
Abstract
Depression is now the leading cause of disability worldwide, and globally more than 300 million people of all ages suffer from depression. Depression, despite its major health consequences, frequently goes unnoticed among university students, since their lives are often filled with symptoms normally associated with depression (e.g., loss of sleep, low energy, anxiety, and sadness). Successful adaptation to depression depends on the use of adequate coping strategies. The extent to which university students in India with high and low levels of depressive symptoms use adequate or inadequate coping strategies has not been evaluated. Based on the Center for Epidemiological Scale for Depression score, students were assigned to either the high depressive symptoms or the low depressive symptoms group. We used the Coping Response Inventory-Adult to determine the dominant coping strategies used by the two depressive symptoms groups. The high depressive symptom group resorted to more avoidant coping strategies than the low depressive symptom group, and women were more likely to use avoidant coping strategies than men.
Introduction
Depression is now the leading cause of disability worldwide, and globally more than 300 million people of all ages suffer from depression (World Health Organization [WHO], 2018). The WHO (2018) estimated that approximately 57 million individuals experience depressive disorders in India. University students are going through major transitions in life and face many new stresses, making them vulnerable to depression (National Institute of Mental Health, 2009). A recent study conducted on 700 randomly selected students from a single Indian university found that almost half of the sample was suffering from moderate to severe depression (Deb et al., 2016). Depression can affect a student’s decision-making ability, social interactions, and overall emotional well-being (Ceyhan, Ceyhan, & Kurty, 2009; Mikolajczyk et al., 2008). Untreated depression can result in serious consequences such as suicide (Cukrowicz et al., 2011; Farabaugh et al., 2012).
Enrolling in a university is a major life-changing event that imposes new stresses on students who may not have the skills or maturity to manage them. Many new students find it difficult to balance their social lives, study time, expectations of family, and relationships with new friends. This can generate negative self-esteem, which in turn can cause new stresses (Ceyhan et al., 2009; Crocker & Luhtanen, 2003; Lee, Olson, Locke, Michelson, & Odes, 2009).
Over time, individuals develop a preference for specific coping styles for dealing with transition and stress. Coping is defined as a response aimed at diminishing the physical, emotional, and psychological burden that is linked to stressful life events (Snyder, Ford, & Harris, 1987). Researchers tend to recognize two broad coping approaches: (1) approach vs. avoidance and (2) problem focused vs. emotion focused (e.g., Moos, 1993). In approach coping, attempts are made to address directly the perceived problems, while in avoidance coping, attempts are made to manage stress by ignoring the problems or repressing the anxiety associated with the problems.
Billings and Moos (1985)identified three specific coping strategies: (1) active behavioral coping, which “reflects behavioral attempts to directly deal with the problem”; (2) active cognitive coping, which “indicates attempts to manage one’s appraisal of the stressfulness of the event”; and (3) avoidance coping, which “includes avoidance, denial and tension reduction.” Approach coping strategies have a more positive impact on depression than avoidance coping (Bouteyre, Maurel, & Bernaud, 2007; Grant et al., 2013). Studies of college students in France and Turkey have shown that students who use approach coping strategies are better adjusted to college stresses and are less vulnerable to depression than those who use avoidance coping strategies (Bostanci et al., 2005; Verger, Guagliardo, Gilbert, Rouillon & Kovess-Masfety, 2010).
Women often cope with stress in social contexts differently than do men (Yeh, Huang, Chou, & Wan, 2009). Women tend to be less instrumental (i.e., less direct) in their approach to social stress problem-solving than men. Women are more likely than men to engage in discussions of their problems and emotionally vent, while men tend to suppress and control their emotions, thus engaging in more cognitive than behavioral avoidance (Melendez, Mayordomo, Sancho, & Tomas, 2012).
The existing studies on depression in university students in India have not focused on the relationship between depression and coping strategies (e.g., Deb et al., 2016; Singh, Lal, & Shekhar, 2010). The objective of the current study is to examine the relationship between gender and coping strategies in groups of students with high and low depressive symptoms from an Indian University. It is expected that students with high depressive symptoms will exhibit less effective coping strategies than those with low depressive symptoms. It is also expected that women will be more likely than men to use avoidance coping strategies to deal with stress and depressive symptoms.
Method
Participants
All participants first completed an informed consent document that gave a brief overview of the study. We used a convenience sample of undergraduate students drawn from colleges affiliated with the University of Delhi. A random selection of participants following a second depression screening produced a total sample of 120 participants (60 men and 60 women). The age range of all participants was 17 to 22 years (M = 18.79, SE = 0.12). In the high depressive symptoms group, 48.33% of participants were pursuing a science major (i.e., physics/chemistry or biology), 45% represented arts majors, and 6.66% was pursuing a business major. In the low depressive symptoms group, 40% of participants were pursuing a science major, 48.33% represented arts majors, and 11.66% was pursuing a business major.
Measures
Center for Epidemiological Studies-Depression Scale
The Center for Epidemiological Studies-Depression Scale (CES-D; Radloff, 1977), a 20-item self-report scale (English version), was utilized to screen for current levels of depressive symptoms (Wright et al., 2012). Participants rate themselves on each item on a four-point Likert-type scale ranging from 0 (rarely or none of the time) to 3 (most or all of the time). Scores range from 0 to 60, with higher scores reflecting more depressive symptoms. The recommended cut-off score of 16 (and above) was used to classify individuals as at risk or not at risk for depression (Mulrow et al., 1995). Cronbach’s alpha coefficients for the CES-D range from .84 to .90 for the general population (Morin et al., 2011; Radloff, 1977). Researchers have demonstrated acceptable reliability and validity for the CES-D when used with other cultures such as Asians (e.g., Kuo & Tsai, 1986). In our sample, Cronbach’s alpha was .90 for the CES-D.
Coping Response Inventory-Adult
We used the Coping Responses Inventory-Adult (CRI-A; Moos, 1993) to assess students’ coping responses (English version). The reliability coefficients of the CRI-Adult range from .58 to .74, thus indicating adequate internal consistency (Pretorius, Walker, & Esterhuyse, 2010). On this scale, participants were asked to identify the most important problem or stressful situation they have experienced in the past 12 months (focal stressor), and then they were asked to rate the frequency with which they engaged in each type of coping strategy on a four-point Likert-type scale ranging from 0 (not at all) to 3 (fairly often). The CRI-A assesses eight subscales of coping, each of which is measured by six items. Approach coping is measured by the first four subscales and avoidance coping is measured by the second four subscales. The four approach coping subscales include: (1) logical analysis, a form of cognitive coping; (2) positive reappraisal, a form of cognitive coping; (3) seek guidance and support, a form of behavioral coping; and (4) problem-solving, a form of behavioral coping. Approach coping is the mean score of participant responses to items in these four subscales. The four avoidance coping subscales include: (1) cognitive avoidance, a form of cognitive coping; (2) acceptance and resignation, a form of cognitive coping; (3) seek alternative rewards, a form of behavioral coping; and (4) emotional discharge, which represents behavioral coping. Avoidance coping is the mean score of participant responses to items in these four subscales.
Procedure
Participants completed the CES-D twice with an interval of two weeks between the first and second testing to provide an estimate of response reliability. At first testing, 364 participants completed the CES-D. Following the first administration of the CES-D, an attempt was made to contact all the study participants who were initially screened.
From the initial screening of 166 high depressive symptom participants, 71 could not be reached or refused to continue. Of the 95 remaining participants with high depressive symptoms who agreed to participate, a random number generator was used to select 30 men and 30 women for the study.
From the low depressive symptom group of 198 participants, 85 could not be contacted or refused to continue. Of the available 113 participants with low depressive symptoms, 30 men and 30 women were randomly selected using a random number generator. Thus, the total sample size was 120. The final sample size was determined by financial constraints, since this study is a subset of a larger study investigating the neuropsychobiological correlates of depression such as cortisol, serotonin, and heart rate variability.
Data analyses
Data were analyzed using the Statistical Package for Social Sciences (IBM PASW Statistics-version 25.0, Chicago) for windows. The alpha error rate was set to .05, and tests were conducted as two-tailed tests. For the given sample size and design, power was initially estimated to be approximately .78.
Results
Depressive symptoms
All analyses for depressive symptoms were computed using the CES-D data from the second screening, since that data most accurately reflected the subjects’ current emotional status. The CES-D test–retest reliability was r = .78, p < .001.
To determine how group and gender differed on each factor of the CES-D, separate 2 (group) × 2 (gender) ANOVAs were computed for each factor and the ANOVA results are presented in Table 1.
Two-way ANOVAs for the CES-D factors by Group × Gender.
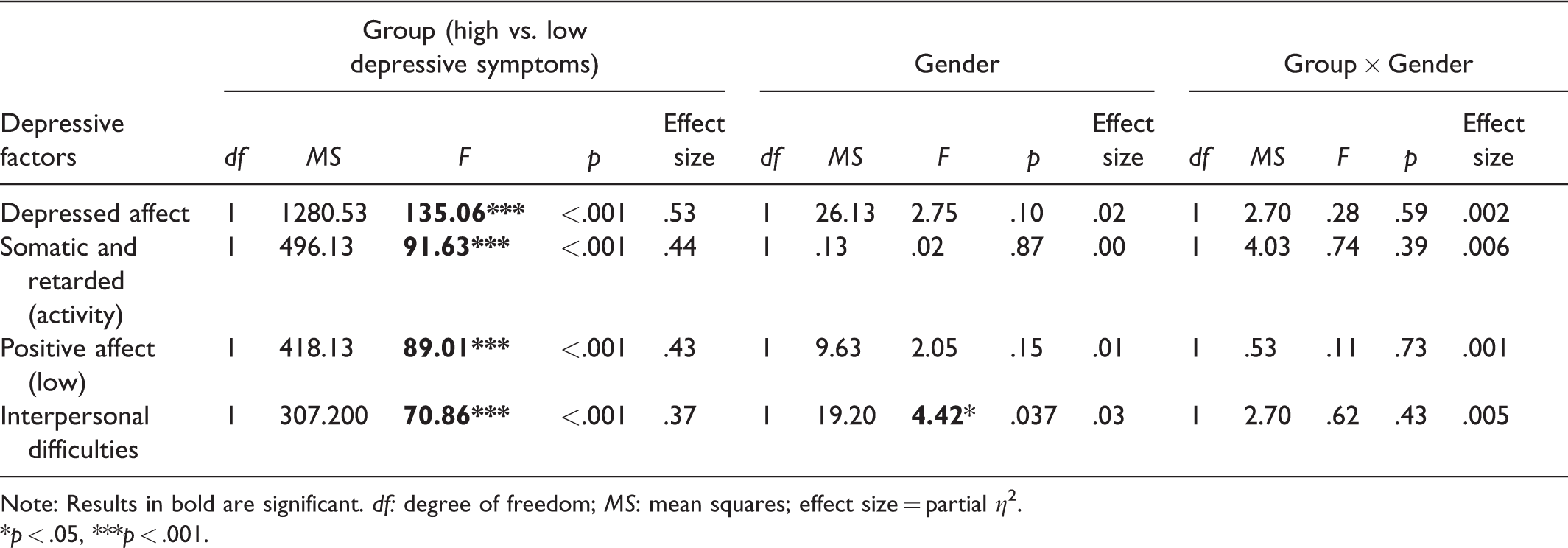
Note: Results in bold are significant. df:degree of freedom; MS: mean squares; effect size = partial η2.
*p < .05, ***p < .001.
Results show significant differences between the high and low depressive symptom groups for all four factors of the CES-D. The high depressive symptoms group reported significantly higher symptoms of depressed affect (M = 8.85, SE = 1) than did the low depressive symptoms group (M = 2.32, SE = 1.95). This group also showed higher somatic and retarded activity (M = 7.92, SE = .69) than the low depressive symptoms group (M = 3.85; SE = .98). Furthermore, the high depressive symptom group showed greater interpersonal difficulties (M = 4.28, SE = .69), indicating more interpersonal challenges (e.g., unfriendliness and dislike), than the low depressive symptom group (M = 1.08; SE = .27). The high depressive symptom group also reported lower positive affect (M = 5.95, SE = .15) than the low depressive symptom group (M = 2.22, SE = 1.76).
Table 1also shows that men and women significantly differed on the CES-D interpersonal skills factor. Men show significantly greater interpersonal difficulties (M = 3.08, SE = .63) than women (M = 2.28, SE = .70). We did not find a significant interaction effect between depressive symptoms and gender.
Coping strategies in depression
Data analysis results for coping strategies involved 2 (group: high depressive symptom vs. low depressive symptom) × 2 (gender: men vs. women) ANOVAs for each of the subscales of the CRI-adult, which are presented in Table 2. We note that there was no significant interaction effect for depressive symptoms and gender in any of the coping subscales. Figure 1shows coping subscales data for the high and low depressive symptom groups.

Coping strategies in high and low depressive groups.
Two-way ANOVAs of coping strategy by Group (high depressive vs. low depressive) and Gender.

df:degree of freedom; MS: mean squares; ANOVAs: analyses of variance.*p<.05, **p<.01, ***p<.001.
Logical analysis
The high depressive symptom group (M = 47.43, SE = 1.89) did not differ on scores for logical analysis from the low depressive symptom group (M = 48.12, SE = 2.19). Women in our sample were more likely to use logical analysis to cope with stressors (M = 46.10, SE = 2.21) than men (M = 49.45, SE = 1.77).
Positive reappraisal
The mean score for the high depressive symptom group did not differ on positive reappraisal (M = 52.40, SE = 1.89) from the low depressive symptom group mean score (M = 54.37, SE = 1.50). There was no difference between men (M = 54.48, SE = 1.54) and women (M = 52.28, SE = 1.80) in the use of positive reappraisal to cope with stressors.
Seeking guidance and support
The high depressive symptom group showed lower scores on seeking guidance and support (M = 46.18, SE = 2.01) than the low depressive symptom group (M = 49.28, SE = 2.10). Men and women did not differ on seeking guidance and support as a coping strategy.
Problem-solving
The mean score for problem-solving for the high depressive symptoms group was lower (M = 47.28, SE = 2.26) than the mean score for the low depressive symptom group (M = 53.29, SE = 2.33). Women were less likely to use problem-solving coping strategies (M = 48.55, SE = 2.24) than men (M = 52, SE = 2.3).
Cognitive avoidance
The high depressive symptom group reported higher cognitive avoidance (M = 61.03, SE = 1.85) than the low depressive symptoms group (M = 53.02, SE = 2.33). Men and women did not differ on this coping style.
Acceptance or resignation
The high depressive symptom group was more likely to deal with a stressor by acceptance or resignation (M = 54.85, SE = 2.26) than the low depressive symptom group (M = 47.72, SE = 9.52). Women had higher acceptance or resignation scores (M = 53.63, SE = 2.50) than men (M = 48.93, SE = 2.39).
Seeking alternative rewards (focusing on other more rewarding behaviors)
The high depressive symptom group did not differ (M = 61.37, SE = 1.72) from the low depressive symptom group (M = 62.47, SE = 1.80) in the frequency in which they used the alternative rewards coping style. Men were more likely (M = 63.5, SE = 1.67) than women (M = 60.33, SE = 1.77) to seek alternate rewards as a coping style.
Emotional discharge
The high depressive symptom group expressed more emotional discharge (M = 63.68, SE = 2.32) than the low depressive symptom group (M = 53.62, SE = 2.62). Women relied on emotional discharge (M = 60.78, SE = 2.69) more often than men (M = 56.52; SE = 2.85).
Discussion
We found all four CES-D factors distinguished the high from low depressive symptom group, confirming the validity of the CES-D factor structure for this sample of college students from an Indian University. Our findings are consistent with previous studies that have demonstrated higher depressed affect and lower positive affect in individuals with higher depression scores (Lewinsohn, Petit, Joiner, & Seeley, 2003). These findings support emotion-based models of depression (Depue & Iacono, 1989), which propose that depression is characterized by elevated negative affect and decreased positive affect and adjustment.
We also found that the high depressive symptoms group reported more interpersonal difficulties than the low depressive symptoms group. While this finding was expected, it is not known whether the poor interpersonal skills precede the development of depression or whether it is a consequence of depression. According to Coyne’s (1976)interpersonal theory of depression, individuals with high depressive symptoms utilize excessive reassurance seeking, which can result in interpersonal rejection and can then magnify depressive symptoms, this finding is supported by other studies (Asnani, Pandey, & Sawhney, 2004; Ceyhan et al., 2009; Joiner, 1997; Mikolajczyk et al., 2008; Olsson, 1998).
Our sample of Indian students with elevated depressive symptoms often experienced low positive affect, and less often repressed affect, somatic symptoms, and high interpersonal difficulties. We did not find somatic complaints to be the chief symptom of depression in this sample of students. Experiencing somatic symptoms as part of depression will likely vary by culture and whether there is “secondary gain” associated with adopting the “sick person” role (Lu, Bond, Friedman, & Chang, 2010). Research has demonstrated that somatic complaints are lower in economically advantaged and more educated individuals (Ryder et al., 2008). The low somatic symptom rate in our sample may reflect the higher than average socioeconomic status of these students.
Our findings reveal that the high depressive symptoms group differed from the low depressive symptoms on five of the eight coping strategies. The high depressive group was more likely to use avoidant coping strategies and less likely to use approach coping strategies. These results are consistent with previous studies that have demonstrated a close relationship between depressive symptoms and maladaptive coping strategies (Bouteyre et al., 2007; Grant et al., 2013). It is not surprising that depression would reduce adaptive coping capacity and increase the use of avoidance coping strategies (Sadaghiani & Sorkhab, 2013).
College students in our study with high depressive symptoms were less likely to seek guidance (an active coping style) than those with low depressive symptoms. Our findings are in line with previous studies that show individuals with high depressive symptoms are reluctant to seek guidance and support compared to those with low depressive symptoms (Osborn & Egede, 2012). While the reason why individuals in the high depressive symptom group generally avoid an active coping strategy is not clear, it could be for fear of criticism, low self-esteem, or concern about rejection (Herres & Ohannessian, 2015). Previous studies conducted with medical students have reported that such students are reluctant to reveal that they are having problems for fear of negative evaluations, which in turn creates additional stress and increases the chances of career failure (Chew-Graham, Rogers, & Yassin, 2003; Hames, Hagan, & Joiner, 2013). Another possible reason can be potential influence of cultural expectations for academic achievement. For example, students in India are expected to academically excel and meet parental expectations for success. These individuals may experience criticism if they do not meet those expectations or show signs of not meeting the expectations by seeking help. Studies have shown that in the Indian culture, family and friends may minimize or trivialize a person’s emotional problems and discourage help seeking, thus causing the stressor to lead to depressive symptoms (Sharma & Wavare, 2013).
The high depressive symptom group was more likely to use cognitive avoidance coping strategies such as acceptance or resignation and emotional discharge than the low depressive symptoms group. Cognitive avoidance, which is arguably the most primitive of linkage-focused styles, is used to reduce stress and anxiety by blocking awareness of issues. This, in turn, restricts an individual’s access to environmental reward and potentially increases punishing experiences, which according to Ferster’s (1973)behavioral model of avoidance, serves as a catalyst for the development of depressive symptom. Cognitive avoidance is known to predict both anxiety and depression symptoms in a nonclinical student samples (Bouteyre et al., 2007). Cognitive avoidance may lead individuals to avoid thinking realistically about their problems and to try to escape from their problems, thus increasing the severity of depression (Blalock & Joiner, 2000).
Men and women did not differ on symptoms of depressed affect, somatic activity, and positive affect. However, there were gender differences for interpersonal difficulties, with men scoring higher on interpersonal difficulties. While there was no difference overall between men and women in depressive symptoms, significant gender differences were found for several coping strategies. Women were less likely than men to use logical analysis and problem-solving strategies. In contrast, women were more likely than men to use avoidance coping strategies such as resignation and emotional discharge. These results are consistent with previous studies showing that men usually are more problem oriented, use more direct actions to solve their problems, and are more likely to use logical analyses when confronting a problem or challenge (Folkman & Lazarus, 1980; Nolen-Hoeksema & Aldao, 2011). This can be partially explained by the socialization hypothesis, which argues that men are socialized to a greater extent to deal instrumentally with stress, whereas women tend to be socialized to express emotion, employ avoidance focused coping methods, and seek the support of others (Mataud, 2004; Melendez et al., 2012).
Conclusion
These results support the use of the CES-D in a sample of Indian university students, since the four CES-D factors distinguished those with high levels of depressive symptoms from those with low levels of depressive symptoms. As expected, Indian students with high depressive symptoms are characterized by high-depressed affect, low positive affect, high somatic symptoms, more interpersonal difficulties, and avoidant coping strategies. In addition, we found, as expected, that women tend to use more avoidant coping strategies than men, independent of depressive symptoms.
Limitations/future areas of research
A limitation of the current study is that we did not study students with DSM-based depression diagnoses. Instead, we analyzed the coping style of two group of students, one with high depressive symptoms and one with low depressive symptoms. While the CES-D is a well-respected depression inventory, future studies should examine depressive symptoms and coping strategies in college students who have DSM-5-based diagnoses of depression. Also, we did not collect demographic data from the participants who refused to participate. Future research should determine if there are unique demographic characteristics of participants who refuse to participate.