
Abstract
A number of studies find that solitary confinement is associated with mental impairment. Yet, confinement dosage and which individual and exogenous variables lead to mental impairment have received less attention. This study of 2 years of data on disciplinary segregation male inmates employs a repeated measures design to examine how isolation affects mental health and psychological needs. The findings indicate that the duration of disciplinary segregation and incarceration, incidence of homelessness, and other individual-level factors had deleterious effects on mental health and psychological needs. Vocational programming and a high school education were found to be protective factors for psychological needs.
Introduction
Prison systems across Western society have experienced a decades-long organizational crisis centered on balancing order maintenance with offender treatment. The deinstitutionalization movement of the 1950s and 1960s resulted in fewer hospital beds for seriously mentally ill (SMI) and indigent patients, with confinement to jails and prisons becoming the more frequent solution (Lamb & Weinberger, 2017). Once incarcerated, these underlying mental health issues increased the possibility of further isolation as a result of perceived rule-breaking (Cloud, Drucker, Browne, & Parsons, 2015), extending the offender’s stay and/or contributing to criminogenic behavior patterns.
Correctional institutions have thus become de facto mental health institutions in the United States (Haney, 2017; Kurki & Morris, 2001). The United States currently boasts 10 times as many people with a SMI in correctional institutions compared with confinement in mental health facilities (Torrey et al., 2014). Notably, persons with psychiatric conditions are over-represented in jails and prisons, especially in restrictive housing (Cloud et al., 2015).
Restrictive housing refers to some condition of limited social contact within a living space while incarcerated, sometimes referred to as isolation, solitary confinement (SC), disciplinary segregation (DS), administrative segregation, or secured housing. Approximately 30% of prison inmates in segregation report past or current SMIs (Beck, 2015). Often, these inmates are sent to isolation for disciplinary reasons, as they have difficulty complying with prison/jail rules, and officials utilize these space alternatives to keep order (Cloud et al., 2015; Labrecque & Mears, 2019). However, placement in isolation can result in inmates experiencing worsened psychological symptoms, intensifying misbehavior, and further prolonging their stay in restrictive housing (Fellner, 2006). While most agencies limit the time an offender remains in isolation, the frequency and duration of isolation placements have been difficult to assess (Morris, 2016). Of particular concern is that, offenders with SMIs are over-represented in SC due to prison efforts to control unruly behavior (O’Keefe & Schnell, 2007).
Importantly, gradual change in correctional policies regarding inmates with SMIs has been slowly implemented. The 2016 American Correctional Association (ACA) advocated for routine behavioral health assessments for offenders in isolation, and that offenders with serious SMIs not be placed in extended restrictive housing. Such policy recommendations represent a marked shift in our understanding of SC, indicating that although the effects of incapacitation on mental health and other offender needs are not fully settled, there is emerging evidence of its negative effects (Labrecque & Mears, 2019; Meyers, Infante & Wright, 2018; Walters, 2018). While inmates may be placed in some form of SC for their own protections, for administrative or disciplinary purposes, there is a debate about the effect of isolation on mentally vulnerable adults (Kapoor & Trestman, 2016; Labrecque & Mears, 2019, p. 200). Kapoor and Trestman (2016, p. 200) summarize for the National Institute of Justice some of the problems with the research on SC’s purportedly psychologically debilitating effects, noting that critics have characterized them as methodologically weak and/or not generalizable. The current study adds some rigor to the research by examining a full 2 years of data in a Western state to determine whether the duration of varying levels of isolation affects offenders’ subsequent mental health functioning and other psychological constructs. We also address a “gap in knowledge” identified by Kapoor and Trestman (2016) in that we collect information about SC inmates regarding their status in the community. Findings from this investigation contribute to the growing body of literature examining the consequences of SC on mentally ill or vulnerable inmates.
Context of Isolation Policy
The use of SC became widespread in the 1980s as the movement to construct supermax prisons gained ground. Supermax prisons utilize the most extreme form of isolation as a means of maintaining prison order, decreasing violence, and deterring violence (Arrigo & Bullock, 2008; Labrecque & Mears, 2019; Mears & Reisig, 2006). “The worst of the worst,” offenders were intended to be placed in supermax prisons to decrease the likelihood of injury to prison staff and other housed offenders (Ward & Kassebaum, 2009, p. 70). Nonetheless, as supermax construction increased the capacity of correctional systems to house high-risk offenders, the number of severely incorrigible offenders did not keep pace with cell construction, widening the net to include “nuisance offenders” who irritate correctional staff, or have minor prison infractions (Shames, Wilcox & Subramanian, 2015; Toch, 2001). Given limited resources, a bed-driven classification policy thrived.
To help differentiate disruptive or dangerous offenders from those less likely to be so, Labrecque and Smith (2019) created an intake assessment designed to inform case management decisions with the ultimate goal of reducing institutional misconduct. This strategy has the potential to improve order maintenance policies by ensuring agencies limit isolation exposure to low-risk groups and by providing specialized case management that seeks to enhance protective factors for institutional violence. Yet, much work on the potential harms and tolerable lengths of isolation is still needed.
Offenders Placed in Isolation
Offenders with SMIs may be more likely to be placed in restrictive housing (Beck, 2015; Labrecque & Mears, 2019). For instance, Hodgins and Côté (1991) assessed offenders from two segregation units and found that offenders in isolation had a higher prevalence of severe SMIs. Furthermore, Andersen et al. (2000) compared rates of psychiatric disorders of offenders in SC to those in the general population. They found that 28% of offenders in SC had psychiatric disorders compared with only 15% of offenders in the general population and suggested these rates of disorders differed due to SC. Generally, it is unknown whether those with more SMIs are put in SC at higher rates, if SC is the cause of decreased psychological functioning, or whether SC affects offenders with pre-existing SMIs differently than those without (Kapoor & Trestman, 2016; O’Keefe, 2007).
In contrast, O’Keefe et al. (2013) found that prisoners who entered SC with a SMI did not suffer significant deterioration in psychological functioning relative to prisoners without SMIs who were subjected to administrative segregation. When the mental well-being of these two groups was measured against comparison subjects in the general population, all four groups showed roughly similar rates of change on psychological functioning during the 1-year observation period. These results would make it appear that the conditions of isolation matter little when considering the mental health of inmates.
Finally, two meta-analytic reviews have demonstrated that the average effect size for SMIs resulting from SC is small to moderate (Morgan et al., 2014; Smith, Gendreau & Labrecque, 2015). However, less than 10% of the studies found met the inclusion criteria in these meta-analyses. Studies with weaker designs tended to have larger negative effects compared with those with more methodological rigor (Gendreau & Labrecque, 2015). In short, more research is required regarding the psychological outcomes associated with SC.
Limitations of Prior Research
Prior findings on the effects of isolation have not been uniform. Whereas some researchers have found that it results in maladaptation, others have found that isolation has little psychological impact on offenders (O’Keefe et al., 2013; Zinger, Wichmann & Andrew, 2001). One explanation for these disjunctive findings may be due to the populations examined being only proxies for those in isolation, as researchers have utilized college students (Bonta & Gendreau, 1990) or excluded offenders with pre-existing psychological conditions (Bonta & Gendreau, 1995). Furthermore, Suedfeld, Ramirez Deaton, and Baker-Brown (1982) found no evidence that isolation was stressful or damaging to mental health, but this was a simulated SC study that selected its sample by relying on volunteers. Given the samples examined, many SC studies may lack external validity and application to real world circumstances.
Another explanation regards methodological design. Researchers have used autobiographies, self-reports, clinical observations (Haney & Lynch, 1997), cross-sectional data (Huebner, 2003), and/or small sample sizes (Grassian & Friedman, 1986; Grassian, 1983), all of which limit the application and validity of their findings. To avoid the concerns raised in Suedfeld et al.’s (1982) simulated study, Haney and Lynch (1997) and Haney (2003) examined a sample of offenders already assigned to SC by administrators. He found that previously healthy offenders could develop SMIs in isolation and that SC can be detrimental for any offender who endures it for a long period of time. Notable caveats to this study include its cross-sectional design, lack of a comparison group, and a focus on an extreme application of isolation that may not be characteristic of other institutions’ uses of SC. While a recent study shows that isolation is used for administrative purposes and for longer durations than was previously known by either the scholarly or practitioner communities (Shames et al., 2015), these findings are based on a subset of institutions who returned census forms. If isolation is widely implemented as a control tactic by prison administrators, additional information may be gleaned from studies that consider the comprehensive uses, rather than extreme exemplars, of isolation by institutions.
Evidence-based research studies balancing rigorous methodological designs and realistic isolation conditions are needed to better assess the outcomes of SC mental health outcomes. Cross-sectional designs often cannot assess offenders’ mental well-being prior to isolation (Smith, 2006). There is also a lack of research evaluating long-term effects, including how isolation affects offenders’ social lives. Rather, the crux of such research has focused on SMIs immediately following isolation, which may still be problematic as some studies have purposefully excluded offenders with pre-existing SMIs. Post-isolation effects may be an important consideration as many offenders who experience isolation will eventually return to the community with typical and perhaps exacerbated needs. Taken together, the weight of prior research underscores the need for assessing the effects of SC on offender needs, taking into account the duration (or dosage) of segregation episodes, as well as its longitudinal effects.
Theoretical Foundation: Epidemiology
Institutions use isolation to enhance staff and offender safety. The ostensible goal is to keep order, not cause offender medical conditions to deteriorate. To assess this phenomenon, the impact of SC can be viewed through an epidemiological lens (Morris, 2016). This perspective examines crime as a public health concern that can be addressed through positive intervention with offenders. SC has been used as a form of punishment and/or incapacitation (Smith, 2016). Yet, its use only moderately considers the potential negative health effects on the recipient. Prolonged isolation has been shown to produce harm, can be considered inhumane, and may undermine attempts to rehabilitate offenders (Rothman, 1980). Several medical organizations have acknowledged the negative effects of isolation on offenders and how this placement may constitute inhumane treatment. For instance, the American Psychiatric Association, American Academy of Child & Adolescent Psychiatry, College of Correctional Physicians, and the American Public Health Association have all published position papers in the last decade that acknowledge some potential harm from the use of SC, particularly for those with a SMI, and recommend reductions in its use or duration (Kapoor & Trestman, 2016).
Isolation is a public health issue because any collateral harm spills over into communities when offenders, their families, and communities struggle with its negative effects (Cloud et al., 2015; Macmadu & Rich, 2015). For instance, offenders released from isolation directly back to the community have been shown to recidivate more quickly and more frequently than offenders who have a transition from isolation to the general prison population and then to the community (Lovell, Johnson, & Cain, 2007). However, administrators are tasked with balancing genuine concerns of order maintenance with a more treatment-oriented approach to incarceration, or with one where correctional practices are more reflective of a “penal help” perspective than a penal harm one (Stohr, Jonson, & Cullen, 2014). Such a perspective should at the very least consider the negative effects of SC on communities. To underline this perspective and the works of many correctional scholars examining organizational management strategies, the current study illuminates the potentially harmful effects of isolation policies.
Factors Tied to Recidivism
Certain individual factors are associated with offender disciplinary infractions (Coid et al., 2003). Younger offenders are more likely to be placed in segregation (Butler & Steiner, 2016; Labrecque & Mears, 2019), as the young tend to have higher rates of disciplinary infractions and rule-breaking (Wooldredge, 1994). Likewise, offenders with shorter sentences tend to have higher infraction rates than those with longer sentences (Ditchfield, Britain, & Unit, 1990), explained by having a shorter adaptation period to incarceration (Flanagan, 1980).
Another individual factor that tends to be of interest in this vein of research is race/ethnicity because disparity in offender placement in SC has been found in some prisons (Labrecque & Mears, 2019; Schlanger, 2013). Yet, disparity may result from some facilities purposefully isolating alleged gang members from one another and from the general population (Fleisher & Decker, 2001), which indeed follows research findings (see Gaes, Wallace, Gilman, Klein-Saffran, & Suppa, 2002). Regardless of gang or race/ethnic disparities in placement, the consequences of SC have not been shown to differ by race or gang affiliation.
Regarding education, the U.S. correctional population is over-represented by offenders who lack an adequate education when compared with the community residents (Macmadu & Rich, 2015). From a theoretical standpoint, offenders with higher levels of education may be more likely to conform to prison rules as a result of exposure to organized indirect control, where these offenders have a greater commitment to conventional norms (Wooldredge, Griffin, & Pratt, 2001). However, some researchers have demonstrated that offenders’ education levels do not affect their likelihood of being placed in SC (Butler & Steiner, 2016; Coid et al., 2003).
Another concern is homelessness. Effects of isolation and/or SC for the homeless are complex (Pedersen, Andersen, & Curtis, 2012). Some studies indicate that social isolation is typical for the homeless (Rokach, 2005; Stewart et al., 2009), whereas other investigations have found that the homeless do not feel isolated (Lagory, Ritchey, & Fitzpatrick, 1991). Pedersen et al. (2012) demonstrated that some of their socially marginalized interviewees described social isolation as positive, which appears counterintuitive, as isolation is frequently related to negative health outcomes. Individuals suffering from SMIs appear to be disproportionately represented in the long-term homeless population (Henwood, Cabassa, Craig, & Padgett, 2013). McNiel and Binder (2005) found that approximately 30% of patients in a county hospital’s psychiatric emergency services unit were homeless. In addition, 8% of the homeless patients displayed violent behavior in the 14 days leading up to the emergency visit. Considering this evidence and the lack of attention it has received in prior SC studies, homelessness is included as a covariate in the current study in the hopes of further illuminating the relationship between homelessness and mental health.
Analysis Plan
The current study is a longitudinal examination of 408 male prisoners assigned to state supervision. It focuses on how isolation (e.g., incarceration, DS) and protective factors (e.g., vocational programming) affect offender needs, including mental health. Each offender was measured at three time points. To examine our dataset, we use generalized estimating equations (GEEs), a repeated measures procedure that accounts for the correlation of measurements of an individual’s status, over time (Hoover, Shi, Burstyn, & Anastos, 2019; Liang & Zeger, 1986; McCullagh & Nelder, 1983). This multi-level procedure is now widely accepted in the medical and epidemiological literature, and we believe our modest sample size is offset by its considerable strengths. 1 To examine SC, we test the following non-directional hypotheses, wherein DS will affect (1) mental health functioning, (2) behavior toward authority, (3) impulse control, and (4) readiness to change.
Method
Data were obtained from a western state Department of Corrections (hereafter referred to as WSDOC) on July 14, 2016. Our goal was to examine the mundane use of SC by utilizing broad sample selection criteria. The sample was first limited to all male offenders who recorded at least one violent infraction in WSDOC custody since 2000. 2 Considering disciplinary SC is generally reserved for violent offenders, we believe this criterion allows for a modest limitation in the sample and focuses on the population of most concern. Second, the sample was limited to offenders with at least three administrations of the state-wide standard needs assessment (hereafter referred to as NA) during 2014-2015. 3 The NA is administered while an offender is incarcerated and/or when he or she is in the community. 4 Therefore, we utilize data from the beginning of 2014 until the end of 2015.
Offender sanction dates for a violent infraction were then matched with maximum custody bed start dates to represent DS, which is our unique measure of SC. Every offender in the sample experienced incarceration and some form of isolation (i.e., administrative, protective, disciplinary) during the 2014-2015 time period; thus, it may be considered a high dosage of isolation sample to varying degrees, relative to non-supervised residents in the community. No matter their isolation status, all offenders had committed a violent infraction since 2000. 5
The first dependent variable measures mental health functionality and was scored by medical professionals during standard evaluation procedures. This variable is not on the NA and not administered by the same staff. The other three dependent variables are measures of offender needs, collected by the NA. These four dependent measures serve as proxies for measures of harm experienced by offenders. Using GEE modeling across three time points, we examine whether DS and incarceration are generally detrimental to our dependent measures.
Independent Variables
Based on theory and prior research, dozens of variables were selected from the database and entered into a bivariate correlation matrix with our dependent variables. Eleven potential covariates emerged as having a significant relationship with at least one of our dependents. The models contained herein utilize each of these covariates respectively. Fixed variables include race (0 = non-White; 1 = White), age, and juvenile conviction (0 = no; 1 = yes). Dynamic variables include homelessness (0 = home; 1 = no home), education (0 = less than HS; 1 = HS or more), incarceration rate, and gang affiliation (0 = no; 1 = yes). Unlike other studies of SC, we found no statistically significant relationship between substance abuse and mental health.
Each measurement point was taken in custody or the community. Thus, incarceration is measured as a rate, rather than days, to account for varying interval lengths. For homelessness, if incarcerated, offenders reported their housing situation during the prior 6 months in the community. Finally, vocational programming hours were included as it is theorized that they have played a role in helping offenders change for the better while incarcerated and one might expect this would lead to fewer placements in SC (see Lipsey & Cullen, 2007).
Dependent Variables
The primary dependent variable was mental health status. 6 Values for this measure are assigned by WSDOC medical professionals who evaluate offenders at key points throughout their prison experience. Accordingly, we were confident in their accuracy, reliability, and ability to generalize a process of change in offender mental health needs relative to days in isolation. WSDOC policy requires that a medical professional assess the mental health functioning of a person placed within DS every 72 hr. Those marked with DS in our dataset had to be in DS for a minimum of 6 days to ensure that a mental health assessment had been completed within the requisite first 72 hr (we added three more days to account for weekends or delays). After reverse-coding and collapsing the two highest-need categories, mental health status ranged from 1 to 4, with 1 indicating the highest need for mental health services.
Additional dependent variables were behavior toward authority, impulse control, and readiness to change. These measures were unweighted and contained on the NA. The behavior toward authority measure captures a dimension of criminal thinking (Mills, Kroner, & Hemmati, 2004). Impulse control is an estimate of offenders’ abilities to exercise discretion before acting. Generally known as “self-control,” low levels of this construct have been associated with criminal behavior, analogous acts such as preferences for simple rather than complex tasks, being self-centered, and losing control of one’s temper (Gottfredson & Hirschi, 1990; Grasmick, Tittle, Bursik, & Arneklev, 1993). Offender non-compliance with institutional or community supervision rules is consistent with weak levels of self-control and is a risk factor for recidivism (DeLisi & Berg, 2006). Finally, for several decades, corrections scholars have studied how offenders make positive changes during incarceration (Lipsey & Cullen, 2007).
Results
While only 5.3% of our total measurement points (n = 65) included the worst mental health status, the distribution was fairly normal. 7 Each of the dependent variables was normally distributed with the exception of readiness to change, which was slightly negatively skewed. Table 1 presents the means and standard errors for each variable across the first interval and across all three intervals. Time points that determined interval length were decided by the date of NA administration. Therefore, intervals varied in length due to the logistics of WSDOC administering hundreds of NAs state-wide per day. Counts for each dependent and independent variable were calculated from the first day of the interval until the last day of the interval. Reported are the average days during the first interval and average across all intervals. The first interval was longer than the subsequent 2 by over 8 days. The average for days in DS was larger for the first interval than the subsequent 2 by about 3 days. Across all intervals, there were 77 instances of DS (M = 21.15 days, sum = 1,629 days) for 74 individuals (not shown). Therefore, 222 of 1,224 intervals assessed DS relative to mental health functioning.
Descriptives (Offenders = 408; Total Observations = 1,224).
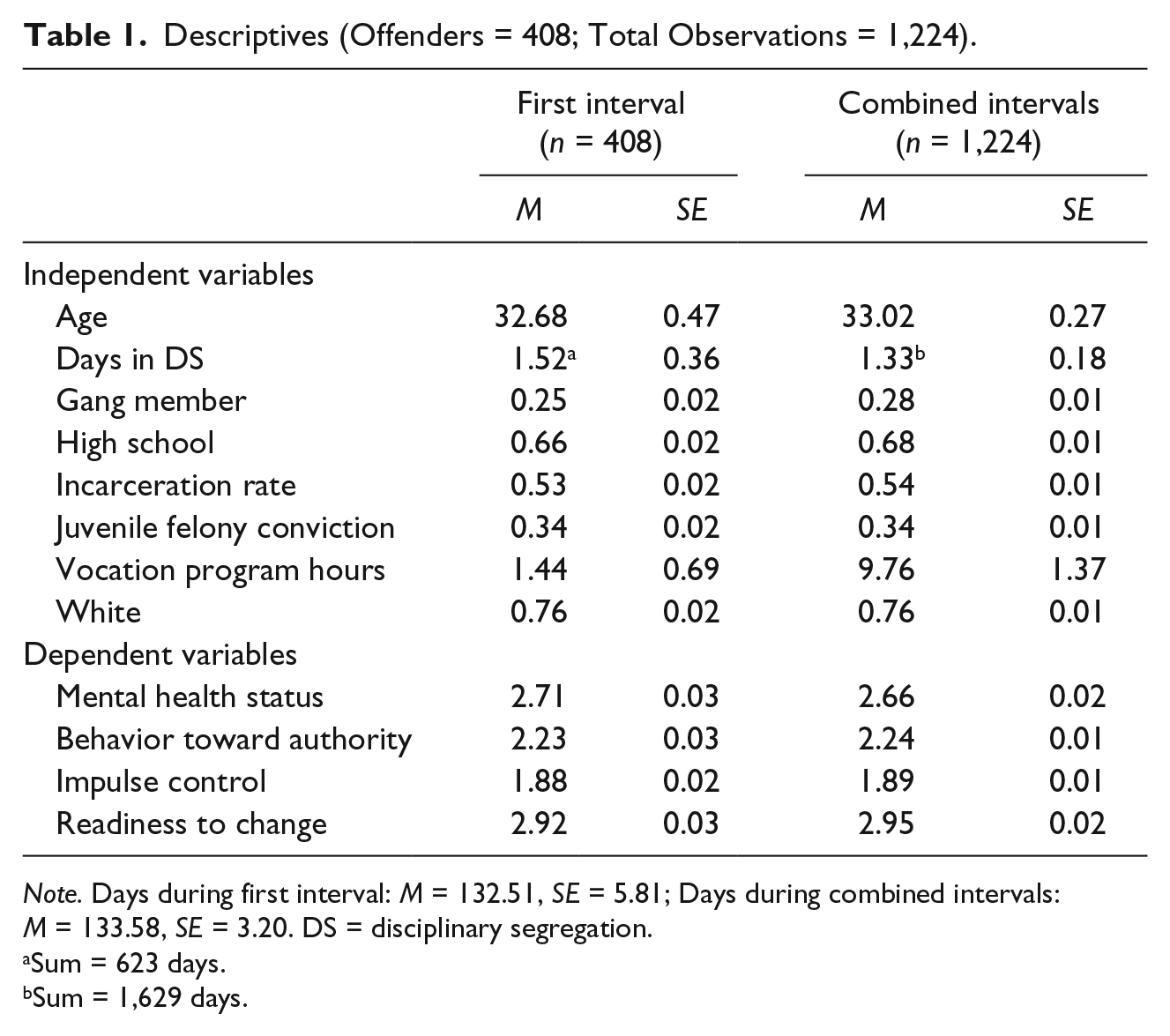
Note. Days during first interval: M = 132.51, SE = 5.81; Days during combined intervals: M = 133.58, SE = 3.20. DS = disciplinary segregation.
Sum = 623 days.
Sum = 1,629 days.
Across all three intervals, 28% of the sample was affiliated with a gang, 68% had graduated high school, 34% had a juvenile felony conviction, 76% were White, and the average incarceration rate during the interval was 0.54, indicating just over half of the time during the interval was spent incarcerated. The mental health status variable averaged 2.66 over all intervals, which indicates a very slight decrease from the first interval that may be related to chance. Readiness to change increased slightly across all intervals compared with the first interval. Behavior toward authority and impulse control did not vary in the aggregate across all intervals.
Mental Health Status
Findings for the primary models are presented in Table 2. When controlling for each of the covariates in the model, days in DS was negatively and significantly associated with mental health status (p < .05). There was a 1.7% decrease in the odds of receiving a higher mental health score for every day spent in DS. In addition, incarceration rate, age, having a juvenile felony conviction, being homeless, and gang membership significantly decreased the odds of being diagnosed with a higher mental health score. Homeless offenders had a decrease of 36.3% in the odds of being diagnosed with a higher mental health score when accounting for other variables in the model. Gang membership and homelessness each decreased the odds of receiving a higher mental health score by over 30%. As expected, older offenders and those who spent more time incarcerated both had a decrease in the odds of receiving a higher mental health score (p < .000). While no variable significantly increased the odds of a positive mental health status, Whites came close to our .05 threshold compared with non-Whites (p = .054). 8 Taken together, the results support the hypothesis that DS has a negative effect on offenders’ mental health, but greater impacts were observed for incarceration rates, criminal history, gang affiliation, and homelessness.
Multinomial Regression.
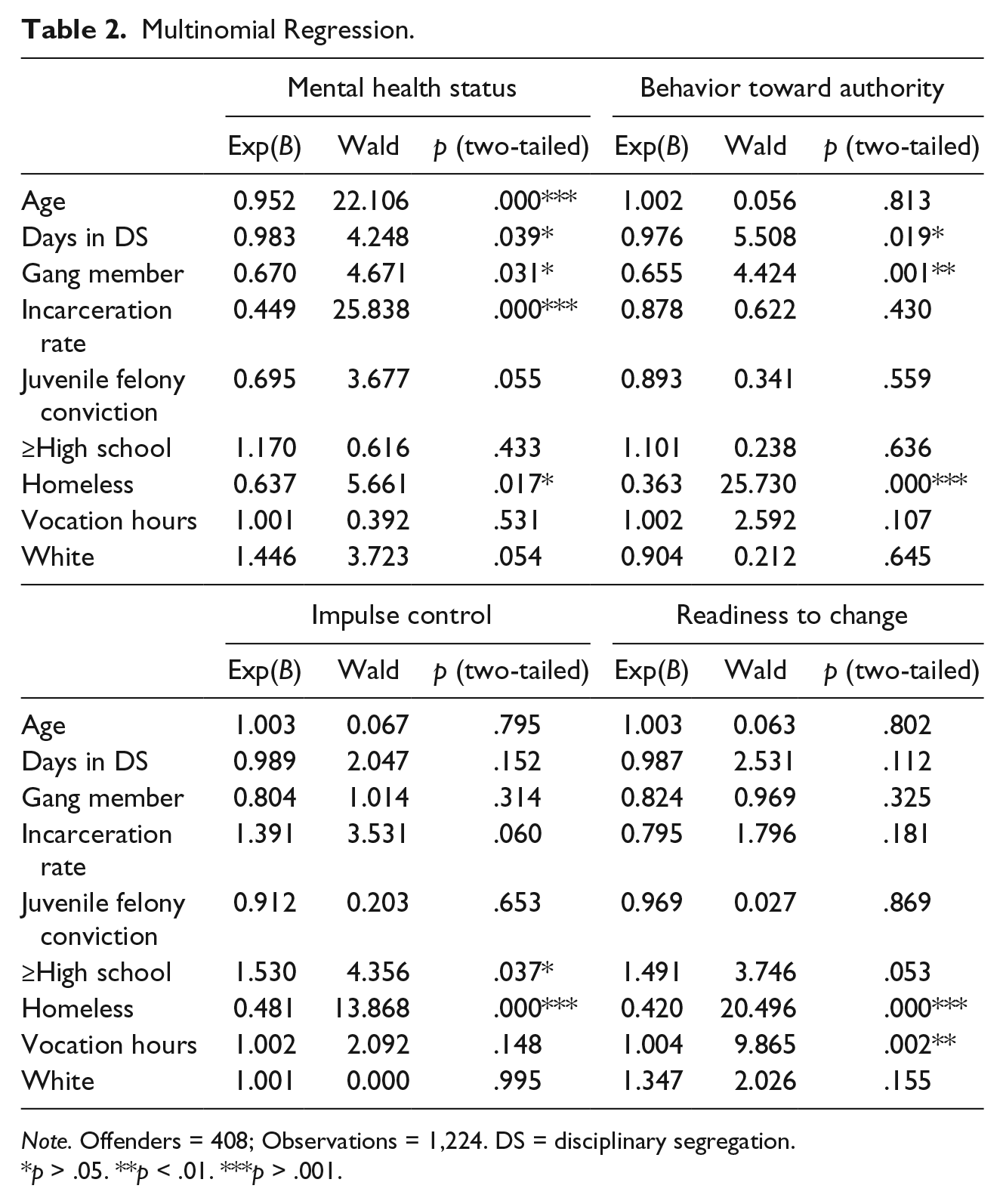
Note. Offenders = 408; Observations = 1,224. DS = disciplinary segregation.
p > .05. **p < .01. ***p > .001.
Behavior Toward Authority
Consistent with our second hypothesis, days in DS was negatively and significantly associated with behavior toward authority figures (p < .05). For every day spent in DS, there was a 2.4% decrease in the odds of exhibiting better behavior toward authority figure.
Likewise, being in a gang or being homeless decreased the odds of having a better behavior toward authority score by 34.5% and 63.7%, respectively. All of the variables that diminished offenders’ odds of exhibiting positive behavior toward authority are consistent with deviant adaptations to adverse circumstances or environments (gang membership and homelessness).
Impulse Control
Days in DS did not significantly affect the odds of an offender increasing their impulse control (Table 2). While this finding is contrary to our third hypothesis, it is consistent with Gottfredson and Hirschi’s (1990) theory of self-control, in that very few factors external to an individual’s intrinsic motivation can affect adult populations’ levels of self-control. Being homeless significantly decreased the odds of receiving a higher impulse control score by over 50%, accounting for the baseline of the other covariates (p <.000). Gottfredson and Hirschi would consider homelessness to be another manifestation of low self-control (e.g., an “analogous act”), even accounting for the observed changes in impulse control frequencies across intervals. Having a high school degree increased the odds of receiving a higher impulse control score over the course of our study by over 150% (p < .05), which is also consistent with Gottfredson & Hirschi’s central premise that one’s self-control is generally consistent across the life course.
Readiness to Change
Days spent in segregation did not affect the odds of being more ready to change (p = .112). Homeless offenders had over a 57% decrease in the odds of having an increased score when holding the other variables at their average (p < .000). Vocational programming hours significantly increased one’s readiness to change score (p < .01). For every hour in vocational programming, there was a 0.4% increase in the odds of an offender being more ready to change. While this increase in the odds seems small, the number of hours spent in vocational training averaged over 9.7 per interval analyzed. When only examining the 91 individuals who received training, the average over all intervals was over 97 hr.
Discussion and Conclusion
The current study examined the effects of DS on mental health functioning with an epidemiological approach. The goal was to understand how much isolation affects mental health. We found that the greater the number of days in DS, the more negative the mental health status and behavior toward authority outcome for offenders. 9 The negative effects of being isolated from the general population on offenders’ mental health and adjustment to prison is consistent with prior literature in this area (e.g., Andersen et al., 2000; Smith, 2004), but we do not find drastic, deleterious effects of isolation on mental health functioning, as prior researchers have (e.g., Haney, 2003). We believe our modest results reflect the typically mundane use and reuse of isolation as an organizational strategy to keep order when dealing with disciplinary infractions.
While the data show that factors other than DS can substantively erode offenders’ mental health functioning and risk/needs scores, being incarcerated in a general population prison environment for months at a time had greater negative effects than DS. This finding is consistent with recent meta-analyses on administrative segregation and prisoner mental health which demonstrated weak-to-moderate (at best) associations with prisoners’ mental health and anti-social behavior (Morgan et al., 2016; Smith et al., 2015). Morgan and colleagues recommend segregation be limited to offenders without mental health problems (SMI), except in the case of extreme circumstances related to safety, a recommendation that our study endorses.
Offenders’ gang affiliations decreased the odds of having better mental health scores and pro-social behavior toward authority to a greater extent than did their number of days in segregation. Finally, in all four models, offender homelessness was the only variable that was statistically significant and substantively related to the reduction in the odds of offender mental health and prison/community adjustment. Offenders who experienced homelessness in the past 6 months prior to their current incarceration had substantially lower odds than their non-homeless counterparts of increased mental health functioning. Taken together, the policy implications of our research suggest that addressing offenders’ psychosocial functioning could best be achieved through correctional/community programming targeting factors associated with criminal associates (gangs) and homelessness.
Our findings provide further evidence to administrators weighing the costs and benefits of segregation policy. While the practical benefits of taking dangerous and/or troublesome individuals out of general population inarguably take precedence in current policy, the detrimental effects on inmates’ psychological needs tied to recidivism should be given more weight than is currently the case. Inevitably, administrators need to develop order maintenance strategies that minimize the use of isolation and keep offenders and staff safe. Given the robust effects of homelessness on the outcome measures in our study, our research may add to policy recommendations of Morgan et al. (2016), in that offenders who were homeless prior to incarceration would benefit from special considerations during an infraction hearing—limiting their exposure to further social isolation or adding a condition of mandatory treatment.
Study Limitations
While our research makes a substantive contribution to the literature on SC, it is not without limitations. We used an epidemiological framework to ground our hypotheses and regression technique. However, our study did not contain explicit, standardized measures of health deterioration, as such measures, as they refer to SC, do not currently exist. Yet, though exploratory, a proxy for health deterioration may be mental health status as determined by physicians. Furthermore, we used institutional records rather than self-reports. The NA tool is not a validated scale, rather a pragmatic NA used to guide case management decisions. Therefore, there may be some inherent bias in these outcome measures, as the WSDOC’s personnel are a filter between the research team and the offenders. Finally, the psychological NA (i.e., the mental health measure) was conducted by medical staff and may have different biases than those administering the NA.
Our study was not experimental; rather, we assessed the population of male offenders who fit our selection criteria. It is possible that these selection criteria, including the lack of female offenders in it, resulted in findings that did not fully capture the effect of isolation on the four dependent variables for all offenders. Non-random assignment to each of our levels of isolation precludes us from determining succinct causal relationships between our predictors and outcomes. Furthermore, despite full cooperation from WSDOC, our measurement of the true DS population was incomplete due to logistical limitations. We also did not assess the severity of the violent infraction that led to DS: an avenue for future research to analyze. We included limited community-level variables that may be relevant to mental health and other psychological needs (e.g., social support groups, religious services, non-WSDOC case management). Finally, homelessness in and of itself is a form of social isolation that may have a comorbid relationship with other forms of isolation (e.g., incarceration, Rokach, 2005). Future research could focus on interaction terms that include homelessness and other personal and community-level variables that affect mental health. Finally, the use of DS was not assessed between facilities within the WSDOC, a potential source of variation in length and instance of DS.
Study Contributions
Using an increasingly desirable epidemiological approach, we were able to assess the dosage effect of a mundane application of isolation on offender outcomes. While much of the literature on isolation considers the effects of SC on offenders’ mental health functioning, we find that exogenous factors (e.g., homelessness) and endogenous factors (e.g., age) have greater effects on these outcomes than isolation. These results do not negate studies that have found SC to be harmful to the human psyche (e.g., Haney, 2003, 2006). Rather, our research suggests that in more ordinary and common applications of SC in prisons, the negative effects on mental health and supervision adjustment are present but overshadowed by sentencing policy (incarceration dosage), perceived opportunities for the future (education, gang involvement), and poverty (homelessness). Furthermore, our approach captures this mundane use better than one with stricter assumptions, because the number of endogenous and exogenous covariates not measured likely outweighs the ones that were. In non-experimental studies of real-life scenarios, researchers should give strong consideration to use of this approach.
Unknowns and Future Research
Future study in this area is warranted to validate our findings regarding those exposed to various levels of isolation. In correctional institutions, remedies to limit harm, while also maintaining the order and the safety of their staff and offenders, are under-developed. Since isolation may harm offenders who have no prior SMIs and exacerbate the symptoms of those who enter isolation with a SMI, it may be prudent to reduce these negative effects, and thus harm, by providing isolated offenders with greater social contact (Arrigo & Bullock, 2008; Smith, 2006) and alternatives to the use of SC (Kapoor & Trestman, 2016; Meyers et al., 2018). The former may be accomplished by increasing contact between staff and segregated offenders, increasing how many visits offenders may have, permitting access to social activities with other offenders, and increased communication between offenders and mental health or correctional staff. Labrecque and Smith (2019) extended this point by developing a risk assessment for institutional misconduct to identify high-risk offenders and supplement them with pro-social programming. In this way, the use of SC might not be reduced, rather pro-social initiatives (e.g., educational and vocational programming) may be increased to offset potential harms from SC. As reported by Kapoor and Trestman (2016), in an effort to reduce harm, some states have devised ways to reduce the use of SC, particularly for those re-entering communities.
In addition, in balancing the needs of correctional facilities (i.e., order maintenance and safety) and the consequences endured by offenders, it may be difficult to establish how much isolation is tolerable or how much social contact and programming is needed to offset the iatrogenic effects demonstrated here and by others (Smith, 2006). Ultimately, further research is needed to determine this balance, as it is likely it would vary among offenders placed in isolation.
Footnotes
Appendix
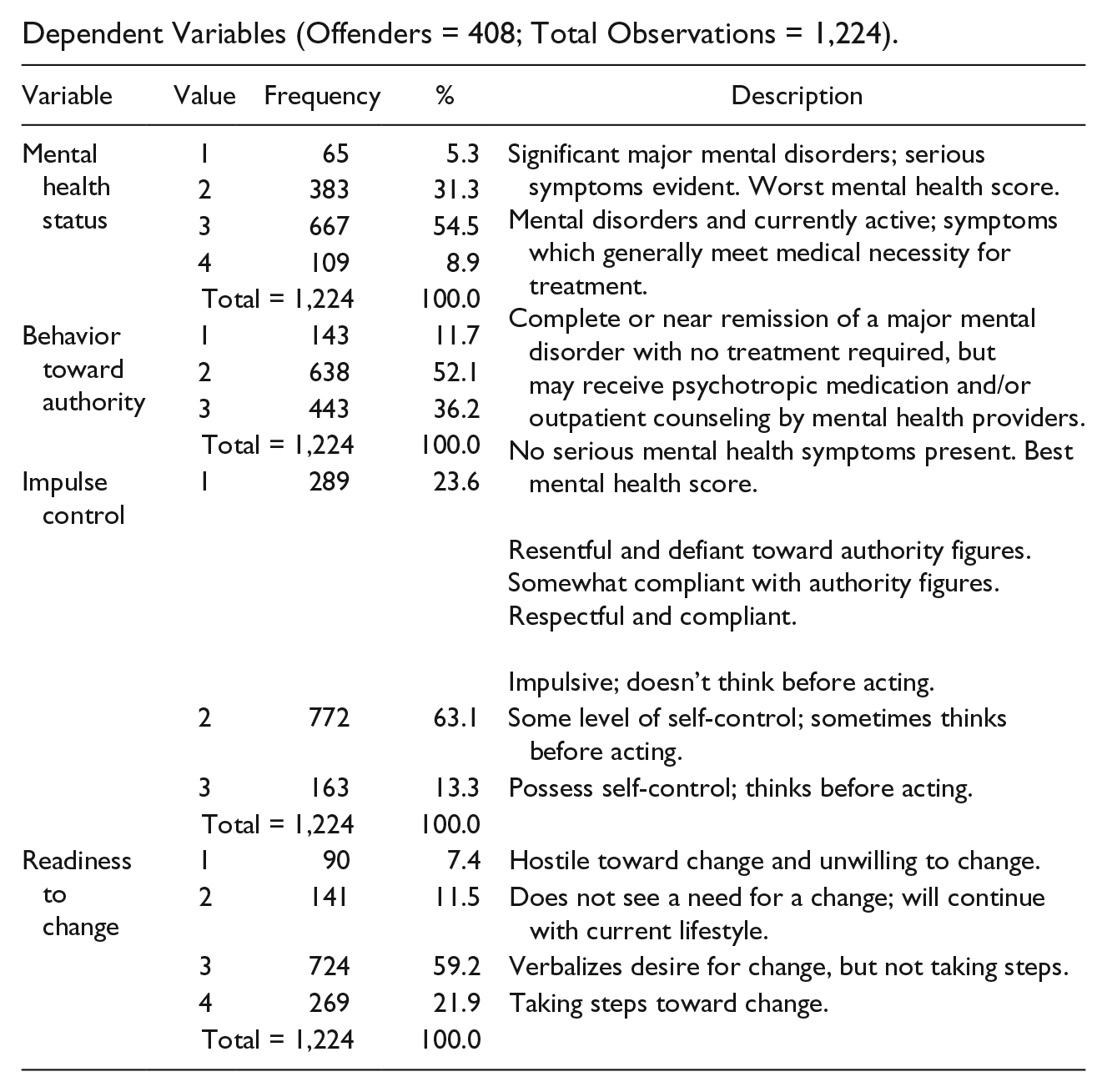
Dependent Variables (Offenders = 408; Total Observations = 1,224).
| Variable | Value | Frequency | % | Description |
|---|---|---|---|---|
| Mental health status | 1 | 65 | 5.3 | Significant major mental disorders; serious symptoms evident. Worst mental health score.Mental disorders and currently active; symptoms which generally meet medical necessity for treatment.Complete or near remission of a major mental disorder with no treatment required, but may receive psychotropic medication and/or outpatient counseling by mental health providers.No serious mental health symptoms present. Best mental health score. Resentful and defiant toward authority figures.Somewhat compliant with authority figures.Respectful and compliant. Impulsive; doesn’t think before acting. |
| 2 | 383 | 31.3 | ||
| 3 | 667 | 54.5 | ||
| 4 | 109 | 8.9 | ||
| Total = 1,224 | 100.0 | |||
| Behavior toward authority | 1 | 143 | 11.7 | |
| 2 | 638 | 52.1 | ||
| 3 | 443 | 36.2 | ||
| Total = 1,224 | 100.0 | |||
| Impulse control | 1 | 289 | 23.6 | |
| 2 | 772 | 63.1 | Some level of self-control; sometimes thinks before acting. | |
| 3 | 163 | 13.3 | Possess self-control; thinks before acting. | |
| Total = 1,224 | 100.0 | |||
| Readiness to change | 1 | 90 | 7.4 | Hostile toward change and unwilling to change. |
| 2 | 141 | 11.5 | Does not see a need for a change; will continue with current lifestyle. | |
| 3 | 724 | 59.2 | Verbalizes desire for change, but not taking steps. | |
| 4 | 269 | 21.9 | Taking steps toward change. | |
| Total = 1,224 | 100.0 | |||
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.