
Abstract
Pregnant inmates represent about 5% of females within the correctional population. Although this is a small portion of the entire inmate population, it is important to adequately address their needs to protect the health of the mother and the fetus. Many states have failed to properly address this issue. However, the states that appear to be the most comprehensive in terms of their treatment of pregnant inmates are California and Pennsylvania. Other states should model their statutes and administrative regulations after these states to effectively address the needs of pregnant inmates.
Keywords
Introduction
In the United States, there has been a significant increase in the number of women who are incarcerated in prisons and jails. A proportion of those who have entered prison and jail do so while pregnant. Estimates are that about 5% of women who are incarcerated in prisons nationwide enter prisons while they are pregnant (Levi, Kunakemakorn, Zohrabi, Afanasieff, & Edwards-Masuda, 2010). Because of the limited resources devoted to incarcerated pregnant women in prisons and jails, programs and resources tailored to this special population have been found to be inadequate in meeting their needs. Some examples of these inadequacies include the absence of special diets, lighter workloads, and medical resources for miscarriages, premature births, and deliveries (Wooldredge & Masters, 1993). Although the treatment of pregnant women outside of the criminal justice system has significantly advanced, this has not been the case with incarcerated pregnant women.
In addition to these inadequacies, many pregnant inmates are classified as high risk because of drug addiction, sexually transmitted diseases, or pelvic inflammatory disease (Parker, 2006). Although drug use during pregnancy is frequently cited by researchers as a critical problem, this has generally been overlooked, even though there has been a trend toward incarcerating pregnant, substance-abusing women to protect the health of the mother and the fetus. Given this trend, health officials in jails must be able to provide appropriate detoxification to pregnant drug addicts because the fetus may experience withdrawal symptoms (Parker, 2006). Many jails, however, have failed to provide appropriate care for pregnant inmates and their unborn children. Research indicates that drugs in prisons are readily available. This means that pregnant inmates are likely to continue using drugs for the duration of their pregnancy (Egley, Miller, Granados, & Ingram-Fogel, 1992). As a result of inadequate care, numerous negative outcomes include increased levels of fetal and neonatal death, intrauterine growth retardation, premature labor and delivery, and other conditions that necessitate admission to neonatal intensive care units (Siefert & Pimlott, 2001). Furthermore, such inmates may experience psychological distress as a result of the separation from their newborn child, which is also related to long-term problems experienced by the child (Wooldredge & Masters, 1993).
As of September 2013, 41 states and the District of Columbia have enacted pregnancy-specific statutes and/or administrative regulations (American Civil Liberties Union [ACLU], 2013). Some states have enacted statutes, while others have passed administrative regulations, and others have done both. This article seeks to analyze court cases as well as statutes and administrative regulations related to pregnant inmates to determine whether their specific needs are adequately addressed, as suggested by Tapia and Vaughn (2010). A model statute is then provided to guide policy makers when considering statutes and regulations that best meet the needs of pregnant inmates.
Pregnant Inmates in Prison
As the number of women in prisons has increased, so too has the number of women who are pregnant when entering prison. By 1998, about 5% of women who entered state prisons and 6% of women who entered jails nationwide were pregnant upon admission (Bureau of Justice Statistics, 1999). This increase has resulted in the need to address the issue of the medical issues of women in prison, particularly with regard to pregnancy and childbirth. This section will address some of the issues related to the health needs of pregnant inmates.
Problems faced by pregnant inmates
Various agencies have presented policy recommendations to reduce the likelihood of pregnant inmates experiencing physical and psychological problems. Such recommendations have included providing prenatal care in prisons, providing full-time nurses and midwives, allowing nursing infants to remain with mothers during their period of incarceration, and extending visiting hours for mothers with their children (Wooldredge & Masters, 1993). A study by Wooldredge and Masters (1993) analyzed the presence of various types of services for pregnant inmates in state prisons. Some of these services included prenatal care, networking with community agencies providing prenatal care, Lamaze classes, and special diets. None of the facilities reported having programs that allowed infants to remain with the mother. Eight wardens noted no problems. Some problems noted by wardens included inadequate resources for pregnancy complications, no maternity clothes, the use of belly chains during transport, and no separate visiting areas for mothers and children. This study was conducted 20 years ago but is the only study that has been conducted with this group of inmates.
Health care and prenatal needs of pregnant inmates
Women who enter correctional facilities are generally in poor health as a result of poverty, substance abuse, and the presence of physical and sexual abuse (Hotelling, 2008; Parker, 2006). As a result, many women who enter prison while pregnant are considered to have high-risk pregnancies. Having histories of drug addiction and sexually transmitted diseases are examples of criteria that are used to consider a pregnancy as high risk. These problems are exacerbated by the lack of gynecological examinations upon admission, the failure to ask appropriate screening conditions, and the lack of on-site physicians who specialize in obstetrics and gynecology (Arnold, 2004).
This is particularly problematic for drug-abusing pregnant women. The failure to provide an appropriate form of detoxification may harm both the mother and the fetus. Pregnant, drug-addicted inmates are forced to undergo withdrawal without consideration for the health of the fetus, even though the fetus can also experience withdrawal symptoms (Parker, 2006). Despite its seriousness, this problem has remained overlooked even though there has been a trend toward incarcerating substance-abusing pregnant women to protect the health of the fetus (Barry, Ginchild, & Lee, 1995). Continued drug use during pregnancy can have a number of adverse effects for the baby, including intrauterine growth retardation, reduced gestation, low birth weight, decreased head circumference, and premature delivery (Siefert & Pimlott, 2001).
Drug-abusing pregnant inmates present a number of psychologically based needs. The link between past and present instances of physical and sexual abuse and current substance use has been well documented in the research literature (i.e., Clark & Foy, 2000; Kaukinen & Demaris, 2005). Women who have been physically and sexually abused at some point are more likely to engage in substance use and abuse. Unless these issues are recognized and dealt with, it is unlikely that such women will be successful in achieving and continuing abstinence from substance use, especially if the abusive partner is the father of the baby (Siefert & Pimlott, 2001).
Although some argue that incarceration is harmful to women and their unborn child because of the level of stress, others maintain that incarceration may improve the health of pregnant inmates because they are receiving an adequate level of food and have limited access to drugs (Parker, 2006). One study indicated that pregnant inmates who experienced short-term incarceration were more likely to experience poor prenatal care, histories of drug abuse, and poor nutrition compared with the long-term incarceration group (Cordero, Hines, Shibley, & Landon, 1991). Another study comparing a group of incarcerated pregnant inmates with a control group indicated that a greater percentage of those who were incarcerated acknowledged the use of illicit drugs and tobacco, yet positive outcomes were still found among those who were incarcerated, despite increased drug use (Egley et al., 1992).
Effect on mothers and children
Incarceration is found to be harmful to the well-being of both mother and child because of the stress related to imprisonment (Parker, 2006). Early studies in this area assumed that the infant would be victimized at birth as a result of the circumstances under which the birth occurred (Johnson, 1969). One study analyzing three facilities in California found that all three sites were lacking in health care plans and case management systems related to prenatal care. In addition, inmates perceived the health care providers at these facilities as insensitive and unresponsive to their health care needs (McCall, Casteel, & Shaw, 1985).
The long-term effects of the mother’s incarceration on the child have not been extensively studied. The few studies that have directly analyzed these children have generally indicated negative results. One study found that most children who were identified as having severe behavioral and disciplinary problems had experienced parental crime, arrest, and incarceration, while some children had a parent who was incarcerated when the study was taking place (Johnston, 1995). The negative impact of a mother’s incarceration, in particular, may persist throughout one’s childhood. Furthermore, forcibly separating children from primary caregivers is devastating to children’s emotional needs, who are in a vulnerable and frightened state. This is further exacerbated by their separation from siblings (Kampfner, 1995). Recent research finds that individuals whose mothers had been imprisoned are significantly more likely to experience arrest, conviction, and incarceration as adults (Muftic, Bouffard, & Armstrong, 2016).
Shackling of pregnant inmates
Shackling is defined as the practice of placing chains on an inmate during pre-labor, labor, or post-labor. Examples of this practice include attaching arms or legs to the bed with chains, shackling legs together during childbirth, and attaching ankles together with chains during the process of inducing labor. Restraints are used on women regardless of their history of violent behavior or flight risk (Amnesty International USA, 2001). The majority of pregnant inmates who are shackled during labor are considered to be nonviolent and not considered to be a flight risk (Griggs, 2011). Although this practice is allowed in most states, it is considered to be unconstitutional and violates human rights guidelines (Sichel, 2008). It is argued that shackling violates the Eighth Amendment right against cruel and unusual punishment because it causes pain and deprives prisoners from receiving adequate medical care (Griggs, 2011). Most states continue to allow this practice during the third trimester of pregnancy, and many of these states allow shackling during labor (Doetzer, 2008). According to the ACLU, 18 states have either prohibited or placed restrictions on shackling pregnant inmates (ACLU, 2012). They discuss numerous problems related to shackling, including health risks to the mother and the fetus, as well as potential violations of constitutional law and international human rights treaties.
Although some states actively engage in shackling of pregnant inmates, Massachusetts has recently passed an anti-shackling law to prevent shackling and promote safe pregnancies. The Massachusetts bill disallows the use of restraints of any kind during any stage of the pregnancy or during delivery and instead uses vehicles with seatbelts to transport inmates to medical providers and court proceedings (Commonwealth of Massachusetts, 2014).
Viewpoints of the National Commission on Correctional Health Care (NCCHC) and American Correctional Association (ACA)
The NCCHC (2010) has addressed guidelines for shackling. It considers the differential application of restraints depending on the phase of labor and delivery. During the prepartum period, restraints should be used restrictively, and their recommended use varies depending on the part of the body being restrained; for example, abdominal, leg, or ankle restraints should not be used, while wrist restraints should be applied in a manner that would allow the inmate to protect herself and her baby in the event of a fall. During the partum period, it is recommended that the use of restraints be avoided unless there is a serious threat of harm to self or others. Similarly, restraints should be avoided during the postpartum period to allow for recovery from labor and delivery, as well as for optimal bonding between the mother and the baby.
Like the NCCHC, the ACA (2012) addressed the use of shackling during transport, delivery, and the postpartum period. They specify that female offenders who are suspected to be pregnant should be restrained in the least restrictive manner as possible. The use of waist restraints is prohibited at any point during pregnancy, while leg restraints should only be used under extreme circumstances during transport, but never during labor and delivery. Also, electronic restraints are not to be used at any point during pregnancy or labor and delivery.
Method
Cases were found by conducting a search on LexisNexis with the search term pregnant inmate to determine lower level federal and state-level cases that specifically addressed pregnant inmates in prison or jail as of September, 2013. A total of 16 cases were found that were relevant to pregnant inmates—14 at the federal level and two at the state level. Links for state statutes and administrative regulations were found through the portion of the ACLU website that discusses state standards for the health care of pregnant inmates (ACLU, 2013). These links are current as of September, 2013. These links addressed various issues related to pregnant inmates, which are grouped into different categories: shackling, prenatal care, counseling, childbirth/postpartum care, and other references, which was a catchall category that includes issues not addressed in the previous four sections.
Court Cases, State Statutes, and Administrative Regulations
Prison health care has been an issue for the past several decades, beginning with Estelle v. Gamble (1976). In this case, an inmate filed a complaint under 42 U.S.C. §1983 because of a back injury received while working in prison. He claimed that he was subjected to a violation of his Eighth Amendment right against cruel and unusual punishment because of the lack of diagnosis and inadequate treatment from prison officials for his injuries. On appeal, the U.S. Supreme Court held that deliberate indifference to serious medical needs by prison constitutes an Eighth Amendment violation. Although this case did not specifically focus on pregnant inmates, it did bring inmate health care to the attention of researchers and practitioners. This would later be extended to pregnant inmates, which is the focus of this section.
Analysis of State and Federal Court Cases
Although cases involving pregnant inmates have yet to reach the U.S. Supreme Court, such cases have been addressed by a handful of lower level federal and state courts, which are summarized in Table 1. Currently, no cases involving pregnant inmates have reached the U.S. Supreme Court. Instead, cases at the federal level have reached the U.S. District Court and the U.S. Court of Appeals.
Summary of State and Federal Court Cases Involving Pregnant Inmates.
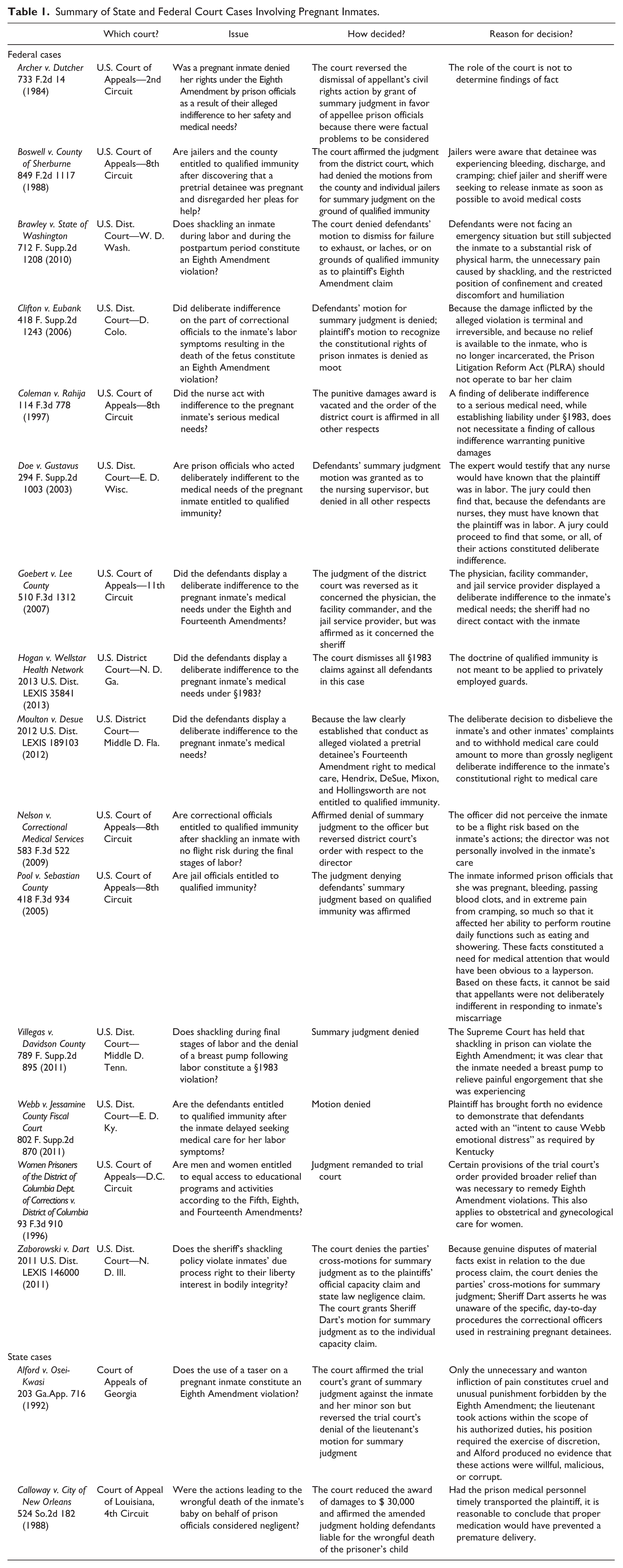
Issues
The issue in the majority of these cases involved either Eighth Amendment violations or the debate surrounding qualified immunity for correctional officials. Specifically, cases involving Eighth Amendment violations were related to various issues, including shackling, indifference to the inmate’s medical needs, and the use of a taser. Regarding qualified immunity, various officials claimed that they were entitled to this because their obligation was not clearly established at the time of the incident. In another case, an inmate was shackled despite being in the final stages of labor and being in severe pain throughout the process. In most of these cases, these lawsuits stemmed from death or serious injury to the baby, or emotional distress on the part of the mother, with the exception of the cases where prison officials were seeking qualified immunity.
Decisions and reasons for the decision
Overall, the decisions in these cases tended to be evenly decided in terms of whether or not they were in favor of the inmate. In cases where the inmate delayed seeking medical care or in cases where factual problems needed to be considered, for example, courts decided against the inmate. However, cases that involved shackling tended to be decided in the inmate’s favor. As it relates to decisions involving qualified immunity, this was granted to individuals who were not directly involved in the care of the inmate. However, this has been denied to correctional officers in private facilities, even those who were directly involved in the care of the inmate.
Analysis of State Statutes and Administrative Regulations
As of September, 2013, 41 states and the District of Columbia had enacted statutes or administrative regulations that relate to reproductive care or the care of pregnant women, including childbirth, in correctional facilities (ACLU, 2013). Links to these statutes and administrative regulations were obtained through the ACLU website. This section will identify and then analyze the 42 states and jurisdictions that have statutes or administrative regulations related to the care of pregnant inmates. A comparison of the statutes and administrative regulations as found on the ACLU website is provided in Table 2.
Analysis of State Statutes and Administrative Regulations Related to Pregnant Inmates.

Note. S = statute; AR = administrative regulation; S/AR = both statute and administrative regulation; DOC=Department of Corrections and TB does = tuberculosis.
Very few of these statutes or regulations specifically address standards set forth by the NCCHC and the American Public Health Assocation (APHA) (ACLU, 2013). The NCCHC provides specific indicators of compliance for pregnancy care in general, including prenatal medical examinations and testing, advice for inmates regarding suitable levels of activity and safety precautions, nutritional guidance and counseling, maintaining lists of specialized obstetrical services, written agreements with local facilities for childbirth, keeping a record of pregnancies and their outcomes, and having written policies and defined procedures that address compliance with this standard. Additional recommendations include providing pregnant inmates with counseling that is suitable with her intentions, depending on whether she wishes to keep the baby, place the baby up for adoption, or have an abortion. The standards provided by the APHA demonstrate some overlap with those of the NCCHC, but some additional important recommendations are provided. Some of these additional recommendations include special housing and diets, proper identification and referral of high-risk pregnancies, treatment to prevent the transmission of HIV to the fetus for women who are HIV positive, prohibiting shackling during labor and delivery, and ongoing access to newborns following delivery.
Shackling
Some states have recently enacted statutes and regulations regarding the shackling of pregnant inmates to reduce the likelihood of enforcement in prisons and jails. Twenty-one states have imposed regulations on their use during the various stages of pregnancy as well as during labor and delivery. When considering the use of shackles during the stages of pregnancy, nine of these states set limitations on their use during the second and third trimesters of pregnancy. For example, New Mexico only allows the least restrictive restraints possible to be used during the second and third trimesters of pregnancy. Most of these statutes and regulations provide an exception to the use of restraints if the inmate has a history of violent behavior. In addition, many of these states either place restrictions on or do not allow the use of restraints during transport. During labor and delivery, many of these states are much more relaxed in terms of the use of restraints, in many cases, disallowing their use.
Prenatal care
The analysis indicated that 31 states addressed some form of prenatal care for pregnant inmates. This ranges from prenatal care for juveniles, in the case of Utah, to the supply of prenatal vitamins to inmates, in the case of several other states. In most cases, however, states simply specify that prenatal care is available for pregnant inmates. Nine states address the possibility of abortion for pregnant inmates.
Counseling
Over half of the states (23 states) addressed the availability of some form of counseling for pregnant inmates; in most cases, this was provided to assist the pregnant offender in planning for her unborn child and assisting in the placement of the child after birth. A couple of states, including Oregon, provide counseling to inmates throughout all stages of pregnancy, including those who choose to have an abortion. Providing counseling to pregnant inmates allows them to express their feelings related to their babies as well as determine what the best possible placement might be for the baby based on the circumstances of the mother.
Childbirth/postpartum period
In terms of care for the pregnant inmate during childbirth and the postpartum period, only 13 states addressed making transfers to outside hospitals for labor and delivery. This is an important consideration, as most prison infirmaries are not equipped to meet the needs of childbirth. In addition, many of these states restrict the mother’s contact with their newborn child. This can be problematic as it relates to bonding between the mother and the baby, especially if the mother intends to keep the baby after her release from prison, or unless she is physically or mentally unable to care for the baby. Ohio differs from the majority of states in that it allows for prison nurseries to be establishes so that inmates and their babies can reside together. Some states (13 states) address some form of postpartum care for mothers; this ranged from simply stating that postpartum care was available to transfer as soon as possible after delivery to a secure facility.
Other references
Only a handful of states (seven) addressed the availability of chemical dependence treatment for pregnant inmates. This is concerning, considering that many pregnant inmates are likely to be addicted to alcohol or drugs. More states should address these issues in the mother so that this will be less likely to have harmful impacts on the baby. A couple of states provide clemency or furloughs for pregnant inmates, which is included in this column.
The majority of states only provided basic information regarding prenatal, intranatal, and postnatal care by only stating that these forms of care were available for pregnant inmates. These states failed to follow the guidelines provided by the NCCHC and the APHA by only referencing a small portion of the recommendations.
Toward a Model Statute
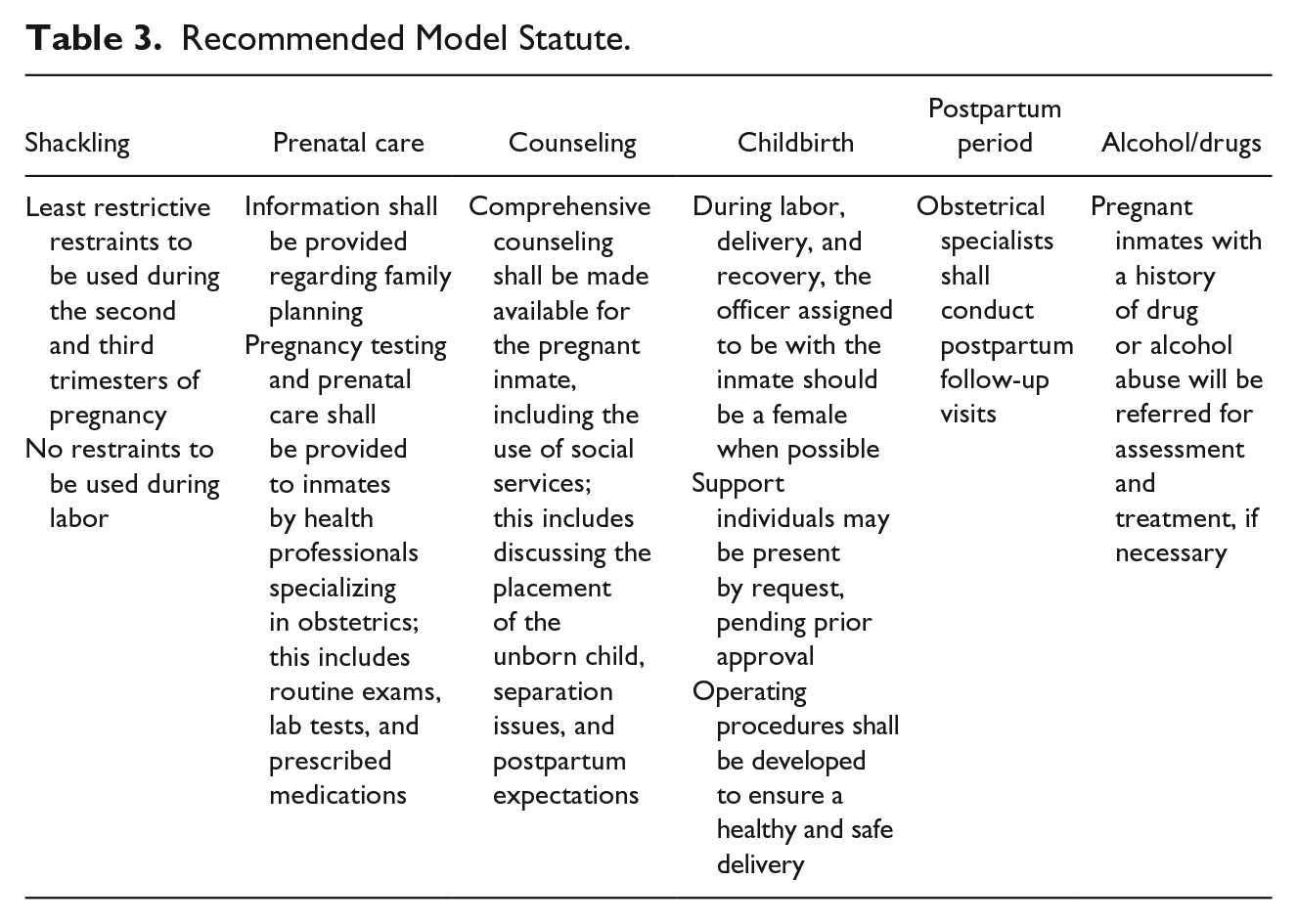
Based on this analysis, the states that appear to be the most comprehensive in addressing the care of pregnant inmates are California, New Hampshire, New Mexico, and Pennsylvania. They address a variety of medical issues related to pregnant inmates, including the care of the pregnant inmate, as well as the baby following birth while the mother is incarcerated. Collectively, these states provide restrictions on shackling pregnant inmates, particularly during the second and third trimesters, as well as during labor. In addition, these states provide for prenatal care for pregnant inmates with regard to family planning and pregnancy testing. These states also consider the best option for the placement of the baby by providing counseling and social services to the pregnant inmate. As it relates to inmates with a history of alcohol or drug use, these states seek to address these issues by recommending treatment. The remaining states should follow the trend of these states as it relates to the treatment of pregnant inmates, because these states appear to provide a variety of options for such inmates. A recommended model statute is summarized in Table 3.
Recommended Model Statute.
Discussion
Although some state statutes and administrative regulations address some of the specific health related needs of pregnant inmates, other states have either failed to do so adequately or not at all. The medical needs of females in the correctional setting need to be properly addressed so that both mother and baby stay healthy in the long run. Many females who enter prisons and jails are in poor health and are at high risk because of substance addiction, sexually transmitted diseases, and being of lower socioeconomic status, which most likely results in fewer visits to physicians. Not only is the health of the fetus at risk because of these conditions, but because not all jails or prisons routinely provide obstetrical and gynecological services to female inmates, such inmates are at risk for having undetected diseases, such as ovarian cancer, breast cancer, and abnormal pap smears (Arnold, 2004).
From this analysis, it appears that many of these state statutes and administrative regulations are inadequate for meeting the needs of pregnant inmates both during the pregnancy as well as during the postpartum period, according to the guidelines provided by the NCCHC and the American Public Health Assocation (APHA). Two states that appear to be the most comprehensive in their coverage of pregnant inmates are California and Pennsylvania. The issue of the use of restraints on pregnant inmates has recently been controversial. Some states have recently passed laws that prohibit the shackling of pregnant inmates during labor. In some instances, policies have attempted to justify the use of shackling by stating that inmates may be a danger to themselves or others, or that they pose a substantial flight risk. Remaining states that have not passed policies prohibiting shackling should follow the example of states that have successfully passed such policies.
To best address the needs of inmates during pregnancy and during the postpartum period, states should consider the best option for the baby. If the mother is physically or mentally unfit to care for the infant, adoption should be considered. For mothers with substance abuse issues, these problems should be addressed as soon as the problem becomes apparent to reduce health risks to the mother and the baby. Also, more states should consider limitations on the use of restraints during the second and third trimesters of pregnancy, as well as during labor and delivery. Any falls resulting from the limited range of motion resulting from the restraints could be detrimental to the baby.
Issues revolving around pregnant inmates continue to be addressed as a problem across prisons and jails, yet little research has been conducted on this group of inmates. Although fewer women are incarcerated in comparison with men, and only a small portion of these women are pregnant, more research is needed to determine the best methods of addressing the medical needs of this population. This article examines the plight of pregnant prison inmates with the hope that the needs of this generally powerless and dispossessed segment of American polity can be better addressed and improved in consonance with the “evolving standards of a decent and maturing society.”
Although only a relatively small number of female inmates enter prison while pregnant, there is a need for rules to determine how these inmates should be treated. These rules are designed for the good of the inmate as well as that of the baby who, after all, is a future member of the free society. Some courts have protested the rights of both the inmate and the baby under the rubric of the prohibition against the cruel and unusual punishment clause of the U.S. Constitution. Legislatures have also enacted laws in the interest of just treatment and humanitarianism.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.