
Abstract
According to the World Health Organization, a major barrier to suicide prevention work is the social stigma surrounding suicide. Since clinical research has long shown that shame and guilt are often involved in suicide and suicide ideation, the present two studies explore the extent to which individuals associate shame and guilt with suicide ideation and behavior according to their cultural background. Using a scenario approach, 1,147 Americans in two separate studies read about a traumatic situation in which the target person experienced intense shame or intense guilt. A mini meta-analysis of these studies showed that all participants were more likely to link the experience of shame to suicidality than guilt. Additionally, participants from U.S. dignity states were more likely to report suicide ideation when the target experienced guilt as opposed to shame. Our findings support the notion that the centrality of the emotions of shame and guilt varies relative to the social context, which has implications on how others perceive suicide.
Keywords
Introduction
With a suicide rate of approximately 800,000 individuals per year, the World Health Organization (WHO, 2017) Mental Health Gap Action Programme has declared suicide a public health priority. However, the stigma surrounding suicide can be a major barrier to establishing adequate suicide preventions across the globe (WHO, 2017). For instance, Kelleher, Chambers, Corcoran, Williamson, and Keeley (1998) showed that countries with greater religious sanctions against suicide were less inclined to share their suicide data. In order to adequately identify and address reasons for suicide, it is imperative to finding ways to combat stigma. We argue that in order to address such barriers, it is critical to understand cultural differences in the perception of suicide and suicide behaviors. One means of addressing how individuals might perceive suicide is to investigate cultural differences in the reasons for suicide.
Patterns of suicide provide a glimpse into the culture of a society (e.g., Durkheim, 1897/1951; Lenzi, Colucci, & Minas, 2012). Mental illness, for example, is a key predictor of suicide in the United States. Yet, in India, suicides are more likely to occur in response to socioeconomic difficulties (e.g., Bhatia, Khan, Mediratta, & Sharma, 1987; see also Parkar, Dawani, & Weiss, 2008). These differences highlight how important it is that preventative efforts address how a society’s broader cultural values and scripts give rise to suicide. Since shared social meanings enable empathy among members of the same culture (Hardin & Higgins, 1996; LeVine, 2007), we expect members of a culture to predict if a given situation is likely to give rise to thoughts about suicide over others. In other words, even though suicide is typically viewed as an unacceptable behavior, shared cultural backgrounds influence what circumstances people might consider plausible or understandable reasons for suicide.
We present two studies that investigated cultural differences in the meaning of suicide. We examined whether individuals from U.S. honor cultures hold different notions about the emotional experiences that may prompt an individual to consider suicide than individuals from U.S. dignity cultures. We focused on the emotions of shame and guilt for two reasons. First, suicide research has well documented that thoughts about suicide often originate in these deeply negative emotional experiences (Hastings, Northman, & Tangney, 2002; Lester, 2010; Mokros, 1995; Sherman, 2014). Second, research also suggests that cultures differ in the extent to which their members are affected by these emotions (cf. Cohen, 2003). We explored whether U.S. honor cultures differ from U.S. dignity cultures in the extent to which they viewed shame and guilt as plausible antecedents of suicide.
Shame and guilt
Shame and guilt are a part of a class of emotions called the “self-conscious emotions.” These emotions, which include embarrassment and pride, occur in response to an evaluation of the self. Whereas the feeling of pride occurs in response to a positive evaluation of the self, shame, guilt, and embarrassment occur in response to a negative evaluation of the self (Lewis, 2008; Tangney, 2001; Wong & Tsai, 2007). Although similar in that respect, shame and guilt differ in important ways. Like embarrassment, shame occurs in response to a negative evaluation by real or imagined others (Sheikh, 2014; Tangney, 1995). However, the evaluation that elicits shame typically stems from violating important moral or social codes of conduct, whereas the evaluation that elicits embarrassment typically stems from relatively minor faux pas (Crozier, 2014; Keltner & Buswell, 1997). Shame’s link to morality renders it conceptually similar to guilt. Yet, the violation that evokes shame renders the global, or entire, self into question, whereas guilt occurs when a violation renders a negative evaluation of the behavior. Though they often co-occur, shame signals that one is a bad person, whereas guilt signals that one has done a bad deed (Giner-Sorolla, Castano, Espinosa, & Brown 2008; Tangney, Miller, Flicker, & Barlow, 1996).
Although both shame and guilt can serve important social functions, such as engaging in reconciliatory behaviors or improving the self (cf. Kemeny, Gruenewald, & Dickerson, 2004; Tangney, Stuewig, & Martinez, 2014), both have also been associated with the inclination to think about or to commit suicide. The feeling that one can never be rehabilitated in the eyes of others (shame) or the feeling of not being able to live with ones actions (guilt) is a recurrent theme in suicide notes and in the accounts of individuals having survived suicide attempts (Coster & Lester, 2013; Foster, 2003; cf. Shneidman, 1998). Some events can elicit such a strong sense of shame or guilt that individuals feel that suicide is their only way out (Baumeister, 1990; Bryan, Morrow, Etienne, & Ray-Sannerud, 2012; Hastings et al., 2002; Lester, 1997). For instance, when individuals are convinced that their social image is irreparably compromised and they feel an intense sense of shame, they may view suicide as a viable option and possibly end their lives. Likewise, when individuals feel that their conscience has been irrevocably damaged by their misdeeds, the ensuing sense of guilt might lead individuals to feel unable to continue living with what they have done (Lester, 1997; Pridmore & McArthur, 2008).
Honor and dignity cultures
Leung and Cohen (2011) distinguish U.S. honor cultures (i.e., the south) from U.S. dignity cultures (i.e., the north). Honor cultures are characterized by the belief that self-worth is synonymous with reputation (Cross et al., 2014; Nisbett & Cohen, 1996). This link renders one’s honor vulnerable to uncertainty and doubt. Since it is not a stable characteristic, continued active maintenance of one’s reputation is essential. This includes engaging in behavior that adheres to cultural mandates as well as engaging in defensive behavior to ward off potential threats to one’s honor (Kim, Cohen, & Au, 2010). Research on crime and violence has long documented that defensive honor maintenance entails elevated levels of aggression. For instance, homicide rates tend to be higher in honor cultures than in non-honor cultures, especially when it involves arguments between acquaintances (Cohen, 1998; Cohen & Nisbett, 1994; Nisbett, 1993).
Having to maintain one’s public image seems to make members of honor cultures more susceptible to suicide (Crowder & Kemmelmeier, 2014; Osterman & Brown, 2011). Suicide rates are elevated among older men in honor cultures, presumably because some members of this group have a harder time living up to the high expectations of masculinity that honor cultures place on them (Crowder & Kemmelmeier, 2017). Additionally, with members of honor states being sensitive to honor threats, mental illness is considered particularly stigmatizing. This deters individuals from honor states from seeking help when psychologically distressed (Brown, Imura, & Mayeux, 2014). A recent investigation demonstrated that a failure to seek treatment for depression could account, in part, for the higher suicide rates in U.S. honor cultures (Crowder & Kemmelmeier, 2017).
In dignity cultures, individuals themselves, and not others, have the power to define their self-worth. Leung and Cohen (2011) argue that for individuals to maintain dignity, they must behave in accordance with their own personal standards. A loss of dignity, in dignity cultures, reflects that an individual has not behaved according to his or her own personal standards. Although research examining the relationship between dignity culture and suicide is limited, evidence suggests that suicide can serve as a means to hold on to one’s dignity (Chochinov, Hack, McClement, Kristjanson, & Harlos, 2002; Van Der Maas, Van Delden, Pijnenborg, & Looman, 1991). For example, many of the arguments in support of physician-assisted suicide stress the importance that patients die with dignity (Hyde, 2001; Kade, 2000). Having a sense of free will over one’s own death may also provide psychosocial support (Lester, 2006; Mayo, 1998). Therefore, to the extent that individuals in honor cultures view the loss of honor as an understandable reason for suicide, individuals in dignity cultures may also associate the loss of one’s personal dignity with suicide.
Culturally appropriate emotional antecedents to suicide
Personal well-being is often contingent on meeting cultural expectations (e.g., Diener & Suh, 2000; Tov & Diener, 2007), and suicide can serve as an ultimate “way out” when people cannot meet important cultural mandates (cf. Crowder & Kemmelmeier, 2017; Tov & Diener, 2007). As such, differences in cultural expectations for behavior can give rise to differences in cultural constructions of suicide.
Arguably, the extent to which shame and guilt are viewed as antecedents to suicide differs across cultural contexts. Cohen (2003) argued that the experience of shame is a particularly potent emotion in honor cultures, as members are more sensitive to how their actions might be viewed by others (Markus & Kitayama, 1991; Singelis & Sharkey, 1995). Others have suggested that the experience of guilt is a particularly potent emotion in dignity cultures, as guilt signals that one has not met important personal standards (Leung & Cohen, 2011). We expected that members of honor cultures are more likely to think of suicide as the result of extreme shame as opposed to guilt, as they may be more likely to empathize with a tarnished reputation being a focal concern. Similarly, we argue that in dignity cultures, guilt is likely a critical emotion because it reveals that the integrity and self-defined worth of a person has been undermined by one’s own untoward behavior. Since members of dignity cultures place a premium on the ability to define their own sense of self-worth, behaving in a manner that challenges their ability to see the self as worthwhile may be intolerable. Thus, when someone engages in behavior that violates their self-definition of worth, members of dignity cultures are likely to be more understanding if the individual, in response to guilt, contemplates ending their life.
Perceived behavioral control
Whether shame or guilt is seen as appropriate precursors to suicide is likely to be dependent upon the actor’s controllability over his or her wrongdoing. An actor who deliberately violated a cultural norm is more likely to be held responsible for the event and its consequences (e.g., Siemer, Mauss, & Gross, 2007; Weiner, 1995). When such a violation is revealed, the actor can be expected to show culturally appropriate emotions of shame or guilt. Conversely, any displayed feelings of shame or guilt on the part of the actor signals that he or she acknowledges his or her agency and blameworthiness (Tracy & Robbins, 2006). If the distress is severe enough, observers might consider it plausible that such an actor is considering suicide—in part because the emotions of shame or guilt signal that the actor is accepting responsibility for his actions.
However, when an actor is not in control of his or her behavior, this circumstance may absolve him or her from responsibility for a wrongdoing, even when he or she experiences shame and guilt in response. That is, observers may be aware of the kind of emotional dilemma that an actor suffers; yet, they will not likely hold him or her accountable. Consequently, observers will not consider suicide or even thoughts of suicide an appropriate response. In short, depending on the cultural context, shame or guilt may serve as understandable instigators of thought of suicide primarily when behaviors are controllable.
Present research
To understand cultural differences in the meaning of suicide, the present two studies test whether suicide is viewed as appropriate or at least understandable depending upon cultural background and the precipitating emotional experience. Any differences could illuminate ways in which preventative strategists could adopt culturally sensitive approaches to suicide. Since honor cultures place greater emphasis on the social environment, we argue that members of these states, and those who endorse honor values more strongly, are more likely to conceptualize and think about suicide as a natural reaction to the reputation-focused emotion of shame than the individual-focused emotion of guilt. Therefore, we expect members of these states to anticipate that ashamed individuals will entertain thoughts of suicide and, therefore, be more understanding if they consider suicide in response to shame rather than guilt (Hypothesis 1). Additionally, since dignity cultures tend to emphasize individual experiences, we argue that members of such states will conceptualize suicide as a reaction to guilt than shame (Hypothesis 2). Thus, we anticipate members of these states to be more understanding of suicide in response to guilt as opposed to shame. These patterns should be more prominent if the shame or guilt is a response to one’s own actions, rather than an uncontrollable, traumatic circumstance (Hypothesis 3).
Study 1
We tested whether members of honor (vs. dignity) states conceptualized suicide as a reaction to shame (vs. guilt). Participants read one of eight short vignettes of a man who experienced a traumatic life-altering event. We varied the emotional experience of the man (shame vs. guilt) as well as the controllability of the event. Participants indicated the extent to which they thought the man would entertain thoughts of suicide, and how understanding they would be if the man did kill himself. We then examined whether the honor-dignity status of participants’ state of residence moderated their responses to the target individual as well as their personal endorsement of cultural values associated with honor and dignity.
Method
The study was administered using the online research tool SurveyMonkey. After providing consent, participants were randomly assigned to a 2 (controllability: controllable vs. uncontrollable) × 2 (vignette emotion: shame vs. guilt) between-subjects design. Participants read a story of a man named Sam who had experienced a traumatic event. Those assigned to the controllable condition read that the life-altering events came about due to Sam’s actions. Those assigned to the uncontrollable condition read the event occurred outside of his control. For participants in the shame condition, vignettes ended by describing Sam as having experienced extreme humility and a sense of shame. Those in the guilt condition read vignettes that ended with a description of Sam having experienced extreme personal anguish and a sense of guilt.
Participants were then asked to complete a series of questions regarding the vignette. The first set of questions asked participants to rate the extent to which they thought Sam had felt a series of 12 emotions including shame and guilt. They then indicated the extent to which they thought Sam was thinking about committing suicide and the extent to which they would understand if Sam had decided to commit suicide. Subsequently, all participants responded to a series of demographic questions, including their current state of residence.
Participants
We obtained two U.S. samples via the online crowdsourcing marketplace, Amazon Mechanical Turk (MTurk; fall of 2013 n = 215 and spring of 2014, n = 606). 1 Participants in 2013 received $0.20 for participating in a 5- to 10-minute survey and participants in 2014 received $1.50 for participating in a 25-minute survey. Twenty-three individuals participated in both rounds of data collection; thus, we removed their later entry. We also excluded seven participants (3.2% of 215) of 2013 who worked on the study for less than 90 seconds, as inattention to research materials might undermine data quality (Maniaci & Rogge, 2014). Similarly, 13 participants (2.2% of 583) in 2014 who worked on the study for less than 3 minutes (n = 6) and more than 40 minutes (n = 7) were excluded. On average, the 2013 participants took 195.44 seconds (SD = 108.98) and the 2014 participants 804.82 seconds (SD = 422.65). Across both samples, we removed an additional 37 individuals who failed the manipulation check and 17 individuals who either resided outside of the United States (n = 15) or in Washington, DC, (n = 2). In total, we excluded 74 participants (9.0%) of the overall sample. 2
Initial analyses showed no differences between the 2013 and the 2014 samples, all main and interaction effects, ps > .08; thus, data were combined. The data included 724 participants (54% female), 77% of which were White, 7% were African American, 7% were Asian, 5% were Hispanic/Latino, and 3% were Native American, multi-racial, or other. The average age of participants was 35 years (SD = 11.92; range: 18–81). Also, 24% reported that their annual household income was less than $25,000, 23% reported that it was between $25,000 and $39,999, 22% reported that it was $70,000 or more, and the remaining 31% reported that their annual household income was between $40,000 and $69,999.
Measures
Vignettes
We generated eight stories to assess participants’ understanding of suicide (see Appendix 1). In four of the stories, Sam did not have control of the event (e.g., as a train engineer, he could not stop his train from running over a teenager; coded 0). In the other set of four stories, Sam had direct control over the traumatic event (e.g., as a physician he made a wrong decision which disabled a child; coded 1). For all eight stories, Sam was described as either experiencing guilt (coded 0) or shame (coded 1) in response to the situation. The four vignettes in which Sam had control described this ending when the focus was on guilt
3
: Sam could not stop blaming himself for what he had done. Whenever he left his house, Sam was constantly reminded of the consequences of his actions. The thought of the pain he had caused and the regret of his behavior eventually grew to be too much to bear. Sam started wondering how he would be able to live with the guilt for what he had done. Sam knew that his family and most people in his community condemned him for what he had done. Whenever he left his house, Sam could not avoid running into someone who knew about, or who was in some way affected by what he had done. The public humiliation eventually grew to be too much to bear. Sam started wondering how he would be able to live with the shame that he had brought upon himself. Although Sam knew there was nothing he could have done, he could not stop blaming himself. The thought of the pain he had caused eventually grew to be too much to bear. Sam started wondering how he would be able to live with the guilt for what he had done. Sam felt as though those around him held him in contempt. The humiliation eventually grew to be too much to bear. Sam started wondering how he would be able to live with the shame that he had brought upon himself.
Suicide ideation
Using a five-point scale ranging from 1 (Not at All) to 5 (Extremely), participants responded a single item: “How much do you think Sam is thinking about suicide?”
Understanding
In 2013 and 2014, participants’ level of understanding was assessed using this item: “Would you find it understandable if Sam decided to commit suicide?” with participants again providing ratings on the five-point scale from 1 (Not at All) to 5 (Extremely). 4
Attributed emotions
To assess the emotions that participants perceived Sam felt, we included a modified version of Brebner’s (2003) emotion intensity scale. Using a five-point scale, participants were asked to indicate the intensity that they thought Sam felt five positive (affectionate, contentment, joy, pride, and shyness) and seven negative (anger, embarrassment, fear, guilt, disgust, sadness, and shame) emotions.
Honor-dignity
Cohen (1998) classified the U.S. states into honor and non-honor states based on cultural and historical considerations. U.S. states are categorized based on their census regions with Southern and Western states classified as honor states and Northeastern and Midwestern states as dignity states. Similar to previous research (e.g., Cohen & Nisbett, 1994; Hayes & Lee, 2005; Leung & Cohen, 2011), we used self-reported state of residence as criterion for whether participants were members of an honor or a dignity culture. Unfortunately, our Study 1 assessment did not include how long participants had lived in an honor or dignity state; however, as reported as part of Study 2, a large majority of residents in one particular type of state also went to high school in the same type of state (see also Hayes & Lee, 2005).
Collectivism
We relied on Vandello and Cohen’s (1999) State Collectivism Index to control for state-level collectivism. Scores range from 31 (least collectivistic) to 91 (most collectivistic).
Analysis plan
Using Stata’s structural equation modeling function, we adopted a path analysis approach to examine the impact of our emotion manipulation on the responses to the two outcome variables: the suicide ideation and suicide understanding items. Model 1 tests the first hypothesis (see Figure 1). Specifically, we examined the influence of our emotion manipulation (shame vs. guilt) on the actor’s perceived level of shame (path a), which ultimately predicted suicide ideation (path b) and understanding (path c). Thus, we expected perceived shame to mediate the effect of the emotion manipulation on both outcome variables. However, we did not necessarily assume that the mediation effect would be complete. As such, we also included the direct effects of the emotion manipulation on suicide ideation (path d) and suicide understanding (path e). To examine whether state honor-dignity status qualified the aforementioned effects, we specified it as a moderator for each pathway (paths f– j). Since we expected participants to respond similarly to each outcome variable, we also allowed them to covary (path k).
Conceptual model of the path analyses used to test Hypotheses 1 and 2. (Control variables are not displayed).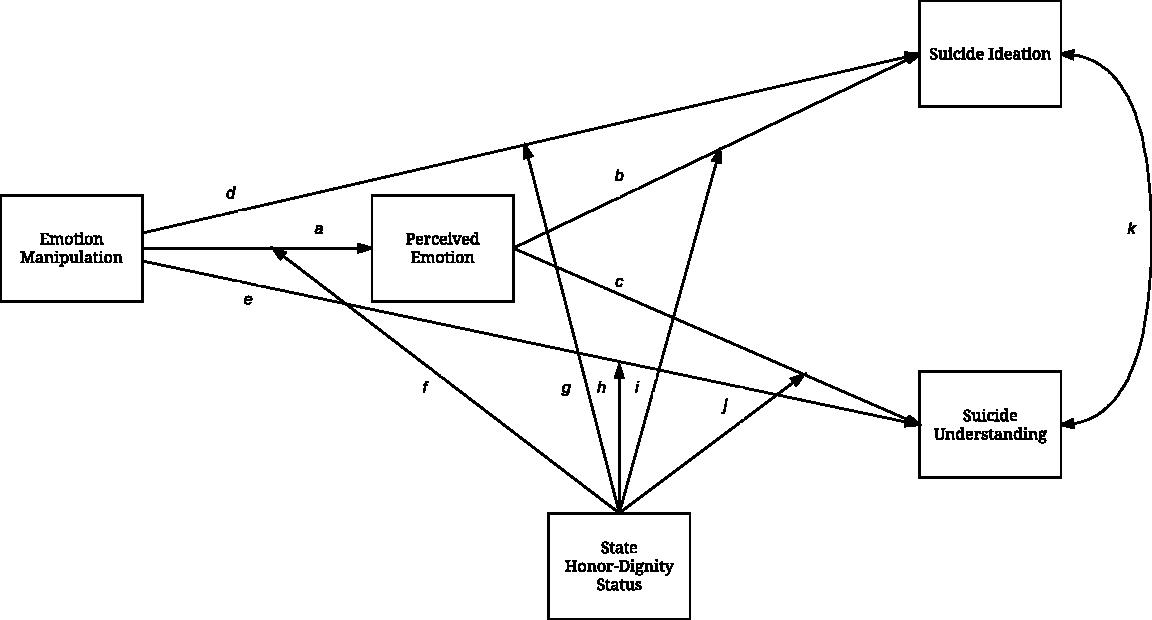
We also included two covariates (not shown in Figure 1): perceived guilt and state collectivism. Previous research has shown that shame and guilt have increasingly become conflated with one another within the United States such that shame has become less salient over time and has increasingly become replaced with more individualistic emotions such as guilt (Cohen, 2003; Fessler, 2007). Therefore, we expected that individuals may have a difficult time differentiating between the two emotions and we examined the effect of vignette emotion on perceived shame and the outcomes while controlling for perceived guilt. Indeed, in our own Study 1, perceived shame and guilt were highly correlated (r = .60). Further, since a state’s honor-dignity status and state-level collectivism are positively correlated (r = .34) but are differentially associated with suicide (Crowder & Kemmelmeier, 2014), state collectivism was included as a covariate. Statistical significance of parameter estimates was determined using robust standard errors (RSE).
The same conceptual model displayed in Figure 1 was also used to test the second hypothesis. We used the same approach except that we examined perceived guilt as the mediator between the emotion manipulation and the two outcome variables, while controlling for perceived shame. Finally, to test our third hypothesis, we used the group command when examining both models to generate separate coefficients for each controllability condition.
Stata reports the path coefficients, rather than the overall between-subjects effects. Therefore, to understand our results, it is important to know that for our dummy variables, groups coded as 0 (guilt condition and dignity-state) are the reference groups. When involved in a two-way interaction, the coefficient associated with the main effect reflects the difference in means when the moderating variable is 0. The interaction term reflects the change in the mean difference as a function of the moderating variable. For example, a main effect for the emotion manipulation on perceived shame reflects the effect when state honor-dignity status is 0 (dignity states). A significant interaction term with state honor-dignity status would show the extent to which that effect (mean difference) varied for members of honor states. In all analyses, and throughout our paper, we set our significance level at p = .050, though regard effects at p < .100 as marginally significant, indication a noteworthy trend.
For simplicity, we do not report findings for the covariates. Note that, across both studies, perceived shame and perceived guilt were consistently related, ps < .001, and state-level collectivism was never related to perceived shame, ps > .06, nor the suicide understanding item, ps > .37. However, state-level collectivism was occasionally related to the suicide ideation item, with bs ranging from −0.12 to −0.002 and ps ranging from .01 to .97.
Results
Hypothesis 1: Is suicide more closely tied to shame for members of honor states?
Stata reports the standardized root mean residual (SRMR) when analyses are based on RSE. For the following model, SRMR indicated good model fit, SRMR = 0.058, markedly below the 0.080 cutoff suggested by Hu and Bentler (1999).
Controllable condition
The effect of our emotion manipulation on perceived shame (path a) showed that those in the shame condition perceived Sam to be experiencing more shame than those in the guilt condition, β = 0.172, RSE = 0.074, p = .020. Members of honor states also perceived more shame than members of dignity states, β = 0.143, RSE = 0.062, p = .021. Both the emotion manipulation and state honor-dignity status were involved in a two-way interaction effect, β = −0.172, RSE = 0.073, p = .019 (path f). The additive effect of the coefficients illustrates that the difference in perceived shame as a function of the manipulation condition occurred among those from dignity states. This difference was not significant among members of honor states, β = −0.014, RSE = 0.034, p = .691. Although members of honor states were more likely to perceive shame than members of dignity states, this did not vary across emotion conditions.
We then turned our attention to the suicide ideation item. Results indicated that perceived shame was positively related to suicide ideation, β = 0.281, RSE = 0.092, p = .002 (path b). There was no main effect of state honor dignity status, β = −0.124, RSE = 0.072, p = .084, and state honor-dignity status did not moderate the relationship between perceived shame and perceived suicide ideation, β = − 0.033, RSE = 0.074, p = .653 (path i). Examining our emotion manipulation showed a somewhat different pattern. Those who read that Sam was experiencing shame were less likely to report that he was thinking of committing suicide than those who read that Sam was experiencing guilt, β = −0.195, RSE = 0.080, p = .015 (path d). This effect was qualified by state honor-dignity status, β = 0.258, RSE = 0.095, p = .007 (path g). Thus, the finding that those in the shame condition reported less suicide ideation occurred among those from dignity states. Members of honor states did not differ in how likely they thought Sam was thinking of suicide as a function of the emotion manipulation, β = 0.084, RSE = 0.066, p = .202. No significant effects emerged when examining suicide understanding, all ps > .08.
Uncontrollable condition
When faced with uncontrollable situations, those who read that Sam experienced shame perceived him to be experiencing more shame than those who read that he experienced guilt, β = 0.182, RSE = 0.072, p = .012 (path a). State honor-dignity status also predicted perceived shame, β = 0.158, RSE = 0.066, p = .017, and suicide ideation, β = 0.139, RSE = 0.071, p = .050. Specifically, those from honor states perceived more shame and reported that Sam was more likely to be considering suicide than members of dignity states. No other effects approached statistical significance in the uncontrollable condition, ps > .06.
Mediation analyses
Standardized path coefficients for honor and dignity states.

Asterisks for the coefficients of the mini-meta analysis indicate that the 95% confidence intervals did not include zero.
+p ≤ .10, *p ≤ .05,**p ≤ .01, ***p ≤ .001.
Average perceived shame by study, emotion manipulation, and state honor-dignity status.
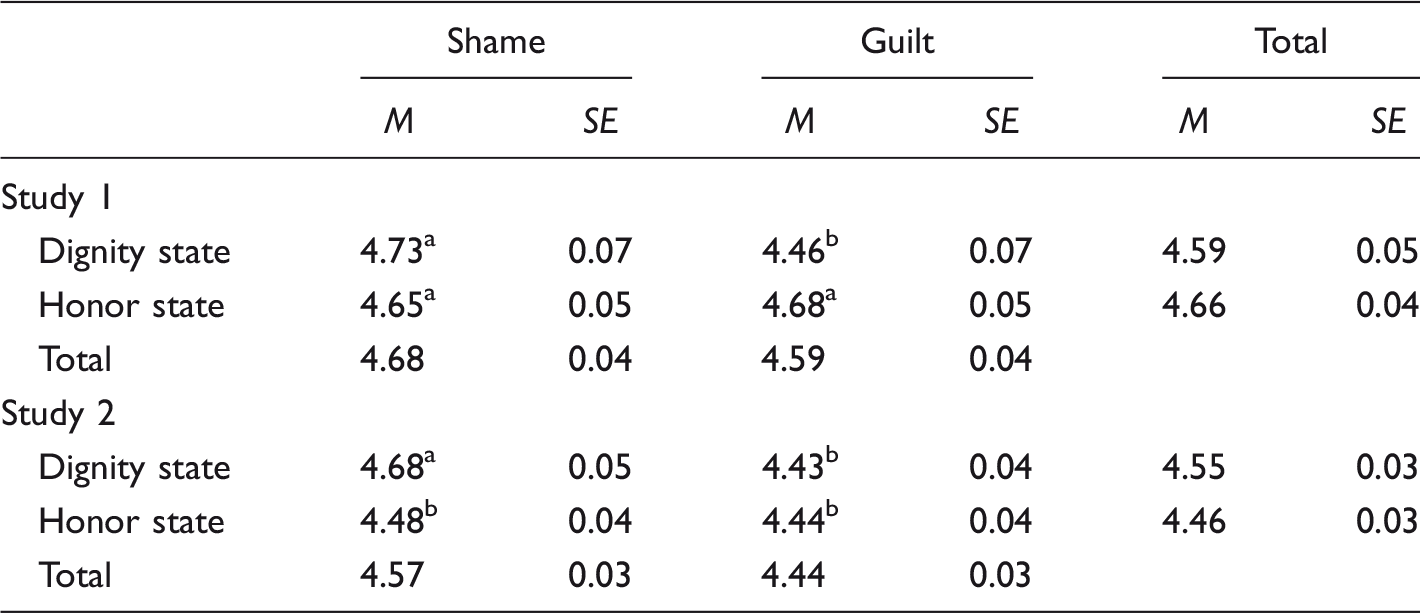
These marginal means reflect analyses that control for perceived guilt. The perceived emotions of Study 1 reflect the items of Brebner’s (2003) scale for those in the controllable condition only. The perceived emotions of Study 2 reflect Tangney’s (1994) State Shame and Guilt Scale (SSGS). Means with different superscripts within the same panel differ at p < .05.
Hypothesis 2: Is suicide more closely tied to guilt for members of dignity states?
To test our second hypothesis, we followed the same series of steps but included perceived guilt as the mediating variable and perceived shame as the covariate, with the model again fitting the data well, SRMR = 0.068.
Controllable condition
Average perceived guilt by study, emotion manipulation, and state honor-dignity status.

These marginal means reflect analyses that control for perceived shame. The perceived emotions of Study 1 reflect the items of Brebner’s (2003) scale. The perceived emotions of Study 2 reflect Tangney’s (1994) State Shame and Guilt Scale (SSGS). Means with different superscripts within the same panel differ at p < .05.
Perceived guilt was not associated with suicide ideation, β = 0.078, RSE = 0.075, p = .299 (path b). However, we did find an effect of our emotion manipulation, β = −0.187, RSE = 0.082, p = .022 (path d), which showed that those in the guilt condition were significantly more likely to indicate that he was thinking of committing suicide than those in the shame condition. Although there was no statistical difference between members of honor and dignity states in perceived suicide ideation, β = −0.117, RSE = 0.070, p = .094, state honor-dignity status did moderate the effect of the emotion manipulation, β = 0.243, RSE = 0.097, p = .012 (path g). The additive effect of these coefficients indicated that members from dignity states were significantly more likely to report suicide ideation in the guilt condition than the shame condition, but there was no difference among members of honor states, β = 0.076, RSE = 0.066, p = .246. All other paths were not significant, ps > .08.
When examining suicide understanding, findings showed that greater levels of perceived guilt were marginally associated with greater levels of suicide understanding (path c), β = 0.133, RSE = 0.071, p = .059. There was no main effect of state-honor-dignity status, β = 0.006, RSE = 0.074, p = .941; however, this was qualified by perceived guilt, β = −0.118, RSE = 0.052, p = .024 (path j). This pattern indicates that the positive association between perceived guilt and suicide understanding emerged among members of dignity states. Perceived guilt was not associated with suicide understanding for members of honor states, β = −0.042, RSE = 0.073, p = .571. No other pathways to suicide understanding were statistically significant, ps > .15.
Uncontrollable condition
The emotion manipulation did not have any effect on perceived guilt, β = −0.084, RSE = 0.075, p = .260 (path a). We found that perceived guilt was positively related to suicide ideation, β = 0.234, RSE = 0.117, p = .047 (path b), but no other pathways reached significance, ps > .07.
Mediation analyses
Examining the indirect effects between our emotion manipulation and our two outcome variables via perceived guilt showed that there were no significant mediation effects in either the controllable or the uncontrollable conditions, ps > .15.
Discussion
Findings of Study 1 lent partial support for all three hypotheses. We hypothesized that that members of honor states would be more likely to associate shame with suicide compared to guilt. Although our findings do not show this directly, they do suggest that members of honor states may be more sensitive to shame-cues. Specifically, we found that members of honor states were much more likely to report that Sam was experiencing shame across both conditions than participants from dignity states. This, in turn, was associated with a greater inclination to report that he would consider suicide. Members of dignity states differentiated between the two contexts more easily in regard to perceived shame.
Findings also confirmed our second hypothesis. Members from dignity states were more likely to report suicide ideation in the guilt condition than the shame condition and were more likely to be understanding of suicide the more guilt they thought Sam experienced. All of these effects occurred when Sam had control over the situation, which supports our third hypothesis. When a trauma is not the fault of the actor, others are less likely to assign the kind of blame that would have made suicide seem warranted.
Study 2
Study 2 sought to replicate and extend our first study. Because findings of Study 1 supported our hypothesis that the effects would emerge when Sam was in control of his situation, participants in Study 2 only saw one of the four vignettes from the controllable condition. Second, since members of honor states were equally likely to report that Sam was experiencing shame for both emotion conditions, we strengthened our emotion manipulation so participants could differentiate between perceived shame and guilt. We also removed any mention of “shame” or “guilt” from the vignettes. Finally, we expanded our assessment of shame and guilt using a widely used, psychometrically sound scale.
Method
The study was administered using the online research tool Qualtrics. As in Study 1, participants were randomly assigned to one of the two vignette emotion conditions (shame vs. guilt) and asked to complete a series of questions regarding how much they felt Sam had felt shame and guilt. Except where noted, all other aspects of Study 2 were identical to Study 1.
Participants
We obtained a sample of 426 U.S. MTurk “workers” who participated in exchange for $1.00 for an expected 10-minute study. Using the same reasoning as Study 1, we removed the responses of 14 individuals who worked on the study for less than 180 seconds (less than 3 minutes) and 6 individuals who worked on the study for more than 1800 seconds (more than 30 minutes) to correct for inattention (5% of the overall sample). Additionally, five individuals were excluded who did not attend high school in the United States. The final dataset consisted of 401 participants whose average time completing the study took 518.28 seconds (SD = 263.84).
Fifty-two percent of these participants were female, 82% were White, 9% were African American, 7% were Asian, 6% were Hispanic/Latino, and 2% were Native American, multi-racial, or other (participants were allowed to select all racial/ethnic categories that applied to them). The average age of participants was 37 years (SD = 12.15; range: 19–75). Also, 25% reported that their annual household income was less than $25,000, 22% reported that it was between $25,000 and $39,999, 24% reported that it was $70,000 or more, and the remaining 29% reported that their annual household income was between $40,000 and $69,999.
Measures
Vignettes
To strengthen our emotion manipulation, we revised the four vignettes by strengthening the language around the emotional experience of the actor, Sam. When Sam was experiencing shame, we highlighted the public repercussions of his actions. For example: Sam knew that his family and most people in his community condemned him for what he had done. Whenever he left his house, Sam could not avoid running into someone who knew about, or who was in some way affected by what he had done. At one point, he was in the grocery store line and he heard people whispering all around him. Eventually someone burst out: “You are the guy who ruined our town!” When Sam looked up, everybody in the busy store was looking at him. Sam just ran out of the store, leaving his full cart behind. Over time, the public humiliation eventually grew to be too much to bear. Sam could not stop blaming himself for what he had done. Whenever he left his house, Sam could not avoid being reminded of the consequences of his actions. At one point, in front of the grocery store he saw a beggar with a sign “Please help – lost job and home” – and he recognized in the older man a former worker at the company. Inside the store, he overheard a conversation between two women with one telling the other that her son had to drop out of college because they could not afford it any more after both she and her husband had lost their jobs when the company closed. The thought of the pain he had caused and the regret of his behavior eventually grew to be too much to bear.
State shame and guilt scale
To examine the extent to which participants perceived Sam to be experiencing shame and guilt, we used a revised version of Marschall, Sanftner, and Tangney’s (1994) State Shame and Guilt Scale. These items are designed to address an individual’s present feelings of shame, guilt, and pride. Although our analyses only focus on the shame and guilt subscales, for this study, we tailored all items to address participants’ perceptions of the extent to which Sam, “…wants to sink into the floor and disappear,”(sample item of shame scale; α = .77), “…feels remorse, regret,” (sample item of guilt scale; α = .84), and “…feels good about himself,” (sample item of pride scale; α = .82). 5
State culture
In Study 2, we assessed both current state of residence as well as the state in which participants attended to high school (Cohen, 1998). These two states might not coincide if participants moved across states or were originally from outside of the United States. However, in the majority of cases (71%), the two states were the same. If the two states varied, participants had mostly migrated from one honor (or dignity) state to another (82%). Put differently, for 86% of our participants the kind of state in which they had attended high school was the same as the kind of state in which they currently resided. We used the state in which participants went to high school to generate our state culture variables. Use of either state variable produced essentially identical results.
Results
We ran the same path models examining perceived shame, model fit SRMR = 0.046, and perceived guilt, SRMR = 0.037, as in Study 1, though we only focused on the vignettes in which Sam had control, since there were no subgroup analyses.
Model 1: Is suicide more closely tied to shame for members of honor states?
Similar to Study 1, we found that that our emotion manipulation was effective such that those in the shame condition perceived Sam to be experiencing greater shame than those in the guilt condition, β = 0.182, RSE = 0.047, p < .001 (path a). However, members from honor states did not differ from members of dignity states in perceived shame, β = −0.010, RSE = 0.048, p = .839. A significant two-way interaction between state honor-dignity status and the emotion manipulation, β = −0.139, RSE = 0.059, p = .019 (path f) showed that, as before, the effect of the emotion manipulation on perceived shame occurred among members of dignity states, but not among members of honor states, β = 0.033, RSE = 0.042, p = .434. As can be seen from Table 2, although efforts to emphasize the distinction between the shame and guilt condition were somewhat effective among members of honor states, relative to the pattern shown in Study 1, members of dignity states were still much more sensitive to the emotion cue; members from honor states were equally likely to perceive shame across both conditions.
Examining suicide ideation showed that higher levels of perceived shame were positively with greater reports of suicide ideation, β = 0.276, RSE = 0.109, p = .011 (path b). No other effects reached statistical significance, ps > .27.
Turning to suicide understanding also revealed a positive effect of perceived shame, β = 0.224, RSE = 0.096, p = .020 (path c): the more that participants thought that Sam experienced shame, the more understanding they said they would be if he decided to commit suicide. Further, members of honor states were equally likely to be understanding as members of dignity states, β = −0.091, RSE = 0.071, p = .200. However, a two-way interaction between perceived shame and state honor-dignity status, β = −0.202, RSE = 0.082, p = .014 (path h), indicated that the positive relationship between perceived shame and suicide understanding occurred among participants from dignity states. Perceived shame was not associated with suicide understanding among participants from honor states, β = −0.015, RSE = 0.091, p = .868.
Mediation analyses
Similar to Study 1, analyses of the indirect effects showed that perceived shame mediated the pathway from the emotion manipulation to suicide understanding, β = 0.136, RSE = 0.066, p = .040, for members of dignity states. This path was marginally significant for suicide ideation, β = 0.097, RSE = 0.057, p = .090. Neither pathways approached significance for members of honor states, ps > .39.
Model 2: Is suicide more closely tied to guilt for members of dignity states?
Again, we found that those in the guilt condition reported that Sam experienced greater levels of guilt than those in the shame condition, β = −0.199, RSE = 0.051, p < .001 (path a). Further, a significant two-way interaction between the emotion manipulation and state honor-dignity status produced a similar pattern as in Study 1 (path f). That is, the difference in perceived guilt as a function of our emotion manipulation occurred for members of dignity states, β = 0.135, RSE = 0.061, p = .027, but not members of honor states, β = −0.055, RSE = 0.040, p = .171. From a different angle, this interaction effect showed that when they read that Sam experienced guilt, no difference between members of honor and dignity states emerged, β = −0.032, RSE = 0.047, p = .499. Yet, when participants read that he experienced shame members of honor states reported significantly higher levels of perceived shame than members of dignity states, β = 0.111, RSE = 0.051, p = .028.
Perceived guilt was positively associated with suicide ideation, β = 0.201, RSE = 0.096, p = .037 (path b), but not suicide understanding, β = 0.141, RSE = 0.093, p = .131 (path c). All other paths, ps > .20.
Mediation analyses
Analyses of the indirect effects showed that perceived guilt did not mediated the pathway from the emotion manipulation to either outcome variables regardless of state honor-dignity status, ps > .15.
Discussion
Results of Study 2 showed that members of honor cultures were equally likely to perceive both shame and guilt across emotion conditions. This pattern suggests that members of dignity states were more sensitive to the emotion cues than members of honor cultures states. Although weak, indirect analyses with regard to perceived shame also replicated: For both studies, perceived shame mediated the effect of the emotion manipulation on suicide ideation for members of dignity states only. A discussion of these findings is provided below.
Internal meta-analysis
Some of the differences we found across studies are likely due to differences in methodology. To obtain a clearer picture of the effects, we summarize our findings using Goh, Hall, and Rosenthal’s (2016) “mini meta” approach of the standardized beta coefficients. To compare “apples-to-apples,” we analyzed the standardized coefficients of the controllable condition of Study 1 to those of Study 2 for honor and dignity states, separately. Using this approach is advantageous because it provides more precise and reliable estimates of our effects across studies and therefore provides a clearer picture of the replicability of these findings (see Table 1). Given the nature of this method, 95% confidence intervals are reported, rather than p values, to reflect statistical significance.
Hypothesis 1: Is suicide more closely tied to shame for members of honor states?
Results showed that the effect of the emotion manipulation on perceived shame was only significant for members of dignity states, β = 0.165, 95% CI [0.052, 0.274], not members of honor states, β = 0.012, 95% CI [−0.081, 0.104]. For both groups, perceived shame was positively associated with suicide ideation, βHonor = 0.262, 95% CI [0.174, 0.346]; βDignity = 0.238, 95% CI [0.127, 0.343], but was only associated with suicide understanding for members of dignity states, β = 0.172, 95% CI [0.059, 0.280], and not members of honor states, β < 0.001, 95% CI [−0.092, 0.092]. Regardless of individuals’ state honor-dignity status, the emotion manipulation did not have a direct effect on either suicide ideation, βHonor = 0.035, 95% CI [ −0.058, 0.127]; βDignity = −0.058, 95% CI [−0.170, 0.055], or on suicide understanding, βHonor = 0.076, 95% CI [−0.017, 0.167]; βDignity = 0.081, 95% CI [−0.033, 0.193]. Thus, individuals were equally likely to say that Sam was thinking of suicide no matter if they read that he experienced shame or guilt. None of the aggregated indirect effects were statistically significant (all confidence intervals encompassed zero).
Hypothesis 2: Is suicide more closely tied to guilt for members of dignity states?
Again, we see that the emotion manipulation on perceived guilt was only significant for members of dignity states, β = −0.180, 95% CI [−0.288, −0.067], not members of honor states, β = −0.046, 95% CI [−0.138, 0.047]. However, perceived guilt was only related to suicide ideation for members of dignity states as well, β = 0.158, 95% CI [0.044, 0.267], not members of honor states, β = 0.005, 95% CI [−0.085, 0.095]. Perceived guilt did not predict suicide understanding across state-honor status, βHonor = 0.074, 95% CI [−0.018, 0.164]; βDignity = 0.079, 95% CI [−0.034, 0.191]. Again, given the similarity of the models, the emotion manipulation did not have a direct effect on suicide ideation, βHonor = 0.035, 95% CI [−0.058, 0.127]; βDignity = −0.058, 95% CI [−0.170, 0.055], nor suicide understanding, βHonor = 0.075, 95% CI [−0.018, 0.167]; βDignity = 0.081, 95% CI [−0.033, 0.193], across state honor-dignity status. Finally, none of the indirect effects were statistically significant (all confidence intervals encompassed zero).
General discussion
The central goal of this research was to understand whether the conditions under which suicide is seen as more or less acceptable vary across cultures. Two studies focused on cultural differences within the United States. We hypothesized that members from honor and dignity states would respond differently to suicidal thoughts depending on the antecedent emotion. Specifically, we expected members of dignity states would be more likely to link suicidality to the experience of guilt, since it indicates that one has behaved in a manner that undermines one’s personal standards and sense of self. Indeed, our findings showed that members of dignity cultures were more likely to associate perceived guilt to suicide ideation compared to members of honor cultures. To the best of our knowledge, this is the first study that demonstrates that members of dignity culture within the United States respond differently to guilt than to shame, and to link that difference to perceptions of suicide. Far more work has been done looking at the relationships among honor cultures, shame, and suicide (cf. Cohen, 2003; Hollander, 2003; Lester, 1997; Leung & Cohen, 2011).
Since it has been shown that members of honor cultures are particularly responsive to the experience of shame given their sensitivity to social threats (Cohen, 2003; Leung & Cohen, 2011), we also expected that members of honor states would be more understanding of suicide in response to shame than members of dignity states. However, this association was not found. Although our findings supported the notion that members of honor cultures were more sensitive to the experience of shame in that they were equally likely to perceive it across shame and guilt eliciting events, the perceived experience of shame was associated with greater reported ideation for members of honor and dignity states equally.
Shame is an incredibly potent emotion. As mentioned, findings from this research show that the influence of shame on perceptions of suicide occurred for everyone, regardless of cultural background. This pattern supports the extensive literature that shows the experience of shame, especially the inescapable experience of shame, can motivate an individual to end his or her life (Breed, 1972; Bryan et al., 2012; Kolves, Ide, & Leo, 2011). When compared to guilt, individuals who participated in the present research were much more likely to associate suicide ideation to shame than to guilt. This is likely due to differences in the nature of these self-conscious emotions. Whereas the blame is largely placed on the behavior with regard to guilt, it is more likely a reflection of the individual, or self, with regard to shame (Giner-Sorolla et al.,2008; Lewis, 2008; Tangney, 2001). This can have devastating consequences on the individual’s ability to cope, as it may seem far easier to change one’s behavior than it is to change one’s self.
This may shed some light as to why members of dignity states were more receptive to our emotion cues than members of honor cultures. Specifically, it may be that members of honor states respond equally to both shame and guilt since they are both self-conscious emotions (Lewis, 2008; Tangney, 2001). Given that both emotions reflect a negative evaluation of the self, members of honor states may be sensitive to circumstances that elicit both. Regardless of whether the event reflects an evaluation of the global self or the behavior, any negative evaluation of the self may be perceived as a threat to one’s reputation. Members of dignity states may be more likely to pick up on the distinction. If they are not led to believe that a person has been humiliated then they may have no reason to suspect so. However, when they are told that the individual has been humiliated, they responded accordingly. Consistent with this speculation, we observed that ratings of perceived shame and perceived guilt were more closely correlated among participants from honor states compared to those from dignity states (Study 1 (controllable condition) rHonor = .78 vs. rDignity = .67, Fisher Z = −2.21, p = .03; Study 2 rHonor = .81 vs. rDignity = .69, Fisher Z = −2.52, p = .01).
Interestingly, different trends emerged depending on whether we examined participant predictions of suicide ideation or their understanding of suicide. For the most part, effects that we found were associated with suicide ideation. We expect that this was because each outcome tapped into suicide understanding in both indirect and direct ways. Whereas our suicide ideation measure asked participants to reflect on the mental state of the target character Sam, our suicide understanding measure asked participants to report their own personal beliefs toward the matter. Asking participants to indicate the likelihood that Sam is thinking of suicide is more likely to portray a form of understanding that encompasses perspective taking and empathy than asking them about understanding outright. We posit that reporting suicide ideation allowed participants to project their own subjective understanding of Sam’s situation and of suicide onto this target person without necessarily running afoul of the otherwise strong cultural prohibitions against suicide. Put differently, the hypotheticality of the scenario may have allowed it to serve as a cultural Rorschach test with regard to a cultural understanding of suicide. Because our measure of suicide understanding likely addresses participants’ attitudinal response to suicide, we argue that it offered participants fewer degrees of freedom to indicate that they would find suicide acceptable under our various contexts. Indeed, it was not until we highlighted the feelings of shame and guilt in each respective condition and focused in on the control vignettes than patterns associated with suicide understanding began to emerge.
Limitations
In this study, we asked participants to respond to a hypothetical scenario with the goal of allowing participants to take the perspective of another individual (Sam). A limitation to this approach is that it is still unclear whether guilt and shame actually precipitate suicide in different cultural realms. Though lacking in verisimilitude, the hypothetical nature of our scenarios may allow a clearer view at the nexus of culture, emotion, and suicide than would responses to actual accounts of suicides. That is, responding to an actual suicide may severely restrain participants’ degrees of freedom when asked to think about an event that severely breaches social norms against self-harm. Yet, those interested in extending the findings presented in this study may gain valuable information from those who have attempted suicide or from the grievances expressed within suicide notes to determine whether expressions of shame and guilt vary cross culturally.
Another component to our novel methodology that warrants further investigation is the characteristics of the target character. To our knowledge, these findings are the first to empirically demonstrate that cultural differences in the meaning of suicide are determined in part by culturally relevant emotions. As a first step in identifying how the link between shame, or guilt, and suicide varies across cultures, we felt that it was important to keep the gender of the target character consistent. Describing a male character also has greater relevance, as males are more likely to commit suicide than women (Phillips, Liu, & Zhang, 1999; cf. Rudmin, Ferrada-Noli, & Skolbekken, 2003). We also did not vary the ethnic-racial background of Sam (which many may have assumed to be White). Again, this decision reflects our primary interest in the effects of culture and emotion on understanding.
Additionally, some may be wary of our use of an MTurk sample. We argue, however, that recruiting an MTurk sample was an easy and inexpensive way to access people from across the United States, which was crucial for our present study. Moreover, research has shown that MTurk samples tend be more diverse, older, more attentive, and reliable in comparison to the frequently used student samples (Buhrmester, Kwang, & Gosling, 2011; Hauser & Schwarz, 2016).
Lastly, various scholars have argued that honor and dignity cultures primarily pertain to White Americans (e.g., Brown, 2016; Crowder & Kemmelmeier, 2017; Hayes & Lee, 2005). Thus, the inclusion of members of U.S. minority groups, such as African Americans and Asian Americans, could have dampened our results. However, re-analysis of both studies focusing on White participants only produced essentially the same results as presently reported. Still, in light of stark variation in patterns of suicide (e.g., Crowder & Kemmelmeier, 2017) and cultural attitudes toward suicide (Walker, Lester, & Joe, 2006), future investigations should tackle how race and ethnicity may qualify the link between guilt, shame, and suicide.
Implications and future directions
Our results add to a relatively new line of research exploring the relationship between cultural variations in suicide relates and the cultural importance of shame and guilt. Several researchers have alluded to the fact that shame may play a larger role for suicide in U.S. honor cultures. Much of the attention in the literature on the importance of shame in honor cultures has focused on how shame can lead to aggression, particularly by men, when they cannot defend their honor or uphold their social image (Bosson, Vandello, Burnaford, Weaver, & Wasti, 2009; Cohen, 2003; Rodriguez Mosquera, Fischer, Manstead, & Zaalberg, 2008). Additionally, it was argued that lower levels of anti-depressant prescriptions are indicative of a hesitance to seek help when psychologically distressed (Crowder & Kemmelmeier, 2014; Osterman & Brown, 2011). When unable to maintain one’s honor, individuals are likely to resist further damaging their reputation with the stigma of mental health (Brown et al., 2014).
Although we expected members of honor culture are to be more affected by shame-eliciting scenarios, what we found was they are more likely to perceive shame across multiple types of scenarios. This may suggest that members of honor cultures are not necessarily sensitive to the experience, or onset, of shame. Instead, they may be higher in what is called, “shame proneness” in that they likely have a propensity to experience state shame in response to a perceived social transgression (Tangney, Youman, & Stuewig, 2009). This likely has implications for suicide prevention strategies. When working within an honor culture community, suicide prevention strategies may benefit from focusing on what individuals attend to in social situations rather than their reactions to them.
Arguably, guilt, as a precursor to suicide, has received far less attention in the empirical literature (cf. Bryan et al., 2012; Coster & Lester, 2013). This may stem from the assumption that guilt often motivates reconciliatory behaviors rather than withdrawal. However, consistent with the idea that guilt also elicits suicidal thoughts and behavior (Bryan et al., 2012; Coster & Lester, 2013), we show that members of dignity culture are particularly sensitive to the experience of guilt. Our findings also imply that a culturally sensitive approach to suicide with regard to honor and dignity cultures means focusing on specific nature of the emotional experience. Since members of honor states seemed to be especially responsive to cues in the environment that might be socially threatening, we surmise that suicide-related interventions should be adapted to anticipate that members of honor cultures may make little distinction between shame- and guilt-arousing situations. On the other hand, our findings suggest that members of dignity states are likely to distinguish between the two emotional experiences. Additional research is needed to investigate implications of these proposed differences for suicide intervention across the United States.
Our approach assumes that the definitions of shame and guilt utilized in our present study generalize to non-U.S. samples. Based on Wong and Tsai (2007) and Sheikh (2014), it is likely that our results are reflective of a Western model of shame and guilt and may not replicate elsewhere. These authors proposed that because individualistic societies promote the idea that the individual is a unique and distinct entity, they are more likely to define emotional experiences in such a way that differentiates the self from others (Markus & Kitayama, 2010). That is, the differentiation between guilt and shame in terms of the orientation inward (toward the self) versus outward (to others), respectively, reflects a Western conception of these emotions. In collectivistic societies, which promote that the individual is an interconnected and mutually dependent entity, the perceived boundaries between the external and internal are less prominent. Therefore, the difference between shame and guilt in this regard is less pronounced (Wong & Tsai, 2007). Although we focus on honor culture, it is important to keep in mind that the broader cultural context may make honor culture within the United States qualitatively different from honor cultures in other parts of the world.
To conclude, despite legal and social sanctions against it, suicide continues to persist. In demonstrating that conceptions of suicide may be reflections of culturally focal emotions, the present study highlights the importance of adopting a culturally sensitive approach to suicide intervention. Understanding the cultural background of someone fighting suicidal thoughts may influence how the source of distress is likely to be appraised (i.e., as shame-evoking or guilt-evoking), which may be an important step in reducing the inclination for suicide. Knowing how individuals are likely to interpret an event may benefit those assisting clients in reexamining their cultural beliefs so that they may view their situation in a different way (Dryden & David, 2008; Ellis, 1994). Psychologists, therapists, and social workers in honor cultures may benefit from focusing on how a person who is thinking of suicide may have lost their status or reputation and can assist them in reducing their feelings of shame and rebuilding their sense of self-worth. Those in dignity cultures may seek to focus on what could be done to reduce the experience of guilt so the individual can forgive him or herself and foster their self-esteem.
Footnotes
Appendix 1
Acknowledgments
The authors would like to thank Marcella Shrout and Anthony Papa at the University of Nevada, Reno, for their valuable comments on earlier drafts of this manuscript.