
Abstract
The American Psychiatric Association (APA) has called for further research on Internet Gaming Disorder (IGD) by placing it in Section III of the Diagnostic and Statistical Manual (DSM-5). Research on prevalence, risk factors, and development of criteria for a diagnosis of IGD is mixed in the literature. This study sought to contribute to these topics by examining a diverse sample of Internet gamers (N = 1,881) from around the world. Results showed a prevalence rate of 4.2%, with varying prevalence rates based on demographic characteristics. Significant risk factors for IGD included gender and hours spent gaming. Finally, frequency counts of IGD criteria showed significant differences between participants meeting IGD criteria and those not meeting criteria, as well as significant differences by gender and age. Low frequency counts and significant differences based on demographics point to criteria that may be less appropriate for a diagnosis, as well as considerations for diagnosing diverse populations. Limitations and future research are discussed.
Introduction
In the DSM-5 released in 2013, “Emerging Measures and Models” appear in Section III of the manual. These potential areas require further research until they can be considered for inclusion in the manual’s main section (APA, 2013b). In previous DSM editions, this material was placed in the appendices; however, the American Psychiatric Association (APA) has reserved a separate section in the manual in the hopes that clinicians will have a greater awareness of the criteria within it. Internet gaming disorder (IGD) is one of eight conditions listed for further research in Section III. Each condition presents suggested diagnostic criteria, as well as information including diagnostic features, prevalence, risk factors, functional consequences, differential diagnosis, and comorbidity. The nine diagnostic criteria for IGD proposed in Section III include: (1) preoccupation with Internet games; (2) withdrawal symptoms when Internet gaming is taken away; (3) tolerance: the need to spend increasing amounts of time engaged in Internet games, (4) unsuccessful attempts to control the participation in Internet games; (5) loss of interest in previous hobbies and entertainment as a result of, and with the exception of, Internet games; (6) continued excessive use of Internet games despite knowledge of psychosocial problems; (7) has deceived family members, therapists, or others regarding the amount of Internet gaming; (8) use of Internet gaming to escape or relieve a negative mood; and (9) has jeopardized or lost a significant relationship, job, or educational or career opportunity because of participation in Internet games (APA, 2013a, p. 795).
Issues with internet gaming disorder criteria
Researchers hope that the publication of nine diagnostic criteria in Section III of the DSM-5 will lead to more consistent evidence-based studies to inform prevention, diagnosis, and treatment of IGD (Dowling, 2014; Kuss & Griffiths, 2012a). However, IGD’s inclusion in the section engenders controversy in the helping and addictions fields. Without a clear conceptualization and definition of IGD and without evidence-based diagnostic criteria, there is room negative impact on public health (van Rooij et al., 2018). Historically, IGD is classified as a behavioral or process addiction (Demetrovics & Griffiths, 2012), hence its inclusion in the DSM-5 with criteria of compulsive-like behaviors associated with cravings, urges, and disruption of social and occupational functioning resembling substance use disorders and gambling disorder (APA, 2013a).
Diagnostic criteria should serve the purpose of distinguishing healthy behavior from pathology, yet researchers express concern about pathologizing recreational gaming behavior based on the criteria as they are currently written (e.g., van Rooij & Prause, 2014). Researchers (Billieux et al., 2015) have found a spectrum of Internet gaming behaviors and psychiatric features that are not captured by behavioral addictions models and thus not by the nine criteria in Section III of the DSM-5. Furthermore, Billieux et al. (2015) along with other researchers (e.g., Billieux et al., 2019; Musetti et al., 2019) have produced findings that distinguish between problematic and non-problematic gaming in more nuanced ways than the nine criteria allow. In addition, the nine criteria for the potential disorder, as they are currently worded, do not adequately distinguish IGD from a more general addiction to the Internet (Kuss et al., 2014). Authors et al. (2016) explain that the Internet is a broad forum where users can engage in many reinforcing activities, not just gaming. Other activities for which the Internet is the medium include Internet gambling addiction (Lee et al., 2012), sex addiction facilitated by the Internet (Jones & Hertlein, 2012), Internet addiction associated with online auctions (Tonioni et al., 2012), and social media and shopping (Murali & Onuba, 2009). Authors et al. (2016) suggest that Internet addiction may be useful as an umbrella diagnosis (Luo et al., 2015) to help explain comorbid addictions to the specific activities.
Many researchers are calling for refinement of the IGD criteria as they are currently written (Dowling, 2014; Tao et al., 2012). Specifically, Tao et al. suggest that some of the criteria are not accurate and some may be more central to the diagnosis of IGD than others. King and Delfabbro (2015) believe that the preoccupation criterion should emphasize the kinds of cognitions gamers experience, not how often they experience them. Further, this criterion may pathologize enthusiastic recreational play when addiction does not exist (Kardefelt-Winther, 2014, 2015) and fail to take gaming context into consideration, since professional or high achieving gamers may devote significant time to considering and discussing gaming strategy (Faust et al., 2013; Ko et al., 2014). Next, tolerance and withdrawal criteria may not be measurable in the same way for a process addiction as it is for a substance addiction because there is no physiological input from a behavior (van Rooij & Prause, 2014). Ko (2014) suggests that tolerance for IGD may be measurable based on the decreased satisfaction gamers experience instead of the need to game more. Specific to withdrawal, researchers explain that withdrawal to IGD is not the unpleasant feelings experienced by gamers when they are suddenly forced to stop gaming, such as the anger a child might feel when a parent forces her to stop gaming. Instead, it is the symptoms, i.e., irritability, anxiety, or sadness, experienced from one hour up to two weeks after gaming has ceased (Kiraly et al., 2015). Next, the criterion illustrating loss of interest in other activities draws criticism from researchers because it does not consider the developmental of the gamer (Kuss et al., 2017), who might be engaging in new activities in a developmentally appropriate way, e.g., an adolescent. Other debated criteria include the escape and deception criteria. Derived from DSM-IV criteria for pathological gambling and substance dependence, these criteria may not be accurate for IGD, as they show low frequency amongst problematic gamers (Ko et al., 2014).
Finally, researchers suggest that the criteria are confusing because they are conceptually too similar to criteria for gambling and substance use disorders (Petry et al., 2014) and because the disorder is often comorbid with such a wide variety of other disorders (Dowling & Brown, 2010). Disorders most commonly comorbid with IGD include depression, anxiety, panic disorder, social phobia (Allison et al., 2006), ADHD (Batthyány et al., 2009), and substance addiction (Ko et al., 2012). Thus, it is difficult to conclude how IGD is associated with these issues. For example, it could be difficult to determine if IGD is being used as a coping mechanism for a condition like anxiety or if the IGD is an exacerbating factor for the anxiety. Authors et al. (2016) suggest that future research should be conducted to determine how people with IGD may be using Internet gaming to cope with symptoms of other mental health concerns, similarly to how people with substance addiction use the substance to cope with symptoms from other mental health concerns.
Prevalence
Prevalence rates for problematic Internet gaming vary in the studies reviewed based on population, criteria, and assessment tools. In fact, over 20 different instruments assessing for IGD have been noted in the literature when prevalence is being reported (Griffiths, 2016). King et al. (2013) reviewed 18 of these instruments and found discrepancies amongst indicators of addiction, poor information on cutoff scores, and lack of interrater reliability and predictive validity. This lack of consistency makes it hard to pinpoint even a meaningful range relative to prevalence of IGD. The following studies demonstrate this inconsistency. A study of German adolescents (N = 11,003) using criteria adapted from the DSM-5 reported a prevalence rate of 1.16% for IGD (Rehbein et al., 2015). A Dutch study using the Compulsive Internet Use Scale (CIUS) and studying two samples (N = 1,572, N = 1,476) of adolescent online gamers age 13-16 showed that 3% of participants reported addiction-like problems including withdrawal, loss of control, salience, conflict, and coping for mood modification (van Rooij et al., 2011). Similarly, in a South Korean study of students between 12 and 18 years of age (N = 600), 2.2% of participants met criteria for addiction according to Young’s Internet Addiction Test (IAT) (Jeong & Kim, 2010). Rehbein et al. (2010) surveyed German ninth graders (N = 44,610) with a video game dependency scale based on the IAT to find that 3% of male and 0.3% of female students would be diagnosed as addicted to video games. In an Australian study of high school and college students (N = 2,031), 5% of participants met criteria for addiction to computer games and the Internet respectively, according to DSM-IV-TR criteria for pathological gambling (Thomas & Martin, 2010). In an international study of adolescent and adult gamers (N = 1,945), researchers used DSM-IV criteria for substance dependence to determine that 8% of participants met criteria for problematic gaming (Porter et al., 2010). The 8% reported having fewer friends in the real world than non-problematic gamers and considered it easier to meet people online than in the real world. A German study sampled young adult Internet gamers with a mean age of 21 years (N = 7,069) and found that 11.9% of participants met criteria for addiction (Grüsser et al., 2007). Yee (2006b) reports that 50% of MMORPG players (N = 30,000), ranging in age from 11-68, consider themselves to be addicted. Although he did not perform a clinical assessment of IGD on the participants, the author reported the statistic to illustrate the emotional investment users have in the games, as well as the high level of appeal of the games. The above studies utilized different assessment instruments, criteria, and populations; however, the findings indicate the potential of a significant problem across generations and nationalities of Internet gamers with real world consequences.
Demographic risk factors
Risk factors are an important consideration in prevention research. Several demographic risk factors are documented in the literature on IGD, but other groups are underrepresented. First, being male has been shown to be a risk factor for IGD (Authors et al., 2019; Batthyány et al., 2009), but less research has been conducted on female gamers, and most studies report a much higher percentage of male participants (e.g., Fuster et al., 2012). Still, recent studies have reported that there is a rising trend of female gamers (Kuss & Griffiths, 2012b), specifically female gamers over the age of 50 (ESA, 2014). Other researchers who have examined gender and IGD have found themes related to their motivation to play Internet games. Authors et al. (2019) found maleness to be a predictor of both social and achievement motivation to play. However, Yee’s (2006a) study reported an association between maleness and achievement motivation and no gender differences for social motivation, also noting an association between femaleness and relationship-building. Park et al. (2011) also found femaleness to be associated with relationship-building. Yee (2006a) and Yee et al. (2012) noted that males and females may both be motivated to engage socially while playing Internet games, but they may pursue online relationship differently. Authors et al. (2019) noted the importance of recognizing the nuanced nature of social interactions and social motivation, both online and in the real world, in order to avoid putting gamers into any one particular box.
Next, living in an Asian country is reported as a risk factor for Internet-related addiction (Lin et al., 2011). However, much of the research on IGD has been conducted in Asian countries, and more research should be conducted in the United States to determine risk factors specific to this culture (Kuss & Griffiths, 2012a). Finally, college students have been shown to be more highly susceptible to Internet-related addictions (Frangos et al., 2010; Lin et al., 2011). Conversely, Authors et al. (2019) tested for age, gender, ethnicity, and student status, and only maleness was a significant predictor of IGD. However, both Authors et al. (2019) and Yee (2006a) found younger age to be a predictor of motivation to achieve in Internet games. Ultimately, IGD has the potential to affect any population with Internet access, and risk factors go well beyond demographic factors to include psychological and psychosocial factors (Dowling & Brown, 2010). The American Psychiatric Association recognizes the potential problem of IGD and has called for further research on the disorder by placing it in Section III of the most updated edition of the DSM (APA, 2013a).
Method
This study used a non-experimental group correlational design and reported both descriptive and inferential statistics to answer the following research questions: What is the prevalence rate for IGD using the current DSM-5 criteria? What are demographic risk factors predicting IGD? What is the utility of the DSM-5 criteria for IGD based on frequency counts and significant differences between groups?
Participants
Participants were adult (18+) Internet games who have played a Massively Multiplayer Online Game (MMO) within the past 12 months. Participants were primarily recruited online via Facebook and Reddit. The sample of 1,881 gamers collected represented both the United States (n = 1,563) and abroad (n = 318). The researcher reports demographic details for the population sampled in the results section.
Measures
IGD was measured using the Ten-Item Internet Gaming Disorder Test (IGD-10) (Kiraly et al., 2015). Participants who meet five or more of the following nine criteria may have a diagnosis of IGD: Preoccupation; withdrawal; tolerance; failed attempts to stop gaming; loss of interest in other activities; continued use despite psychosocial problems; deception; escapism; and relational, educational, or vocational consequences. A demographic questionnaire collected information on age, gender, ethnicity, student status, hours spent on work per week, and hours spent gaming per week.
Procedure
Data collection began after institutional review board approval, entailed digital and face-to-face methods, and used purposeful sampling to reach a diverse sample of gamers. The digital measures, namely using Facebook and Reddit, allowed for thousands of gamers from around the world to complete the survey. The researcher cleaned data for missing cases, transformed variables for analysis, identified and eliminated outliers, and conducted descriptive statistics to test for linear regression and ANOVA assumptions. The researcher used SPSS (Version 24.0) to conduct all analyses.
Statistical analysis
The researcher reported descriptive statistics related to population demographics, prevalence of IGD, and frequency of IGD criteria by demographic group. The researcher identified significant predictors of IGD using linear regression and significant differences between groups using t-tests and one-way ANOVA tests.
Results
Population demographics
Data collection in this study produced an international sample of Internet gamers (N = 1,881) from 56 different countries around the world on six continents, and from 49 of the 50 United States, plus Washington D.C. and Puerto Rico. Based on the wide net cast to collect data from the Internet gaming population and on the international access to gamers afforded by electronic means of data collection, the researcher expected demographic diversity related to age, gender, ethnicity, and student status. However, the population sampled was particularly homogenous in the areas of age and ethnicity. Of the population sampled 45.5% of the gamers in the study were 25 years of age or under (n = 853), and 70.5% were 30 years of age or under (n = 1,320). The other 29.5% of the population sampled represented participants in their 30s, 40s, 50s, and beyond (n = 561), with only 2.4% of the population sampled over the age of 51 (n = 53). In addition, more than three-quarters of the population sampled identified as White/Caucasian (n = 1,456), leaving less than 20% represented by African American, Hispanic/Latino/Latina, Asian, and multiracial ethnicities (n = 356). The population sampled is more diverse related to gender, with almost 60% of participants (n = 1,118) identifying as male and almost 40% identifying as female (n = 732). While the author offered non-binary choices for gender, few participants (n = 31) chose those options. Finally, 38% of the population reported student status (n = 722), providing an adequate proportion to compare to the non-student population. Because of the younger age reported by participants in the study, it is logical that a significant proportion would be students. Overall, if these demographic statistics were applied to the general population, it would appear that younger, White males and females are most representative of the Internet gaming population. The population sampled in this study is comparable to populations sampled in the literature when IGD is examined, and it is generally more representative of age and ethnicity than these other samples.
Internet gaming disorder prevalence
One of the most valuable aspects of this study is the results related to IGD prevalence and the specific criteria reported by the gaming population, in general, and by the population with a diagnosis of IGD. Of the population sampled, 4.2% met criteria for IGD (n = 79), meaning they reported five or more of the criteria listed in Section III of the DSM-5, as measured by the IGD-10. This prevalence rate is slightly higher than prevalence rates for other process addictions, including Anorexia Nervosa at up to 1.5% (APA, 2013a), gambling addiction at 2%, sex addiction at 3%, exercise addiction at 2%, and eating addiction at 2% (Sussman et al., 2011).
Potential risk factors for internet gaming disorder
The researcher also conducted analyses to report prevalence rates for demographic groups, including gender, age, ethnicity, student status, and geographic location (US or non-US). For gender, 8 out of 10 participants with IGD were male. Logically, the prevalence rate of IGD was higher for males in the study at 5.7%, and the prevalence rate for females was 1.5%. Similarly, 85% of participants with IGD were age 30 or younger. Prevalence rates in the current study were significantly higher for participants age 30 or younger (5.1%) versus 31 or older (2.1%). Overall, prevalence rate for males (5.7%) and for people age 30 or younger (5.1%) were higher than the prevalence rate for the overall population sampled in the study (4.2%), indicating that male gender and younger age status may be risk factors for IGD. For ethnicity, IGD prevalence amongst the sample who identified as White was 3.6%, lower than the overall prevalence rate. And prevalence for students was 4.3%, just slightly higher than the overall rate of IGD. Finally, prevalence rates varied based on geographic location. Participants living in the US had a prevalence rate of 3.4%, lower than the general IGD prevalence rate, while participants living outside the US had a significantly higher prevalence rate of 7.8%. These findings are important for informing screening and prevention when counselors are working with diverse populations.
In order to further clarify if gender, age, ethnicity, student status, or geographic location may be risk factors for IGD, the researcher conducted a regression of IGD on gender, ethnicity, age, student status, and geographic location, as well as hours spent gaming in order to understand their predictive relationships with IGD. These variables significantly predicted IGD in the overall model, F (6, 1723) = 17.626, p < .001, R2 = .058. However, only gender (β = −.13) and hours spent gaming (β = .22) were significant predictors of IGD. Since hours gaming was also a significant predictor of IGD, some details are provided about the way that variable interacted with IGD. When the entire sample was analyzed the average game play per week was 16.73 hours, but when the IGD population was analyzed the average play per week increased to 36.45 hours. In the non-IGD population 33.5% (n = 587) reported playing 16 hours a week or more, while in the IGD population 78% (n = 59) reported 16 hours per week or more.
Frequency of internet gaming disorder criteria
The researcher also examined descriptive statistics for the nine individual criteria measured by the IGD-10. Table 1 displays the criteria as reported by participants in the study from most frequently reported to least frequently reported. The table shows the frequency counts for the sample population without IGD and for the participants in the study meeting IGD criteria. Percentages of both populations that report each criterion are provided.
IGD criteria.

The researcher conduced t-tests to compare IGD scores in participants with IGD and participants without IGD. There was a significant difference in the scores for participants with IGD and participants without IGD, t(1880) = 9.079, p < .000. There were also significant differences between individual scores for all nine items of the IGD-10 for participants with IGD and participants without IGD at the p < .000 level. See Table 2 for mean scores, standard deviations, and effect size.
Means, standard deviations, and T test.
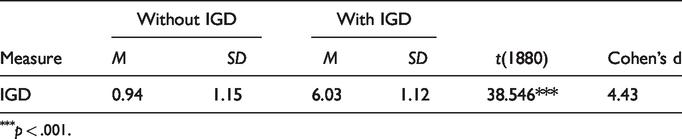
p < .001.
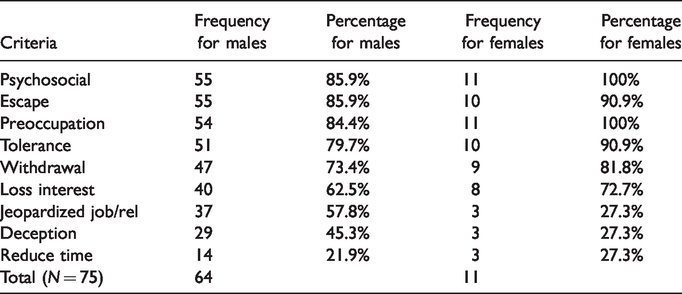
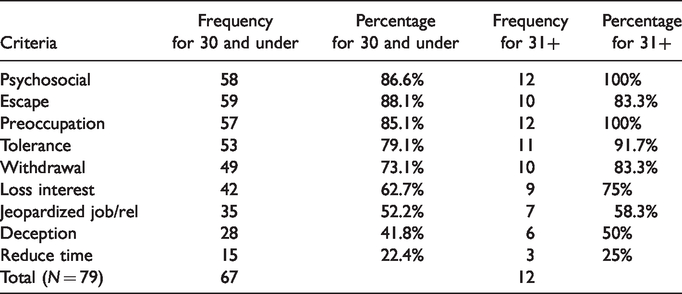
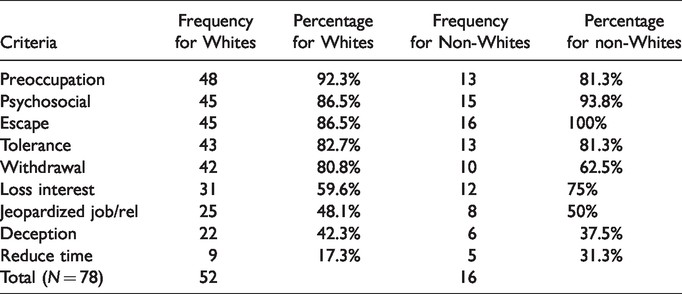
In an effort to add cultural context to the understanding of the IGD criteria, the researcher examined gender, age, and ethnicity differences in frequency of criteria reported in the study. Table 3 shows frequency differences by gender, Table 4 shows frequency differences by age, and Table 5 shows frequency differences by ethnicity. Reports on significance of the differences between groups follows each table.
Gender differences in IGD criteria among participants with IGD.
Age differences in IGD criteria among participants with IGD.
Ethnicity differences in IGD criteria among participants with IGD.
The researcher conduced one-way ANOVA tests to compare IGD scores based on gender. Results were nonsignificant for differences between males and females with IGD.
When one-way ANOVAs were conducted on IGD scores based on age, the researcher found a statistically significant difference between groups (F(1,77) = 4.864, p = .030). Table 6 reports mean scores, standard deviations, and effect size.
Means, standard deviations, and one-way analyses of variance.

***p = .030.
The researcher found no significant differences between ethnicity groups when ANOVA tests were conducted.
Discussion
The population sampled in this study is comparable to populations sampled in the literature when IGD is examined, and it is generally more representative of age and ethnicity. Yee (2006a) collected data from 3,035 participants who were 91% male. Yee et al. (2012) sampled two populations, one with 2,071 participants (65.6% male) with an average age of 29.95, and another with 645 participants from Taiwan and Hong Kong (80% male) with an average age of 23.59. They found that 22.2% of the population he sampled was represented by students. This author’s sample had more male participants than the current study, though average age is comparable, as is the percentage of participants with student status. Next, Jeng and Teng (2008) sampled 92 Taiwanese college students (age 18-27) with 60% being male. Park et al. (2011) also sampled Asian college students between the ages of 17 and 28. Of the 524 respondents, 47.6% were male. These smaller sample populations are equally representative of gender as the current study, but lack representation in the areas of age and ethnicity. Next, Caplan et al. (2009) sampled 4,278 participants ranging in age from 18 to 65 with a mean age of 32.47 and 81% being male. This larger sample had a similar age range as the current study with a slightly older average age and a significantly larger male population. Similarly, Graham and Gosling (2013) reported on a population of 1,413 comprised of 88% males, who had an average age of 26.04. Compared to these two studies, the population in the current study had a more equal sample of males (60%) and females (40%). Cole and Hooley (2013) collected data on 163 participants (56% male, 40% female) with an average age of 27.3. This small sample is comparable to the demographics of the population collected in the current study related to gender and age.
Prevalence rates in the literature vary significantly based on population sampled, criteria used, and assessment tool employed. Thus, it is most useful to compare prevalence rates among studies that use the same DSM-5 criteria. Compared to other studies using DSM-5 criteria for IGD, the prevalence rate in this study (4.2%) appears normal to high. Rehbein et al. (2015) found that 1.16% of the adolescents (N = 11,003) in their study had IGD according to DSM-5 criteria. Male participants in the study had a higher prevalence rate (2.02%) than females (.26%). Müller et al. (2014) also assessed prevalence in an adolescent sample (N = 12,938) across seven European countries and found that 1.6% met IGD criteria. A study of Dutch adolescents and adults (N = 2,444) found that 5.4% had IGD according to DSM-5 diagnosis (Lemmens et al., 2015). The researchers also reported a higher prevalence rate among male participants (6.8%) than female participants (4.0%), consistent with the current study.
Prevalence rates for IGD are based on the nine criteria in Section III of the DSM-5. The criteria are currently under research to determine their appropriateness for diagnosing IGD. The frequency order of criteria reported among the population sampled in this study with IGD were: psychosocial consequences, escape, preoccupation, tolerance, withdrawal, loss of interest in other activities, jeopardized job or relationship, deception, and unsuccessful attempts to reduce time playing. Rehbein et al. (2015) also reported on the frequency of criteria reported among the population meeting IGD criteria in the DSM-5 and, similarly to the current study, found escape and preoccupation to be the most highly reported criteria among the population they sampled meeting IGD criteria. However, those researchers reported that the lowest frequency criteria were loss of interest in other activities and jeopardized relationships, which fell into slots six and seven out of nine in the current study. Future research is needed to determine the least frequently reported criteria among the nine, as part of deciding the most appropriate diagnostic criteria for IGD.
Of additional importance is the observation that IGD criteria reported by participants with a diagnosis of IGD closely matches the order of frequency of IGD criteria reported by the general population not meeting diagnostic criteria, with the main exceptions that psychosocial problems is more prevalent than escape, preoccupation, and tolerance; withdrawal is more prevalent than loss of interest in other activities; and jeopardizing of job and relationships is more prevalent than deception in the IGD population. However, even though the population meeting IGD criteria reported IGD criteria in almost the same order of frequency as the general population, there was a higher percentage of each criterion reported in the IGD population. For example, using games as a means of escaping from negative emotions is the number one criteria reported in the general population and the number two criteria in the IGD population. In the general population 26.8% of participants reported using gaming to escape, but a much larger 87.3% of the population with IGD reported the criteria. Similarly, preoccupation was reported by 26.9% of the general population, but by 87.3% of people with IGD. It is logical to report that more criteria are reported more frequently among the population meeting diagnostic criteria for the disorder. However, this finding calls into question whether the criteria as they are currently presented in the DSM-5 are meaningful to discriminate gamers with addiction from gamers without addiction. Lemmens et al. (2015) explained that some criteria may lack specificity to IGD. These researchers found that preoccupation, tolerance, and withdrawal were particularly specific to gamers with IGD, but that escape was not especially useful for this purpose, despite its high frequency rate. Further research, beyond just frequency count, is needed to assess for the usefulness of the nine criteria in Section III of the DSM-5 for determining an actual addiction to Internet games.
In an effort to add cultural context to the understanding of the IGD criteria, the researcher examined gender, age, and ethnicity differences in frequency of criteria reported in the study. Only differences by age produced statistically significant results, which may be due to the small number of participants who met criteria for IGD (n = 79). Still, it is noteworthy that 60% of participants in the study were male, but 80% of participants meeting criteria for IGD were male. Furthermore, though in a slightly different order, female participants meeting criteria for IGD had the same top five criteria for frequency reported: psychosocial consequences, preoccupation, escape, tolerance, and withdrawal. One area of interest, however, is that a significantly low percentage of female gamers with IGD report jeopardizing job or relationship, deception about gaming behavior, and difficulty reducing time spent gaming. The nonsignificant difference between males and females meeting IGD criteria and the similarity in top reported IGD criteria indicates that screening using current DSM-5 criteria for IGD can be conducted similarly for males and females, but some criteria may be less relevant for females than for males.
Implications for age and ethnicity groups follow suit. For age, 7 out of 10 participants in the study were 30 or younger, yet 85% of participants meeting IGD criteria were in this younger age bracket. However, while 85% of participants with IGD were 30 or younger, their mean IGD score (5.91) was lower than the mean IGD score (6.67) for participants 31 and older. Similarly to gender, older participants with IGD reported the same top five criteria, supporting similar screening for people of all ages. For ethnicity, three-quarters of participants identified as White/Caucasian and two-thirds of participants meeting IGD criteria were White/Caucasian. Again, though in a slightly different order, non-White participants with IGD had similar top five criteria for IGD as the dominant White/Caucasian group. However, non-White participants with IGD reported loss of interest in other non-gaming activities as the fifth most frequent criteria met, while White participants with IGD maintained withdrawal as the fifth most frequent criteria. Though they did not achieve statistical significance for differences between groups, these results point to the possibility that there may be subtle differences between White and non-White groups when screening for IGD criteria, but that screening with current DSM criteria can be conducted similarly across ethnic groups. More research with a more diverse sample, specifically related to age and ethnicity, is needed to draw definitive conclusions.
Frequency of criteria is just one way to measure how appropriate criteria may be for making a particular diagnosis. However, the literature suggests potential problems with several of the IGD criteria listed in Section III of the DSM-5. Ko et al. (2014) suggest that low frequency of the escape and decision criteria may indicate that they are inaccurate for IGD. However, the current study showed that escape was the second most frequently reported criterion among participants with IGD, with 87.3% reporting the behavior. Deception, on the other hand, was reported with lower frequency by the population in the current study, with only 43% of participants with IGD identifying the behavior. It was not the least frequent criterion reported, however, with unsuccessful attempts to reduce time gaming coming in last slot at 22.8%. Both deception and unsuccessful attempts to reduce time gaming were reported with particularly low frequency among the female participants with IGD. Further research may indicate that deception is not an appropriate criterion for diagnosing IGD, but the escape criterion was consistently reported across gender, ethnic, and general population groups, and may remain as a valid criterion for assessing IGD.
Limitations and future research
The descriptive nature of the current study does not measure causation and is subject to flaws in internal and external validity. Equivalency between groups, including age and ethnicity, was also a limiting factor. However, since the demographic statistics in the current study matched samples in other studies examining IGD, it may be that members of the Internet gaming population are more likely to be White and younger. Next, the self-report nature of the data in this study is alto a threat to internal validity. Selection bias is a potential risk to generalizability in this study; however, the similarities between this sample’s demographic characteristics and other studies examining the population show this to be a minimal risk. Above all, the use of electronic methods allowed for collection from a diverse sample, and gamers from all six continents were able to contribute to the sample pool.
Future research needs to determine the appropriateness of the nine proposed diagnostic criteria in Section III of the DSM-5. Researchers need to determine if IGD is a separate condition or construct than other types of problematic Internet conditions. It would seem that the next step in this line of research would be to design a measure to test the diagnostic criteria for problematic internet conditions (perhaps factor analysis) to see if the symptomology of these conditions cluster on one factor (perhaps suggesting one diagnosis) or load on multiple factors (disorders). Furthermore, qualitative inquiry could help to describe the context of Internet gaming and the experiences gamers have with the technology, simulation, and social interactions in the games, especially when they meet criteria for addiction or identify as having an addiction.
Conclusion
Above all, should research show that IGD is a legitimate diagnosis meriting inclusion in the DSM, the diagnostic criteria should reflect the context of gaming, i.e., the technology, simulation, and social nature of the games. There may be overlap with substance use disorder criteria because of common features in addictions and with gambling disorder as another process/behavioral addiction. However, criteria should also be worded to recognize both the similarities and differences between the digital and real world. Also to be recognized should be the legitimate social relationships games may have in the games, as well as the use of gaming as a way to socialize with real world friends.
In addition to adding context to existing criteria, removing some criteria may improve the diagnostic process as well. Deception, consistently questioned in the literature, is of particular concern. It may be difficult to deceive others, because gaming is a hard activity to hide. When playing, gamers are visibly engaged in the activity, often wearing headphones, looking at a screen, and using a gaming console. Even if not physically visible to significant others, gamers’ usernames are often visible online and their activity may be trackable. Finally, unsuccessful attempts to stop, also consistently questioned, may not be relevant because it is based on an abstinence model. Fully abstaining from process/behavioral addictions is a less common practice than it is with substance addictions, and it may not be a desirable or feasible approach to take when attempting to treat or manage the addiction.
Escape, preoccupation, tolerance, and psychosocial problems are the most commonly reported criteria. Developing these criteria by adding gaming context and gaming references could improve the diagnostic specificity for the potential of an Internet Gaming Disorder diagnosis. For example, psychosocial problems could distinguish between social interaction the game and in the real world. Escape from negative feelings could pull from emerging research on the effects technology has on dopamine release in the brain. Preoccupation could consider the level of simulation possible in the gaming world and specify the role gaming plays in the gamer’s life (e.g., competition, occupation). While these are just suggestions, further research will show what context is most essential to these potential diagnostic criteria, in order to move away from the generic terminology in the criteria currently in Section III.