likely due to the timing of the pandemic waves and loosening of pandemic protocols. The largest share of deaths in 2020 occurred in April and December (18% each), coinciding with the early stages of the pandemic and holiday gatherings, respectively. But the greatest share of deaths in 2021 coincided with the Delta variant surge in August (19%) and September 2021 (23%). Monthly Trend in COVID-19 deaths, total population and law enforcement officers. Note: Total COVID-19 deaths in the US by month were obtained from the APM research lab and the US centers for disease control and prevention.
Figure 2 shows regional and state differences in the number and share of deaths (p < 0.05). For the 2-year period, 62% of officer deaths occurred in the south (60% in 2020 and 64% in 2021). One state—Texas—accounted for nearly one quarter of these deaths in the 2-year period. In 2021, the share of officer deaths declined by 5 percentage points in the northeast and 1 percentage point in the Midwest over the previous year. Officer deaths in the west increased by roughly 4 percentage points in 2021. Although they represented the smallest share, officer COVID-19 deaths in territories decreased from 2020 to 2021. Distribution COVID-19 fatalities by location 2020-2021.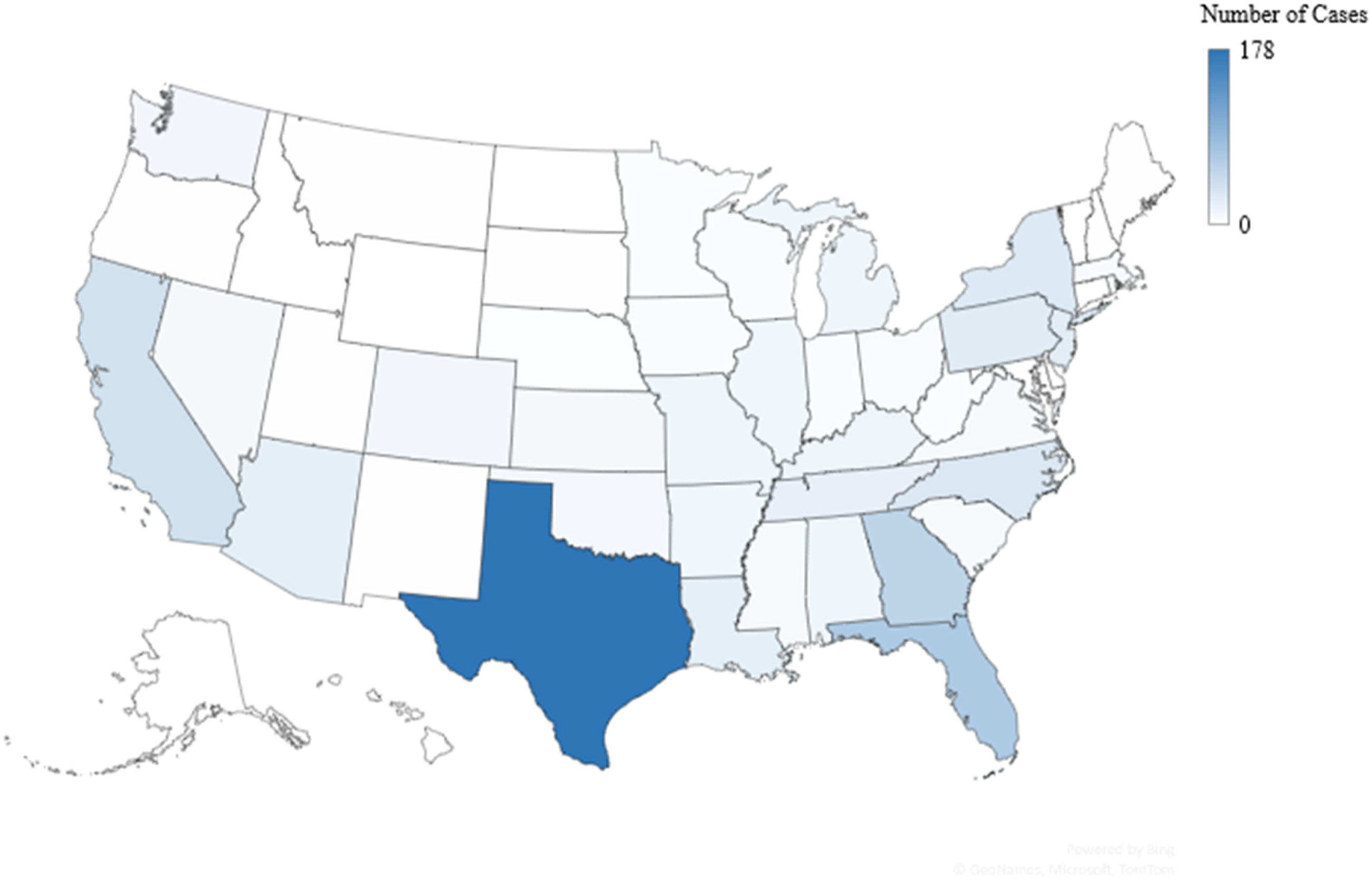
Discussion and Conclusion
This study examined characteristics of LEOs who died from COVID-19 in the line of duty for the years 2020 and 2021. These characteristics are somewhat similar to those of the LEO workforce as COVID-19 deaths affected a larger share of officers who were male, White, and older. It is not surprising that more deaths occurred among male officers than female officers and among White officers relative to officers of color, since law enforcement is a predominantly male and White occupation (Hyland and Davis, 2021). These trends also aligned with COVID-19 deaths in the total population as the number of deaths were higher for males and for Whites (Centers for Disease Control and Prevention, 2022c). However, COVID-19 deaths have disproportionately affected racial/ethnic minority groups (Hill and Artiga, 2022). Similarly, this study found that the share of officer COVID-19 deaths was disproportionately higher for officers of color; yet, officers of color are underrepresented in law enforcement (Brooks, 2021; Hyland and Davis, 2021). More specifically, Black and Hispanic officers each accounted for 20% of COVID-19 deaths in the 2-year period. For Black officers, the share of deaths declined significantly in 2021. These patterns were likely influenced by race and gender differences in preventive behaviors (e.g., mask wearing, use of sanitizers). Females and persons of color tended to comply with these behaviors (Bish and Michie, 2010; Choi et al., 2022; Gette et al., 2021; Green et al., 2021).
LEOs who died from COVID-19 were more likely to be older—and older than the estimated median age of officers of 40 years (Bureau of Labor Statistics, 2022). This finding is also comparable to national trends where COVID-19 deaths have been greater among older adults (Centers for Disease Control and Prevention, 2022a). However, among other types of essential workers, older workers were less likely to contract COVID-19 (Houlihan et al., 2020). And while the mean tenure of service among those officers who died from COVID-19 was more than 20 years, this finding is likely due to the age of the officer. Nevertheless, these findings on age and tenure may alter the general trends on officer deaths in the line of duty as these deaths tend to be greater among younger and less experienced officers (Federal Bureau of Investigation, 2020a).
This study also found that COVID-19 deaths of officers were greatest in the south. The northeast region initially had the highest rates of infection and largest number of deaths nationally, but this trend shifted to the south (Jones, 2022). However, given that the ratio of officers to inhabitants in the south is above the national average (Federal Bureau of Investigation, 2020c), it seems that face to face interactions between officers and civilians could have been reduced, indicating that other factors likely contributed to officer COVID-19 deaths. One possible explanation for this regional difference may lie in the population characteristics of the south. Southern states tend to be disproportionately racial/ethnic minorities, rural, and poor—three factors linked to lower compliance with COVID-19 prevention policies, such as wearing face masks and vaccine uptake (Callaghan et al., 2021). These factors, when paired with lower policy compliance, may have increased officer exposure to COVID-19. Additionally, the south is characterized as politically conservative, which is also associated with lower compliance of COVID-19 prevention policies (Callaghan et al., 2021; Kahane, 2021; Sun and Monnat, 2022). States with politically conservative leadership also had less restrictive social and physical distancing policies (Kahane, 2021), which may have inadvertently placed officers at a greater risk of COVID-19 exposure. And even though federal guidelines placed LEOs, as essential non-healthcare workers, in one of the earliest prioritization groups (Tolbert et al., 2021), this priority did not necessarily equate to their vaccine uptake, especially in places with greater vaccine hesitancy, such as the southern region of the country.
Similar to Violanti et al.’s (2022) study, LEOs working either for police or sheriff’s departments and correctional facilities accounted for a higher percentage of COVID-19 deaths for both years. This finding may be explained by several factors. First, even during the pandemic lockdown, prisons and jails continued to see individuals flow in and out of these facilities resulting from arrests, facility transfers, and early releases (Nowotny et al., 2021). This influx of individuals in and out of the facilities may have exacerbated both sheriff’s deputies and correctional officers’ exposure to COVID-19. A second potential explanation could be limited access to personal protective equipment (PPE) within these facilities, as early shortages included protective eyewear and N95 masks (Jennings and Perez, 2020). Due to the already limited resources available to both those working and incarcerated in these facilities (Nowotny et al., 2021), it would not be surprising that some prisons and jails may not have enough resources, such as masks and hand sanitizers, for both groups. A third explanation for these findings could be reluctance of both officers and incarcerated individuals in getting the COVID-19 vaccine. Research by Khorasani et al. (2021) revealed that although most jail staff (including medical or mental health staff) in their study showed an interest in getting the vaccine, front-line correctional officers were more reluctant to receive the vaccine. Additionally, they found that those incarcerated were less willing to get the vaccine; thus, potentially increasing the risk of officers and other staff in contracting the virus.
Although line of duty deaths have declined and are generally rare, the pandemic increased these numbers more than 50% over 2019 and about 45% over the average annual deaths for the years 2011–2019 (National Law Enforcement Officer Memorial Fund, 2022). LEO line of duty deaths due to COVID-19 represent the largest increase in officer deaths since the terrorist attacks in 2001 (White et al., 2019).
Limitations
This study, to our knowledge, is the one of two studies exploring characteristics of COVID-19 deaths among law enforcement officers. However, this study is not without its limitations. First, interpreting the results should be approached with caution as the data source (ODMP) is limited to reported deaths classified as due to COVID-19. Not all line of duty deaths are reported to the ODMP, resulting in some underreporting in the number of line of duty deaths, and the missing data may skew the general patterns and associations. The ODMP uses strict criteria for classifying line of duty deaths, thus reliability and validity issues should be minimal, although misclassification of cause of death is not improbable. Second, this study only focused on deaths directly due to COVID-19. The increased reports of domestic situations, and their volatile nature, during the earliest months of the pandemic may have led COVID-19 to function as an indirect cause of death for officers who responded to these situations. Similarly, job stress experienced by officers has been linked to work-related injuries and deaths (Ferguson et al., 2011), and the increased stress placed on officers due to COVID-19 may have indirectly contributed to other types of deaths (e.g., accidents). Another unknown factor—the presence of other comorbidities (e.g., heart disease, diabetes)—may also have increased the risk of death from COVID-19 (Hartley et al., 2011; Gu et al., 2014). More specifically, prior research has shown that police officers have one of the poorest health profiles of any occupation. A study by Hartley et al. (2011) found that, when compared to the general employed population, police officers were more likely to sleep less than 6 hours a day, had higher average total cholesterol levels, and higher levels of non-traditional risk factors associated with cardiovascular disease. Third, this study only provides a description. Future research could explore how state-level characteristics, such as length of mask mandate in public settings, vaccination priorities that explicitly included officers in the first round, and political conservatism, may have shaped the risk of exposure to COVID-19.
Recommendations and Conclusion
These findings have several policy and practice implications to promote the safety and wellbeing of LEOs, and therefore the public. First, law enforcement agencies and other entities employing LEOs should continue to implement infection control strategies, such as providing officers with the necessary resources to reduce COVID-19 incidence (Jennings and Perez, 2020). These resources include personal protective equipment (PPE), such as masks, which were found to decrease infection rates in essential healthcare workers when COVID-19 rates were increasing in the general population (Lan et al., 2020). Additionally, employers should encourage preventive behaviors, such as testing protocols, to minimize the risk of contraction. Due to the risk of infectious disease (e.g., Hepatitis B, HIV) that officers faced prior to the pandemic, law enforcement agencies and employers already have existing protocols and training for exposure to infection (Jessop et al., 2014). However, these existing protocols and trainings may need to be modified. One potential modification is the suggested partnerships between law enforcement and healthcare providers to create effective training and pool resources (Jennings and Perez 2020). Another preventive measure concerns the COVID-19 vaccine, which has been found to reduce infection incidence among officers (Mourtgos and Adams, 2021). Some employers require the vaccine, and such requirements should not only align with existing vaccine mandates and exemptions, but be accessible and free (International Association of Chiefs of Police, 2021). Similarly, COVID-19 testing after potential exposure should also be accessible and free. To increase vaccination compliance, officers should be ethically educated on the vaccine benefits (Berkman et al., 2022). Providing incentives, such as additional vacation days and free gym memberships, to fully vaccinated officers may also reduce infection risk of officers and the public. While research on the efficacy of such incentives is inconsistent, they may be effective practices for the vaccine reluctant (Carpio et al., 2021; Fishman et al., 2022; Serra-Garcia and Szech, 2022).
Second, encourage exposed and infected officers to stay home until cleared to return to work per the most current CDC guidelines. One potential strategy to ensure compliance with this preventive behavior is to consider special COVID-19 medical leave. While law enforcement officers and other first responders may be excluded from extended medical leave due to COVID-19, the inclusion of LEOs in such a policy could reduce infection incidence by allowing officers to receive pay while quarantined. Access to medical leave is important for workers in low wage, high stress jobs. COVID-19, like workplace injuries, may have increased officer medical treatment (and thus out of pocket expenses) and days of work lost. This assertion may especially affect those who recovered from a COVID-19 infection as they may experience other health issues (i.e., Long COVID). Although needed, special COVID-19 medical leave for officers may also pose an issue for departments experiencing officer shortages prior to the pandemic. The Police Executive Research Forum (2021) reported that responding agencies hired fewer officers and both retirements and resignations increased (also see Charman and Bennett, 2022). Both prior concerns with officer shortage and the challenges of the current pandemic have resulted in “healthy” officers working longer shifts which has been shown to increase officer burnout. Additionally, officer burnout has been shown to contribute to both anxiety and depression among officers (Davies and Brooks, 2022; Martin-Howard, 2022; Newiss et al., 2022).
Third, provide mental health services and resources to potentially alleviate work-related stressors. Officers already face mental health challenges due to high stress and exposure to trauma, which can lead to post-traumatic stress disorder (PTSD) and suicide ideation (Violanti et al., 2017, 2018). Preliminary research has shown that COVID-19 likely elevated stress and anxiety and increased the risk of PTSD (Martin-Howard, 2022; Newiss et al., 2021). For example, Martin-Howard (2022) found that a sample of Black female correctional officers employed at Rikers’ Island Jail reported increased feelings of stress as well as developing chronic health challenges (i.e., high blood pressure and sleep apnea). Another consideration is that mental health issues may lead to poorer physical health (Ramey et al., 2011; Gu et al., 2012), so wellness offerings related to diet, exercise, and sleep may also be beneficial and improve overall wellbeing. Not only should adequate support be provided, but also various types of support (e.g., yoga, therapy, coping skills) due to the complexity of factors shaping mental health needs and related outcomes (Stogner et al., 2020; Drew and Martin, 2020). Mental health services and resources should also consider the delayed psychological effects linked to trauma, and thus monitor the long-term mental health of officers, as well as identify those officers at greater risk of trauma exposure.
Fourth, increase options for remote work. Officers in many areas are already using technology to work remotely, such as remote-controlled drones for monitoring inmates, search-and-rescue drones and bomb-disposal robots (Simmons, 2019). Expanding this technology for other job responsibilities may reduce unnecessary interactions with others but may also allow some officers to potentially work from home. Research has already shown that usage of such technology is promising, with search-and-rescue drones covering larger areas than human officers and bomb-disposal robots accessing areas that may be difficult for human officers to reach (Simmons, 2019).
And a fifth and final recommendation would be for government policies and strategies to increase the officer workforce. Many states have focused on strategies to increase healthcare workforce in the age of COVID-19, but LEOs could also benefit from similar strategies. As previously mentioned, shortages in law enforcement have implications for officer burnout which, in turn, has been shown to increase levels of anxiety and depression among officers and officer turnover.
Other challenges in recent years have led policing to become a less attractive, and pervasively stigmatized, career (Ashworth and Kreiner, 2014; Chatterjee and Ryan 2020). Recently, Chatterjee and Ryan (2020) explored whether individuals described policing in stigmatizing terms and found they had more negative perceptions and greater distrust in police officers. The overall wellbeing and safety of officers, including the prevention of COVID-19, should remain a top priority for employers. Practices promoting officer well-being, such as those proposed, may improve job satisfaction (Wolfe et al., 2018) and employer recruitment and retention efforts.
Footnotes
Author Notes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.