
Abstract
While attachment assessments developed for infancy and adulthood are well established, no such gold standard measure exists for school years, where measures are not yet sufficiently robust. Nevertheless, the last decade has witnessed some progress in this field with the development of the Child Attachment Interview (CAI), a semistructured interview designed to access children’s mental representations of their attachment relationships. This study aimed to test the validity and reliability of the CAI for an Italian population, using a normative group and a clinical group of disruptive behavior disorder and somatic symptom disorder patients. A total sample of 311 Italian children (213 normative and 98 clinical) aged 8 to 15 years completed a battery of measures assessing attachment, verbal IQ, and symptomatology. The psychometric properties of the CAI alongside other children (Kerns Security Scale, Inventory of Parent and Peer Attachment) and parents (Adult Attachment Interview) attachment measures in normative sample, as well as the distribution of attachment patterns in normative and clinical samples, were examined. The results revealed the CAI to have adequate interrater and test–retest reliability, as well as discriminant, and convergent validity. Significant differences in the CAI’s distribution of attachment patterns for normative and specific clinical groups were found. Taken together, the findings show that the CAI Italian version is a reliable and valid measure for assessing attachment in school years and beyond.
Keywords
Introduction
Attachment research (Fearon et al., 2010; Groh et al., 2012) has shown that emotional and behavioral regulatory patterns developed within the parent–child relationship influence the way that children express their emotions and behaviors and, consequently, their mental health. The majority of attachment research examining the link between attachment and mental health has been conducted within community samples using a developmental psychopathology theoretical framework or within clinical samples of infants or adults with heterogeneous pathology. Little is known regarding attachment in middle childhood and early adolescence. This is due because the research on attachment during this period remains relatively modest compared with the study of attachment in infancy or adulthood, reflecting the need for an appropriate measure of attachment for this developmental period (Bosmans & Kerns, 2015).
Middle childhood and early adolescence are interesting periods connoted by cognitive and emotional changes in which also the attachment system is characterized by profound change: the goal of attachment shifts from maintaining proximity to assuring the availability of the attachment figure; the attachment relationship evolves into a collaborative partnership between child and parent, with greater co-regulation of contact; and attachment representations become more elaborate and organized (Bosmans & Kerns, 2015). Therefore, approaches to assessing attachment during this period must take into account the moving target of child development, in terms of both the evolving function of the attachment system and the ever-changing abilities of the child (Jewell et al., 2019). Although no gold standard tool exists for assessing attachment in middle childhood and early adolescence, four measurement approaches dominate: self-report questionnaires, projective assessments, interviews, and secure base script assessments (Bosmans & Kerns, 2015). The differences between these measurement approaches make it difficult to compare findings across studies (Borelli et al., 2016). Furthermore, many tools (e.g., questionnaires) do not capture attachment disorganization, which is the strongest predictor of psychopathological outcomes (Fearon et al., 2010; Groh et al., 2012; Madigan et al., 2016). As a consequence, many of the methodologies lack robust validation (Jewell et al., 2019).
As a response to the need for a developmentally appropriate measure for assessing attachment in middle childhood and early adolescence, the Child Attachment Interview (CAI; Target et al., 2007) is a semistructured interview designed to access children’s mental representations of their attachment relationships. Using verbatim transcripts and videotapes of the interview, coders classify attachment both categorically and dimensionally (Shmueli-Goetz et al., 2008). The CAI was originally intended for use with 7- to 12-year-olds (Shmueli-Goetz et al., 2008) but has subsequently been used up to the age of 17 years (Venta et al., 2014).
The CAI has been used with nonclinical and clinical populations (for a review, see Privizzini, 2017). In particular, the use of CAI in a clinical context mainly has focused on heterogeneous clinical samples (Hart et al., 2017; Jardin et al., 2017; Shmueli-Goetz et al., 2008; Target et al., 2003; Venta et al., 2014; Venta et al., 2015) but recently also on samples of children with specific clinical conditions, such as depressive symptoms and shyness accompanied by parental reports of social anxiety, inattention, and thought problems (Borelli et al., 2010), Attention Deficit Hyperactivity Disorder (Rasmussen et al., 2019), somatic symptom disorders (SSD; Bizzi, 2019), disruptive behavior disorders (Bizzi et al., 2015, 2018, 2019), obese adolescent females (Holland et al., 2012), and adolescents with self-harm and suicide-related thoughts and behaviors (Glazebrook et al., 2015; Venta & Sharp, 2014).
The original validation study of CAI was based on a UK sample and reported good psychometric properties (see Shmueli-Goetz et al., 2008; Target et al., 2003). Subsequent cross-cultural studies have since established its validity for other cultures and languages (Borelli et al., 2016; Röder et al., 2015; Venta et al., 2014; Zachrisson et al., 2011). For example, Zachrisson et al. (2011) tested the psychometric proprieties of CAI in a sample of Norwegian children, while Venta et al. (2014) in a sample of US adolescents with psychiatric disorders; Borelli et al. (2016) found associations in American children between CAI variables and self-report measures of attachment, CAI variables and internalizing symptoms above and beyond self-reported attachment, and CAI variables and child temperament; and Röder et al. (2015) demonstrated the relation of CAI with personality characteristics and aggression in a German-speaking sample. Nevertheless, in the Italian context, a paucity of cross-cultural studies on attachment during school years is evident (Cassibba et al., 2013). For these reasons, we believe that it is essential to increase research in this field.
In this regard, a preliminary study (Cavanna et al., 2018) has already been conducted on a subset of the current study’s sample, testing the CAI’s convergent validity with other attachment measures (i.e., Separation Anxiety Test), and comparing the CAI’s attachment distribution with the findings of other attachment studies, as well as subjects with psychopathology with subjects with normal development. Nevertheless, several aspects remained unexplored. For this reason, the current study aimed to be innovative in that to our knowledge it is the first to compare the CAI’s classification of children with another measure of attachment (i.e., the Kerns Security Scale (KSS)) and with the Adult Attachment Interview’s (AAI) classification of fathers as well as mothers. Second, it is the first validation study to compare two specific clinical disorders with opposite characteristics in terms of externalizing and internalizing problems (respectively, disruptive behavior disorders (DBD) and SSDs)).
The reasons for choosing those two clinical groups (DBD and SSD) are due to (a) the need to know a priori the type of psychopathological condition and to be able to control through its selection. In other studies, there is usually a general clinical group, where all disorders and their intensity are included; (b) the possibility of exploring whether the CAI is capable of discriminating between specific psychopathological conditions that have opposite characteristics in terms of internalizing and externalizing disorders. Despite DBD (i.e., a disorder associated with a range of problematic oppositional, aggressive, destructive, and antisocial behaviors) and SSD (i.e., a disorder characterized by multiple physical complaints without identifiable physiological causes accompanied by thoughts, feelings, and unusual behaviors related to the physical symptom presentation) are characterized by different clinical manifestions, both are similar being among the most reasons for consultation in primary care clinical settings and increasing in the pediatric population. They also constitute disorders with high social cost, since they can greatly impair the adaptive functioning of the child in various contexts of life, as school (poor performance, failure), family life (verbal and physical conflict), and social conflict (isolation, school dropout, entry into dissociative groups) (Greenberg et al., 2001; Schulte & Petermann, 2011).
The first objective of the current study was to test the cross-cultural validity of the CAI in an Italian sample following the original validation study (Shmueli-Goetz et al., 2008). Under this main objective, several aims were subsumed: (a) to establish the CAI’s interrater reliability, using two expert, independent coders; (b) to test its test–retest reliability, after three-month and one-year intervals; (c) to establish its discriminant validity, in terms of its (expected) independence of age, gender, socioeconomic status (SES), and verbal IQ; (d) to test its convergent validity, in terms of its (expected) overlap with other attachment measures (self-report); and (e) to test its convergent validity, in terms of (expected) correspondence between the attachment classification of the parents and the child. The second objective was to compare—in terms of both CAI categories and CAI dimensions—the attachment patterns of a normative (nonclinical) group and a clinical group made up of the specific clinical disorders DBD and SSD.
Method
Study design
To establish the cross-cultural adaptation of the CAI in the Italian context, the study was conducted in five stages. Initially, the original English version of the CAI was translated into Italian (phase 1). In the second phase, a total of 311 (clinical and normative) children were recruited to assess attachment both categorically and dimensionally. Successively, the normative group composed of 213 children (n = 142 aged 8–12 years and n = 71 aged 13–15 years) were selected to test the correspondence between CAI attachment and self-report attachment measures, as well as to test the relations with gender, age, socioeconomic status, and verbal IQ (phase 3). Following this, a subsample of 53 normative children selected voluntarily was identified to take part in a three-month test–retest, while 49 were selected to take part in a one-year follow-up (phase 4). The dropouts were due to parents refusing to continue the study. In the fifth phase, a subsample of 77 children selected voluntarily was recruited from the normative group to test correspondence between the attachment classifications of the children and those of their parents captured using the AAI. Specifically, 77 mothers and 71 fathers were assessed. The limited number of participants in the phase was due to difficulties with being audio/video-recorded, time constraints, and lack of interest. Figure 1 shows a concise overview of which participants were used in several phases to test the psychometric proprieties of CAI’s Italian adaptation. The methodological choice to test test -retest reliability, convergent, and discriminant validity only in the normative group was made in order to limit possible influences by clinical outcome.
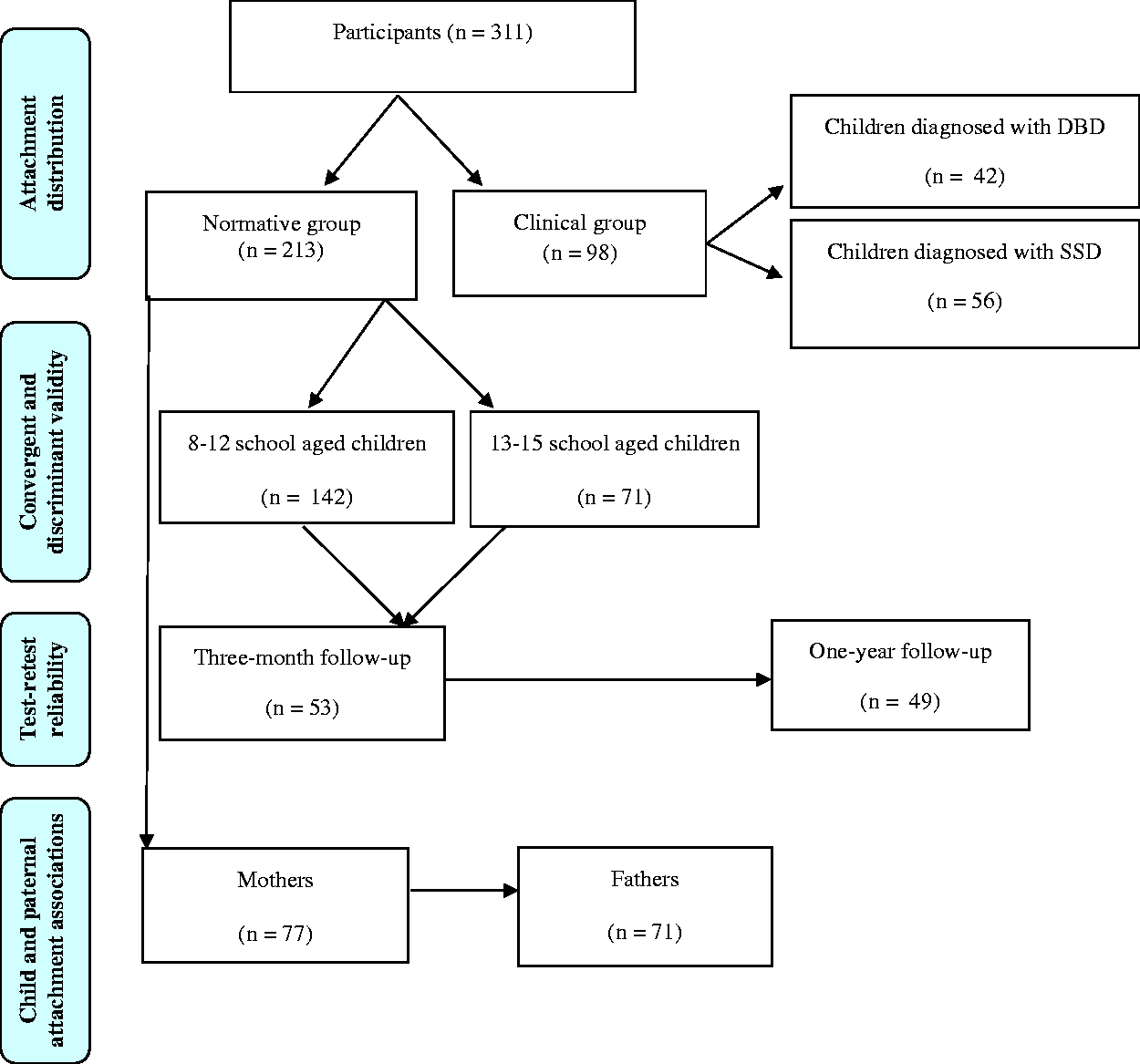
Participants recruited for the cross-cultural adaptation of Child Attachment Interview in the Italian context.
Participants
The total sample consisted of 311 Italian children (aged 8–15 years), whose parents were approached for permission for their children to participate in a study on social and emotional development in childhood. All participants were Caucasian, born and lived in Italy. Two-hundred and thirteen children with no known mental health problems (parents completed the Child Behavior Checklist 6–18 Version; Achenbach & Rescorla, 2001) were recruited from urban and rural schools: they constituted the normative group. A further 98 children were recruited from an Italian pediatric hospital: they constituted the clinical group. Children in the clinical group had received a diagnosis of DBD (N = 42) or SSD (N = 56) from two Italian child mental health specialists following several clinical interviews with parents and the child (regarding the child’s developmental history and functioning); other specialists also examined them to exclude causes of organic origin in suspected SSD (through laboratory test, computed tomography, body magnetic resonance imaging). During the diagnostic process, parents also completed the Child Behavior Checklist 6–18 Version (Achenbach & Rescorla, 2001), and children whose scores exceeded the clinical cut-off for oppositional defiant/conduct problems or somatic problems (t score ≥65) were selected; however, those with comorbid symptomatology in the DBD and SSD groups were excluded from the study.
The gender, age, SES, and verbal IQ of the participants are shown in Table 1. Comparing normative (N = 213) and clinical (N = 98) groups, two groups differed significantly on gender (male: 46% in normative group vs. 58% in clinical group; χ2(2) = 3.99, p = .046) and SES (low SES less than 15,000 €/y: 14% in normative group vs. 52% in clinical group; χ2(2) = 17.85, p < .001). Conversely, comparing the two clinical groups (DBD and SSD), the children differed significantly with respect to gender (male: 79% in DBD group vs. 43% in SSD group; χ2(1) = 12.580, p < .001) and mean age of 11.9 years (SD = 2.03) in DBD group vs. 10.78 years (SD = 2.1) in SSD group; t(96) = –2.85, p = .005.
Demographic characteristics of the sample.

DBD: disruptive behavior disorder; SSD: somatic symptom disorder; SES: socioeconomic status.
*p ≤ .05, **p < .001.
Measures
CAI (Target et al., 2007) is a semistructured interview used to assess attachment by accessing children’s mental representations of attachment relationships. The development of the interview and coding system was informed by existing methodologies, including the AAI (George et al., 1985), which focuses on discourse analysis; the Strange Situation Procedure (SSP; Ainsworth et al., 1978), which focuses on meaningful behaviors in context; and Luborsky and Crits-Christoph’s (1990) system of partitioning narratives into discrete relationship episodes. The current interview protocol contains 19 questions (CAI revised edition VIII; Shmueli-Goetz et al., 2008) and opens with a warm-up question eliciting information on family composition. This is followed by a series of questions tapping into the child’s self-representation, representations of his/her primary caregivers, and times of conflict, distress, illness, hurt, separation, and loss. The interview, which lasts approximately 45 minutes, must be video-recorded and transcribed to aid coding; it may only be conducted by individuals who have a reliability certificate for this purpose.
The CAI coding comprises the following subscales: Emotional Openness (EO), Balance of Positive and Negative Reference to Attachment Figures (BAL), Use of Examples (UoE), Preoccupied Anger to mother/father (IA-M/F), Idealization to mother/father (ID-M/F), Dismissal to mother/father (DS-M/F), Resolution of Conflicts (RES), and Overall Coherence (COH). A score between 1 and 9 is assigned to each of the scales. Three scales (Preoccupied Anger, Idealization, and Dismissal) are rated separately for each attachment figure. The pattern of scores on the above dimensions in part determines the child’s attachment classification for each caregiver separately. Four attachment patterns can be identified: Secure (S), Dismissing (Ds), Preoccupied (P), and Disorganized (D). The Secure pattern reflects undistorted affective and cognitive information about the availability of the attachment figures and their capacity to provide safety and comfort. The Dismissing and Preoccupied patterns reflect representations of the attachment figures as being unavailable and/or unpredictable and strategies to cope with these experiences; the Ds pattern is characterized by an idealization of the caregivers and/or dismissal of the impact of separation and loss, while the P pattern is manifested in angry or passive blame of attachment figures for their shortcomings. The Disorganized category (having no coherent strategy to cope with unpredictable or unresponsive attachment figures) is based on a qualitative judgment and is not anchored in the rating scales. Its coding procedure is based on the presence versus absence of certain markers of attachment Disorganization informed by two major sources: behavioral manifestations, including those identified as characteristic of Disorganized attachment in the SSP but with some additional markers appropriate to the behavior of older children (e.g., the child exhibits immature and controlling behaviors or shows inconsistent engagement with the interviewer), and disruptions to the narrative used in classifying certain AAI transcripts as Unresolved. Besides, clear contradictions between verbal and nonverbal behavior are considered.
KSS (Kerns et al., 1996; Italian version; Calvo, 1998) is a 15-item self-report measure for children aged 8 to 12 years. It assesses an attachment figure’s (either mother’s or father’s) responsiveness and availability and the child’s perceived ability to rely upon that parent. The measure is rated on a 4-point scale in which responses are selected based on Harter’s (1982) format (i.e., some kids … vs. other kids … ). There is a separate form for mothers and fathers, although the questions on both are identical. After deciding which statement applies most to them, children then select between really true for me and sort of true for me. Adequate psychometric properties have previously been demonstrated (Kerns et al., 2005). In the present study, internal consistency was good, with Cronbach’s α = .73 for the mother form and .81 for the father form.
Inventory of Parent and Peer Attachment (IPPA; Armsden & Greenberg, 1989; Italian version; San Martini et al., 2009) is a self-report measure for children aged 13 to 15 years that measures children’s security perceptions of their parents (Attachment scale). Twenty-five mother and 25 father items are scored on a 5-point Likert scale (ranging from 1 = almost never or never true, to 5 = almost always or always true), yielding a total score on Trust, Communication, and Alienation (reversed, so that higher scores correspond to less alienation) subscales for each parent. Previous research has demonstrated adequate internal reliability (Armsden & Greenberg, 1989), as does the present study (Cronbach’s α = .84 for both parent items).
Wechsler Intelligence Scale for Children-IV (WISC-IV; Wechsler, 2003; Italian version; Orsini et al., 2012) is a well-established and validated measure of the intellectual abilities of children aged 6 to 16 years. For the current study, the following subtests were used as a measure of verbal IQ: (a) Similarities, (b) Vocabulary, and (c) Comprehension. In the present study, internal consistency was good, with Cronbach’s α = .80.
AAI (George et al., 1985) is a semistructured interview comprising 20 questions covering early childhood, adolescence, and adulthood. The AAI attempts to capture the adult’s current state of mind concerning attachment rather than his/her actual or probable experiences, although the latter is also considered when coders assign a classification. The AAIs are transcribed verbatim and coded using the Adult Attachment Scoring and Classification System (Main et al., 2002). This system employs 17 ordinal scales of 1 to 9 points each, organized into two groups: the subject’s inferred childhood experience and current attachment states of mind, both relating to their parents and global. Five attachment classifications are obtained—three organized: Free/Autonomous (F/A), Dismissing (Ds), and Entangled (E) and two not organized: Unresolved to Loss/Abuse (U) and Cannot Classify (CC). In our study, there were no cases under CC. The transcripts in our study were rated by two expert coders, both of whom had a reliability certificate. The AAI coders were different from the CAI coders and were blind to the CAI rating. Kappa was calculated as an estimate of agreement on the AAI classifications (ranging from .81 to .96) and intraclass correlation coefficients (ICCs) on the AAI scales (higher values of .80).
Procedure
The Italian version of the CAI was translated according to a process of back-translation (Brislin, 1970). Three independent researchers (authors of this study) with excellent knowledge of English and an extensive psychological vocabulary translated the protocol from English to Italian, trying to avoid jargonistic expressions and ambiguous phrases. A common version of the interview was subsequently agreed, translated into English by a bilingual person with an extensive psychological vocabulary.
The study was approved by the Ethics Committee of Gaslini Hospital (Genoa, Italy) for the clinical groups and by the Ethics Committee of the Department of Educational Science of University of Genoa (Italy) for the normative group. About the clinical group, during the children’s hospitalization, the doctors responsible for their assessment and treatment informed first the family and then the child about the study, handed out an information sheet, and asked them to consider participating. If they agreed, a visit by the researcher was scheduled. With the normative group, both parents were contacted first with information regarding the study; the parents and their children then provided informed written consent/assent and were advised about their option to withdraw from the study at any time should they so wish.
Assessments were conducted in a private room at the hospital for the clinical group and at home for the normative group, by a psychologist/researcher who had been trained in administering the study’s battery of assessment measures (two consecutive days of training in the CAI were run by one of the authors in person). The CAI was administered first, followed by the KSS or IPPA and the three subtests of the WISC-IV (Similarities, Vocabulary, and Comprehension). In a separate room, parents were asked to complete a sociodemographic questionnaire. In the test–retest phase, only the CAI was readministered to the child, while in phase 4, both parents completed the AAI.
Statistical analysis
The data were analyzed using the Statistical Package for the Social Science (Version 21.0; IBM Corp., Armonk, NY, USA). Demographic variables were depicted using descriptive statistics. Frequency analyses were used to test nominal and categorical variable distributions; the chi-square test was used to test nominal and categorical variables, and Student t tests and variance analysis were used to compare group means. Correlations were assessed by Pearson’s r coefficient; Kappa and ICC coefficients were used to calculate interrater agreement on the categorical and numerical variables. Results were considered statistically significant when p was ≤.05.
Results
Italian psychometric proprieties of CAI
Interrater reliability of CAI
The total number of CAI interviews included in the calculation of interrater reliability was 355 (311 CAIs and 44 retests CAIs for normative and clinical samples combined). Interrater reliability was tested by two expert CAI coders who had attended specific training (three-day training course resulting in the reliability coding of 30 interviews) on administration and coding. Kappa (κ) was calculated as an estimate of agreement: for two-way classifications (Secure vs. Insecure), agreement was 95.3% (κ = .90) for mothers and 95.9% (κ = .91) for fathers; for three-way classifications (S, Ds, P), agreement was 94.9% (κ = .92) for mothers and 95.9% (κ = .93) for fathers; and for four-way classifications (S, Ds, P, D), agreement was 89.4% (κ = .85) for mothers and 91.9% (κ = .89) for fathers. The ICC used to calculate interrater agreement on the scales showed values ranging from .58 to .98.
Test–retest reliability of CAI
Fifty-three normative children completed the CAI (administered by the same interviewer) after three months and 49 after one year. Attrition analyses were conducted to test whether this group who agreed to the follow-up interviews was significantly different on demographic variables than the group who did not continue. Results showed no significant differences on age (t(211) = .68, p = .498), verbal IQ (t(211) = .71, p = .475), and SES (χ2(1) 1.48, p = .223), but only on gender (male: 41% in group who agreed to the follow-up interviews vs. 60% in group who did not continue; χ2(1)= 5.95, p = .015).
To test test–retest reliability two independent coders, blind to the baseline CAI classifications, rated the interviews at the two retest periods. Classifications of both parents at three months and one year were stable, with kappa’s values ranging from .68 to .96 for two-, three-, and four-way classifications (except for Disorganization, which showed a kappa of .50 for mothers and .62 for fathers after one year). CAI scales were also stable at the three-month interval (with correlation values from .77 to .93) and after one year (with correlations ranging from .72 to .92).
Relations with gender, age, SES, and verbal IQ
We examined the discriminant validity of the CAI by exploring associations between demographic variables (including verbal IQ) and attachment classifications (two-way) for both parents in the normative sample. One-way analyses of variance (ANOVAs) and chi-square tests were computed. Age and SES emerged as significantly different as a function of mother (age: F(1, 212) = 15.74, p = .000, eta2 = .069; SES: χ2(2) = 4.35, p = .038, eta2 = .026) and father (age: F(1, 210) = 6.92, p = .009, eta2 = .032; SES: χ2(2) = 5.11, p = .025, eta2 = .030) attachment classifications. There was a significant tendency for children rated as Secure with both parents to be older (Msecure = 12.24, SD = 2.34; Minsecure = 10.95, SD = 2.55) and to have a higher SES (47.8% of parents earned more than 36,000 €/y, 43.5% between 15,000 and 36,000 €/y, and 8.7% less than 15,000 €/y) than their Insecure counterparts. Gender did not emerge as significantly different with respect to mother (χ2(1) = 2.58, p = .108, ns) or father (χ2(1) = 2.02, p = .156, ns) attachment classifications. In establishing the relation of verbal IQ and attachment classifications, one-way ANOVAs did not reveal statistically significant differences between secure and insecure children in terms of mother (F(1, 212) = .80, p = .738, ns) or father (F(1, 210) = .84, p = .688, ns).
Correlations with self-report measures of attachment
We examined the convergent validity of the CAI by exploring associations between scales of the KSS or the IPPA (self-report measures of attachment) and CAI scales in the normative sample. The KSS was administered to the 142 children aged 8 to 12 years and the IPPA to the remaining children aged 13 to 15 years. As shown in Table 2, significant correlations between the CAI and KSS scales with respect to mother (not to father) were found. Significant correlations between CAI and IPPA scales to both parents were also found.
Correlations between Child Attachment Interview scales and attachment self-report measures (Kerns Security Scales and Inventory of Parents and Peer Attachment scales).

KSS: Kerns Security Scale; Security mother: Perceived Attachment Security to mother; Security father: Perceived Attachment Security to father; Total: Perceived Attachment Security to both parents; Discrepancy: discrepancy between Perceived Attachment Security to mother and to father; IPPA: Inventory of Parents and Peer Attachment scales; EO: Emotional Openness; BAL: Balance of Positive and Negative Reference to Attachment Figures; UoE: Use of Examples; IA-M/F: Preoccupied Anger to mother/father; ID-M/F: Idealization to mother/father; DS-M/F: Dismissal to mother/father; RES: Resolution of Conflicts; COH: Overall Coherence.
*p < .05, **p < .01.
Correlations with parental attachment
In order to test another aspect of the CAI’s convergent validity, correlations between the CAI classifications of the children and parents’ attachment as measured by the AAI were examined. Attrition analyses were conducted to test whether this group (i.e., the groups of 77 normative participants who agreed to test correlations with parental attachment) was significantly different on demographic variables than the group who did not continue. Results showed no significant differences on gender (χ2(1) = .01, p = .934), verbal IQ (t(211) = –1.78, p = .076), and SES (χ2(1) 7.12 p < .399), but only on age (M = 10.81, SD = 2.22) in group who agreed to the follow-up interviews vs. (M = 11.86, SD = 2.32) in group who did not continue; t(211) = .29, p = .004.
As shown in Table 3, the correlation between the CAI and AAI with two-way classifications was significant: 30 children classified as having Secure attachment on the CAI had AAI-classified Autonomous (Secure) mothers, and 21 had Autonomous (Secure) fathers (χ2(1) = 9.674, p = .002, κ = .32; χ2(1) = 5.757, p = .016, κ = .29, respectively). Besides, significant associations were found for fathers (χ2(2) = 10.95, p = .027, κ = .11) but not for mothers (χ2(2) = 7.25, p = .123, κ = .09) for three classifications.
Associations between children and parental attachment representation.
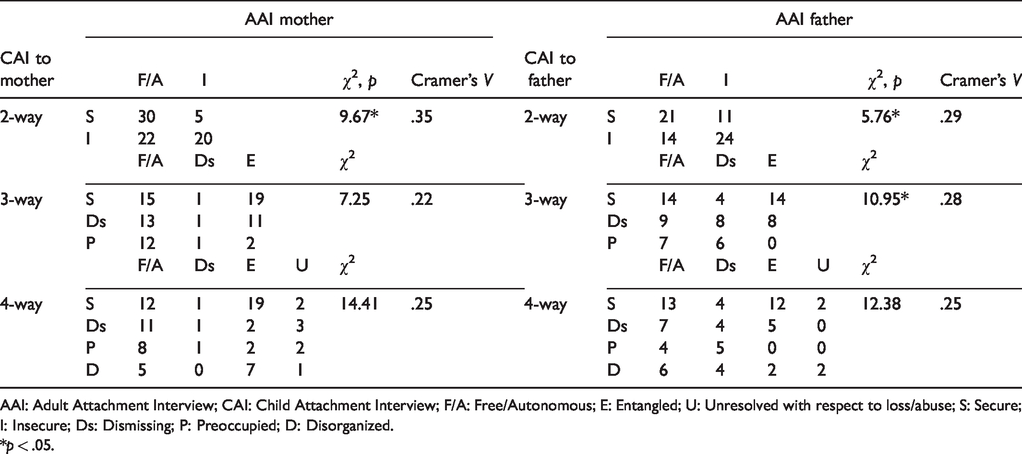
AAI: Adult Attachment Interview; CAI: Child Attachment Interview; F/A: Free/Autonomous; E: Entangled; U: Unresolved with respect to loss/abuse; S: Secure; I: Insecure; Ds: Dismissing; P: Preoccupied; D: Disorganized.
*p < .05.
Differences in attachment between normative and clinical groups
This second section considers the normative group and the two specific clinical groups (up until now considered together as a single clinical group) with opposite characteristics in terms of externalizing and internalizing problems.
First, we examined differences between the clinical and nonclinical participants to two-, three-, and four-way classifications and the CAI dimensions. Distributions and chi-square tests are presented in Table 4. As the overall concordance in CAI attachment between mothers and fathers was very high (95.4%, κ = .91 for two-way; 92.1%, κ = .88 for three-way; 90.8%, κ = .87 for four-way), it is not surprising that the general picture of difference appeared to be very similar for both attachment figures.
Distribution of attachment classifications for normative and clinical groups.
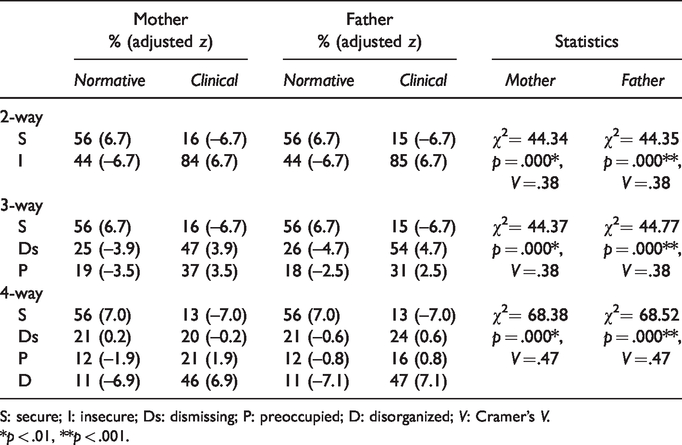
S: secure; I: insecure; Ds: dismissing; P: preoccupied; D: disorganized; V: Cramer’s V.
*p < .01, **p < .001.
The attachment distributions of the two participant groups differed significantly for two-, three-, and four-way classifications (see chi-square tests in Table 4). For the two-way classifications, Secure attachment was prevalent in the normative group (56% of the children were classified as Secure) and by far a minority in the clinical group (only 15% of the children of this group were classified as Secure). Inspection of the z transformed standardized residuals in Table 4 for three-way classifications showed that both the Preoccupied and Dismissing categories contributed significantly (|z| > 2) to this difference. The inclusion of the Disorganized category in the comparison of four-way classifications, however, showed that the difference is chiefly due to a significantly higher presence of this category in the clinical group than in the normative group (for mothers, |z| = 6.9; for fathers, |z| = 7.1). A marginally significant contribution (|z| = 1.9) of the Preoccupied category can also be observed, but for the maternal data only.
CAI mean scale scores for the two groups, as well as t tests, are presented in Table 5. Observed means were fairly high in the normative group on the scales considered to reflect a secure strategy (EO, BAL, UoE, RES, COH), ranging from 4.72 to 4.82, and low on the scales considered as possible indices of insecure attachment (IA-M/F, ID-M/F, DS-M/F), ranging from 2.27 to 2.68. The opposite pattern was apparent in the clinical group. Moreover, the groups differed statistically significantly on all scales (p values from .000 to .021).
Mean differences for CAI scales between the normative and clinical samples.
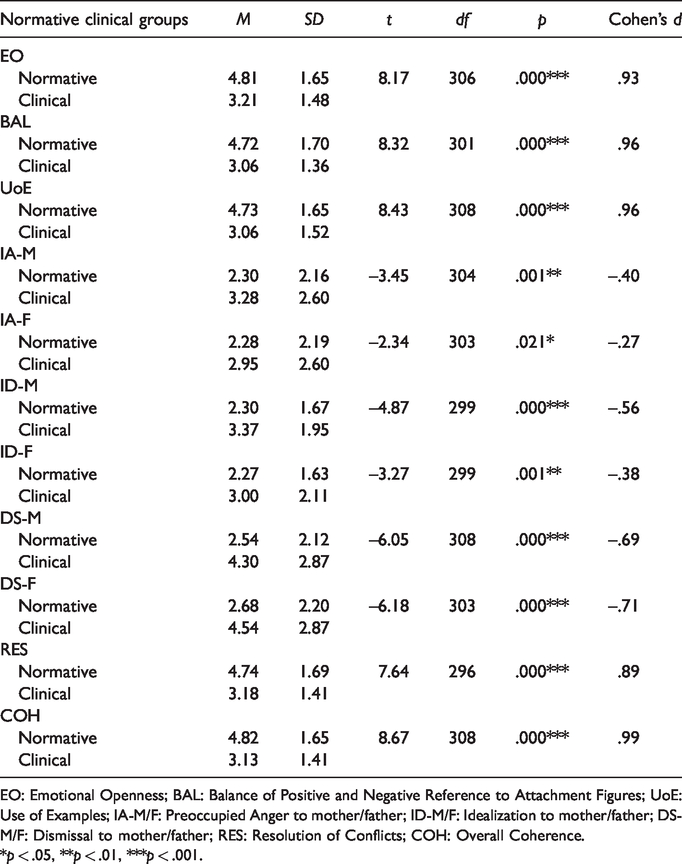
EO: Emotional Openness; BAL: Balance of Positive and Negative Reference to Attachment Figures; UoE: Use of Examples; IA-M/F: Preoccupied Anger to mother/father; ID-M/F: Idealization to mother/father; DS-M/F: Dismissal to mother/father; RES: Resolution of Conflicts; COH: Overall Coherence.
*p < .05, **p < .01, ***p < .001.
Table 6 presents the correlations between the CAI scales. Most correlations were as expected, with high correlations apparent between scores on the same scales for mothers and fathers. Most children in both groups showed the same pattern of attachment with both of their parents.
Correlation matrix for Child Attachment Interview scales for normative group above the diagonal (N = 213) and clinical group below the diagonal (N = 98).

EO: Emotional Openness; BAL: Balance of Positive and Negative Reference to Attachment Figures; UoE: Use of Examples; IA-M/F: Preoccupied Anger to mother/father; ID-M/F: Idealization to mother/father; DS-M/F: Dismissal to mother/father; RES: Resolution of Conflicts; COH: Overall Coherence.
*p < .05, **p < .01.
Differences in attachment between DBD and SSD groups
Comparing the two clinical groups, the distribution of attachment patterns in the DBD group for two-way classifications revealed a high prevalence of Insecure classifications for both mothers (83%) and fathers (85%) of DBD children. With three-way classifications, Dismissing was the dominant strategy with both mothers and fathers (57% and 68%, respectively) of DBD children, while the Preoccupied strategy was more prevalent with mothers than with fathers (26% and 17%, respectively). Fifty percent of DBD children were coded as having a Disorganized pattern of attachment with at least one parent when four-way classifications were considered. Turning to the SSD group, two-way classifications here too revealed a high prevalence of Insecure classifications for both parents (85%); with three-way classifications, Dismissing attachment to mothers was found in 40% of SSD children and to fathers in 43% of SSD children, while Preoccupied attachment to mothers was found in 45% of SSD children and to fathers in 43% of SSD children; and finally, for four-way classifications, 43% of SSD children were coded as Disorganized with at least one parent. The two clinical groups differed significantly on the three-way classifications with respect to fathers (χ2(2) = 7.67; p = . 022, Cramer’s V = .28), but not to mothers (χ2(2) = 3.93; p = . 140, ns). No significant differences on two-way (mothers χ2(1) = .08, p = .775, ns; fathers χ2(1) = .00, p = .980, ns), and on four-way classifications (mothers χ2(3) = 1.82, p = .611, ns; fathers χ2(3) = 2.28; p = .517, ns) were found.
Finally, the mean CAI scale scores for the DBD and SSD groups are showed in Table 7.The DBD group scored significantly higher than the SSD group on the scales of Dismissal to mothers (t(95) = 2.06, p = .042) with a small effect (d = 0.42) and to fathers (t(92) = 2.66, p = .009) with a medium effect (d = 0.55), while the SSD group scored higher than the DBD group on the scale Preoccupied Anger to fathers (t(92) = –2.82, p = .006) with a medium effect (d = 0.59). Differences on all the other CAI scales failed to reach statistical significance.
Means and standard deviations for Child Attachment Interview scales in DBD and SSD groups.
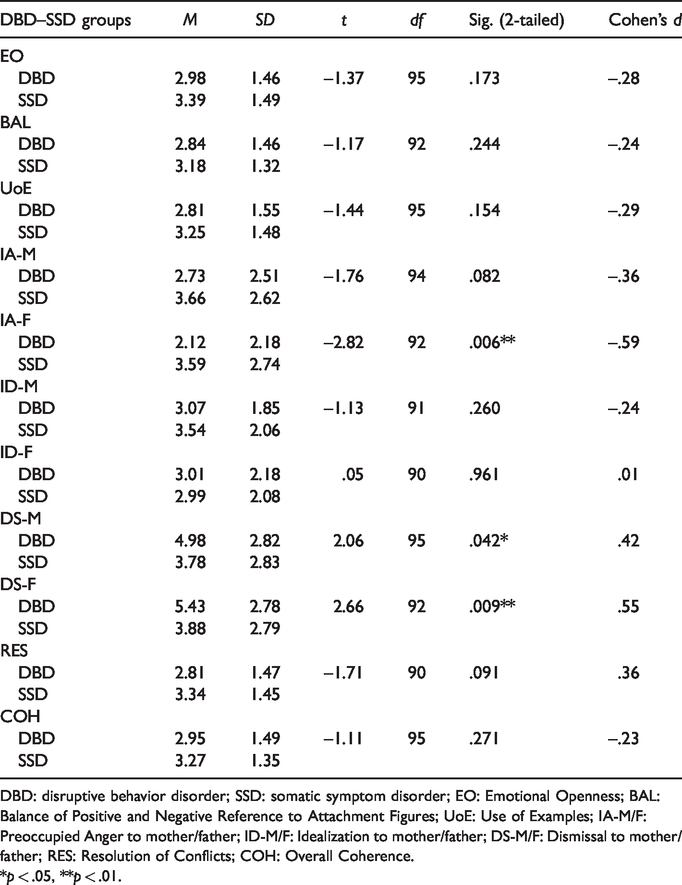
DBD: disruptive behavior disorder; SSD: somatic symptom disorder; EO: Emotional Openness; BAL: Balance of Positive and Negative Reference to Attachment Figures; UoE: Use of Examples; IA-M/F: Preoccupied Anger to mother/father; ID-M/F: Idealization to mother/father; DS-M/F: Dismissal to mother/father; RES: Resolution of Conflicts; COH: Overall Coherence.
*p < .05, **p < .01.
Discussion
Starting from the argument that the study of attachment during school years continues to prove challenging (Bosmans & Kerns, 2015) and that the variety of available measures of attachment lack robust validation (Jewell et al., 2019), this study concerned the cross-cultural adaption of the CAI to an Italian context on the grounds that it appears a particularly promising instrument in this field. Therefore, in line with the first objective of this study, the CAI’s interrater reliability, test–retest reliability, discriminant validity, and convergent validity were investigated.
Our findings on interrater reliability show particularly high agreement between the two expert coders on the CAI classifications and subscales. They are in line with the interrater reliabilities reported by Shmueli-Goetz et al. (2008) in their development and validation study, as well as with those reported by Borelli et al. (2016) and Röder et al. (2015) in subsequent cross-cultural CAI studies, and they are somewhat higher than that reported by Venta et al. (2014). This suggests that despite the CAI being a complex system, trained raters can become reliable coders, and this is not restricted to English-language or UK-based samples.
The data on its test–retest reliability indicate the stability of the CAI’s attachment classifications (from moderate for Disorganization, to very good for the others) and the stability of its scales (exceeding .70) after three months and even a year. This suggests that the CAI is a reliable measurement of the attachment in scholar years regardless of the changes linked with child development. However, the lower stability after 12 months observed for children classified as Disorganized can be explained in part by the difficulty of understanding the configuration of attachment disorganization in middle childhood and early adolescence (Shmueli-Goetz et al., 2008). As Shmueli-Goetz (2014) suggested, during this period, there are critical aspects involved in reliably identifying attachment Disorganization due to the move from a more behavioral to a more representational manifestation of various attachment behaviors. This could represent a critical element in the assessment of Disorganization in general and also in the specific evaluation of tools for assessing Disorganization in school years.
Our findings on discriminant validity show that the CAI is independent of gender and verbal IQ, again in keeping with the findings of Shmueli-Goetz et al. (2008), but not of SES and age. Children classified as Secure were more likely to come from families with higher SES and to be older than their Insecure counterparts. Nevertheless, the psychometric aim of this study did not permit us to establish whether these differences were linked to the sample, related to different modalities of sample recruitment, or attributable to substantial differences between the two sociocultural backgrounds (Cavanna et al., 2018).
The findings on convergent validity demonstrated agreement between CAI and self-reported measures of total perceived attachment security (KSS—Mother, IPPA—father, IPPA—father), trust (IPPA—mother, IPPA—father), communication (IPPA—mother, IPPA—father), and alienation (IPPA—mother, IPPA–—father), as expected. However, these relations were stronger about maternal attachment and in older children, lending further evidence to the aforementioned notion that the CAI may be more accurate in assessing maternal attachment (Venta et al., 2014). Importantly, the Coherence correlated with both self-report measures, suggesting that the coherence subscale may be used to represent overall attachment security to parents. Similarly, EO and RES were associated with higher perceived attachment security to parents. These associations suggest that CAI and other self-report attachment measures assess a similar and overlapping aspect of attachment (Bizzi et al., 2018; Cavanna et al., 2018).
Finally, the correspondence between the attachment classification of children and that of their parents, based on the AAI and previous robust findings of intergenerational consistency in attachment classifications (van IJzendoorn & Bakermans-Kranenburg, 1997), was investigated to test another aspect of the CAI’s convergent validity. In line with Shmueli-Goetz et al. (2008), our data suggest a significant association between AAI parental classifications and their children’s CAI codes (two-way), with a concordance of 65%. Similar results for three-way classification for paternal attachment were also found. This study is the first in which the AAI was administered not only to mothers but also to fathers and the significant transgenerational association observed between the AAI classifications of both parents and their children’s CAI codes indicate convergent validity. The correspondence between adult Unresolved codes and the Disorganized classification of CAI narratives deserves further exploration. In our sample, most parents with Unresolved classifications had children who were not coded as Disorganized. This could suggest a lack of sensitivity in the CAI’s current coding of Disorganization as suggested by Shmueli-Goetz et al. (2008).
The second objective of this study was to compare—in terms of both CAI categories and CAI dimensions—the attachment patterns of a normative (nonclinical) group and a clinical group made up of the specific clinical disorders DBD and SSD—having opposite characteristics in terms of externalizing and internalizing problems, respectively. Starting with a comparison between the normative group and the clinical group (DBD and SSD combined), our findings confirm that the CAI can discriminate between children drawn from a clinical sample and those drawn from a normative group, to both scale scores and attachment classifications. This supports the use of CAI in the clinical context as an assessment measure of attachment in the school years. Besides, within each group, similar classifications of attachment to mothers and fathers (exceeding 90% agreement) were found, suggesting the integration of these representations into a unitary, overarching current state of mind from middle childhood (Bizzi et al., 2018; Shmueli-Goetz et al., 2008).
No other Italian data are currently available to compare attachment distribution during middle childhood and early adolescence; however, these findings are in line with those reported in the Italian meta-analysis by Cassibba et al. (2013) albeit conducted on different developmental periods (Italian infants and adolescents). Conversely, concerning findings reported by other CAI validation studies (Röder et al., 2015; Shmueli-Goetz et al., 2008), we found lower frequencies of Dismissing attachment and higher frequencies of Preoccupied attachment in our normative Italian sample. However, these differences may reflect cultural differences between the samples, underscoring the fact that Italian childrearing is less individualistic and more focused on the child–caregiver relationship (Cassibba et al., 2013).
Comparing our clinical findings with those reported in other CAI studies on clinical samples, there is considerable divergence in the frequency of Disorganized attachment: it appears to be overrepresented in our study, where it exceeds 46%, compared with the 9% found by Shmueli-Goetz et al. (2008) and 17% reported by Venta et al. (2014). Although this datum underlines the essential role of Disorganized attachment for understanding the child psychiatric problems, the larger proportion of Disorganized cases in the present sample may be related to the more severe clinical status of our young patients, who were evaluated during their hospitalization rather than at the posthospitalization stage when they would have received psychiatric medication (Venta et al., 2014).
Comparisons between DBD and SSD show that these two opposing manifestations of childhood conditions (externalizing and internalizing problems) differed on three-way classifications only with respect to fathers (categorical approach) and on several scales associated with Insecure attachment (dimensional approach): the DBD group scored significantly higher on the scales of Dismissal to fathers, while the SSD group scored higher on scales of Preoccupied Anger to fathers. This highlights that these two opposing manifestations of childhood conditions have opposite features also to the attachment perspective. The prevalence of a Dismissing strategy in DBD children, which is in line with the literature (e.g., Fearon & Belsky, 2011), as well as the prevalence of a Preoccupied strategy in SSD, even though it is mainly documented in adulthood (Noyes et al., 2003; Schmidt et al., 2002; Wearden et al., 2006), might be explained by the fact that children with these clinical conditions often show representations of the attachment figures as being unavailable and/or unpredictable and strategies to cope with these experiences. Nevertheless, it is noteworthy that the difference was only significant to the attachment to fathers. In other words, this highlights the possibility that the father–child attachment relationship could play a key role not only in the child’s adjustment during middle childhood and early adolescence (Bosmans & Kerns, 2015) but also in understanding specific child psychopathologies of varying etiology and trajectory (Rasmussen et al., 2019). For this reason, because it captures information about the current availability and responsiveness of mother and father separately as perceived by the child, the CAI has great utility in a clinical context.
In conclusion, the innovative study presented here opens up the possibility of further valuable research assessing attachment patterns in specific psychopathological conditions that affect children during middle childhood and early adolescence. This phase of life is one in which young people can be more vulnerable, and attachment could be key to better understanding the onset of clinical manifestations. The clinical implications of focusing on this stage could be particularly important in terms of improving attachment-based intervention programs for more vulnerable populations. An example of this are the video feedback (Steele et al., 2014) an attachment-based intervention focused on infants and young children, the Circle of Security (Marvin et al., 2002) an attachment-based intervention focused on the promotion of the parental sensitivity, and the Connect (Moretti et al., 2009) an attachment program to help parents of teens with serious behavior problems. Moreover, the use of CAI with other clinical conditions, applying it not only as an assessment tool but in the evaluation of therapeutic outcomes, should enrich future research.
Although there are several strengths to this study, we also recognize its limitations. The follow-up (three months and one year), convergent and discriminant validities of this study did not include participants from clinical groups. Therefore, results cannot be generalized outside of healthy populations. Future researchers should fill this gap. In addition, this study includes the assignment of attachment classifications to only two attachment figures per child and not to additional caregivers. To our knowledge, additional relationships can be of great importance to adolescents and therefore warrant further attention (Venta et al., 2014).
In conclusion, we argue that the CAI can be used as a tool to assess attachment in middle childhood and adolescence for research purposes in Italian samples. This measure also represents a very useful tool for clinicians, in terms of providing information on children’s experience, family relationships, and parents’ availability in school years. It may also have crucial utility in the assessment process, the design of interventions for populations at risk, and the evaluation of child psychotherapy and child custody. Moreover, the role of attachment in the process of psychological treatment for children and adolescents is underresearched, and the development of psychometrically sound measures will help to advance understanding in this area (Jewell et al., 2019).
Ethical considerations
All procedures performed in studies involving human participants were following the ethical standards of the institutional and/or national research committee of the University of Genoa, of the Gaslini Hospital (Genoa, Italy), and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent was obtained from all individual participants included in the study. Parents completed consent forms, and children completed assent forms.