
Abstract
In considering that body image-related perceptions may be associated with weight trainers’ exercise dependence, the purpose of this study was to examine the (a) relationship between body dissatisfaction and drive for muscularity and (b) drive for muscularity as a mediator of the body dissatisfaction–exercise dependence relationship. In sum, 278 male weight trainers (Mage =29.03 years, SD = 7.83) residing in a southern city of Taiwan completed scales of body dissatisfaction, drive for muscularity, and exercise dependence. Pearson correlation analysis found that body dissatisfaction, drive for muscularity, and exercise dependence were all correlated. Further, the indirect mediation model with bootstrapping found that drive for muscularity partially mediated the body dissatisfaction–exercise dependence relationship (c path: β = .51, SE = 0.07, p=.001: c′ path: β = .13, SE = 0.80, p = .03). We concluded that male weight trainers’ body image-related perceptions influence exercise behavior and suggested that body image-related perceptions might be considered in studying exercise dependence.
Introduction
Although regularly participating in exercise brings many physical and mental health benefits (Center for Disease Control and Prevention, US Department of Health and Human Services, 2016; Ward-Ritacco et al., 2015; Wen et al., 2011), it is estimated about 3%–13% of exercisers engage in an unhealthy exercise behavior termed exercise dependence (Hamer & Karageorghis, 2007; Hausenblas & Symons Downs, 2002a; 2002b; Lejoyeux, Avrill, Richoux, Embouazza, & Nivoli, 2008). Exercise dependence is also referred to as exercise addiction (Adams & Kirkby, 2002; Allegre, Souville, Therme, & Griffiths, 2006), compulsive exercise (Dalle Grave, Calugi, & Marchesini, 2008), excessive exercise (Davis, Brewer, & Ratusny, 1993), or morbid exercise (Morgan, 1979) and is evidenced to be detrimental to exercisers’ physical and psychological well-being.
Dependent exercisers generally exhibit a constellation of behavioral and psychological impairments such as unhealthy tolerance of exercise intensity/frequency, psychological withdrawal when unable to exercise, exercise more than intended, lack of control over exercise, a great deal of time spent in activities, reduction in other activities because of exercise, and continuing to exercise despite recurrent physical and/or psychological problems (Hausenblas & Symons Downs, 2002a, 2002b; Symons Downs, Hausenblas, & Nigg, 2004). Research indicates that exercise dependence is associated with many negative consequences such as eating disorders (Harris, Geei, D’Acquisto, Ogani, & Pritchetti, 2015), lowered immune function (Furusawa, Jajima, Okawa, Takahashi, & Ogata, 2007), lowered global health (Kim et al., 2012), ignoring job and family responsibilities (Hausenblas & Symons Downs, 2002a; 2002b), and continuing exercise with physical injuries (Diekhoff, 1984; Morgan, 1979).
Because exercise dependence is associated with negative health and psychological outcomes, it is imperative to examine the factors associated with it. Specifically, it is important to examine factors underlying the relationship between individuals’ perceptions and exercise dependence. In this regard, some research found body image-related perceptions associated with exercise dependence revealing a new research direction. For example, in a large scale of investigation with 1766 runners, Cook et al. (2015) found social physique anxiety and exercise identity predicted exercise dependence, and social physique anxiety moderated the exercise identity–exercise dependence relationship. Similarly, in a systematic examination of the associations of drive for muscularity (DM), eating disorder, and exercise dependence, Tod and Edwards (2015) found that DM has moderate effects on weight training (.31), disordered eating (.30), and exercise dependence (.43). Based on this preliminary research, we proposed that two body image perceptions—DM and body dissatisfaction—might be associated with exercise dependence, and that DM might mediate body dissatisfaction–exercise dependence relationship.
DM is referred to a desire to increase muscularity in the body shape (Edwards, Tod, & Molnar, 2014; McCreary, 2007; McCreary, Karvinen, & Davis, 2006; McCreary & Sasse, 2000; McCreary, Saucier, & Courtenay, 2005). According to related research (e.g., Bergeron & Tylka, 2007; Daniel & Bridges, 2010; Lantz, Rhea, & Cornelius, 2002), men are preoccupied with developing big muscles in pectorals, biceps, quads, shoulders, and abdominals in order to make them look like a muscular mesomorph which is defined as having a large bone structure, large muscles, and a naturally athletic physique (Baechle & Earle, 2008, p. 145). Research has found DM prevalent in adolescents, body builders, and college students (e.g., Chittester & Hausenblas, 2009; Edwards et al., 2014; McCreary, 2007; McCreary & Sasse, 2000; McCreary et al., 2005). To achieve a muscular physique, men may use steroids, ephedrine, and diet to control their body weights and increase muscle mass (Cafria, Thompson, Ricciardelli, McCabeb, Smolakc, & Yesalisc, 2005; Drewnowski, Kurth, & Krahn, 1995; Tod & Edwards, 2015), but the most common strategy that men adopted is weight training (Hildebrandt, Lagenbucher, & Sclundt, 2004; Grogan, 2017; Kyrejto, Mosewich, Kowalski, Mack, & Crocker, 2008; Thompson & Cafri, 2007). Empirical studies found when men are driven for muscularity, they engage in heavy training, which is associated with exercise dependence (Chittester & Hausenblas, 2009; Hale, Roth, DeLong, & Briggs, 2010; Tod & Edwards, 2015).
In addition to DM, we considered body dissatisfaction as another psychological variable that predicts exercise dependence. Body dissatisfaction refers to a person’s negative thoughts and feelings about his or her body because of a difference between the ideal body and current body (Grogan, 2017; Thompson, 1990). Traditionally, research on body dissatisfaction has focused on women. However, research has also found men disturbed by their body images. For example, Frederick et al. (2007) administered Multidimensional Body Self-Relations Questionnaire to 2206 male undergraduates and found 15% of men were not satisfied with their bodies. Similar results were found by Cash, Winstead, and Janda (1986). Generally, these studies found most men aspire to a muscular mesomorphic shape, such as well-developed muscles on chest, arms, and shoulders (Franko et al., 2015; Frederick et al., 2007).
Further, men use all types of measures to achieve their ideal body shapes. Specifically, research found that men engage in weight training to increase their muscle mass. Baker (1994) indicated that half a million British men engage in weight training in order to increase muscles. Similar results were found in the United States (Thompson & Cafri, 2007), Australia (O’Dea & Abraham, 2002), and Taiwan (Chang & Huang, 2015). Moreover, the research also indicates that men’s body dissatisfaction is associated with heavy training and exercise dependence (Hausenblas & Fallon, 2002; Hausenblas & Symons Downs, 2002a, 2002b).
Therefore, it seems that there are positive relationships among body dissatisfaction, DM, and exercise dependence. Based on previous literature, DM stands in the middle between body dissatisfaction and exercise dependence. On one hand, body dissatisfaction leads to DM (e.g., Arbour & Martin-Ginis, 2006; Grabarek & Cooper, 2008; McCreary & Sasse, 2000; Tylka, Bergeron, & Schwartz, 2005; Robert, Munroe-Chandler, & Gammage, 2009), on the other hand, DM leads to exercise dependence (e.g., Chittester & Hausenblas, 2009; Hale et al., 2010; Tod & Edwards, 2015). Based on the related research, it can be inferred that DM is the mediator between body dissatisfaction–exercise dependence. Unfortunately, to best of our knowledge, there is no single study that examines men’s body dissatisfaction, DM, and exercise dependence or specifically examines the mediating role of DM on the body dissatisfaction–exercise dependence relationship.
The present study
The purposes of this study were to examine the relationships among DM, body dissatisfaction, and exercise dependence and examine the mediating role of a DM on the body dissatisfaction–exercise dependence relationship. We hypothesized that DM would mediate the relationship between body dissatisfaction and exercise dependence. As Baron and Kenny (1986, p. 1176) suggested that mediator is a third variable (i.e., DM) that explains how the independent variable (i.e., body dissatisfaction) affects the dependent variable (i.e., exercise dependence). We hypothesized that body dissatisfaction, DM, and exercise dependence would be correlated, and DM would mediate body dissatisfaction–exercise dependence relationship.
Methods
Participants
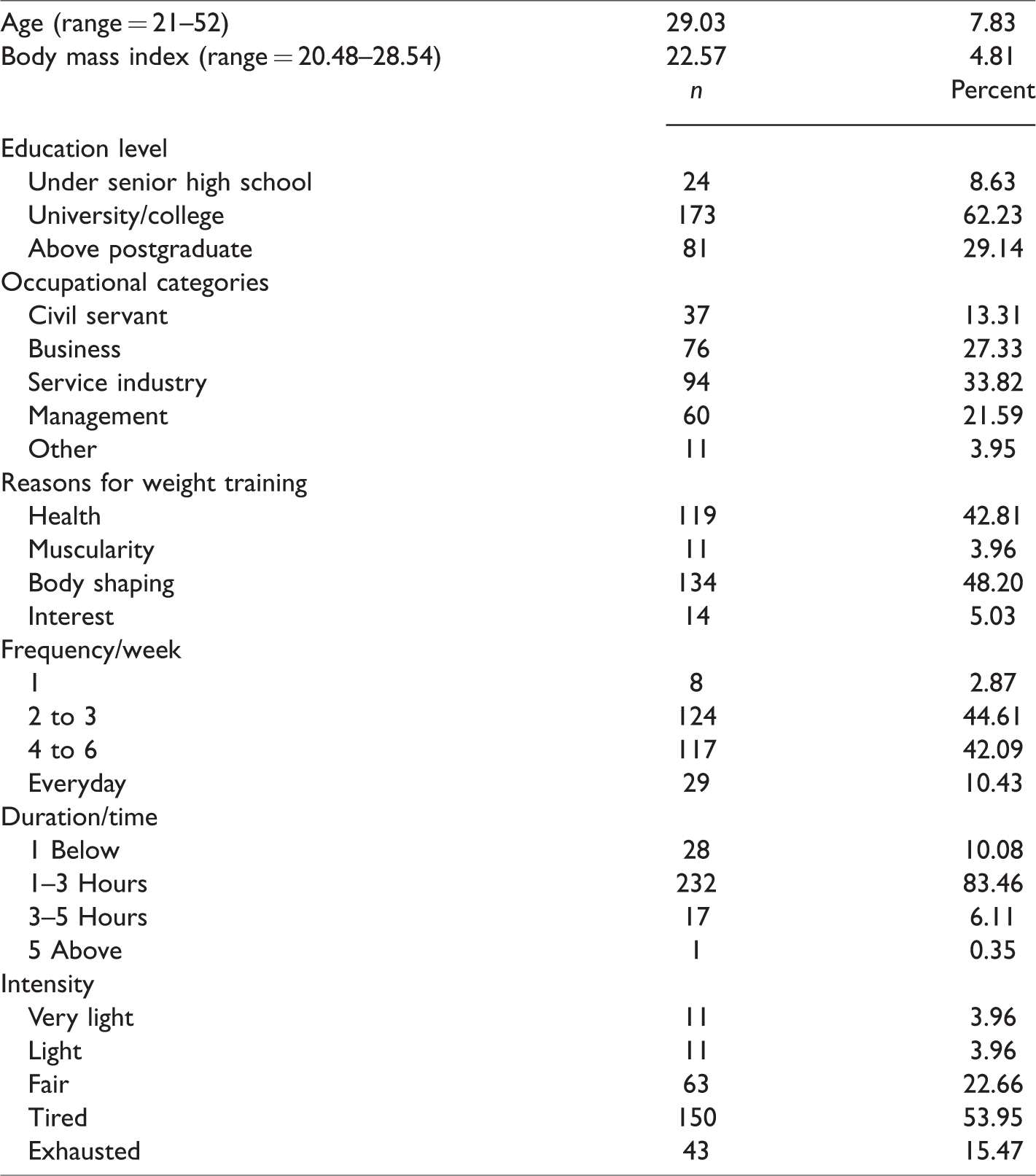
Originally, 305 participants completed the survey package. After we excluded those who participated in weight training for competition, nonregular exercisers, and those who engaged in competitive sports for those participants might contaminate research findings. Finally, a total of 278 males (Mage =29.03 years, SD = 7.83) voluntarily participated in this study. Participants were community residents in a southern city of Taiwan. Nearly half, 48.02% (n = 134), reported their reasons for weight training were for body shape, and the other, 51.98% (n = 144), reported health, fitness, and recreation reasons. They engaged in weight training for an average of 3.14 years (SD = 1.84), four times/week, and 89.2% (n = 250) trained more than 1 hour each time.
Measures
Demographic questionnaire
The demographic questionnaire was designed to collect participants’ background information including age, height, weight, current training behavior (including frequency per week, duration and intensity of each time), years of experiences, and reasons for training.
Muscular Figure Rating Scale
Adopted from Higgins’ (1987) self-discrepancy theory, Muscular Figure Rating Scale (MFRS; Peters & Phelps, 2001) is used to assess one’s evaluation of the discrepancy between actual and ideal body size. The higher scores on the MFRS represent higher body dissatisfaction (Frederick et al., 2007). To measure body size discrepancy, participants rated nine drawings of body shape arranged and numbered from 1 (thin) to 9 (very muscular). Two items of the MFRS were adopted in the present study: actual body size perception and ideal body size perception. For “actual body size perception,” the participant identified the figure that represents his current body size, while “ideal body perception” is the body shape he desired. Subtracting the ideal body perception from the actual body perception yields the body perception discrepancy. Body perception discrepancy ratings larger than zero indicate that the participants would like to be muscular, zero represents no discrepancy, whereas negative ratings indicate no desire of muscularity (Lynch & Zellner, 1999). The MFRS has been validated in Taiwan with appropriate validity and reliability (Shih & Kubo, 2013). Also, MFRS has good test–retest reliability (two-week intra-class correlation: 0.75 in boys and 0.91 in girls, respectively) with Taiwanese populations (Chen, Fox, & Haase, 2008).
Drive for Muscularity Scale
Developed by McCreary and Sasse (2000), the Drive for Muscularity Scale (DMS) is a 15-item, self-reported inventory in evaluating one’s desire to attain a muscular physique. DMS represents an individual’s desire to be muscular. Participants rate each item on a six-point Likert-type scale ranging from 1 (never) to 6 (always). The DMS has shown good internal consistency, with a Cronbach’s α of .87, and good construct validity (McCreary & Sasse, 2000). The internal consistency of DMS in this study was also acceptable (Cronbach’s α = .87).
Exercise Dependence Scale-Revised
The Exercise Dependence Scale-Revised (EDS-R; Symons Downs et al., 2004) is a 21-item, self-reported inventory evaluating maladaptive symptoms of exercise behavior. Participants rated each item on a six-point Likert-type scale ranging from 1 (never) to 6 (always). A lower score indicates fewer exercise dependence symptoms and vice versa. The EDS-R has been evidenced a good internal consistency (Cronbach’s α ranging from .78 to .91) and good construct validity (Tucker–Lewis Index = .85; Confirmatory Fit Index = .96; root mean square error of approximation = .06; average absolute standardized residuals = .03) (Symons Downs et al., 2004). The Cronbach’s α of this study was .83, which is an acceptable level. The EDS-R measures seven syndromes of exercise dependence—tolerance, withdrawal, intention effects, lack of control, time, continuance, and reduction in other activities. To evaluate participants’ overall exercise dependence behavior, we used a composite score by adding all seven factors together.
Procedure
Following the approval of the university research ethical committee, we visited eight fitness centers located in southern Taiwan and asked permission to collect data at these selected centers. We set up a booth to recruit participants from those who came to fitness centers. If participants were interested in the study, we introduced the general purpose of the study, the methods of completing questionnaires, and their rights as a participant. To prevent social desirability effects, we informed participants that this is a study to explore their exercise experiences, and there are no right or wrong answers. In addition, we asked participants to answer the questions as truthfully as possible, and all responses would be confidential. After the briefing, participants who interested in this study then signed a consent form and completed the survey package. It took about 20 minutes to complete the questionnaire. After that, each participant received a convenience store coupon (equal to 3.3 US dollars) as a token of appreciation.
Statistical analyses
First, we used descriptive statistics to examine skewness, kurtosis, and outliers. Pearson product–moment correlation analysis was used to examine the relationships of all variables and provide the information about whether the independent variable (i.e., body dissatisfaction), dependent variable (i.e., exercise dependence), and mediating variable (i.e., DM) were all correlated. This analysis was conducted as a prerequisite analysis for testing mediator effects (Baron & Kenny, 1986). According to Baron and Kenny (1986), to examine mediation, the following conditions should be met: (a) body dissatisfaction should predict DM, (b) DM should predict exercise dependence, and (c) body dissatisfaction should predict exercise dependence. If all three conditions were met, the subsequent mediating effects of DM on the relationship between body dissatisfaction and exercise dependence were further analyzed.
Next, we followed Preacher and Hayes’s (2004, 2008) procedures for examining mediation model with bootstrapping. Mediation analyses testing the a path (i.e., the effect of body dissatisfaction (independent variable) on DM (mediator variable)); b path (i.e., the direct effect of the mediator on the exercise dependence (dependent variable)); the c′ path (i.e., the direct effect of independent variable on dependent variable); and c path (the total effect of the independent variable on the dependent variable) were conducted (see Figure 1). Further, an estimate of the indirect effect was tested using the standard error and 95% confidence intervals calculated from 1000 bootstrapped samples.

Mediation model with study variables.
Results
Preliminary analysis
The descriptive statistics revealed that participants were mostly mature adults (age ranged from 21 to 52 years) with normal body shape (body mass index ranging from 20.48 to 28.54), well education, and white-collar occupations. There are 48.2% of participants engaged in weight training for body shape, 97.1% trained at least two times/week, 89.92% trained more than 1 hour, and 69.42% indicated their training intensity was “somehow heavy.” Further, all variables had adequate skewness (ranging from 0.28 to 1.23) and kurtosis (ranging from 0.39 to 1.38) indicating that study variables did not exceed ±2, and all variables were in an acceptable range of normality. In addition, no outliers were found (see Table 1).
Participants characteristics (N = 278).
Bivariate correlations
As presented in Table 2, body dissatisfaction, DM, and exercise dependence were all positively correlated. Body dissatisfaction correlated with DM (r = .19, p < .01) and exercise dependence (r =.22, p < .001). Exercise dependence positively correlated with DM (r =.54, p < .001).
Bivariate correlations of study variables.
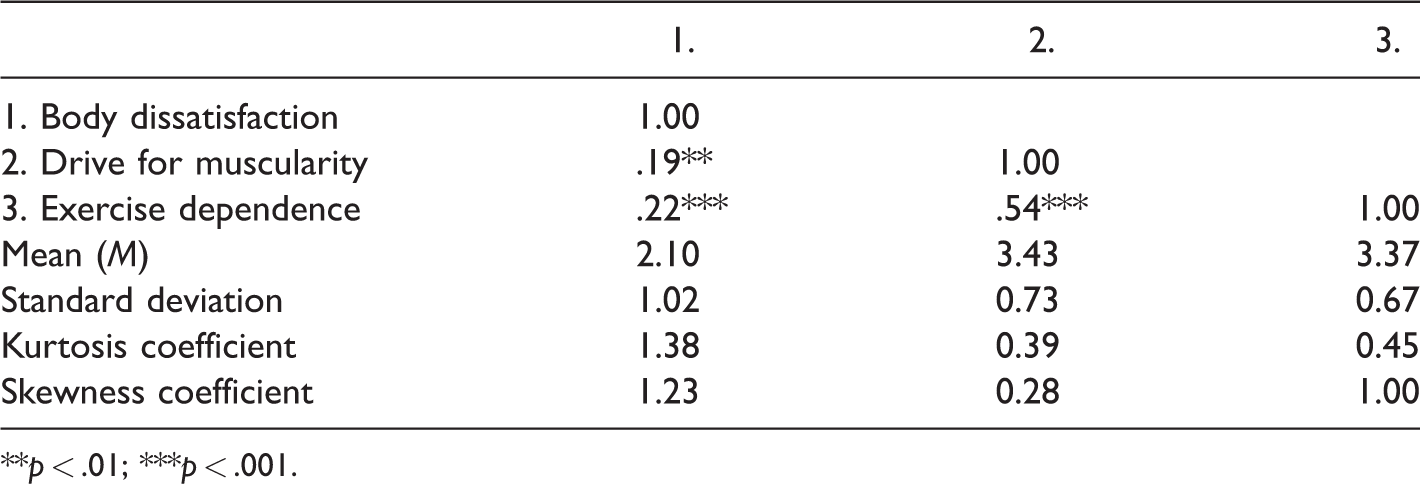
**p < .01; ***p < .001.
Mediating effects of DM on body dissatisfaction–exercise dependence relationship
Figure 1 shows a significant effect of the a path (β = .19, SE = 0.72, p = .01), b path (β = .51, SE = 0.07, p = .001), the c′ path (β = .13, SE = 0.80, p = .03), and the c path (β = .51, SE = 0.07, p=.001). The bootstrapped indirect effect (c′ = .35, SE = 0.03, 95% CI = (0.01–0.08)) was significant, indicating that DM mediated the relationship between body dissatisfaction and exercise dependence. This mediation model accounted for 30% of the variance in the relationship between body dissatisfaction and exercise dependence.
Discussion
Theoretical contributions/implications
In considering that body image-related perceptions may be associated with exercise dependence, the present study sampled male weight trainers and examined the relationships among DM, body dissatisfaction, and exercise dependence. Results found that all study variables were positively correlated, and DM partially mediated the body dissatisfaction–exercise dependence relationship. The results supported the associations of body dissatisfaction and exercise dependence (e.g., Hausenblas & Fallon, 2002; Hausenblas & Symons Downs, 2002a, 2002b), the associations of body dissatisfaction and DM (e.g., Arbour & Martin-Ginis, 2006; Grabarek & Cooper, 2008; McCreary & Sasse, 2000; Robert et al., 2009; Tylka et al., 2005), and the association of DM and exercise dependence (e.g., Chittester & Hausenblas, 2009; Hale et al., 2010; Tod & Edwards, 2015). Further, the present study advanced our knowledge in that DM mediated the male weight trainers’ body dissatisfaction–exercise dependence relationship. The preliminary results provide several implications for researchers and practitioners as follows.
The association of body dissatisfaction and DM confirms that men are also disturbed by body shape and aspire to have a muscular physique (Cash et al., 1986; Franko et al., 2015; Frederick et al., 2007). Men’s body dissatisfaction association with DM can be explained by cultural, media, or social influences. For example, Monaghan (2008) found that western men are preoccupied with a slender, toned, and muscular physique as ideal image. Further, Holmqvist-Gattario et al. (2015) found that western males (United States, United Kingdom, Australia, and Sweden) generally conform to peers’ norms on ideal physical shape and believe a muscular physique is attractive. McCrary and Saucier (2009) found that when males have more information about socially desired body image, they had a higher DM. We suggest future study may examine the relationship between the DM and exercise dependence from a social comparison perspective (Robert et al., 2009). Moreover, some research suggests internalization of the muscular physique (Cash, 2012), self-efficacy (Burgess, Grogan, & Burwitz, 2006), and body appreciation (Tylka & Wood-Barcalow, 2015) might be associated with body dissatisfaction and DM. Future research may consider how these variables influence the relationships among body dissatisfaction, DM, and exercise dependence.
The association between the DM and exercise dependence is an important issue for researchers and health professionals. DM is prevalent in adolescents and college students (Edwards et al., 2014; McCreary & Sasse, 2000; McCreary et al., 2005), and those who are extremely occupied by a muscular physique might use unhealthy behaviors such as anabolic steroids to increase muscles (Drewnowski et al., 1995), which may increase the risk of sudden cardiac death, liver disease, aggression, infertility in males, and development of male sex characteristics in females (Kanayama, Brower, Wood, Hudson, & Pope, 2010). Exercise dependence has been associated with negative effects such as eating disorders (Harris et al., 2015), lowered immune function (Furusawa et al., 2007), global health (Kim et al., 2012), ignoring job and family responsibilities (Hausenblas & Symons Downs, 2002a, 2002b), and keeping exercise under physical injuries (Grandi, Clementi, Guidi, Benassi, & Tossani, 2011). Thus, researchers and practitioners should pay attention to exercisers’ DM and its association with exercise dependence.
The association between body dissatisfaction and exercise dependence and the mediating role of DM needs to be carefully interpreted. First, our study was cross-sectional. It cannot be interpreted as cause-and-effect, although past research found that DM is the consequence of body dissatisfaction (e.g., Arbour & Martin-Ginis, 2006; Grabarek & Cooper, 2008; McCreary & Sasse, 2000; Robert et al., 2009; Tylka et al., 2005), and DM lead to exercise dependence (e.g., Chittester & Hausenblas, 2009; Hale et al., 2010; Tod & Edwards, 2015). The bootstrapping model simply provided preliminary evidence of a mediating effect of DM on the body dissatisfaction–exercise dependence relationship. We recommend that future study adopts longitudinal designs to examine the causal links among body dissatisfaction–DM–exercise dependence.
Our participants’ characteristics and exercise behaviors also provide guides for research in the area of body image and exercise dependence. They were mostly urban residents, mature males, and middle class. Their goals for weight training were body shaping, muscularity, and health. They engage in weight training more than three times per week and more than 50% exercise more than 1 hour per time with fair to high intensity. Such demographics support that young males engage in weight training to enhance one’s body image (e.g., Baker, 1994; Chang & Huang, 2015; Pope, Phillips, & Olivardia, 2000; Thompson & Cafri, 2007). Also, their training behavior fits the recommendation for the development of muscles and muscular power (Bompa & Haff, 2009). Worthy of note is that more than 50% of participants have engaged in high frequency, intensity, and duration exercise, which increases the incidence of exercise dependence (Hausenblas & Symons Downs, 2002a; 2002b). Thus, our results provide evidence that the DM is also prevalent in Taiwan, along with the risk of body dissatisfaction and exercise dependence.
Limitations and future suggestions
Several limitations should be addressed. First, our study was cross-sectional in nature. Therefore, the cause–effect relationship cannot be determined. Future study may adopt longitudinal designs to examine how body dissatisfaction influences DM and, subsequently, influences exercise dependence. Second, our samples were recruited from Taiwanese male weight trainers, the results may not be generalized to women or men from other cultures. Moreover, because we used weight trainers, whether the relationships among body dissatisfaction, DM, and exercise dependence are similar for participants in different types of exercise, such as aerobic dance, running, and swimming, needs further examination. Furthermore, although we used body dissatisfaction and DM as research variables, we recommend future researchers to examine the associations of other body image-related perceptions (e.g., social physique anxiety, physical self, and body esteem) and with exercise dependence.
Conclusion
Regularly participating in physical activities can bring both physical and mental health benefits. However, our study found body image-related perceptions associated with unhealthy exercise behavior. To promote overall health and well-being from participating in physical activities, researchers and practitioners should be aware that some men engage in weight training and become dependent because of body dissatisfaction and DM. Therefore, practitioners should try to reduce exercisers’ body dissatisfaction, promote positive body image, and arrange flexible exercise programs in order to offer a healthy exercise and physical activity environment.
Footnotes
Article Notes
Ethical approval
All procedures performed in this study involving human participants were in accordance with the ethical standards of the National University of Kaohsiung Institutional Review Board (# NUK-REC-2011001) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.