
Abstract
While research tends to focus on understanding risk factors associated with adverse childhood and adolescent experiences, there is growing empirical support within the field of human services to also focus on strengths and protective factors that bolster resilience in life. This study investigated the psychometrics of the Resilience Protective Factors Checklist (RPFC), which is a questionnaire that assists in the identification of protective factors empirically linked to resilience and positive outcomes. In addition, associations between protective factors, childhood adversity, and quality of life outcomes were examined. Participants were undergraduate college students (n = 1,256). The results revealed good psychometric properties for the RPFC and the factor analysis supported the resilience structural model of three interrelated areas of protective factors - Individual, Family, and Community influences. All three areas of protection were positively correlated with all four domains of positive life outcomes (physical health, psychological health, social relationships, and a healthy environment) and negatively correlated with adverse childhood experiences. RPFC’s individual protective factors positively predicted physical health and psychological health outcomes, while the community protective factors positively predicted environmental health outcomes. In addition, the RPFC’s family protective factors moderated the path between adverse childhood experiences and social relationships. That is, for individuals who have experienced more adverse childhood experiences, those with higher levels of RPFC family protective factors had positive social relationship outcomes, while those with lower levels of family protective factors had negative social relationship outcomes. These findings lend support for the utilization of assessment measures for identifying and promoting protective factors that can buffer life adversity and heighten resilient positive outcomes.
Keywords
Introduction
The field of mental health and criminal justice has historically placed a strong emphasis on targeting problem behaviors and risk factors linked to recidivism and negative outcomes (Andrews et al., 1990; Rogers, 2000; Seligman & Csikszentmihalyi, 2000). In more recent years, this emphasis has expanded to investigate negative outcomes associated with adverse childhood experiences (ACE; Anda & Felitti, 2003). The deleterious effects of ACEs on psychological, behavioral, academic, physical, and neurological functioning are well established (Baglivio et al., 2014; Craig et al., 2017; Danese & McEwen, 2012; Flaherty, et al., 2013; Fox et al., 2015; National Children’s Advocacy Center, 2011; Sciaraffa et al., 2018). However, there is also a substantial proportion of people who respond to ACEs and other risk factors in adaptive, resilient ways. The field is gaining more knowledge about these resilient responses and the specific variables (protective factors) that appear to help buffer life stressors and enhance the capacity to cope in adaptive ways (Domhardt et al., 2015; Farrington et al., 2016; Jolliffe et al., 2016; Langton & Worling, 2015; Perez-Gonzalez et al., 2017). There is growing support within human services to not only attend to problems and risks, but also embrace a strengths-based orientation that incorporates variables that can prevent and mitigate problems of childhood adversity, as well as promote positive life outcomes (Edwards et al., 2017; Powell, 2015). The constructs of ‘resilience’ and ‘protective factors’ are part of this strengths-based movement.
Defining resilience and protective factors
Resilience and the interrelated protective factors are a multidimensional, dynamic process. Windle (2011) defines resilience as “the process of effectively negotiating, adapting to, or managing significant sources of stress or trauma”. The second sentence in Windle’s description provides a definition of protective factors, “Assets and resources within the individual, their life, and environment that facilitate the capacity for adaptation and ‘bouncing back’ in the face of adversity”. An ecologically-based exploration of protective factors is required due to the heterogeneity of protections that include both external resources (from the person’s family and community) and internal attributes within the person. Some of these factors lead to positive outcomes by mitigating the effects of a particular risk factor or life stressor (an interaction effect in statistical models), while others have been found to promote positive outcomes regardless of risks that are present (a main effect in statistical models and often referred to as ‘assets’). Additionally, some factors can have both protective and promotive effects (Losel & Farrington, 2012). An in-depth investigation of the directional effects (protective vs. promotive influences) of protective factors is beyond the scope of this study. For the purpose of this study we will use the term ‘protective factors’ in a broad sense to investigate individual traits, family influences, and community variables that are associated with ‘resilience’ per self-report of childhood adversity and quality of life.
Development of the RPFC:
Investigating protective factors linked to resilience is an important area of study due to the growing evidence for many influential protections derived from individual, family, and community resources (Moses & Villodas, 2017; Woods-Jaeger et al., 2018). The Resilience Protective Factors Checklist (RPFC) is a strengths-based questionnaire that was developed and utilized as a clinical tool by the first author during two decades of work in a maximum-security detention center serving adolescents, young adults, and their families. The clinical utility of the RPFC has been evident over the years, in regard to positively engaging at-risk (at-promise) clients and their families in treatment services. Rather than focusing on what is ‘wrong’ with clients or their families, the RPFC provides opportunities to look at what is ‘right’ with them by identifying, developing, and strengthening protective factors linked to resilient positive outcomes.
The initial selection and early revisions of the RPFC items were based on empirically-supported protective factors (individual, family, and community influences) linked to resilience that had been summarized in the literature (Masten & Coatsworth, 1998; Masten et al., 2009; Masten & Reed, 2002). Over the past two decades, additional items have been added to the RPFC based on contemporary research, including a post-traumatic growth item (Collier, 2016; Meyerson et al., 2011; Schaefer et al., 2018; Seery et al., 2013) a physical exercise item (e.g., Ahn & Fedewa, 2011; Emerson et al., 2009; Otto & Smits, 2011; Weir, 2011), an internal motivation item (Karver et al., 2006; Miller & Rollnick, 2002; Walters et al., 2007) and a psychological-mindedness, problem-solving item (Nyklicek et al., 2010; Roxas & Glenwick, 2014). The wording of the RPFC items were modified over time based on feedback from youth, as well as the mental health professionals administering the RPFC. The RPFC items use basic language that require a sixth-grade reading level. While there are other commendable measures investigating protective factors associated with resilience, including some with a strong emphasis on internal, individual traits (e.g., Connor & Davidson, 2003; Prince-Embury, 2007) and other measures with an emphasis on cultural and community connections (e.g., Ungar & Liebenberg, 2011), this study investigates a new measure, the RPFC, which provides a more comprehensive ecologically-based exploration of protective factors. The content of the RPFC adds to the currently available assessment measures in several ways including its balanced emphasis on assessing individual, family, and community protective factors linked to resilient, positive outcomes. The ‘individual’ protective factors assess a broad range of variables including problem-solving skills, self-regulation, positive self-perception, talents, self-efficacy (hope), sense of meaning in life, positive outlook on life, post-traumatic growth, internal motivation, and physical exercise. In addition, the ‘family’ and ‘community’ protective factors assess much more than just whether a person ‘feels connected’ to their family and community/culture. The RPFC explores the utilization of authoritative parenting strategies (e.g., providing structure, rules, and supervision; regular communication and providing an explanation/rationale for rules and limits; believing in your child and having positive expectations for their future); the protective influence of safe, predictable homes and neighborhoods; parental involvement in their child’s schooling and parental commitment to the value of education; and the influence of community-based factors, such as positive friends, positive romantic partners, positive activities, and enrollment in safe, supportive schools.
Purpose of study
The purpose of this study was twofold. First, to begin the process of assessing the psychometric properties of the Resilience Protective Factors Checklist (RPFC; Powell, 2015). The RPFC is a clinical tool used to assess the presence of protective factors empirically linked to resilience and positive outcomes. The second objective for this study was to provide initial evidence of validity by exploring associations between the RPFC’s protective factors (individual, family, and community factors) and important variables impacted by protective factors, including ACEs and quality of life outcomes. A comparison with another protective factor measure was also conducted. Based on previous research on protective factors, we hypothesized that items of the RPFC would load onto three factors representing individual traits, family dynamics, and community resources. We also hypothesized that RPFC scores would positively correlate with other measures of protective factors and negatively correlate with ACES. Lastly, we hypothesized that RPFC scores would positively predict quality of life outcomes and moderate the relation between ACES and quality of life outcomes.
Methods
Participants and procedures
Participants were undergraduate students who completed a battery of questionnaires, including the RPFC, in exchange for class credit as part of a larger study on personality and health risk behaviors. Participants were provided with informed consent and debriefing information and completed the online surveys in a lab with private cubicles to ensure confidentiality. Participants in the total sample were 1256 college students (40.7% female, M age = 19.36) from a local university in the Western United States. In addition to completing the RPFC, 535 participants (M age = 19.71) of the total 1256 participants completed other measures to assess convergent and predictive validity. Full descriptive data about the sample is presented in Table 1.
Participant demographics.
Measures
Resilience Protective Factors Checklist (RPFC) Scale
The Resilience Protective Factors Checklist (RPFC; Powell, 2015) is a 25-item questionnaire that assesses what strengths and resources (i.e., protective factors) are available to a person. The RPFC content explores three areas of protection: individual, family, and community protective factors. Each RPFC protective factor is assessed by jargon-free single items, which allow respondents to rate how true each item is in their lives using a 4-point Likert-type rating scale (1 = Not True, 2 = Sometimes True, 3 = Often True, 4 = Almost Always True). For example, item #5 assesses self-efficacy and internal hope (which is an individual protective factor) by asking the question, “I believe I can influence what happens in my life with my decisions and actions”, and Item #11 assesses the family protective factor of having a close relationship with a competent, prosocial family member by asking, “I have a positive family member who gives me support in good and bad times (i.e., parent, grandparent, aunt, uncle, older sibling)”.
Other measures
The Resilience Research Centre Adult Resilience Measure (RRC-ARM; Ungar, 2016; Ungar & Liebenberg, 2011) is a 28-item screening tool designed to measure the resources available to individuals that may bolster resilience. The RRC-ARM is the adult version of the Child and Youth Resilience Measure (CYRM) and was used due to the age of the participants in this study. The RRC-ARM includes three subscales comprised of Individual (α = .87), Relationship with Primary Caregiver (α = .81), and Context/Belonging (α = .80). Reported alphas were calculated with the current sample. Participants responded to 11 items on the ‘Individual’ subscale (e.g., “I cooperate with people around me”), 7 items on the ‘Relationship with Primary Caregiver’ subscale (e.g., “My family has usually supported me through life”), and 10 items on the ‘Context/Belonging’ subscale (e.g., “Spiritual beliefs are a source of strength for me”). The version of the RRC-ARM used for this study included a 5-point response scale (1 = Not at All, 2 = A Little, 3 = Somewhat, 4 = Quite a Bit, 5 = A Lot).
Positive life outcomes were measured using the World Health Organization Quality of Life-Brief (WHOQOL-BREF; WHO, 1996), which is a 26-item questionnaire that assesses an individual’s perceived quality of life. This measure defines quality of life as “individuals’ perceptions of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns”. This questionnaire derives four domain scores using 24 of the 26 items associated with quality of life as it relates to Physical Health (α = .79), Psychological Health (α = .85), Social Relationships (α = .64), and Environment (α = .77). Reported alphas were calculated with the current sample. Participants responded to 7 items on ‘Physical Health’ (e.g., “To what extent do you feel that physical pain prevents you from doing what you need to do?”), 6 items on ‘Psychological Health’ (e.g., “How much do you enjoy life?”), 3 items on ‘Social Relationships’ (e.g., “How satisfied are you with your personal relationships?), and 8 items on ‘Environment’ (e.g., “How safe do you feel in your daily life?”). The WHOQOL-BREF uses a 5-point Likert-type scale and depending on the wording of the question, the response scale was modified and included (1 = Very Dissatisfied, 2 = Dissatisfied, 3 = Neither Satisfied nor Dissatisfied, 4 = Satisfied, 5 = Very Satisfied); (1 = Very Poor, 2 = Poor, 3 = Neither Poor nor Good, 4 = Good, 5 = Very Good); (1 = Not at all, 2 = A Little, 3 = A Moderate Amount, 4 = Very Much, 5 = An Extreme Amount); (1 = Not at all, 2 = A Little, 3 = Moderately, 4 = Mostly, 5 = Completely); or (1 = Never, 2 = Seldom, 3 = Quite Often, 4 = Very Often, 5 = Always).
The Adverse Childhood Experiences Scale (ACES; Felitti, et al.,1998) is a 10-item questionnaire that assesses an individual’s childhood (during their first 18 years of life) exposure to multiple types of abuse, neglect, domestic violence, and other household stressors including substance abuse, parental divorce or separation, and parental mental illness. Participants responded to items such as, “Did a parent or other adult in the household often or very often … Swear at you, insult you, put you down, or humiliate you? or Act in a way that made you afraid that you might be physically hurt?” and “Did a household member go to prison?” The ACES uses a yes-no response format (α = .66). The reported alpha was calculated with the current sample.
Analysis
Exploratory factor analysis
The total sample (N = 1256) was randomly split into two halves, one for exploratory factor analysis (EFA) and one for confirmatory factor analysis (CFA). Using the EFA sample, descriptive statistics were calculated for all items of the RPFC using SPSS version 26 (IBM Corp, 2019).
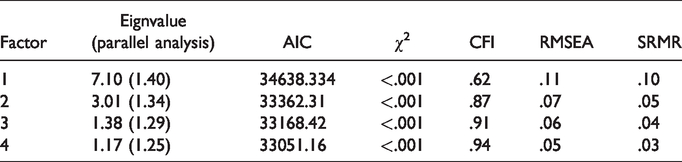
An EFA was conducted to identify the factor structure of the RPFC using Mplus Version 8 (Muthén & Muthén,1998–2019). Factors were rotated with Geomin rotation. Because we hypothesized 3 factors in the model, we ran models with 1- through 4- factors. Using Mplus to conduct the EFA allowed us to examine eigenvalues, parallel analysis, and multiple indices of model fit in order to identify the number of factors that are best represented by the data. Several indices of model fit were examined. One model fit index, the chi-square (χ2) statistic, indicates if the proposed model deviates from the model reflected by the data, with non-significant values indicating the specified model does not significantly differ from the model presented by the data (Ullman, 2013). However, the χ2 is sensitive to sample size, showing significant misfit when sample sizes are large and differences are small, as is the case herein. Thus, other indices were used to examine model fit. The AIC is an index of relative fit, with values closer to 0 indicating improvement in fit. Comparative fit index (CFI) values range from 0 to 1; better fit is indicated by scores closer to 1, with good fit indicated by scores greater than .90 and excellent fit by scores greater than .95 (Hu & Bentler, 1999; Ullman, 2013). Root mean squared error of approximation (RMSEA) values range from 0 to 1, with good fit indicated by scores less than .10 and excellent fit indicated by scores less than .06 (Hu & Bentler, 1999; Ullman, 2013). Lastly, standardized root mean square residual (SRMR) values range from 0 to 1, with adequate fit indicated by scores less than .08 and good fit indicated by scores less than .05 (Hu & Bentler, 1999; Iacobucci, 2010).
After determining the factor structure, we examined the Geomin rotated loadings to identify which items significantly loaded onto the identified subscales (Please Note: to avoid confusion about the term “factors”, and confusion with the items measuring protective factors, we will refer to the three model factors as “subscales”). Items were considered to load onto a subscale if their Geomin loadings were at least .40. Items were considered for omission if they did not have a factor loading of at least .40 or if they cross-loaded onto another factor with a factor loading of .20 or greater.
Confirmatory factor analysis
A confirmatory factor analysis (CFA) was conducted after identifying the number of subscales present in the model and trimming items with poor psychometric properties. The CFA was conducted with the second random half of the total sample using Mplus Version 8 (Muthén & Muthén, 1998–2019) and the Maximum Likelihood estimation method. Similar to the EFA, conducting the CFA in Mplus generated multiple indices of model fit, including the χ2, CFI, RMSEA, and SRMR. After confirming the model identified by the EFA, we calculated Cronbach’s α for each factor.
Initial validity evaluation
After confirming the model, we assessed initial evidence of convergent, discriminative, and predictive validity of the RPFC. A subsample (N = 535) of the total sample completed measures related to protective factors, positive life outcomes, and adverse experiences. For convergent validity, we ran correlations between the three subscales of the RPFC and the subscales of the RRC-ARM. For discriminant validity, we ran correlations between subscales of the RPFC and the ACES. We assessed initial evidence of predictive validity by first examining relations among ACES total scores, RPFC subscales, WHO-BREF subscales, and key demographic variables (age, sex, gender, race, and ethnicity). Correlations were examined among Age, ACES, RPFC subscales, and WHOQOL-BREF subscales using Mplus version 8 (Muthén & Muthén,1998–2019). The demographic variables sex, gender, ethnicity, and race were dummy coded for analysis and entered as categorical variables. After examining correlations among variables, we conducted a path analysis with ACES total score entered as an observed exogenous variable, each of the WHOQOL-BREF subscale scores entered as observed endogenous variables, and each RPFC subscale total score entered as observed moderating variables. We controlled for participants’ age, sex, gender, race, and ethnicity, with nominal variables dummy coded. We elected to enter sex and gender into the model as separate variables to account for differences between individuals’ self-reported biological sex and gender identities. The path analysis allowed us to examine direct paths between ACES and each WHOQOL-BREF subscale, between each RPFC subscale and each WHOQOL-BREF subscale, and any moderating effects of RPFC subscales on the relation between ACES and WHOQOL-BREF. Because we were primarily interested in these paths for individuals who had experienced adverse childhood experiences, analysis was conducted with a subsample of individuals who had ACES scores equal-to-or-greater than 1. The final model was identified after trimming non-significant paths between RPFC and WHOQOL-BREF subscales that were theoretically justified. Multiple indices of model fit (AIC, CFI, RMSEA, and SRMR) were examined.
Results
Scale development of the RPFC
Exploratory factor analysis
The initial review of the item statistics indicated high skew and kurtosis on the items “I have a parent/caregiver who thinks education is important” and “I have a parent/caregiver who believes in me and expects me to do well in life” (see Table 3). Because it is likely that the kurtosis evident in these two items is an effect of the college-student sample, we elected to retain these items in the EFA. The hypothesized model structure for the RPFC, which is categorized into three subscales of protection (Individual Factors, Family Factors, & Community Factors) was identified in the EFA. Specifically, a review of the eigenvalues and parallel analysis indicated a 3-factor solution. Further, multiple indices of model fit indicated a 3-factor model fit better than the 1- and 2- factor models (see Table 2). Examination of the Geomin rotated loadings indicated most items loaded onto each subscale as hypothesized, with the exception of two items (“regular use of physical exercise” and “having a positive boyfriend or girlfriend who supports me and stays out of trouble”), which did not load onto subscales at or above the .40 threshold and had similar factor loadings across two subscales (see Table 3). Also, the item “I have positive activities I like to do” fit better in the ‘individual subscale’ rather than the ‘community subscale’. Lastly, the item “I have religious beliefs/spirituality that give me support and help me make decisions” had a factor loading of .32. Because this item did not cross-load onto other subscales and literature suggests that religious or spiritual practices or beliefs are empirically tied to resilience, we elected to retain this item for the CFA.
Parallel analysis and model fit indices for the RPFC EFA.
RPFC item statistics and exploratory factor analysis.
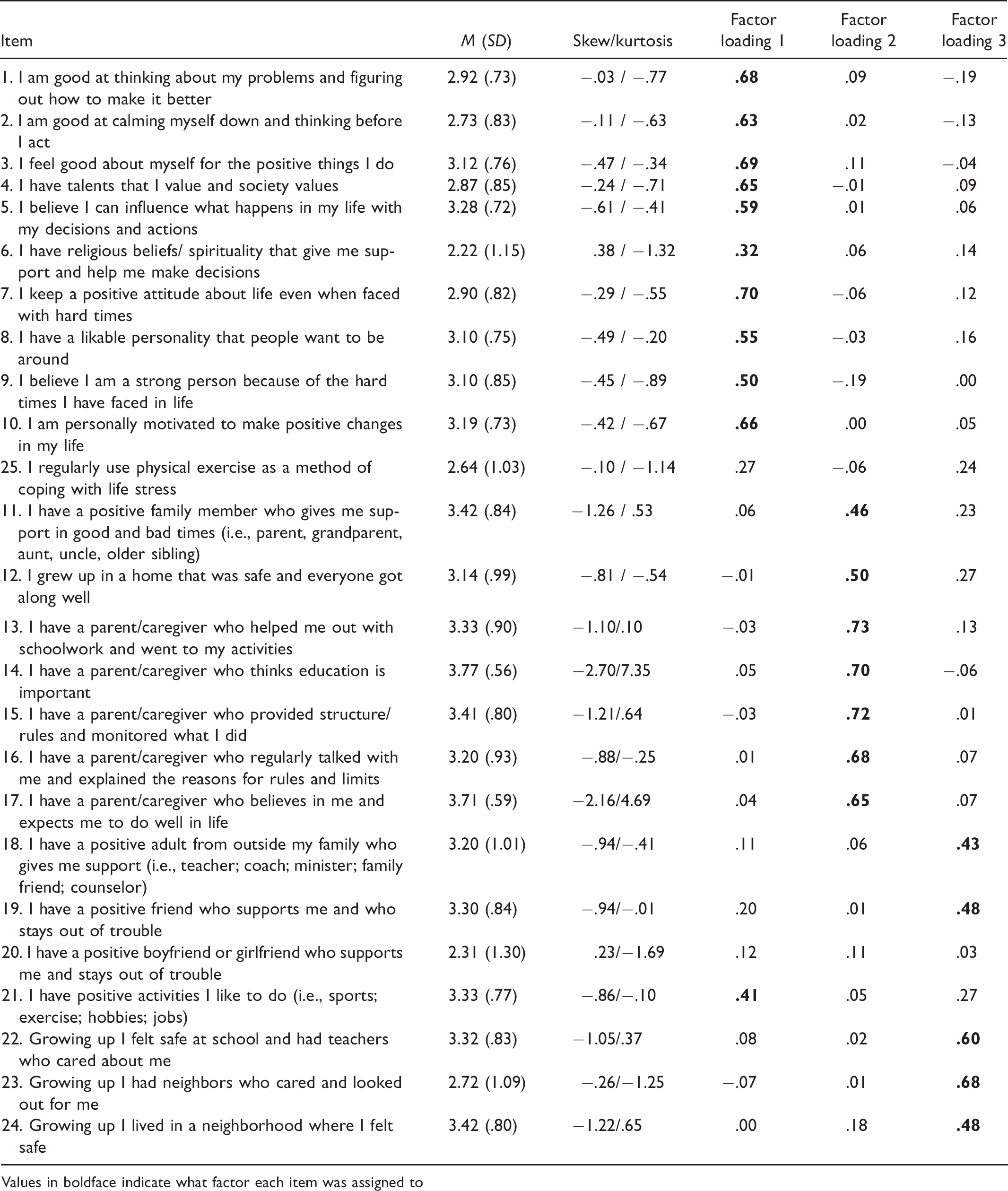
Values in boldface indicate what factor each item was assigned to
Confirmatory factor analysis
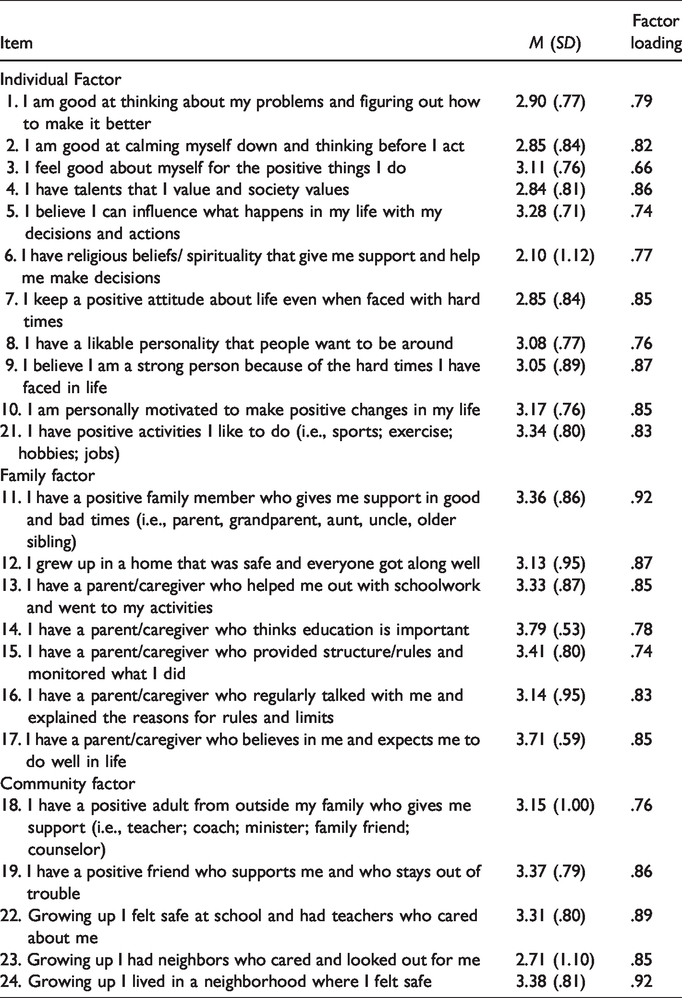
We conducted a CFA with the second half of the randomly split sample after removing the two questions described above (“regular use of exercise” & “having a positive boyfriend/girlfriend/partner”) and moving the “positive activities” item to the Individual Factors category. Similar to the EFA, several indices of model fit were examined and indicated good fit (χ2 < .001; CFI = .95; RMSEA = .08; SRMR = .03). All items’ standardized factor loadings were acceptable. The final version of the RPFC with factor loadings is presented in Table 4. The internal consistencies of the three subscales were evaluated using Cronbach’s alpha. Across all three factors, good internal consistency was indicated (Individual = .85; Family = .86; and Community = .74).
CFA standardized item factor loadings of the final RPFC.
Initial validity evaluation
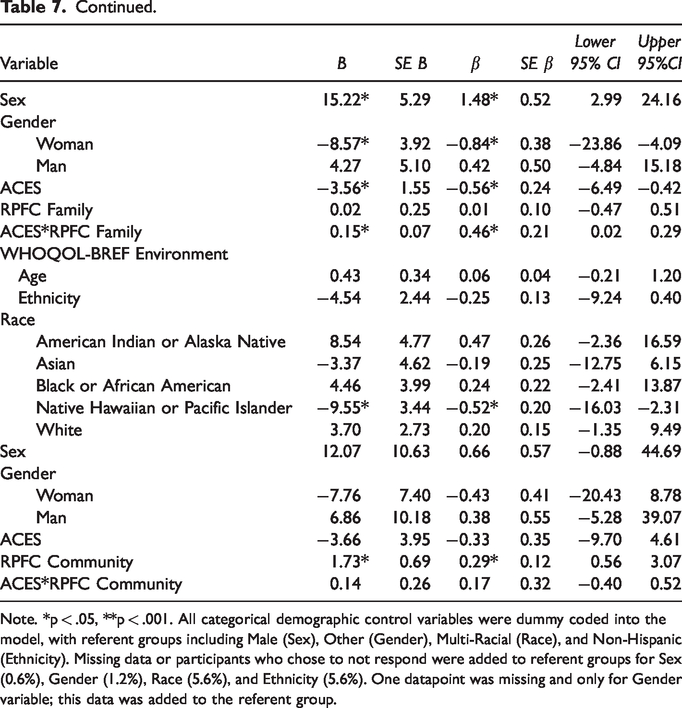
Convergent validity of the RPFC was assessed using the RRC-ARM. Each of the RPFC subscales (Individual, Family, and Community) were significantly and positively correlated with the RRC-ARM scores (Individual, Relationship with Primary Caregiver, and Context/Belonging), indicating initial evidence of convergent validity. Regarding discriminant validity, each of the three RPFC subscales were significantly negatively correlated with the ACES total score. Results of these correlations are presented in Table 5. For the evaluation of predictive validity, we first examined associations among demographic variables (with categorical variables dummy coded), ACES, RPFC subscales, and WHOQOL-BREF subscales, as presented in Table 6. The associations between the ACES and all RPFC subscales and between the ACES and all WHOQOL-BREF subscales were significant and negative, and associations between all RPFC subscales and WHOQOL-BREF subscales were significant and positive. The final path model is depicted in Figure 1 and included the ACES total score entered as an exogenous variable and WHOQOL-BREF subscales entered as endogenous variables. The WHOQOL-BREF subscales were correlated with each other. The RPFC Individual subscale was entered as moderating the paths between ACES and WHOQOL-BREF Physical Health and ACES and WHOQOL-BREF Psychological Health; the RPFC Family subscale was entered as moderating the path between ACES and WHOQOL-BREF Social Relations; and the RPFC Community subscale as moderating the path between ACES and WHOQOL-BREF Environment. The model controlled for age, sex, gender, race, and ethnicity. Model fit was acceptable (AIC = 10805.06; χ2 = 73.39, p < .001; CFI = .92; RMSEA = .10; SRMR = .07). In the final model, ACES significantly negatively predicted the WHOQOL-BREF Social Relationships subscale, and this path was significantly moderated by the RPFC Family subscale. Specifically, the simple slope for ACES and WHOQOL-BREF Social was -1.35 (SE = .65, p = .04) for individuals at 2 SD below the mean for RPFC Family and 1.22 (SE = .76, p = .11) for individuals at 2 SD above the mean for RPFC Family (see Figure 2). Simple slopes and simple slope tests were calculated using code (Stride et al., 2015) for Mplus. Further, the RPFC Individual subscale significantly positively predicted WHOQOL-BREF Physical Health and Psychological Health subscales, and the RPFC Community subscale positively significantly predicted the WHOQOL-BREF Environment subscale. Results of the final model are presented in Table 7.
Correlations between the RPFC and RRC-ARM and between the RPFC and ACES.
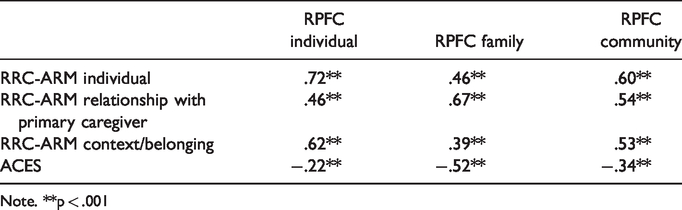
Note. **p < .001
Correlations among demographic controls, ACES, RPFC subscales, and WHOQOL-BREF subscales.

Note. *p < .05, **p < .001. All categorical demographic control variables were dummy coded into the model, with referent groups including Male (Sex), Other (Gender), Multi-Racial (Race), and Non-Hispanic (Ethnicity). Participants who chose to not respond were added to referent groups for Sex (0.6%), Gender (1.2%), Race (5.6%), and Ethnicity (5.6%). One datapoint was missing and only for Gender variable; this data was added to the referent group.
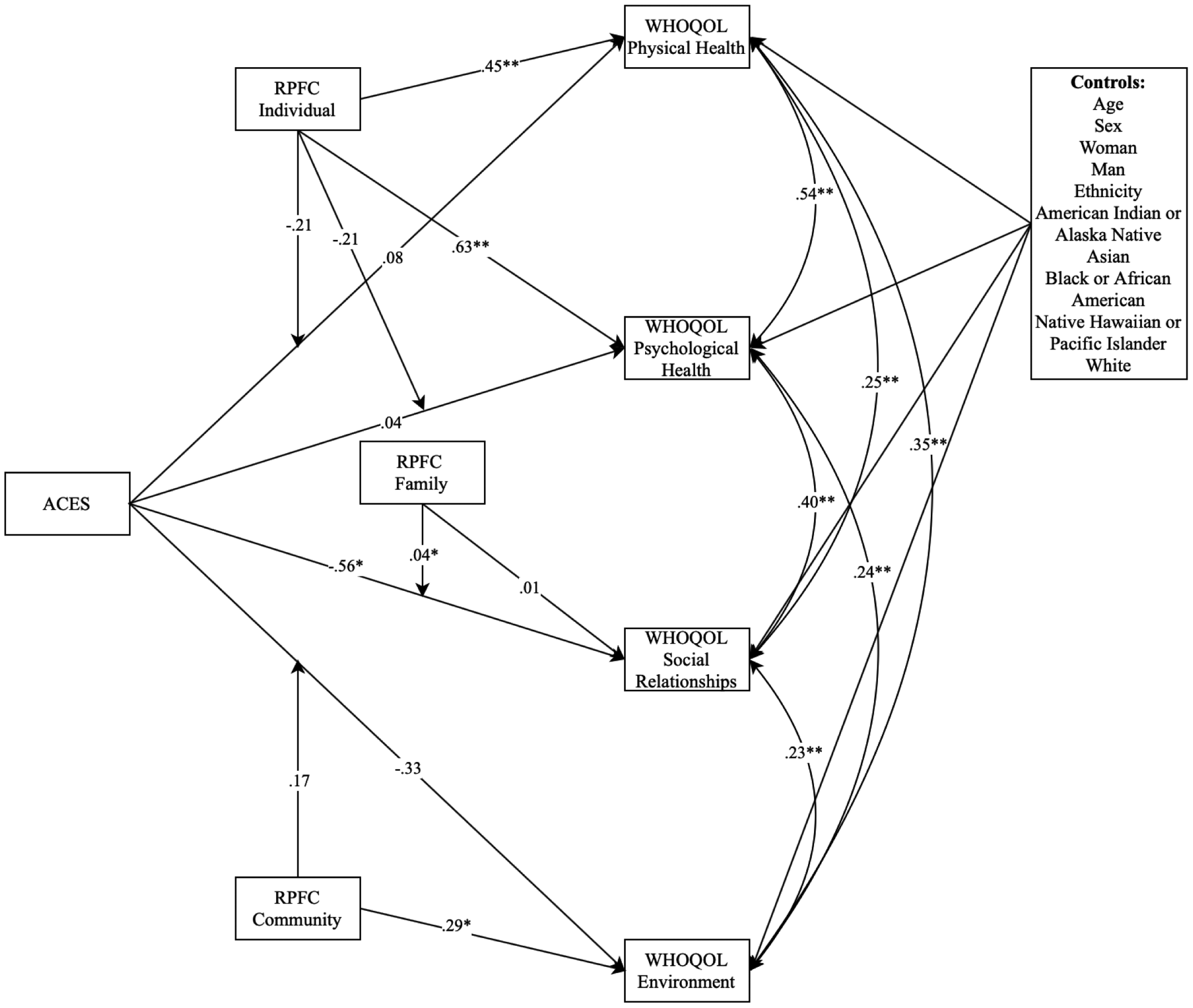
Path analysis of ACES predicting WHOQOL-BREF, RPFC predicting WHOQOL-BREF, and RPFC moderating paths from ACES to WHOQOL-BREF. Note. *p < .05, **p < .001. For ease of interpretation, individual paths and results between control variables and WHOQOL-BREF variables are not represented in this model (see Table 7 for results).
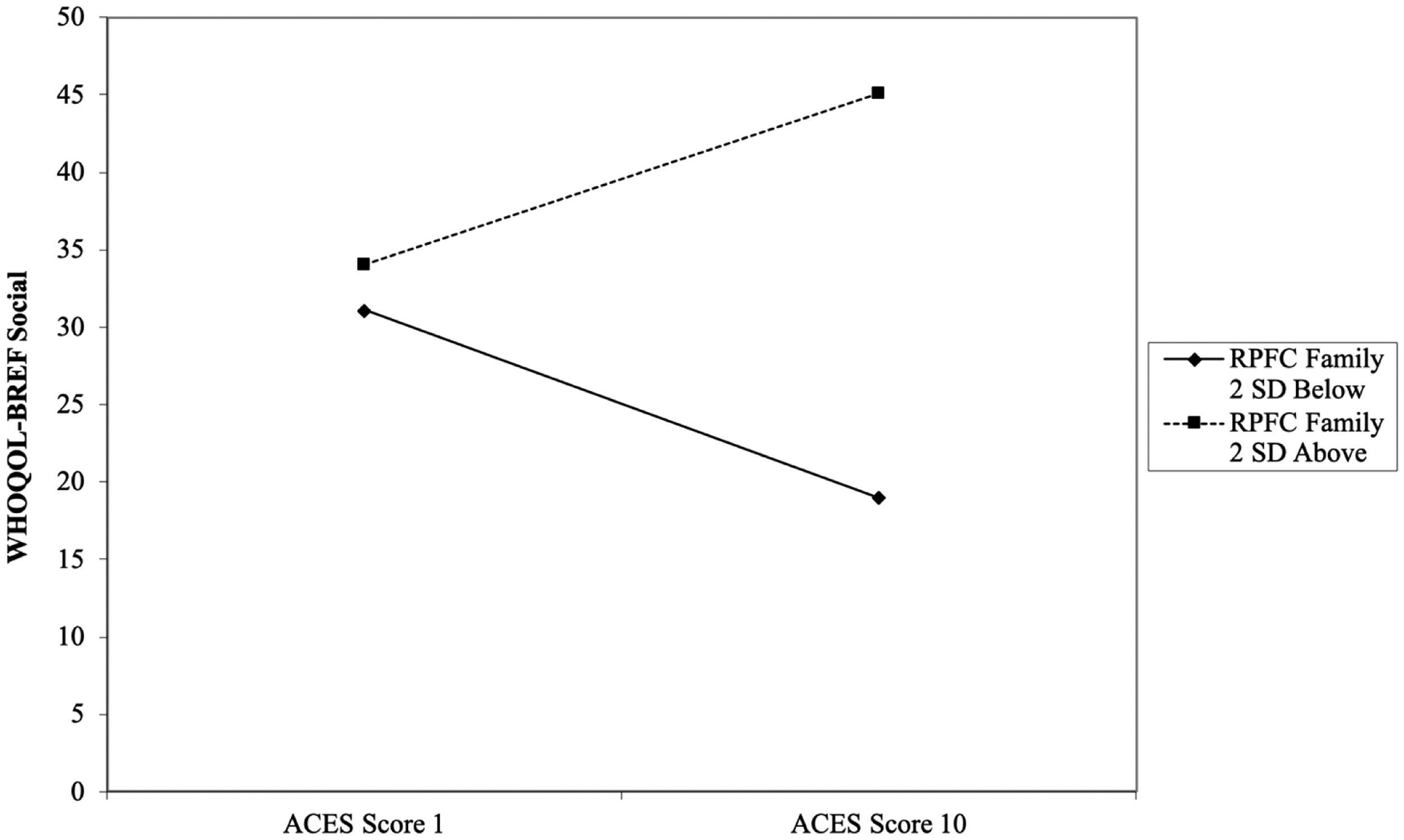
Moderating effect of RPFC family on the relation between ACES and WHOQOL-BREF social.
Path model between ACES and WHOQOL-BREF subscales moderated by RPFC subscales.

Note. *p < .05, **p < .001. All categorical demographic control variables were dummy coded into the model, with referent groups including Male (Sex), Other (Gender), Multi-Racial (Race), and Non-Hispanic (Ethnicity). Missing data or participants who chose to not respond were added to referent groups for Sex (0.6%), Gender (1.2%), Race (5.6%), and Ethnicity (5.6%). One datapoint was missing and only for Gender variable; this data was added to the referent group.
Discussion
This study investigated the psychometrics of the Resilience Protective Factors Checklist (RPFC) and its association with adverse childhood experiences and quality of life outcomes. The RPFC demonstrated good psychometric properties including good internal consistency, good convergent validity relative to another measure of protective factors associated with resilience, and the factor analysis supported the resilience model structure (Luthar et al., 2000) of three main areas of protection - individual, family, and community protective factors. Each of the RPFC subscale scores (the Individual Protective Factor, Family Protective Factor, and Community Protective Factor scores) were significantly positively correlated with each of the four quality of life domains (Physical Health, Psychological Health, Social Relationships, and Environment). This indicated that as participants’ protective factor scores increased, their life quality increased across all four domains. The RPFC results also revealed evidence of discriminant validity with all three subscales being negatively correlated with Adverse Childhood Experiences (ACEs). While this finding is not causal, it is consistent with what would be expected; people who have fewer protective factors are likely to be at higher risk of adverse childhood experiences.
When taking a closer look at the participants who had one or more adverse childhood experience (ACE), there were several notable findings related to RPFC predicting positive life outcomes. Increased individual protective factors predicted more positive life outcomes associated with physical health and psychological health. Increased RPFC community protective factors positively predicted positive life outcomes relating to a healthy living environment. The path analysis also revealed that as ACEs increased, the quality of social relationships declined; however, RPFC family protective factors significantly moderated this relation. That is, the impact of ACEs on social relationships changed from negative to positive at higher scores of RPFC family protective factors. These positive effects for a broad range of protective factors remained strong even when controlling for age, sex, gender, race, and ethnicity.
Several limitations of this study were identified, including the utilization of only self-report measures. Future research investigating the RPFC will benefit from incorporating other measures of adversity and resilience beyond self-report. Another limitation was the homogeneity of the subjects who were all adult-age college students. This subject pool was appropriate for the first steps in validating the RPFC and the subjects represent a potentially resilient group of individuals who have obtained the academic achievement of being accepted and attending a college. Future studies will benefit from the utilization of a broader, heterogenous group of subjects. Future research should include a sample of adults not in college and parents/caregivers, as well as subjects who possess differences in presenting problems, severity of childhood adversity, gender, age, ethnicity, and cultural identity. There is growing awareness of the importance of the looking at the cultural context of resilience and protective factors (Masten, 2014; Unger, 2011). Future versions of the RPFC will potentially benefit from the addition of items that explore cultural and ethnic identity beyond the RPFC question that asks about religious beliefs and spirituality. In addition, further investigation of the two items that did not significantly load on any of the three subscales (the ‘regular use of physical exercise’ item and the ‘having a positive boyfriend or girlfriend [partner] who supports me and stays out of trouble’ item’) is needed due to the face validity of these items as protective factors. Another limitation that will need to be addressed in future studies is the wording of some of the RPFC items. The RPFC items were initially selected for inclusion based on their clinical utility and association with resilience; however, some of the RPFC items include two related concepts in one question (e.g., Item #2 states “I am good at calming myself down and thinking before I act”), which can impede researchers’ ability to accurately determine the specific influence of each protective factor component. Breaking apart some of the protective factor items into two separate items will benefit future examination of the RPFC (e.g., “I am good at calming myself down” and “I am good at thinking before I act”).
Implications
The findings of this study add to the growing evidence for incorporating resilience-enhancing protective factors into human services. The field is increasingly gaining insight into the importance of not only targeting problems and risk factors, but also adopting a strengths-based orientation that promotes strengths, protective factors, and resilient outcomes (Edwards et al., 2017; Jones et al., 2015, 2016; Langton & Worling, 2015; Powell, 2015; Sabina & Banyard, 2015; Sanders et al., 2015). The goal of human services work is to not only stop future problems and abusive acts but also assist people in acquiring the strengths, resources, and skills for leading prosocial, meaningful lives.
Utilizing a strengths-based tool like the RPFC, can positively impact the process and content of human services. When services include an emphasis on protective factors linked to resilient outcomes, clients and students are more likely to be engaged, hopeful, and internally motivated, which are key components for effective services (Holdsworth et al., 2014; Kemp et al., 2014; Powell, 2017; Waters et al., 2019). Incorporating resilience-enhancing protective factors that move beyond a risk and problem-focused emphasis, heightens the clinical utility of assessment, case conceptualization, treatment planning, school engagement, academic achievement, educational interventions, therapeutic interventions, treatment progress appraisal, and safety/health promotion planning. The RPFC appears to be a promising new measure for assessing a broad spectrum of ecologically-based protective factors (including individual traits, familial supports, and community resources) that can assist in the promotion of resilient, positive life outcomes.
Footnotes
Author Biographies
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.