
Abstract
This research examines perceived physical health, psychological distress, and social support among prison officers in the United Kingdom. The study found that prison officers reported poor perceived physical health and a high level of psychological distress. There were significant correlations between measures of perceived physical health and a measure of psychological distress (indicating that as perceived physical health decreased, psychological distress increased). There was some evidence that social support from within the prison moderated the relationship between perceived physical health and psychological distress, whereas social support from significant others did not. Future research and clinical implications of these findings are considered.
Introduction
In England and Wales, Her Majesty’s Prison Service employs more than 43,000 prison staff, of whom 25,000 are prison officers (Coyle, 2005). Prison officers work with more than 80,000 prisoners, across 138 prisons. The workplaces vary in demands on prison officers and have been described as “emotional labour” (Crawley, 2006). The National Audit Office’s (2004) report, The Management of Sickness Absence in the Prison Service, in the United Kingdom suggested that the work of prison officers could lead to negative physical and psychological health consequences. Research in the United States has found that prison officers suffer a higher rate of physical health problems than people in other occupations (Cheek & Miller, 1983; Woodruff, 1993), and higher levels of self-reported health symptoms have been found to be associated with higher levels of psychological distress (Dollard & Winefeld, 1998).
A number of studies have documented the emotional reactions of prison staff to their work and have used various different terms to refer to their psychological health difficulties. These terms include work stress (Armstrong & Griffin, 2004; Cullen, Link, Wolfe, & Frank, 1985; Grossi & Berg, 1991), stress (Cheek & Miller, 1983; Lindquist & Whitehead, 1986; Owen, 2006), burnout (Cieslak, Korczynska, Strelau, & Kaczmarek, 2008; Drory & Shamir, 1988; Griffin, Hogan, Lambert, Tucker-Gail, & Baker, 2010), tedium (Shamir & Drory, 1982), psychological distress (Dollard & Winefeld, 1998; Johnson et al., 2005; Liebling, Tait, Durie, Stiles, & Harvey, 2005; Long & Vogues, 1987), and trauma (Wright, Borrill, Teers, & Cassidy, 2006). Levels of psychological distress have been found to be high (Dollard & Winefeld, 1998; Liebling et al., 2005) and have been reported to be higher than those in other normative samples (Johnson et al., 2005; Long & Vogues, 1987).
Not only has research examined the extent of prison officers’ psychological and health difficulties but also has documented their sources of stress (i.e., stressors; Armstrong & Griffin, 2004; Dowden & Tellier, 2004; Griffin, 2006; Schaufeli & Peeters, 2000). The most prominent factors to contribute to stress in prison work are role problems; stressful contact with peers, supervisors, and prisoners; work overload; and the poor social status of the job (Schaufeli & Peeters, 2000). Moreover, a lack of social support was in itself a source of stress among prison officers (Schaufeli & Peeters, 2000).
Social support is an important construct to consider in the light of these challenges to the physical and psychological well-being of prison officers. It has been argued that strong ties between individuals can protect them from the pathogenic effects of stressful life events (Berkman & Syme, 1979; Cobb, 1976; Cohen, Gottlieb, & Underwood, 2000).
Research has been carried out in countries other than the United Kingdom examining social support among prison officers (Armstrong & Griffin, 2004; Auerbach, Quick, & Pegg, 2003; Cieslak et al., 2008; Cullen et al., 1985; Dignam, Barrera, & West, 1986; Dignam & West, 1988; Dollard & Winefeld, 1998; Drory & Shamir, 1988; Gerstein, Topp, & Cornell, 1987; Grossi & Berg, 1991; Holahan & Moos, 1982; Lambert, Altheimer, & Hogan, 2010; Lambert & Hogan, 2009; Lindquist & Whitehead, 1986; Owen, 2006; Peeters, Buunk, & Schaufeli, 1995; Shamir & Drory, 1982). Most of these studies have examined the relationship between social support and psychological health, whereas a minority have examined the relationship between social support and physical health (Armstrong & Griffin, 2004; Dignam & West, 1988; Dollard & Winefeld, 1998). Only one study has been carried out in the United Kingdom (Wright et al., 2006). Generally, these studies vary in whether they take social support as the main focus of their research or include it as one predictor variable among a set of others.
Studies that have included social support as just one predictor, along with other personal and environmental variables, have been equivocal in their findings. Some have found that social support has been associated with measures of work stress or burnout (Armstrong & Griffin, 2004; Drory & Shamir, 1988; Lindquist & Whitehead, 1986; Owen, 2006), whereas others did not find a correlation with measures of either work stress, burnout, or trauma (Gerstein et al., 1987; Grossi & Berg, 1991; Wright et al., 2006). Furthermore, a third finding is that social support might play a detrimental rather than a beneficial role in relation to stress and burnout. Cullen et al. (1985), for example, found that a high level of social support was associated with higher stress and burnout.
Similarly, studies that have examined specific models of social support have also been equivocal in their findings (Dignam et al., 1986; Dignam & West, 1988; Peeters et al., 1995). There has been some support for a “direct” model of social support on burnout (Dignam & West, 1988), some support for a “stress-buffering” role (a model postulates that social support is beneficial for individuals only when they experience stressor; Dollard & Winefeld, 1998), and some support for an indirect model (an indirect model postulates that social support indirectly influences health outcomes through its direct influence on reducing perceived or actual stressors; Dignam et al., 1986). However, other research did not find a direct effect (Dignam et al., 1986), a “stress-buffering” role (Dignam & West, 1988), or support for an indirect model (Dignam & West, 1988). Furthermore, Peeters et al. (1995), who tested the buffering role of social support, concluded that received instrumental support aggravated the relationship between stressful life events and negative affect, instead of acting as a buffer to the negative consequences of experiencing stressful life events.
When previous research has examined social support in relation to psychological and physical health, physical health has been conceptualized as the final outcome in the model, an outcome associated with poor psychological health (Dignam et al., 1986; Dignam & West, 1988). However, it could be argued that perceived physical health may contribute to increased levels of psychological distress. Indeed, individuals differ in their psychological responses to physical health difficulties, and health problems can lead to psychological distress (White, 2001). No previous research with prison officers has examined physical health as an independent variable and its possible association with social support and psychological health. Moreover, research among prison officers has predominantly measured social support within the workplace, and only a handful of studies have examined different forms of social support, both work-based social support and family support (Gerstein et al., 1987; Grossi & Berg, 1991; E. G. Lambert et al., 2010; Triplett, Mullings, & Scarborough, 1996). This article sets out to examine perceived physical health and psychological distress among prison officers and to consider the role of social support in relation to these variables. This present research has three aims:
To ascertain the level of perceived physical health difficulties and level of psychological distress among prison officers;
To examine the correlation between perceived physical health, psychological distress, and perceived social support among prison officers; and
To consider whether or not social support moderates the relationship between perceived physical health and psychological distress.
Method
Design
This study used a cross-sectional design and correlation and multiple regression analyses. It used group comparisons to ascertain whether there were any group differences on the measures used.
Participants
One hundred prison officers took part and were recruited through convenience sampling across all areas within one male prison in the United Kingdom. Officers were eligible to take part if they had direct contact with prisoners; non-discipline staff were excluded. Five officers who were approached refused to take part.
Instruments
Demographic information was gathered for age, gender, ethnicity, officer grade, and length of time in service. In addition, the following measures were included:
Perceived physical health
The Medical Outcome Study–Short Form 36 Version 2 (SF-36 II; Ware, Kosinski, & Dewey, 2002) was used to measure perceptions of physical health. Four of the subscales are reported here: Physical Functioning (which measures limitations in physical activities due to health problems), Role Physical (which measures limitations in usual role activities because of physical health problems), Bodily Pain (which measures the degree of perceived body pain), and General Health (which measures perceived general physical health). Scores were coded for each dimension, summed, and then transformed into scaled scores ranging from 0 to 100 (0 = worst possible health status; 100 = best possible health status).
Perceived social support from a significant other (Significant Other Scale [SOS] adapted)
An adapted version of the SOS (Power, Champion, & Aris, 1988) was used as a measure of perceived social support from a significant other. The scale is comprised of 10 items that are scored on a 7-point Likert-type scale from 1 to 7 (1 = never, 7 = always), and the participant rated the scale in relation to the person they felt closest to. Given the adaptations, a principal component analysis (along with the items that comprise the Prison Social Support Scale [PSSS], discussed in the following section) was carried out and the 10 items from the SOS formed one factor. Cronbach’s alpha showed high internal reliability (α = .923.).
Perceived social support within prison (PSSS)
A brief three-item scale was created to measure support within prison (PSSS). The three items that comprise the scale are as follows: (a) How supported do you feel by other peers/colleagues in this prison? (b) How supported do you feel by your line manager in this prison? and (c) How supported do you feel by the governor grades in this prison? Each of these items was scaled from 1 to 10 (1 = not at all supported; 10 = completely supported). All three items from the PSSS formed one factor. Cronbach’s alpha showed high internal reliability (α = .769).
Psychological distress
Psychological distress was measured using the 12-item self-report instrument, the General Health Questionnaire (GHQ-12; Goldberg & Williams, 1988). It measures minor mental health problems such as depression and anxiety. The GHQ-12 was scored using the 0,1,2,3 method. An overall score greater than 12 indicates clinical caseness; a higher score indicates higher psychological distress.
Procedure
Participants were asked whether they would like to take part in the study, and if they agreed, they were given a questionnaire pack in an envelope that contained a participant information sheet, consent form, and the questionnaires. An opportunity for questions was also given before and after completion.
Analysis of Data
Data were analyzed using SPSS 14.0. Descriptive statistics were generated to describe the sample and for each of the main variables. Group comparisons were carried out (using parametric or non-parametric tests) to ascertain whether there were any differences (by demographic and occupational variables) on perceived health, psychological distress, and social support variables. Univariate correlations (using Spearman’s Rho) were generated before testing the models set out in this research. Each of the models was tested using the forced entry method of multiple regression.
Results
Descriptive Statistics of the Sample
The majority of participants were male (79%) and were White British (78%). More than 40% were aged between 40 and 49 and 32% were aged between 30 and 39. Of those sampled, the majority of the participants were basic grade prison officers (77%). The participants varied in their length of time in service. Of the sample, 29.3% were relatively junior and had worked between 1 year and 3 years in the prison service, and 39.4% were senior and had worked 10 years or more.
Descriptive Statistics for the Variables
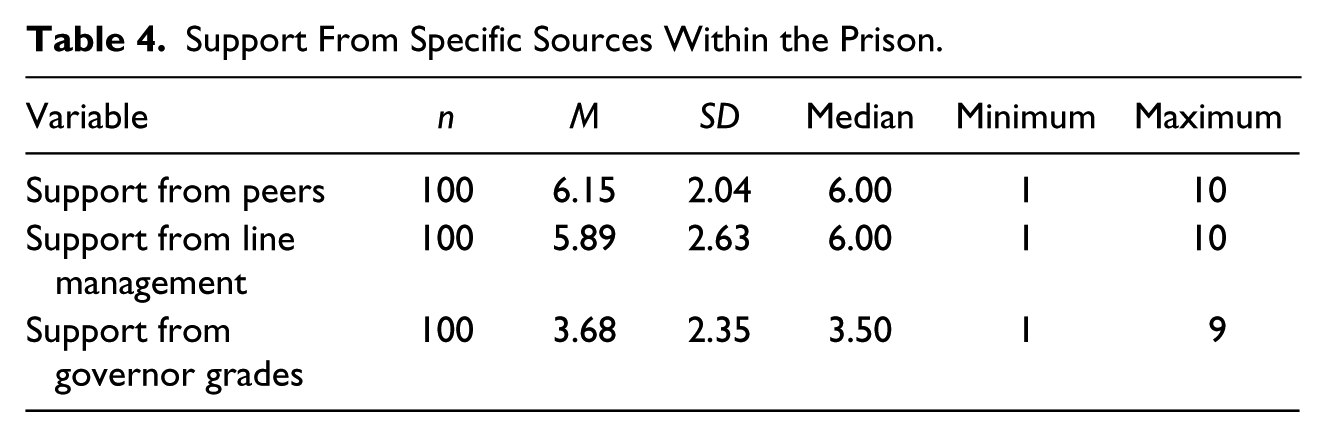
Table 1 presents descriptive statistics for the physical health dimensions of the SF-36 and the GHQ-12. On the SF-36, participants scored lowest on general health and highest on physical functioning. On the GHQ-12, the mean score was 13.06 (SD = 5.39). Norm-based scores were calculated and the percentages of cases above or below the norm (score of 50) were examined. As Table 2 shows, 83.8% scored below the U.S. average on general health, 50% scored below average on bodily pain, 52% scored below average on role physical, and 32% scored below average on physical functioning. In all, 56.6% (n = 56) reached caseness on the GHQ-12. Table 3 presents the descriptive statistics of the social support variables. These scales ranged from 1 to 7 for the SOS and 1 to 10 for the PSSS. Table 4 presents the descriptive statistics of the three items that were included with the PSSS measure. The mean score for support from peers was the highest, followed by support from line managers; the lowest mean score was for support from senior management.
Descriptive Statistics for SF-36 II and GHQ-12.

Note. SF-36 II = Medical Outcome Study–Short Form 36 Version 2; GHQ-12 = General Health Questionnaire.
Percentages of Cases Above and Below the Norm (SF-36 II).
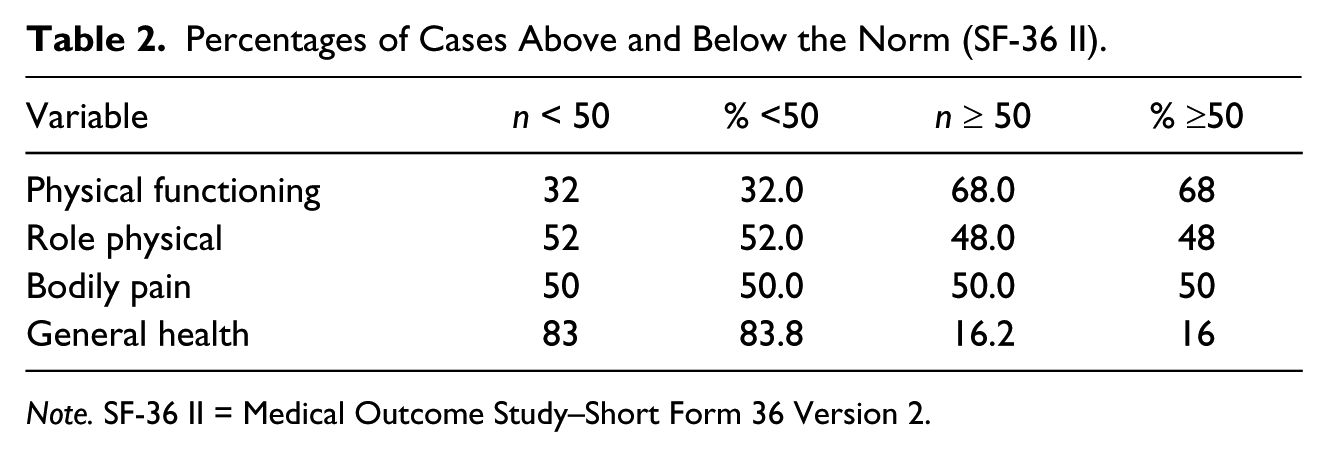
Note. SF-36 II = Medical Outcome Study–Short Form 36 Version 2.
Descriptive Statistics for Social Support Variables.

Note. SOS = Significant Other Scale; PSSS = Prison Social Support Scale.
Support From Specific Sources Within the Prison.
Comparison of Different Groups on the Variables
It was important to ascertain whether or not there were differences according to age, gender, ethnicity, officer grade, and length of time in service on the physical health dimensions of the SF-36, the GHQ-12, and the social support variables. The analyses revealed that participants who were older reported lower scores on the measure of bodily pain (i.e., they reported higher bodily pain) than younger participants (U = 725, p = .009), that participants who had worked ≥7 years reported lower scores on this measure of bodily pain (i.e., they reported higher bodily pain) than those who had worked ≤6 years (U = 94, p = .044), that participants who had worked ≥7 years reported lower scores on this measure of general health (i.e., poorer general health) than those who had worked ≤6 years, t(98) = 2.22, p = .029) and that non-White officers reported a lower level of psychological distress than White officers, although the number of non-White participants is small, t(97) = 2.27, p = .025. These differences will be taken into account when carrying out the regression analyses.
Univariate Correlations
Table 5 presents the univariate correlations between the main variables. For consistency, Spearman’s Rho was carried out, because the majority of the variables were non-normally distributed. To recap, a higher score on the physical health dimensions indicated better perceived physical health, a higher score on the GHQ-12 indicated a higher level of psychological distress, and a higher score on the social support measures indicated higher levels of perceived social support. There was a significant negative correlation between each of the four measures of physical health and the GHQ-12 (physical functioning, r = −.202, p = .045; role physical r = −.366, p = .001; bodily pain r = −.328, p = .001; and general health, r = −.359, p = .001). There was a significant negative correlation between scores on the PSSS and scores on the GHQ-12 (r = −.401, p = .001), a significant negative correlation between scores on general health and scores on the SOS (r = −.255, p = .011), and a significant positive correlation between scores on bodily pain and scores on the PSSS (r = .211, p = .035).
Univariate Correlations.

Note. SOS = Significant Other Scale.
p < .05. **p < .001.
Moderator Models
Multiple regression analyses were carried out to determine whether or not social support moderated the relationship between perceived physical health and psychological distress. A total of eight models were tested: four models examining SOS (one model for each dimension of physical health) and four models examining PSSS (one model for each dimension of physical health). Because differences were found according to age, length of time in service, and ethnicity, these variables were included within the models. Six of the eight models yielded non-significant interactions. There were no significant interaction effects of physical functioning and SOS (β = −.122, p = .249), role physical and SOS (β = −.100, p = .358), bodily pain and SOS (β = −.028, p = .790), general health and SOS (β = −.045, p = .667), bodily pain and PSSS (β = −.144, p = .122), and general health and PSSS (β = .024, p = .790).
Two significant interaction effects were found. The first significant interaction effect was found between physical functioning and PSSS (see Table 6). The overall regression model was significant, F(6, 91) = 6.51, p = .001, and there was a main effect for ethnicity (β = −.196, p = .038), a main effect for physical functioning (β = −.222, p = .026), a main effect for PSSS (β = −.394, p = .001), and an interaction effect between physical functioning and PSSS (β = −.326, p = .001). Social support within the prison moderated the relationship between physical functioning and psychological distress. The second interaction effect was found between role physical and PSSS (see Table 7). The overall regression model was significant, F(6, 85) = 2.68, p = .001, and there was a main effect for ethnicity (β = −.217, p = .017), a main effect for role physical (β = −.234, p = .011), a main effect for PSSS (β = −.408, p = .001), and an interaction effect between role physical and PSSS (β = −.223, p = .017). There were no other main effects. The interaction effect indicated that PSSS moderated the relationship between role physical and psychological distress.
Interaction Between Physical Functioning and PSSS.
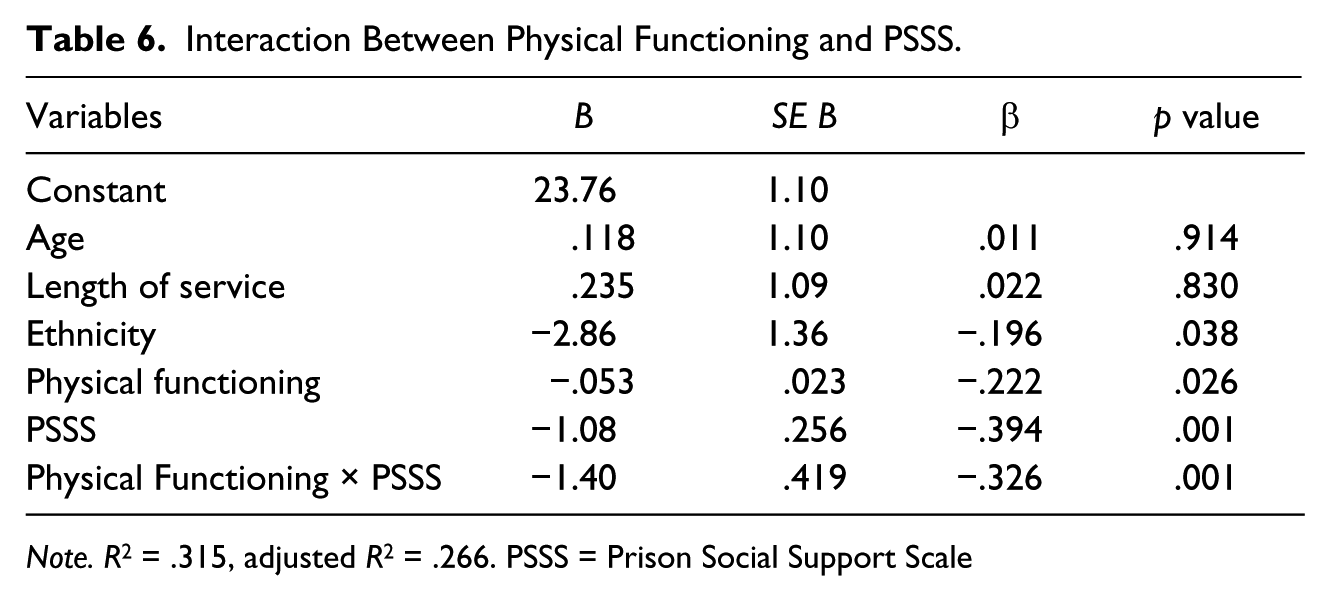
Note. R2 = .315, adjusted R2 = .266. PSSS = Prison Social Support Scale
Interaction Between Role Physical and PSSS.
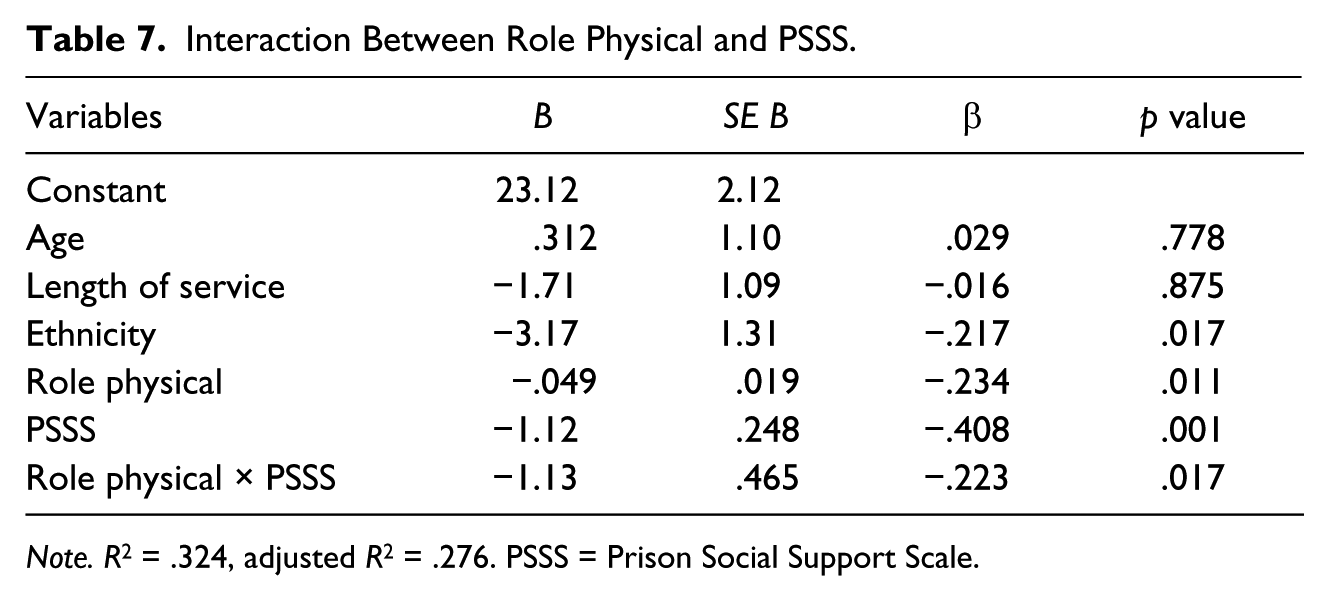
Note. R2 = .324, adjusted R2 = .276. PSSS = Prison Social Support Scale.
Discussion
This is the first study in the United Kingdom to examine physical health perceptions among prison officers using the SF-36 II. Prison officers scored lowest on their perception of their general health (M = 57.88) and highest on their level of perceived physical functioning (M = 85.35). Prison officers also scored lower on each of the physical health dimensions than staff who worked in prisons in the United States (Deitch, Koutsenok, & Ruiz, 2004). Moreover, by comparing normative data from the United States, it was found that 83.8% of prison officers within the current research scored below average on general health, 52.0% below average on role physical (limitations in usual role activities), 50.0% below average on bodily pain, and 32.0% below average on physical functioning. Moreover, the present results show lower scores on each of the physical health dimensions when compared with data using the SF-36 II with other occupational groups in the United Kingdom (Jenkinson, Stewart-Brown, Petersen, & Paice, 1999). Therefore, it seems that prison officers have poorer perceptions of their health than do the general population.
Why do a high proportion of prison officers perceive themselves to have relatively poor physical health? First, it is possible that individuals who join the prison service are a pre-selected group who are more prone to suffer from physical health difficulties. Second, it could be that the stressful nature of the work leads to prison officers being susceptible to physical health difficulties. Vingerhoets (2004) argued that exposure to stress may facilitate the development of organic health difficulties due to the impact of stress on the automatic nervous system, the neuroendocrine system, and the immune system, and also because people exposed to stress may engage in health risk behaviors as a means of coping. Third, some of the officers in the sample may be suffering from medically unexplained symptoms, somatic symptoms that do not have an adequate organic explanation (De Gucht & Maes, 2006). It has been argued that individuals who are exposed to stressful events may develop such symptoms (Pennebaker, 1982).
The reported mean for psychological distress in the present study, measured by the GHQ-12, was 13.06 (SD = 5.39). A total of 56.6% met the criteria for caseness (scoring >12). Previous research among prison officers has used the GHQ-12 (Dollard & Winefeld, 1998; Liebling et al., 2005; Long & Vogues, 1987). These studies do not report caseness statistics but they do report mean scores. Dollard and Winefeld (1998) in their study in the United States found that the mean score on the GHQ-12 was 12.18 (SD = 7.22) and Long and Vogues (1987) in their study in New Zealand found that the mean score on the GHQ-12 was 12.23 (no SD was provided).
Perceived physical health (all four dimensions) and psychological distress were correlated with one another. Social support from outside prison (SOS) did not significantly correlate with psychological distress and did not significantly correlate with three of the four perceived physical health measures. However, there was a significant correlation between scores on general health and on the SOS. This correlation indicates that, as perceptions of general health improved, participants rated a lower level of perceived social support from significant others; or that participants who rated a higher level of perceived social support from others rated poorer general health. It is possible that individuals with poorer health had in fact accessed more support and therefore, rated the level of support received as higher. Scores on the PSSS were correlated with bodily pain indicating that the more support an individual perceived to be available within the prison, the less they perceived themselves to have bodily pain. Moreover, social support from within the prison (PSSS) was significantly negatively correlated with psychological distress. This correlation between PSSS and psychological distress is in line with findings from previous research that has found a direct effect of social support on burnout (Dignam & West, 1988). Moreover, other studies have found that social support was associated with psychological health in a positive manner (Armstrong & Griffin, 2004; Drory & Shamir, 1988; Lindquist & Whitehead, 1986; Owen, 2006). Given the cross-sectional design of this study, it was not possible to establish causality.
But why might there be a difference between the two measures of perceived social support in their associations with levels of psychological distress? It could be that the scale for measuring support from a significant other failed to capture a full range of responses in perceived social support, for the scale was rated in relation to the person closest to each participant. Another explanation for the differences between the two measures of support is that social support within prison is indeed more strongly related to psychological distress. It is possible that officers believe in keeping the two worlds (that of the prison and the outside world) separate and, if this were the case, it would be support from within the establishment that would be crucial, rather than support from others outside work.
Moderator models were carried out to ascertain whether perceived social support from a significant other or from within prison moderated the relationship between perceived physical health and psychological distress. There were no significant interactions between perceived physical health and support from a significant other; the relationship between health and distress did not depend on the level of support an individual perceived from a significant other. However, there were significant interactions between perceived physical health and support from within prison. There was a statistically significant interaction between physical functioning and perceived social support within prison and role physical (limitations in usual role activities) and perceived social support from within prison. It could be argued that social support from within the prison played a protective role by helping officers not to be distressed, when they thought that their poor health was affecting their work. These findings are in line with those of Dollard and Winefeld (1998) who found an interaction between high-strain jobs and low level of social support in predicting psychological distress and physical health symptoms among prison officers. No interaction effects were found for the other two measures of perceived physical health (bodily pain and general health) and thus there was only limited support for the moderating models.
It is important to consider the limitations of the study. First, there is a difficulty in establishing causality due to the cross-sectional design of the study. Although the models being tested specified psychological distress as the outcome variable, it is possible that psychological distress predicted variance in perceived social support. Indeed, psychological difficulties may prevent an individual from seeking support in the first place. The cross-sectional design of the study also made it difficult to understand whether a lack of support was associated with increased psychological distress or whether the presence of support led to a decrease in psychological distress. To overcome these difficulties, a carefully designed longitudinal study would be useful. A second limitation of the study was that the sampling technique was non-random and could have introduced a selection bias. However, that is unlikely, as the researcher visited all areas of the prison and asked all visible officers to take part.
The results of the study lend themselves to further exploration. Social support within prison emerged as the variable most strongly associated with psychological distress, stronger than social support from a significant other. It would be of interest to carry out qualitative work to explore further the construct of prison social support. This research has focused exclusively on perceived social support using a brief quantitative measure and has not examined social support within the context of particular social relationships or particular transactions of social support.
Another area of study to examine further would be illness beliefs. The beliefs of individuals about their symptoms have been found to affect their appraisal of their condition and level of distress (Marks et al., 2002; Scharloo & Kaptein, 1997). Yet another area of particular interest would be to examine whether or not officers suffer from medically unexplained symptoms. It is not known whether the prison officers in the sample suffered from organic conditions, medically unexplained symptoms, or a combination of both (within the sample and within each individual). Epidemiological studies have found that patients with medically unexplained symptoms have higher levels of anxiety and depression than patients with organic conditions (Jackson, Kincey, Fiddler, Creed, & Tomenson, 2004) and report more negative illness beliefs than patients with acute organic disease (Frostholm et al., 2007).
This study has a number of clinical implications. First, a high proportion of prison officers reached caseness in their levels of psychological distress. It would be important for all officers to be screened regularly for psychological health problems and for officers to be given the opportunity of onward referral for further psychological support if needed. Second, a proportion of officers perceived their physical health to be poor and that there was an association between poor perceived physical health and psychological distress. Individuals who were distressed by their physical health difficulties may benefit from psychological therapy. It would of course be important to determine whether these health problems were organic or medically unexplained in nature, as the difference would determine the focus of the therapy (Brown, 2004).
In addition, it is important to consider the organizational implications of the research. This research found that support within prison was beneficial for officers: It was positively related to distress, and there was some evidence that it served as a buffer between perceived poor physical health and psychological distress. One implication for this research is that management teams should continue to develop supportive relationships with the staff.
This article has examined perceived physical health, psychological distress, and social support among prison officers. It has found some evidence that social support within the prison is a protective factor for prison officers. Of course, this research has only examined a single potential protective factor, and it would be useful to think more broadly about what other factors may improve the well-being of prison officers, and to focus on factors at both the individual and organizational levels. Indeed, rather than locating the difficulties solely within the individual, through exploring individual and systemic framework, this would encourage the researcher to take a psychosocial perspective to the well-being of prison officers. Moreover, a more contextual understanding of the difficulties of prison officers would allow for clinical interventions with this group to focus not only on the individual but also on systemic factors that are endemic to the prison community.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.