
Abstract
This research aimed to investigate the effect that rational-emotive behavior therapy had on the symptoms of burnout among undergraduate electronics work students in Southeast Nigeria. This study utilized a pretest–posttest design involving a no-intervention group versus an intervention group. Participants were 124 undergraduate electronics work students who met the inclusion criteria of the study. The intervention consisted of 12 weeks of rational-emotive behavior therapy treatment and 2 weeks of follow-up meetings conducted at 6 months. Self-report questionnaire was used for data collection. Repeated measures analysis of variance and t test were used for data analysis. The results show that rational-emotive behavior therapy had a significant effect on the symptoms of burnout syndrome among the electronics work students in the treatment group compared to their counterparts in the no-intervention group. Finally, the positive gains were significantly maintained by the treatment group at the follow-up. The current study suggests that rational-emotive behavior therapy program can be effective for dealing with burnout syndrome among the population of undergraduates in Nigeria. Further clinical evaluation is needed.
Keywords
Introduction
The term burnout was pioneered by Freudenberger (1974). According to Perlman and Hartman (1982), burnout is a response to chronic emotional stress characterized by emotional and/or physical exhaustion, lowered job productivity, and overdepersonalization. Maslach (1993) defined burnout as “a psychological syndrome of emotional exhaustion, depersonalization and a feeling of reduced professional accomplishment that can occur among individuals working with other people in some capacity” (p. 20). Burnout is a response to chronic interpersonal stressors at place of work characterized by emotional exhaustion, depersonalization, and reduced personal accomplishment (Schaufeli, Leiter, & Maslach, 2009). Specifically, student burnout refers to a psychological syndrome which occurs in the form of an exhaustion state due to coursework demand, a cynical and detached attitude toward the college degree, and a feeling of low efficacy and academic achievement (Schaufeli, Martínez, Pinto, Salanova, & Bakker, 2002).
Burnout is due to adverse stress (Danhof-Pont, van Veen, & Zitman, 2011; Maslach & Jackson, 1981; Smith, Segal, Robinson, & Segal, 2016). Its manifestation is now being examined among the student population (Elliot et al., 2015; Friedman, 2014; Gerber et al., 2015a; Kuittinen & Meriläinen 2011; Schaufeli et al., 2002; Tomaschewski-Barlem et al., 2014). Burnout problems primarily result from strong irrational beliefs (Balevre, 2001; Bond & Dryden, 2002). According to rational-emotive behavior therapy (REBT) perspective by Albert Ellis, irrational beliefs result in maladaptive emotions and thoughts, such as burnout (Terjesen & Kurasaki, 2009). One study showed that burnout thoughts and burnout behaviors significantly correlated with irrational beliefs (Balevre, 2001). A recent study further supported the fact that maladaptive thinking patterns may be related to burnout thoughts and behaviors (Balevre, Cassellsand, & Buzaianu, 2012). According to Ellis, Gordon, Neenan, and Palmer (1997), the REBT model can be used to help the individual understand that their negative affective response (in this case, burnout syndrome) emanates from how they perceive and evaluate some of these negative life events rather than from the events themselves.
According to Awa, Plaumann, and Walter (2010), intervention programs against burnout symptoms can be beneficial. Thus, there may be possible explanations as to why and how REBT intervention might change cognitive-emotionally distorted concepts, which seem to underlie burnout. An REBT intervention can target clients’ maladaptive cognitions and disturbed emotions by improving their mental toughness, hardiness, and resilience through its cognitive, emotive, and behavioral techniques (College of Cognitive Behavioural Therapies, 2015; Dryden, 2007; Jarrett, 2008; Jarrett, 2013; Roghanchi et al., 2013; Terjesen & Kurasaki, 2009; Turner & Barker, 2012). Mental toughness is used to describe a person’s capability to be consistently successful in coping with stressful life situations (Clough, Earle, & Sewell, 2002). Jones, Hanton, and Connaughton (2002) described mental toughness as the capacity to cope with and/or handle adversity, stress, and pressure; the capacity to overcome and recover from an intense failure; and the capacity to endure and persevere. Gerber, Brand, and Feldmeth (2013) and Gerber, Kalak, et al. (2013) demonstrated that individuals who scored higher in mental toughness were more resilient against stress. Brand et al. (2014) found that greater mental toughness was related to more favorable quality of life. Furthermore, recent studies by Gerber et al., (2015a) and Gerber et al., (2015b) also showed that individuals who were mentally tougher in a stressful situation were at a low risk of burnout symptoms compared to those with lower scores for mental toughness. On the other hand, several authors (e.g., Balevre, 2001; Shumba, 2016) have also noted that irrational beliefs, a major concept in REBT model, build maladaptive cognitive pattern leading to burnout. Thus, a change in burnout-related irrational beliefs can lead to a corresponding reduction in the burnout symptoms. A study by Nucci (2002) showed that the REBT approach enabled clients to address issues pertaining to their personal and professional accomplishment. Furthermore, studies by REBT practitioners also support the idea that one’s pattern of thinking and feeling may be related to one’s pattern of symptomatology (e.g., Eseadi, Anyanwu, Ogbuabor, & Ikechukwu-Ilomuanya, 2015; Howlett, 1994; Popov & Popov, 2013). Based on the REBT model, Howlett (1994) found significant associations between general patterns of beliefs and patient’s symptomatology. Given that cognitive vulnerabilities can predispose clients to burnout thoughts and behaviors, it is possible that REBT approach can be applied to change cognitive-emotionally distorted concepts underlying burnout. Through REBT approach, clients can be taught how to modify their low frustration tolerance beliefs into high frustration tolerance beliefs and become resilient (College of Cognitive Behavioural Therapies, 2015) against burnout. However, clients’ compliance with the REBT treatment modality is very essential. Evidence suggests that compliance with therapeutic recommendations is associated with decreased levels of burnout in individuals with stress-related exhaustion (e.g., Lindegard, Jonsdottir, Borjesson, Lindwall, & Gerber, 2015).
The need to employ the REBT approach in the management of burnout among the student population cannot be overemphasized. Schaufeli et al. (2002) found that there is a link between burnout and students’ poor learning outcomes, negative views of the learning environment, and available support. Burnout can affect students in the early undergraduate years (Barboza & Beresin, 2007; Watson, Deary, Thompson, & Li, 2008) and final undergraduate years (Deary, Watson, & Hogston, 2003; Gibbons, 2010). In undergraduate students, there is a link between burnout and withdrawal from the course (Oliveira, Caregnato, & Câmara, 2012) and between burnout and hardiness (Silva et al., 2014). Burnout syndrome is a significant health problem (Gerber et al., 2015a) which affects vocational students (Elliot et al., 2015; Gerber et al., 2015). Furthermore, from our examination of the literature, there is a dearth of empirical studies that have examined how an REBT program can help to mitigate undergraduate students’ burnout syndrome. Therefore, the main objective of the current study was to investigate the effect of an REBT program on burnout syndrome among undergraduate electronics work students in tertiary institutions in Southeast Nigeria. It was hypothesized that an REBT program would lead to a reduction in the symptoms of burnout syndrome among undergraduate electronics work students over time.
Method
Ethical approval
The approval for conducting this study was granted by the Research Committee, Faculty of Vocational and Technical Education at the University of Nigeria, Nsukka (no. VTE/ERA/0046). Written permission to conduct the study was granted by the heads of department, and the participants’ written informed consent was obtained. The authors adhered to research ethics of the American Psychological Association (2010).
Participants
The participants were 124 undergraduate electronics work students in public tertiary institutions in Southeast Nigeria (see Figure 1). The sample size was determined using GPower 3.1 software (Faul, Erdfelder, Lang, & Buchner, 2007) based on effect size f = 0.25, alpha (α = .05), power (1–β = .93), and statistical test (F tests–analysis of variance (ANOVA): repeated measures, between factors). Participants were selected after summing up of their burnout scores that enabled researchers identify those with high level of the burnout symptoms. There are two approaches for obtaining burnout scores of respondents—sum and average methods (Maslach, Jackson, & Leiter, 2016). We used the sum method in which high Maslach Burnout Inventory-Student Survey (MBI-SS) scores indicate the manifestation of a high level of the symptoms of burnout syndrome, which was an inclusion criterion for participation in the study. According to Maslach et al. (2016), one approach used in burnout assessment has been to use arbitrary, statistical “cutoff” scores to identify individuals with “high levels of burnout” which is valuable for assessing the overall burnout pattern of a group. Hu and Schaufeli (2009) used the sum method to determine the existence of symptoms of burnout in their study sample. However, Beheshtipour, Nasirpour, Yektatalab, Karimi, and Zare (2016) used the average method to indicate the presence of burnout in the study participants at baseline.
Participant eligibility criteria. REBT: rational-emotive behavior therapy.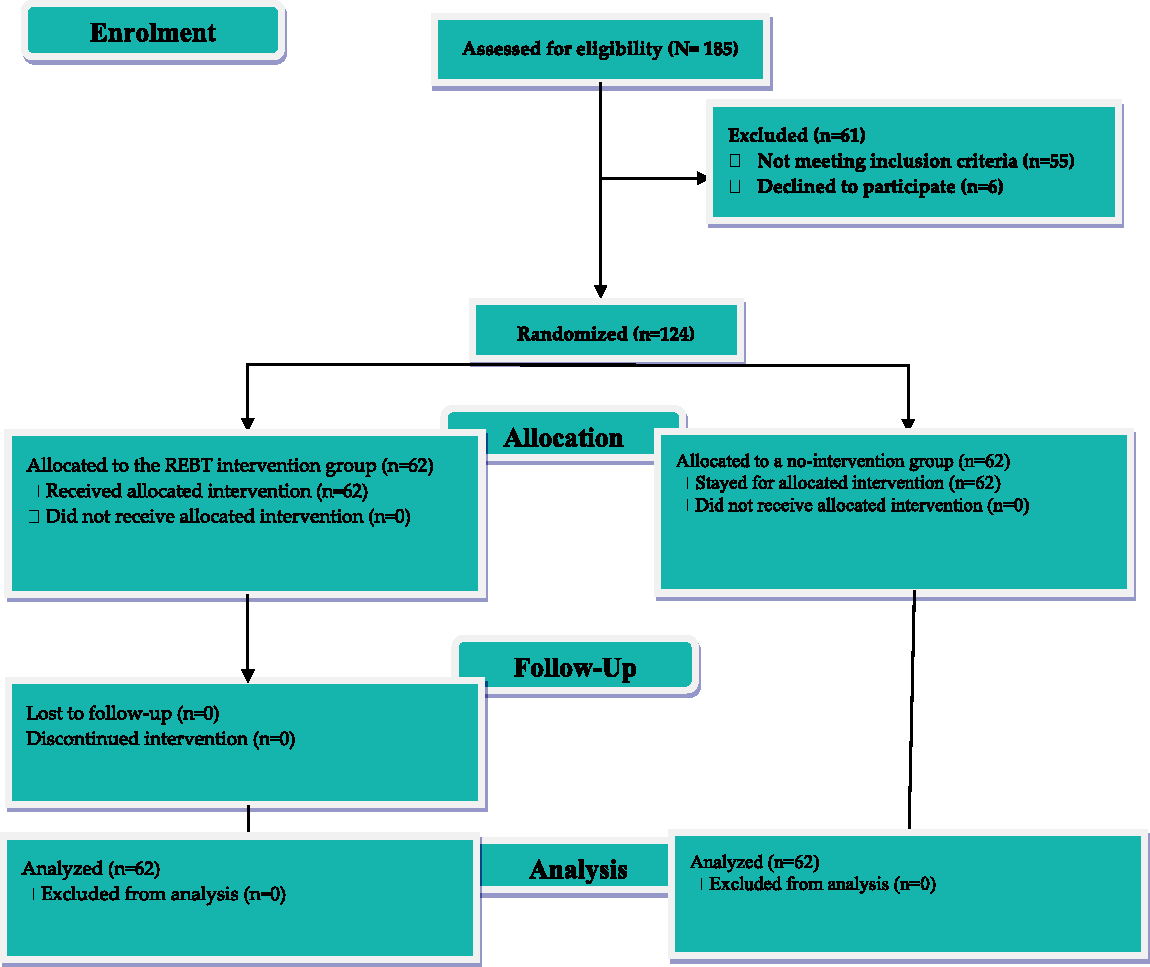
Demographic characteristics of the participants.

REBT = rational-emotive behavior therapy; χ2 = chi-square.
Mean age (SD) of participants in years.
t = test results for age.
Table 1 shows that the mean age of the REBT group was 22.65 ± 1.52 years, while that of the no-intervention group was 22.52 ± 1.51 years, with no significant difference, t = .424, p = .673. Of the 124 participants who took part in the study, those in the REBT group comprised 40 (33.9%) male participants and 22 (16.1%) female participants, while the no-intervention group comprised 42 (32.3%) male participants and 20 (17.7%) female participants, with no significant difference, χ2 = .072, p = .788. Of those in the REBT group, 20 (16.1%) were from rural areas and 42 (33.9%) were from urban areas, while in the no-intervention group, 24 (19.4%) were from rural areas and 38 (30.6%) were from urban areas, with no significant difference, χ2 = .282, p = .791.
Design
The study utilized a pretest–posttest design involving a no-intervention group versus an intervention group.
Measures
Maslach Burnout Inventory-Student Survey
Descriptive statistics for the MBI-SS based on the current sample (N = 124).

Procedure
The researchers collected data between September 2015 and August 2016 from two participant groups (experimental and no-intervention groups), and three measurements (pretest, posttest, and follow-up test) were administered. Information about the study was displayed in strategic locations and on bulletin boards in tertiary institutions offering electronics work courses in the zone. At baseline (Time 1), a total of 185 participants responded to the notices, and their symptoms of burnout syndrome were measured. The first 124 undergraduate electronics work students who fulfilled the study criteria were selected for participation in the study. Participants were randomly assigned to one of the two groups: 62 participants were assigned to the experimental group and 62 participants were assigned to the no-intervention group by means of simple randomization. The randomization was achieved using a computer-generated random list that was produced by Saghaei’s random allocation software, version 1.0 (Saghaei, 2004). An REBT program consisting of twenty 90-minute sessions was implemented for participants in the experimental group for 12 weeks. Two of the researchers who have adequate background in the principles and practice of REBT delivered the intervention. Participants in the experimental and no-intervention groups also completed the MBI-SS posttest (Time 2). Follow-up assessment (Time 3) was performed six months later for participants in the treatment group. Thus, participants in the no-intervention group completed questionnaires only at pretest and posttest assessments.
Intervention
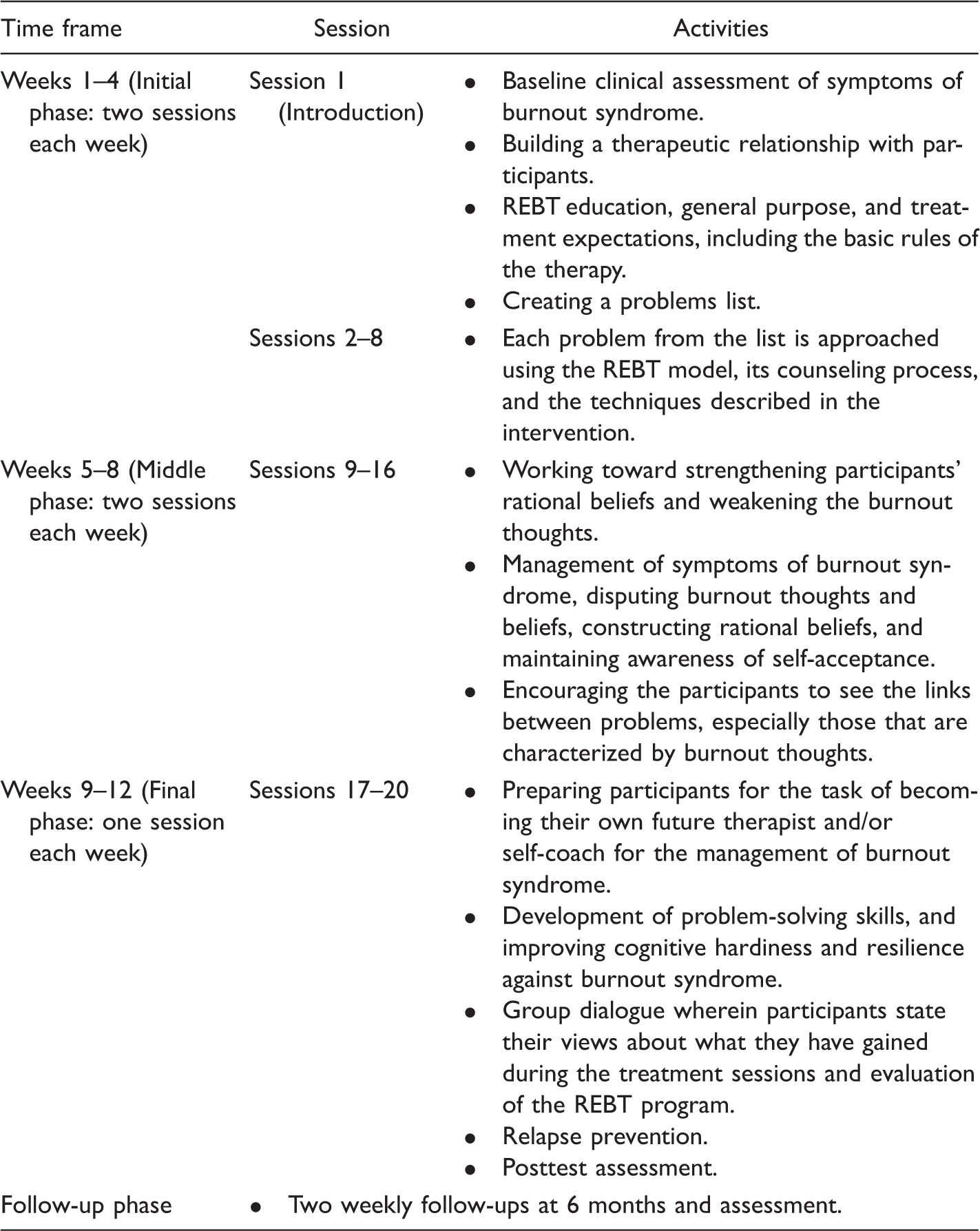
REBT program manual
Summary of the rational-emotive behavior therapy program manual.
REBT: rational-emotive behavior therapy.
Data analysis
We conducted ANOVAs for repeated measures with the factors—Time (within-subjects variables), Group (between-subjects factors), and Time × Group interaction; post hoc tests were done with Bonferroni–Holm corrections for p values. We reported partial η2 as a measure of the effect size for this design. The one-sample t test was used to analyze the follow-up test of the treatment group. The paired-samples t test was also performed to determine whether the assessment scores differed over time and across treatment and no-intervention group participants. The t test for independent samples was conducted also, while chi-square was used for checking participants’ demographic characteristics equivalence. All statistical analyses, including screening for missing values and violation of assumptions were conducted using SPSS(R) 20.0 (IBM Corporation, Armonk, NY) for Windows(R)/Apple Mac(R) (IBM Corp., 2011).
Results
Results on the effects of REBT on symptoms of burnout as measured by MBI-SS.

CI: confidence interval; M: mean; MSI-SS: Maslach Burnout Inventory-Student Survey; N: number of participants; REBT: rational-emotive behavior therapy; SD: standard deviation; ηp2: effect size.
Significance value from t test.
Significance value from ANOVA test.
Results revealed significant Time × Group interaction effect for burnout syndrome, F(1,123) = 394.27, p < .001, ηp2 = .868. Based on the one-sample t test analysis, the follow-up assessment (Time 3) performed after 6 months revealed a significant reduction in the burnout syndrome for the treatment group, t(61) = 68.31, p < .001. The paired-samples t test of the Time 1 and Time 2 scores for the MBI-SS was significant for the treatment group, t(61) = 14.29, p < .001. The paired-samples t test showed that the Time 2 and Time 3 scores for the MBI-SS, t(61) = 8.36, p < .001, was also significant for the participants exposed to the REBT treatment, which is an indication of the program’s sustainability effect on burnout reduction over the time period. Furthermore, paired-samples t test showed that the differences with regard to burnout in experimental group at Time 1 and Time 2 were statistically significant, t(61) = 12.99, p < .001, 95% CI = 18.29, 25.12. On the other hand, the paired-samples t test showed that burnout scores did not significantly change over time in the no-intervention group at Time 1 and Time 2, t(61) = −571, p = .572, 95% CI = −.15, .08. In addition, the t test for independent samples showed that there were significant differences in burnout between experimental and no-intervention group at Time 2, t(122) = −19.86, p < .001, 95% CI = −29.65, −24.22 (see Table 4). The results provide support for the hypothesized effect of REBT on the burnout syndrome. Figure 2 is a graphical presentation of the Time × Group interaction effect.
Graphical presentation of Time × Group interaction effect. MBI-SS: Maslach Burnout Inventory-Student Survey; REBT: rational-emotive behavior therapy.
Post hoc tests with Bonferroni–Holm corrections for p values.

CI: confidence interval.
Based on estimated marginal means.
Adjustment for multiple comparisons: Bonferroni–Holm.
The mean difference is significant at the .05 level.
Discussion
The main purpose of the present investigation was to examine the effects that REBT had on burnout symptoms among undergraduate electronics work students in tertiary institutions in Southeast Nigeria. Our finding revealed that REBT had a significant effect on the symptoms of burnout syndrome among the undergraduate electronics work students in the treatment group compared to their counterparts in the no-intervention group. Moreover, the results showed that the gains were sustained significantly for the treatment group at follow-up after a 6-month period. These findings lend credence to those of Walter, Krugmann, and Plaumann (2012) who found that burnout intervention programs tend to be effective, and that their effects can be enhanced. The results also support the evidence that indicated that a cognitive-behavioral intervention program decreased student burnout (Breso, Schaufeli, & Salanova, 2010). The current study suggests that an REBT program can be effective for dealing with the symptoms of burnout syndrome among undergraduate students in Nigeria.
Our study suggests that individual students suffering from burnout could benefit from REBT-based therapeutic treatment. In addition, the situations that lead students to manifest symptoms of burnout syndrome, such as emotional exhaustion, need to be recognized in future research considering the specificity of their study environments (Tomaschewski-Barlem et al., 2014). Furthermore, REBT practitioners need to focus on employing evidence-based strategies for identifying and challenging students’ burnout beliefs and constructing more adaptive beliefs, emotions, and behavior. According to Dryden (2007), REBT offers a clarification of how individuals disturb themselves about life’s adversities, how they inadvertently maintain that disturbance and how practitioners could help them tackle that disturbance effectively so that they could lead healthier lives.
By implication, REBT practitioners with knowledge of psychological medicine must realize that a client’s response to a burnout event with a set of irrational beliefs may play a crucial role in predicting the development of symptoms of burnout syndrome and thus provide an insight into what kind of REBT treatment process will be suitable for such clients considering the different facets of the irrational beliefs of people suffering from burnout. REBT proposes that discomfort disturbance is due to a person’s illogical beliefs about his/her ability to cope, tolerate, and withstand depressing or stressful events (College of Cognitive Behavioural Therapies, 2015). Given our findings, the REBT program can be considered a promising intervention which can be implemented as an alternative therapy to pharmacotherapy to also reduce doctor burnout. In fact, it appears that up to 60% of doctors are suffering from burnout syndrome (Black, 2017) which may be due to different facets of maladaptive beliefs and interpretations of their own ordeal, job and personal expectations, and other’s expectations.
Limitations of the current study
Despite the positive outcomes, this study is not without some limitations. The authors acknowledge that the study’s sample size was small and that it included only undergraduate students from tertiary institutions in Southeast Nigeria that offer electronics work courses. As a result, the current study can be considered preliminary. Future studies should include large samples and undergraduate students from various disciplines to determine whether the findings are generalizable to undergraduate students in various fields of study. Furthermore, the effectiveness of the REBT program was assessed using only quantitative data. In future, research should make use of qualitative data involving an interview schedule and the students’ opinions. Even though a follow-up assessment was performed in this study, consideration of the much more long-term effect of the REBT program on the symptoms of burnout syndrome might be necessary. The authors feel that it would be helpful in future research endeavors to focus on carrying out multiple long-term follow-up assessments in order to evaluate the sustainability of the reduction in students’ burnout syndrome due to exposure to an REBT program. Future research should also consider the moderation effect of certain sociodemographic factors, such as the participants’ income level, marital status, and religion.
Another limitation of the study is that whereas participants of the REBT program had a highly structured and professional social interaction (group therapy), this was apparently not the case for the no-intervention group. As a group, they needed to have met for chats, for instance, at the same rate/times as the REBT group which would have at least partialled out the fact that meeting as a group for a few informal chats about anything was not as effective as a directed intervention. Future studies should provide participants in control condition with opportunities for meeting as a group and having informal discussions even if they would be waitlisted.
Further limitation of the present study is that participants in the no-intervention group completed questionnaires only at pretest and posttest assessments. The lack of follow-up evaluation for control group participants limits the present study. Therefore, future investigators should as a matter of concern, endeavor to acquire follow-up evaluation data from participants in a no-intervention group. However, it should be noted that this method of assessment for the control group participants has been successfully applied to ascertain the effectiveness of REBT-based intervention in recent times (e.g., Ogbuanya et al., 2017; Ugwoke et al., 2017).
Conclusion
The authors investigated the impact of a 12-week-lasting REBT intervention program on the symptoms of burnout among a sample of adult students offering electronic work courses. The present study contributed to the extant literature by noting the effectiveness of an REBT program on the reduction in students’ symptoms of burnout syndrome. Based on the findings of the current study, the authors conclude that the REBT program offered to the undergraduate students in Nigeria significantly decreased their symptoms of burnout syndrome, relative to a no-intervention group. Further evaluation and therapeutic effort by REBT practitioners for the prevention and management of burnout syndrome among students is warranted in other countries.
Footnotes
Authors’ Contributions
TCO, CTO, and CE conceived the idea and editing of the manuscript. CTO, CE, NCE, SCU, JIA, and JCO did the data collection, statistical analysis, and writing of the manuscript. TCO, CTO, CE, NCE, SCU, JIA, and JCO did the final review and approval of the manuscript for submission.
Acknowledgments
The authors are thankful to all the study participants for granting the informed consent and for their commitment to the treatment intervention. The authors would like to thank the Associate Editor and two Anonymous Reviewers for their useful comments which helped to improve the quality of this research.