
Abstract
In a novel pilot study, we investigated how emotional state is related to inflammatory responses to acute pain among women with rheumatoid arthritis. Nine women completed four 5-hour visits that varied only by manipulation of emotion (anger, sadness, happiness, vs. control); in each visit, acute pain was elicited, with blood draws at baseline, 10 minutes, 60 minutes, and 100 minutes post-pain. We examined the effects of within-subjects factors on circulating inflammatory biomarkers interleukin (IL)-6, IL-10, tumor necrosis factor-α, C-reactive protein, and cortisol. There was a main effect of state anger on IL-6, with higher reported anger associated with higher IL-6 across conditions. Further, there were several interactions between state emotion and condition. For example, when individuals reported higher state anger in the sadness condition compared to their own average, they showed higher levels of IL-6 and cortisol. Findings are discussed within a larger literature suggesting that mixed emotional states can contribute to psychological stress and inflammatory responses.
Introduction
Novel psychosocial targets for symptomatology associated with rheumatoid arthritis (RA) are critically needed (Kasle, Wilhelm, McKnight, Sheikh, & Zautra, 2010; Keefe & Somers, 2010; Leverone & Epstein, 2010). Current pharmacological therapies can confer serious side effects and may not fully control the discomfort and inflammation common in RA (Khurana & Berney, 2005). There is growing evidence that mood and psychological stress play a role in pain severity and RA symptomatology specifically (e.g., Evers et al., 2014; Graham-Engeland, Zawadzki, Slavish, & Smyth, 2016; Kasle et al., 2010; Keefe & Somers, 2010). As such, optimal treatment may require consideration of such factors and how they contribute to inflammation and symptomatology in RA. Very little is known about the effects of state emotion on inflammatory responses to pain or stress in any population. This knowledge might be particularly beneficial for RA patients, for whom short-term changes in inflammation are clinically meaningful. This manuscript summarizes relevant findings from the extant literature and presents new findings from a pilot study that was designed to examine the degree to which manipulated emotional state may affect short-term inflammatory responses to pain among women with RA. In doing so, we present a novel research paradigm to illuminate such phenomena and, further, highlight the need for more nuanced research on the ways in which complex emotional patterns may either buffer effects of stress or function as stressors themselves to modulate inflammatory responses.
The most common autoimmune disease worldwide, RA is diagnosed in approximately 1.3 million adults in the United States and affects two to four times more women than men (Khurana & Berney, 2005). The disease is characterized by persistent and symmetric joint inflammation and is often accompanied by joint stiffness and pain, as well as disability and general malaise (Khurana & Berney, 2005). Inflammation is thus a key therapeutic target for RA. It is well established that psychosocial and pain-related stressors can exacerbate inflammation among individuals with RA to an even greater extent than they do among healthy controls (for reviews, see Evers et al., 2014; Straub & Kalden, 2009). The greater stress-induced aggravation of inflammation in those with RA seems to be due at least in part to their having poorer control over inflammation by norepinephrine and cortisol, biomarkers of sympathetic nervous system and hypothalamic-pituitary-adrenal activation, respectively, that play an important inhibitory role in inflammation (Davis et al., 2008; Geenen, Van Middendorp, & Bijlsma, 2006; for review, see Straub, Dhabhar, Bijlsma, & Cutolo, 2005). Moreover, research consistently indicates that emotional state and stress in daily life can influence RA symptoms (Connelly et al., 2007; Evers et al., 2014; Graham-Engeland et al., 2016; Zautra, Johnson, & Davis, 2005). For example, the regulation of both positive and negative emotion from one day to another across a 30-day period predicted lower daily pain among individuals with RA (Connelly et al., 2007). In a separate study, both momentary negative and positive emotion were associated with momentary arthritis-related restrictions (Graham-Engeland et al., 2016).
There is relatively little published research linking levels of inflammation with specific emotional states, whereas there is considerable research linking inflammation to broad trait tendencies that include negative emotion, such as depressed mood and hostility (Graham et al., 2006; Kiecolt-Glaser, Derry, & Fagundes, 2015) or psychological stress more broadly (Glaser & Kiecolt-Glaser, 2005; Marsland, Walsh, Lockwood, & John-Henderson, 2017). However, although results have been mixed and include some null findings, a small but growing literature suggests that specific emotional tendencies can relate to levels of inflammation observed in peripheral (circulating) blood samples. For example, one study with middle aged adults that used retrospective global assessments of affect (recalled over the past week and obtained on the same day as a blood draw) found that higher negative affect was associated with higher levels of interleukin(IL)-6 and higher positive affect was associated with lower levels of IL-6 (Sturgeon et al., 2016). Chronic elevation of IL-6, a cytokine with many inflammatory functions, confers risk of frailty and disease (e.g., Black, 2003; Pradhan, Manson, Rifai, Buring, & Ridker, 2001; Stoner et al., 2013). This same study by Sturgeon and colleagues did not show a significant association between negative affect and C-reactive protein (CRP), which is a broad marker of inflammation and an independent risk factor for disease (Ridker, 2007; Stoner et al., 2013). Further, several experimental studies suggest that emotional states are associated with inflammation in certain contexts. For example, both anxious and anger responses to a speech-based laboratory stressor were associated with greater IL-6 responses 30 minutes post-stressor among a relatively healthy community sample (Carroll et al., 2011), and manipulated increases in positive emotion (via a humorous film) were related to decreased production of tumor necrosis factor (TNF)-α, another inflammatory cytokine, in a healthy sample of young adults (Mittwoch-Jaffe, Shalit, Srendi, & Yehuda, 1995). Finally, recent research using intensive ecological assessment methodologies also highlights the importance of investigating the role of recent positive and negative emotion on inflammation. For example, momentary positive emotion was linked with lower levels of CRP and IL-6 among midlife women (Steptoe, O'Donnell, Badrick, Kumari, & Marmot, 2008). Further, in a diverse sample of mid-life adults, momentary negative affect was associated with higher levels of a composite of inflammatory cytokines that included IL-6 and TNF-α (Graham-Engeland et al., 2018).
Given that both emotion and state pain may influence inflammatory markers, likely via somewhat distinct mechanisms, it is possible that emotion and pain may have synergistic effects on inflammatory processes. A recent finding in healthy women supports the premise that negative affect may influence the association between pain and inflammation: Among healthy women who had vaccination-induced elevations in circulating IL-6, those who had greater levels of negative affect than others showed less tolerance to pain (Lacourt et al., 2015). However, no study to our knowledge has examined how acute manipulated emotional state affects inflammatory cytokine responses to pain in any population.
The present study was designed to examine effects of manipulated emotion—anger, sadness, and happiness—on biomarker responses to acute pain among nine women with RA using a repeated measures design. We expected that, relative to the control condition, the anger and sadness conditions would result in (1) greater increases in the levels of three inflammatory biomarkers (IL-6, TNF-α, and CRP) and cortisol, a key stress hormone, and (2) (on a more exploratory basis) greater decreases in IL-10, a cytokine with anti-inflammatory properties. The production of IL-10 has been observed to increase in response to manipulated stress and pain (e.g., Mika, Zychowska, Popiolek-Barczyk, Rojewska, & Przewlocka, 2013) and to decrease with prolonged pain among those who respond to a stressor with elevated anxiety (Maes et al., 1998; Mika et al., 2013). We tested both anger and sadness because they represent negative emotions that vary in the levels of activation with which they are commonly associated (Posner, Russell, & Peterson, 2005; Russell, 1980), thus enabling a test of our expectation that negative emotion, as opposed to activating emotion, would be associated with greater inflammatory responses. Although we manipulated what is likely a relatively high activation form of happiness, women in the happiness condition were expected to evidence lower elevation of cortisol and inflammation relative to themselves in the control condition. On a more exploratory basis, we also tested whether reported pain and state emotion were associated with outcomes regardless of condition, again with the expectations that anger and sadness would be associated with greater inflammatory responses.
Method
Participants
Participants were community residents recruited from a local rheumatology clinic as well as local newspaper advertisements and flyers. Participants were required to be between 18 and 80 years of age and to be able to participate in four visits at a General Clinical Research Center (now Clinical Translational Research Center) on a university campus in central Pennsylvania. Because the sample size for this pilot study was expected to be too small to enable moderation analyses by gender, only women were recruited. All participants had a confirmed diagnosis of adult-onset RA based on criteria established by the American Rheumatism Association (Arnett et al., 1988). Prospective participants were screened for comorbid conditions, medication use, and medical history using an online questionnaire. Exclusion criteria included any anti-TNF-α medication use, daily use of more than 7.5 mg of the anti-inflammatory drug prednisone, a body mass index (BMI) of >40, reported consumption of >21 alcoholic drinks per week and/or >10 cups of coffee per day, and comorbid diseases with immunological or endocrinological components (e.g., cancer and Crohn’s disease). Women who were pregnant, nursing, or who had been pregnant or nursing in the past three months were also excluded. Further, no study visit was started within three months of a hospitalization or surgery.
The final sample, which is described in further detail in the Results section, consisted of nine women with a mean age of 54.11 years (SD = 15.59). Before each scheduled visit, participants were asked to refrain from eating or drinking anything other than water after midnight the night before. They were also asked not to take ibuprofen, acetaminophen, or aspirin from 10 pm the day before each visit or to take any medications for breakthrough pain. Participants taking methotrexate had not taken it for at least 48 hours before each visit. Participants with obvious signs of illness on the day of their scheduled visit, including fever >100.4°F, were rescheduled.
Detailed procedures
All study procedures were conducted in compliance with institutional review board and Health Insurance Portability and Accountability Act (HIPAA) guidelines. Following the screening application and prior to their first visit, participants were asked to complete an online questionnaire to assess recent RA severity, demographics, and baseline psychosocial characteristics. Participants were then scheduled for their first of four, approximately 5-hour, in-person visits, which varied only by experimental manipulation as described below. The visits were required to be at least two weeks apart. A study coordinator greeted the participant at 8:00 am and a nurse collected vital signs including blood pressure. The nurse then settled the participant into a semi-reclined position on a hospital bed in a private room. Next, the nurse applied LMX numbing cream to an intravenous (IV) catheter insertion site on the participant’s arm to minimize discomfort with IV insertion, using a heating pad to facilitate blood flow at the IV insertion site. As part of a 30 minutes recovery period, participants were provided with a standardized breakfast in bed, after which they completed questionnaires.
A trained research assistant who had no interaction with study participants randomly assigned each participant to one of the four conditions (anger, sadness, happiness, or control) prior to the study visit. The experimental manipulation took place at approximately 9:50 am. The emotion manipulation protocol was based on a recall interview procedure shown previously to elicit specific emotional states in expected directions (see Burns, Kubilusa, & Bruehl, 2003); it was run by trained facilitator who was someone other than the coordinator running the rest of the protocol for that day. On an emotion condition visit, the participant was first asked to focus on recent emotional experiences related to the specific emotion condition. For example, in the sadness condition, the participant was asked to “think about a time or times in the past month or so” when you felt “depressed, sad, or down” and to “focus on the time when you were saddest.” Examples of emotion-provoking events consistent with the target emotion were provided, after which the participant was given a few minutes of quiet time to identify a relevant experience. Next, the participant was given 10 minutes in the room by herself to write in detail about that experience and was asked to focus on her feelings of the given emotion being elicited (e.g., sadness). Finally, the facilitator discussed with the participant what she had written, providing further prompts to elicit the given emotion (e.g., what exactly about ____ made you sad that day?) or reinforcing statements (e.g., “so at that time you were really sad!”). The control task was set up similarly: The facilitator asked each participant to (1) focus on her plans for the afternoon and next day and (2) to write about them non-emotionally for 10 minutes. Then, the participant discussed her plans with the facilitator, who took care to be neutral and to not elicit emotional responses. At the end, the facilitator said “thank you for sharing your plans with us” and briefly described mock research about time management that might be useful for individuals with chronic pain.
Starting at approximately 10:20 am, the coordinator applied pressure to the first of the participant’s three most tender joints until the participant reported pain, using a palpometer (Palpometer Systems, Inc.) in increasing increments on a modified Chatillon scale (100, 250, 425, 700, or 1000 gf/cm2). The level of pressure at which pain was reported was maintained for 30 seconds; this stimulus was then applied in turn to each of the participants’ other two most tender joints. Serum and plasma were obtained at a baseline time point at ∼9:40 am (T1) and three post-pain time points: 10 minutes post-pain (∼10:35 am; T2), 60 minutes post-pain (∼11:25 am; T3), and 100 minutes post-pain (∼12:05 am; T4). A standardized lunch was provided in bed at ∼11:45 am.
Double-blind controls
All study staff, including the coordinator and nurses, were blind to the experimental condition with the exception of the facilitator who performed the emotion manipulation. Staff were asked to not to be overly enthusiastic or emotional and participants were not permitted to use any entertaining materials during the study visits. The coordinator told participants only that this was a study “to investigate the associations between emotion, stress, pain, and inflammation among individuals with rheumatoid arthritis” and that the difference between their four visits would be the content of the “writing/thinking task.” At the end of their fourth visit, the coordinator debriefed each participant.
Measures
Blood-based measures
A nurse collected three tubes of blood via an in-dwelling catheter. Two vacutainer BD SST tubes (for serum) were obtained, inverted five times, and left to clot for 15 minutes at room temperature. One BD EDTA tube (for plasma) was kept on ice prior to collection and then put back on ice for processing. Samples were centrifuged for 15 minutes at 1500 g (4C). Extracted serum and plasma were stored at −80°C until assayed. Samples were assayed via enzyme immunoassay for serum IL-6 and IL-10 levels (Assay Designs, Ann Arbor, MI), TNF-α (Assay Designs, Ann Arbor, MI), and serum cortisol (DSL Labs, Webster, TX) in the Penn State Biomarker Core Laboratory. All assays were run in duplicate and all assays for a given participant were run on the same plate. The sensitivity of the assays (lowest detectable concentration) was 0.1 mg/L for CRP, 8.43 pg/mL for TNF-α, 6.0 pg/mL for IL-6, 3.75 pg/mL for IL-10, and 0.1 μg/dL for cortisol. The coefficients of variability for each was less than 8%.
State pain
Current acute pain was measured by a Visual Analog Scale (Wewers & Lowe, 1990) on a scale from 0 to 10 with 0.5 increments, an often-used and well-accepted manner of assessing fluctuations in pain over time (Dworkin et al., 2005). The Visual Analog Scale was administered six times: at baseline (roughly 9:15 am), immediately after the emotion manipulation (∼10:15 am), during and immediately after the pain stimulus (∼10:23 am), just before the first post-pain blood draw (∼10:30 am), and near the end of the visit (∼12:30 pm).
State emotion
Self-reported state anger, sadness, happiness, and anxiety were assessed with items from the Profile of Mood States (Usala & Hertzog, 1989) and from the Positive Affect Negative Affect scale (Watson, Clark, & Tellegen, 1988). Anger was assessed with the items angry, grouchy, furious, bad-tempered, and mad. Sadness was assessed with the items blue, depressed, gloomy, glum, and sad. Happiness was assessed with the items content, pleased, enthusiastic, cheerful, and happy. Anxiety was assessed with the items nervous, worry, uneasy, tense, and on-edge. Participants rated the degree to which they felt each emotion “right now” on a scale from 1 to 5 for all items. These scales were administered at baseline (∼9:15 am), just before the first post-pain blood draw (∼10:30 am), and near the end of the visit (∼12:30 pm). At the first time point and in the control condition, Cronbach’s α for anger, sadness, happiness, and anxiety was .89, .91, .94, and .79, respectively; similar inter-item reliability was observed at the second two time points and across conditions, with no scale exhibiting lower than Cronbach’s α of .76 at any time point.
Baseline markers of arthritis severity
We utilized a Disease Activity Score (DAS), one of the most widely used and validated measures of disease severity in RA (Anderson et al., 2012). Near the start of the study, a nurse practitioner trained by a rheumatologist on our team performed a 28-joint count to determine the number of tender and swollen joints. Via the appropriate formula (Flendrie, Pittiman, & Fransen, 2015), a DAS-28-CRP score was computed from the number of tender joints and the number of swollen joints, along with serum CRP level from the control visit, and baseline self-reported pain from prior to the first study visit on a 0–100 scale. DAS-28-CRP scores range from 0–10, with a score of 2.6 or less indicating remission, scores of 3.2 to 5 indicating low to moderate disease severity, and scores of 5.1 or greater indicating high disease activity (Anderson et al., 2012; Kiely, 2007).
Participants also completed the daily living subscale of the Modified Health Assessment Questionnaire (mHAQ), which provides a non-disease specific indication of functional capacity (Pincus, Yazici, & Bergman, 2005). Via eight items, participants use a 4-point scale from 0 (“without any difficulty”) to 3 (“unable to do”) to indicate how difficult it is for them to do certain behaviors such as “get in and out of bed” and “bend down to pick up clothing from the floor.” The item scores are summed and then divided by 8, with greater scores indicating greater overall disability; mHAQ scores less than 0.3 are considered normal (Pincus et al., 2005). Cronbach’s α for the mHAQ in the present research was .92.
Recent pain and depressed mood
Recent pain severity was assessed using items of the pain severity subscale of the West Haven-Yale Multidimensional Pain Inventory (MPI; Kerns, Turk, & Rudy, 1985), a widely used inventory with extensive validation among individuals with chronic pain (Kerns et al., 1985; Riley, Zawacki, Robinson, & Geisser, 1999). Participants responded from 0 to 6 on three items asking about pain severity at the present moment as well as both pain severity and suffering over the past week, with 6 indicating more extreme severity and suffering. Cronbach’s α for the MPI in the present research was .76. The Center for Epidemiological Studies Depression Scale (Radloff, 1977) was used to measure depressed mood. The CES-D is commonly used to identify depressive symptomatology among chronic pain patients (Geisser, Roth, & Robinson, 1997; Tait, 1999). Responses to 20 items are measured on a scale that ranges from 0 to 3, with 3 representing the greatest frequency of depressed mood over the past week. Cronbach’s α for the CES-D in the present research was .74.
Statistical analyses
Preliminary analyses assessed continuous variables for normality. Biomarker variables exhibited skew and a square root transformation was applied. Although transformed values were used in the analyses, means based on raw scores are reported in the text and used in figures to aid in interpretability. There were 108 possible observations across the 36 total visits for analyses comparing across the four conditions and three post-baseline blood draws. We used a mixed effects model estimated with restricted maximum likelihood, which offers greater flexibility in handling data issues when compared to the traditional repeated measures analysis of variance estimated with least squares (Bagiella, Sloan, & Heitjan, 2000). We used a multilevel data structure with level 1 variables relating to the time of the blood draws (biomarker levels at baseline and three other time points of the blood draws during each visit), level 2 variables at the visit-level (emotional condition, reported state emotion after emotion manipulation, and reported pain immediately after the pain stimulus), and level 3 variables being person-level covariates (age, BMI, DAS total score as a measure of disease severity, and baseline biomarker levels). Four separate linear mixed-effects models were fit to each of the four biomarker responses (IL-6, TNF-α, IL-10, and CRP) to the pain stimulus to test effects associated with the two within-subject factors; specifically, the main effect for emotion condition, the main effect for time, and the interaction between emotion condition and time. Time effects were not examined for CRP because it was only measured at the first and last time points. Additionally, average state levels of anger, sadness, and happiness reported across all post-manipulation time points and average pain ratings during and immediately after the pain stimulus were entered as level 2 variables to examine the main effects of state emotion and pain and the interaction between state emotion and condition.
The mixed effects models described above were fit using PROC MIXED from SAS version 9.3 (SAS Institute, Cary, North Carolina), applying the Kenward-Roger method of degree of freedom correction (Kenward & Roger, 1997) and using the Bayesian Information Criteria to select the compound symmetry as the appropriate variance-covariance structure. When the effects of either time or condition were significant at p < .05, we examined them further by using the Tukey’s post-hoc test. For reported state emotion or pain ratings, the pattern of interaction was examined by comparing the estimated mean and the standard error of biomarker levels for emotional conditions while fixing the reported emotion (or pain) at the mean and 1 standard deviation above and below the mean in the regression equation. The effect size estimation of pseudo R2 value (Holden, Kelley, & Agarwal, 2008) for the mixed model results was reported to show the proportional reduction in residual variance between the baseline model without any predictor and the tested model with significant predictors. The residual variance of level 1 variables (e.g., IL-6) was used to calculate the pseudo R2.
Results
Preliminary analyses
Sample characteristics
At baseline, the average age of the nine participants was 54.11 (SD = 15.59, range 31–75) and the average BMI was 26.08 (SD = 5.19). All participants were White and relatively well-educated (all had at least a high school diploma, with five having an either 2- or 4-year college degree), but they reported greatly varied household income (from <10K to >100,000). Eight were married and one was divorced. Participants had been diagnosed with RA for an average of 11.89 years (SD = 13.44): They had been living with RA from 2 to 41 years, and they had experienced symptoms for an average of 13.11 years (SD = 13.30). The average DAS-28 score was 4.52 (SD = 0.68), with no participant having a score less than 3.2 and two participants with scores over 5.1; this distribution of scores suggested that RA severity among participants was moderate, that no participant was in remission, and that two participants experienced what would be considered severe RA. At baseline, the average mHAQ score across the four visits was 1.49, with a range of 1.43–1.57, and the average pain severity score on the MPI was 6.11 (SD = 1.97). The average depressed mood score was 8.33 (SD = 5.07), suggesting that the typical participant was not depressed.
Manipulation checks on emotion and pain
As a check of the efficacy of the emotion manipulation, we compared mean emotion scores after each emotion manipulation to the mean emotion score for the control condition. The happiness mean score was greater in the happiness condition, t(8) = 2.83, p < .05, the sadness mean score was greater in the sadness condition, t(8) = 2.85, p < .05, and the anger mean score was marginally greater in the anger condition, t(8) = 2.24, p = .06. Further, in no emotion condition was the mean score for the emotion other than the specific emotion that had been manipulated significantly greater than the corresponding mean score that participants reported when they received the control condition, including anxiety. Thus, the emotion manipulation was deemed successful.
As a manipulation check on the efficacy of the pain stimulus, we used repeated measures analysis of variance to examine change in reported pain from the time point prior to the pain stimulus to later measurements. In each condition, acute pain increased with the pain stimulus, peaking with the ratings during the pain stimulus and returning to near baseline levels 10 minutes later. For example, during the control visit, pain ratings increased around the pain stimulus, F(1,4) = 6.70, p < .001. Average pain (across conditions) at baseline was 2.74 (SD = 2.14), immediately prior to the emotion manipulation 2.64 (SD = 1.94), during the pain stimulus 4.07 (SD = 1.77), immediately after the pain stimulus 2.94 (SD = 1.91), 10 minutes after pain 2.85 (SD = 2.02), and near the end of the study 2.61 (SD = 1.87).
Changes in response to pain across visits by emotion condition
IL-6
There was no significant main effect of time, emotional condition, reported pain, or time by condition interaction on IL-6 levels. There was, however, a significant main effect of reported state anger on IL-6 (F(1, 85.5) = 5.19, p < .05): Levels of state anger reported across the four visits were positively associated with levels of IL-6, such that when participants’ state anger in any condition was higher than their average across conditions, they evidenced higher IL-6 in that condition compared to their own average IL-6 across conditions. Further, there was a significant interaction between state anger and emotional condition for IL-6 (F(3, 84.8) = 2.72, p < .05). As shown in Figure 1, a post-hoc contrast indicated that IL-6 levels were significantly higher in the sadness condition compared to the control condition when individuals reported average or 1 SD higher than average levels of state anger relative to their own average state anger across conditions (estimated mean difference = 4.12, SE = 1.15, p < .01 for average state anger, and 9.36, SE = 3.05, p < .01 for +1 SD state anger). The pseudo R2 was .36, indicating a 36% reduction in the residual variance of IL-6.
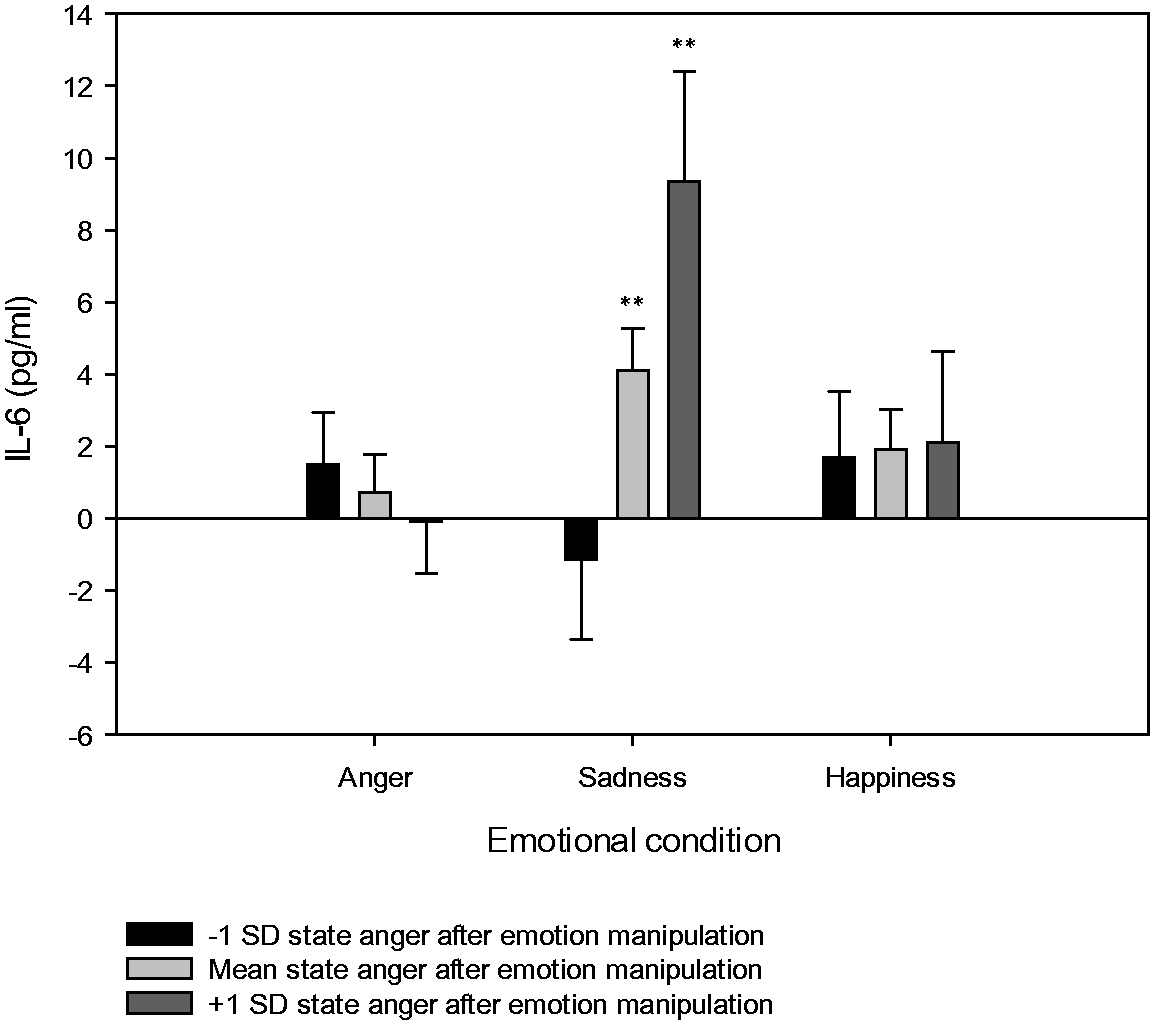
Reported anger by condition interaction effect on IL-6. The Y-axis represents the levels of average IL-6 after subtracting the level in the control condition, in each of the three emotional conditions (**p < .01).
TNF-α
There was no significant main effect of time, condition, or time by condition interaction on TNF-α. However, there was a marginal main effect of reported pain (F(1, 27.2) = 3.84, p = .06) and a significant reported pain by condition effect on TNF-α (F(3, 85.7) = 3.33, p < .05), illustrated in Figure 2. The post-hoc test indicated that TNF-α levels in the sadness condition were significantly lower than in the control condition when participants reported 1 SD lower than average levels of pain after the pain stimulus compared to their own average across visits (estimated mean difference = −7.24, SE= 2.39, p < .01). The pseudo R2 was .38, indicating a 38% reduction in the residual variance of TNF-α.

Reported pain by condition interaction effect on TNF-α. The Y-axis represents the levels of average TNF-α in each of the three emotional conditions after subtracting levels in the control condition (**p <.01).
IL-10
There was a significant main effect of time (F(2, 94) = 3.71, p < .05) that was driven by an increase in IL-10 from 10 minutes (estimated mean difference = 13.96, SE = 1.12) to 60 minutes (estimated mean difference = 17.69, SE = 1.12) at p < .05. The pseudo R2 was .07, indicating a 7% reduction in the residual variance of IL-10. There was no significant main effect of condition, time by condition interaction, or reported pain and state emotion, for IL-10.
CRP
There was no effect of pain, emotion, or condition at 100 minutes post pain on CRP.
Cortisol
The condition and time main effects and the condition by time interaction for cortisol were not statistically significant. However, as shown in Figure 3(a) to (c), there were three separate state emotion by condition interactions. First, there was a significant state anger by condition effect (F(3, 63.4) = 3.09, p < .05). As shown in Figure 3(a), cortisol levels in the sadness condition were higher than the control condition when participants reported either average or 1 SD higher than average levels of state anger compared to their own average across visits (estimated mean difference = 2.87, SE = 1.01, p < .01, and 6.93, SE = 2.58, p < .01, respectively). The pseudo R2 was .25, indicating a 25% reduction in the residual variance of cortisol. As shown in Figure 3(b), there also was a main effect of state sadness (F(1, 26.9) = 6.06, p < .05) and a marginally significant reported sadness by condition effect on cortisol levels (F(3, 82.2) = 2.47, p =.06). Cortisol levels were significantly higher in the happiness condition than the control condition when participants reported average or 1 SD higher levels of sadness compared to their own average across visits (estimated mean difference = 4.00, SE = 1.49, p < .01, and 10.76, SE= 4.25, p < .05, respectively). The pseudo R2 was .34, indicating a 34% reduction in the residual variance of cortisol. Finally, as shown in Figure 3(c), there was a significant reported happiness by condition effect on cortisol levels (F(3, 81) = 2.70, p =.05). The post-hoc contrast indicated that cortisol levels were higher in the anger condition than the control condition when participants reported a level of happiness that was at least 1 SD less than their average state happiness across conditions (estimated mean difference = −2.32, SE= 1.19, p = 05). The pseudo R2 was .29, indicating a 29% reduction in the residual variance of cortisol.
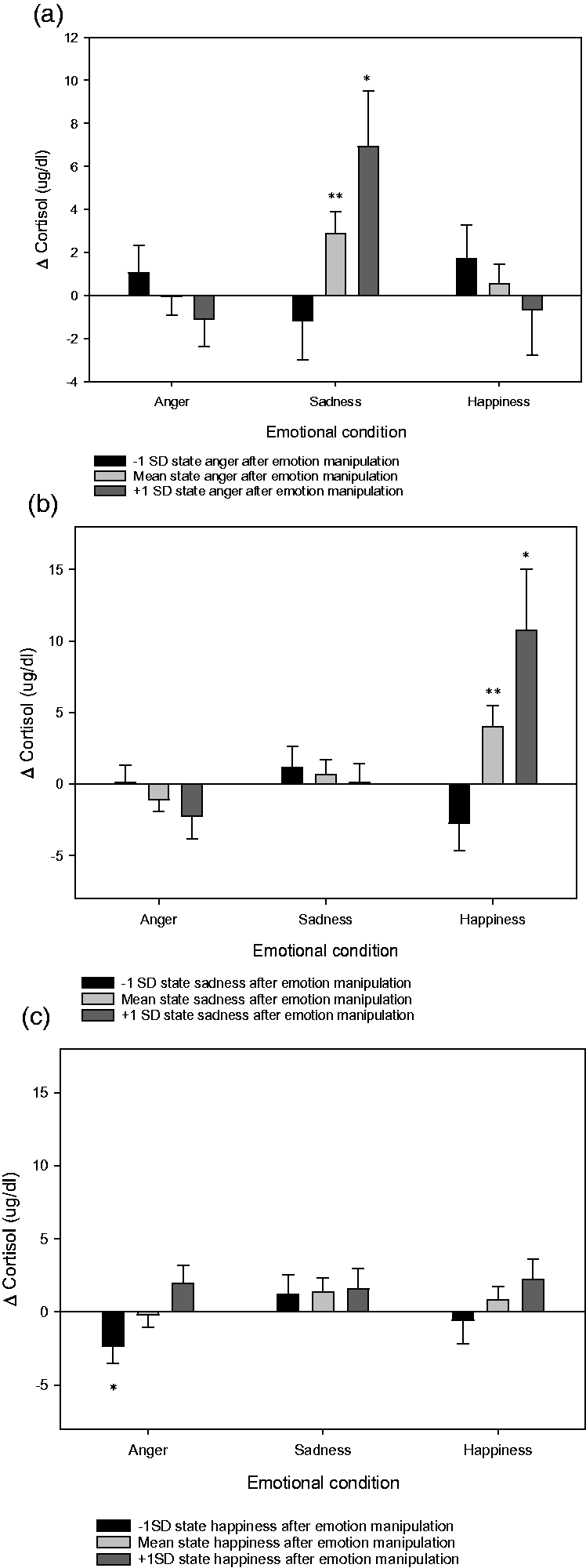
(a) State anger, (b) state sadness, and (c) state happiness by condition interaction effects on cortisol. The Y-axis represents the levels of average cortisol in each of the three emotional conditions after subtracting the levels in the control condition (*p <.05, **p <.01).
Discussion
Very little is known about how emotional state (as compared to depressive symptomatology or global recalled affect) is related to inflammatory responses to stress or pain. The present study’s preliminary results are based on a small sample of women who were living with moderate to severe RA, and for whom inflammatory responses are clinically meaningful. Our emotion manipulation encouraged the experience and expression of a particular emotion (anger, sadness, or happiness) across separate, double-blind visits that were compared to a control visit (with no emotion manipulation). Manipulated acute pain was a constant across conditions. Drawing on our planned within-subject comparisons, we found no significant effect by experimental condition. However, our planned but relatively exploratory analyses by emotion (across conditions) revealed that when participants reported greater anger than their own average, they showed elevated IL-6 levels relative to their own average IL-6 across conditions. This association between anger and IL-6 responses was in the expected direction.
One of our strongest and most consistent findings, albeit unexpected, was that when a negative emotion was experienced in the context of a manipulation for a different emotion, participants showed elevated markers of inflammation and cortisol relative to themselves in the control condition. For example, when participants in the sadness condition reported average or greater than average levels of anger, they showed elevations in the proinflammatory marker IL-6 and stress hormone cortisol. Also, participants who reported average or greater levels of sadness in the happiness condition also showed elevations in cortisol. These results were not anticipated but they are consistent with the arguments advanced by multiple theoretical perspectives related to mixed emotions and stress as well as with empirical findings related to emotional expression and suppression in the context of pain. Although our emotion manipulation was successful at increasing levels of the target emotion more than any other assessed emotion, participants nonetheless often reported multiple emotions following the emotion manipulation, as is typical. Participants who experienced anger in the experimental condition where they were asked to focus on sadness may have felt the need to suppress their anger and/or have had difficulty regulating their emotion, both phenomena related to adverse behavioral, cognitive, and physiological outcomes (Gross, 2002; Hayes, Wilson, Gifford, Follette, & Strosahl, 1996). For example, a tendency to suppress anger is associated with greater pain severity among healthy adults (Burns et al., 2003). Moreover, issues with negative affect regulation appear to influence pain responses more so than do trait tendencies to experience higher negative affect overall (Bruehl, Chung, & Burns, 2006).
Overall, our results support a broad theoretical view of how negative emotional states can function as stressors under circumstances where they cannot be identified or expressed, when they are not consistent with the social context, or when they otherwise create conflict. In response to stress, it is normative for individuals to report increased negative affect as well as decreased positive affect, and the identification and expression of negative emotion in such contexts has been linked with an attenuation of stress-provoked physiological changes (Graham et al., 2009) and pain (Burger et al., 2016; Slavin-Spenny, Lumley, Thakur, Nevedal, & Hijazi, 2013). Indeed, research on emotional disclosure more generally indicates that health benefits can arise from expressing negative emotions (Pennebaker, 1997; Smyth, 1998), in part because this can help spur the process of making meaning out of and resolving difficult experiences and feelings (Pennebaker, 1997; Pennebaker, Mehl, & Niederhoffer, 2003). However, in cases where negative emotions cause conflict (Carson et al., 2007) or cannot be identified or expressed (Pegram, Lumley, Jasinski, & Burns, 2016; Slavin-Spenny et al., 2013), negative emotions themselves may function like stressors. In the present research, a mismatch between (a) the participant’s emotional state and (b) what emotion was encouraged to be expressed may have been stressful. In support of this, similar results were seen with both IL-6 (a cytokine that has been shown to rise with psychological stress) and cortisol. From the perspective that it is stress as opposed to negative emotion per se driving inflammatory responses, these results are in concordance with recent findings that anxiety (but not anger) induced with a written laboratory task predicted greater inflammatory cytokine levels in oral fluids at 30 minutes following a stressor among undergraduates (Moons & Shields, 2015). Such results, however, have been used to support the theory that avoidance-related emotions, such as anxiety, are more likely to trigger inflammatory responses than approach-related emotions, such as anger (Moons & Shields, 2015). Our current findings do not necessarily contradict this view as much as they suggest that the experience of anger may be proinflammatory in contexts that give rise to stress-related feelings (such as anxiety or feeling out of control). Stress-related phenomena may be exacerbated among individuals living with chronic pain, for whom problems with alexithymia (difficulty in identifying and describing emotions) and emotion management appear to be particularly common (Baeza-Velasco, Carton, Almohsen, Blotman, & Gely-Nargeot, 2012; Corbishely, Hendrickson, Beutler, & Engle, 1990), and in those with RA, who also may have exacerbated inflammatory responses to stress.
It is important to remember that all of the effects observed in the present research were in the presence of an acute pain stimulus. Indeed, in one case, there was a significant interaction between experimental condition and pain, such that those who experienced lower pain after the pain stimulus in the sadness condition showed decreased TNF-α relative to their control visit. It would be valuable for future research to investigate whether strong emotions and pain might interact to predict inflammatory responses and/or how inflammation and negative emotion might interact to predict pain responses.
Limitations
The present study is limited by its small sample size. However, the within-subjects design with randomized conditions increased power for our primary analyses and reduced the need to control for between-subject constants. Nonetheless, specific results (both null and significant) should be interpreted with great caution given our small sample of women with RA and the fact that we were likely underpowered except to observe large effects. Although exclusion based on any prednisone use also would have been ideal from the standpoint of greater control, this was not feasible because the vast majority of potential participants were taking prednisone. It is also important to note that even with post-pain time points up to 100 minutes, we may not have determined the full peak of inflammatory reactivity to pain, which has been observed as late as 150 minutes post-stimulus (Geiss et al., 2005).
Laboratory methodologies in which emotion and pain are manipulated can be used to test novel hypotheses about how stress, emotion, pain, and inflammation connect in RA and other populations. Future research is also needed to examine more thoroughly our broader assertion that factors such as social context, personality, and regulation of complex negative emotion modify the degree to which negative and positive affective responses relate to physiological responses (and, in turn, physiological dysregulation and disease), and to what extent (and how consistently) identification, acknowledgement, appropriate expression, and comfort with negative emotion buffer adverse cognitive, behavioral, and physiological outcomes of affective responses to stress. In doing so, it will be important to investigate the role of naturally occurring emotion in daily life, both between-subjects as well as via within-subject designs.
Conclusions
We used a novel methodology to test whether manipulated emotional state modulated inflammatory and stress hormone responses to physical pain among a small sample of women living with RA. Research on the impact of emotion and other psychological factors on inflammatory responses among populations for whom such responses are clinically meaningful is needed to help illuminate the potential impact of such factors among those with inflammatory pain conditions. For the most part, our hypotheses were not confirmed: There was no main effect of condition or of sadness. There was, however, a main effect of anger on IL-6 across conditions, in line with expectations. Moreover, unexpected and exploratory findings were in concordance with a few recent studies suggesting that emotional states can have discernable effects on specific patterns of physiological responses to stress or pain (e.g., Carroll et al., 2011; Moons, Eisenberger, & Taylor, 2010). Further, findings were in concordance with the perspective that the experience of mixed negative emotion under certain circumstances can give rise to both psychological stress and inflammatory responses. Additional research to confirm and advance the findings of this preliminary research is needed, both among clinical as well as relatively healthy populations. Such work is important, because a more nuanced understanding of the role of emotion, psychological stress, and pain on inflammatory states may eventually elucidate novel clinical tools for inflammation and pain or help augment current pain management techniques.
Footnotes
Acknowledgments
The authors would like to thank the research assistants and the Clinical Research Center nursing staff for assistance with data collection and the participants.
Article Notes
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.