
Abstract
Surface acting—the management of emotional displays as part of a nurse’s work role—is increasingly getting scholars’ attention in organizational behavior. Previous research focused on the relationship between surface acting and outcomes (such as psychological well-being) on the basis of resource-centric theories, ignoring the subjective stance of surface acting provider. According to self-determination theory, surface acting affects an individual’s well-being through stimulating autonomous or controlled work motivation. Taking nurses as the subjects, the current study proposed that surface acting would affect job satisfaction and further psychological well-being through nurses’ controlled work motivation, and work and family support would moderate the above relationships in diverse directions. An online survey of n = 342 nurses working at a hospital in central China was conducted, evaluating surface acting, job satisfaction, psychological well-being, workplace support, and family support. Results indicated that surface acting negatively influenced nurses’ psychological well-being through job satisfaction. In addition, the results highlighted the two-faced aspect of social support, in which work support positively moderated the relationships between surface acting, job satisfaction, and psychological well-being, while family support intensified the abovementioned relationships negatively. These findings have important implications for surface acting, social support research, and managerial practices.
Keywords
Introduction
Nurses around the world are at high risk for low job satisfaction (Nantsupawat et al., 2011), especially in China, where healthcare reform is much needed. Nurses are expected to provide high-quality patient care to patients wanting perfect service (Maxime et al., 2009), and they tend to use surface acting (SA) when having to increasingly deal with difficult patients, as in, such a situation, it may be easier to just fake emotions (Chou et al., 2012). Therefore, SA becomes one of the most important requirements for nursing care.
Emotional labor, defined as “the management of feeling to create a publicly observable facial and bodily display’’ (Hochschild, 1983, p. 7), requires nurses to utilize emotional regulation strategies to figure out emotional dissonance (Grandey, 2003; Hochschild, 1983). As one of the strategies of emotional labor, SA is recognized as a way for employees to regulate emotional expression to align with the requirements of the organization without changing their internal emotional state, a good illustration being employees briefly faking a smile when they face patients (Grandey et al., 2015; Hochschild, 1983). Along the line, SA is performed based on wages and economic rewards, and this is inherently detrimental for them by creating an emotion that is different from their own feelings (Grandey et al., 2013; Hochschild, 1983). A series of research has revealed that SA has significantly adverse effects on nurses’ job strain and well-being (Kim et al., 2017; Schmidt & Diestel, 2014).
Moreover, previous research is based on resource-centric theories (e.g., conservation of resource theory, effort-recovery model, or the job demand-resource model) to explain the adverse effect of SA. Drawn upon resource-based models, SA is particularly resource-consuming because it requires a tremendous investment of physical, cognitive, and emotional resources to control inner emotions as well as to constantly alter their emotional expression (Grandey & Melloy, 2017), thus having a negative effect on individuals’ well-being (Grandey & Melloy, 2017; Kinman et al., 2011; Uy et al., 2016). However, the role of individual psychological motivation has been neglected and recent studies call for a person-centric perspective to clarify the relationships (Grandey et al., 2015). Person-centric perspective argues against treating a person as an object in an organizational system, instead favoring a comprehensive and focused appreciation of the individual at work, their thoughts, feelings and behaviors, which highlight subjectivity as the most fundamental nature of human existence (Weiss & Rupp, 2011). Along these lines, self-determination theory (SDT) is a motivation model that guides the current study with regard to basic psychological needs and employees’ optimal functioning, such as job satisfaction, and psychological well-being (PWB) (Deci & Ryan, 2000; Gomez Baya & Lucia Casademunt, 2018; Huyghebaert et al., 2018). Therefore, the SDT model is used to explore how and when SA affects nurses’ well-being.
Psychological well-being (PWB) refers to well-being as a result of realizing human potential through personal fulfillment and the pursuit of complex goals (Ryff & Singer, 2008). Nurses with poor PWB affect patient safety, quality and performance of care, and organizational profitability (Rose & Glass, 2010). Therefore, there is an urgent need to explore what factors could alleviate the negative effects of SA on PWB. Following previous studies (Chen et al., 2012; Duke et al., 2009; Grandey, 2000; Hur et al., 2015), we believe that social support can function as a moderator in the link between SA and employees’ well-being. As indicated in SDT, social environment (i.e., social support) could both promote or hinder the formation and development of an individual’s autonomous motivation through facilitating or threatening the three psychological needs (Deci & Ryan, 2000). Several scholars have called for studies to examine the moderating roles of different types of social support between emotional labor and work outcomes (Kim et al., 2017), yet empirical literature is insufficient. Work and family are important support sources and prior research has provided a great deal of evidence for their buffering effect in weakening emotional burnout (Duke et al., 2009; Hur et al., 2015; Kinman et al., 2011). To better understand the boundary condition, by integrating social support theory with SDT, this study attempts to explore the moderating roles of workplace support and family support.
Our study makes multiple contributions to the literature because of the following reasons. First, unlike the resource-based perspective of “emotion regulation” and “resource depletion”, this study utilizes SDT as an overarching theory to propose a moderated mediation model, which provides an innovative lens to explain the effect of SA on employees’ PWB. Second, our research contributes to the influencing mechanisms between SA and PWB by examining the mediating role of job satisfaction, indicating that low self-determination in a job may trickle down to other areas of life, resulting in a low sense of individual growth and achievement. Finally, we enrich the boundary conditions of the relationship between SA with job satisfaction and PWB by exploring the two sources of social support. We explain that each is unique, and that they would not matter the same in buffering the negative effect of SA.
The framework is illustrated in Figure 1. Theoretical model.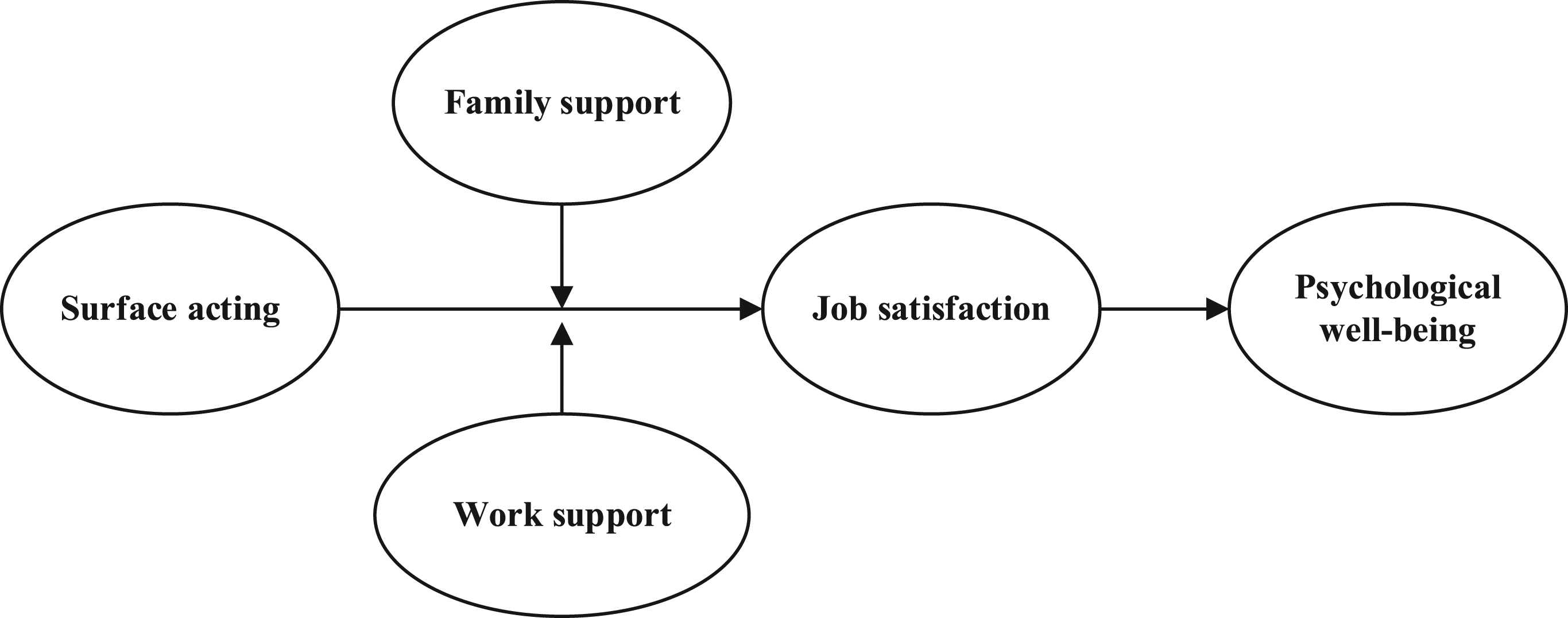
Theoretical Background and Hypotheses
Self-Determination Theory
SDT proposes that individuals have three basic psychological needs—autonomy, relatedness, and competence. Autonomy refers to individuals’ need to make choices about their actions on their own behalf; relatedness is individuals’ need to feel connected to, accepted by, and relate with others; and competence refers to individuals’ need to succeed in challenging tasks and achieve desired outcomes (Deci & Ryan, 1987). When these needs are met by an individual’s work, life, or environment, they experience self-determination satisfaction, which helps to form autonomous motivation to engage in behaviors conducive to self-development (Deci & Ryan, 2000).
SDT is proposed for the purpose of describing individual behaviors in the context of promoting the satisfaction of needs, and a recent line of study proposed that not only can the work environment satisfy psychological needs but it can also thwart them (Gillet et al., 2012). Further, scholars showed that psychological need satisfaction and thwarting are not the opposite ends of a continuum, but instead are two distinct psychological experiences (Bartholomew et al., 2011). In other words, the work environment can give employees a sense of high need satisfaction, but it can also make them feel high need thwarting (Huyghebaert et al., 2018). Therefore, when the needs are threatened by an individual’s work, life, or environment, these factors will limit autonomous motivation and be detrimental to self-development.
The Mediating Effect of Job Satisfaction Between SA and PWB
Job satisfaction, a comprehensive appraisal of how employees feel and experience work, includes emotional (referring to an individual’s emotions about work) and cognitive satisfaction (an individual’s evaluation of work) (Sironi, 2019). According to Hochschild (1983), SA is a form of externally regulated behavior driven by external contingencies concerning threats of punishment and material or social rewards. Thus, we propose that SA limits autonomous motivation and induces controlled motivation by threatening the autonomy, competence, and relatedness needs of nurses, which decreases their job satisfaction. First, in their daily interactions with patients, nurses are required to frequently engage in SA by amplifying the expression of positive emotions and suppressing the expression of negative emotions to express appropriate emotions, which threaten their autonomy needs due to losing one’s control of emotional self-expression (Grandey & Melloy, 2017; Hochschild, 1983). Additionally, frequently engaging in SA by amplifying and suppressing emotions is effortful and depletes one’s energy resources. Moreover, SA might lead to a view that one’s genuine emotions are neither valuable nor fit for the job (Grandey et al., 2015), leading to a perception of being less efficient, thus threatening the nurses’ need to feel competent. Finally, nurses are often required to understand the patient’s feelings, to show concern and sympathy, and suppress feelings of disgust or fear while interacting with patients. Therefore, SA could harm nurses’ relatedness needs by creating an atmosphere where nurses perceive that their dignity and respect are not important, and thus ignored (Grandey et al., 2007). When employees perceive that their essential psychological needs are threatened in the workplace, they are likely to evaluate their work experience adversely. This negatively impacts their workplace well-being, such as, job satisfaction (Gagné & Deci, 2005; Huyghebaert et al., 2018). Hence, we propose that SA might thwart employees’ need satisfaction, resulting in low job satisfaction.
PWB is a context-free construct that identifies well-being with the complete fulfillment of humanness through the expression of personal value and potential in aspiring complex goals (Ryff & Singer, 2008; Zheng et al., 2015). An individual’s work is an important domain of their life (Zheng et al., 2015) and their feelings of PWB are thus obviously influenced by their job (Sironi, 2019). The spillover theory suggests that individual experiences in one life domain can subtly influence experiences in other domains (Timothy et al., 1994). In other words, low self-determination in one’s job may spill over to other wider domains, yielding low self-determination to pursue goals and develop potential. Alternatively, it has been revealed that negative work emotions (such as sadness, anger, concern, or fear) can negatively affect personal accomplishments (Zapf, 2002). In contrast, employees with high job satisfaction are likely to obtain a high perception of personal progress, eventually benefiting their realization of self-potential (Gomez Baya & Lucia Casademunt, 2018; Ilardi et al., 1993). Thus, it could be argued that low workplace well-being probably will lead to low PWB.
Therefore, engaging in high levels of SA can lead employees to perceive the restriction of essential psychological needs—autonomy, competence, and relatedness—leading to lower job satisfaction, which can eventually be detrimental to the realization of self-potential and personal growth. Hence, we propose that job satisfaction mediates the link between SA and PWB.
H1: Job satisfaction mediates the relationship between SA and employees’ PWB.
The Moderating Role of Work Support
Social support is defined as actual resources provided by social interactions or relationships to deal with stress, or a sense of attachment to a person or group which is considered to be “caring or loving” (Chen et al., 2012). Support can be in the form of emotional concern, instrumental aid, information, or appraisal (Eisenberger et al., 2002). Work support is an important material and emotional resource for coping with requirements and reducing job strain (Kinman et al., 2011). Research has found that supervisors’ support is directly related to employees’ motivation and psychological adjustment (Gallie et al., 2017). According to SDT, when perceiving high work support within the workplace, employees engaging in SA will feel less controlled motivation with regard to the less restricted basic psychological needs. Therefore, it can be deduced that the negative influence of SA on job satisfaction is weaker when nurses perceive high work support, as a higher degree of work support can compensate for the individual’s psychological needs, helping them internalize the external motivation made by SA. The reasons are as follows:
First, high-quality interactions with their supervisor and coworkers helps nurses better grasp the significance of their job or tasks (Grant, 2007). This makes them less resistant to the emotional demands of the organization and increases the internalization of the emotional requirements. Therefore, the perception of restricted autonomy is eliminated. Second, when guidance and aid from supervisors and coworkers are readily accessible, nurses complete their tasks quicker and more effectively (Grandey et al., 2012). Consequently, emotional disturbance from SA, such as confusion about their own competence, lasts for a shorter time, resulting in less damage to their sense of competence. Third, when nurses are aware that supervisors and coworkers value their contributions and care about them (Eisenberger et al., 2002), their emotional isolation due to SA is likely to be compensated for, and quickly recovered from. Thus, the reduction in relatedness resulting from SA slows down. In other words, with high work support, nurses experiencing SA are more likely to change their opinions toward emotional demands. They distance themselves from emotional disturbance or emotional isolation, which reduces the thwarting for psychological needs, bringing about higher levels of job satisfaction, compared to low work support situations. In prior studies, work support was found powerful enough to stop SA from negatively affecting job satisfaction (Duke et al., 2009; Grandey & Melloy, 2017). Therefore, we propose that when nurses perceive a high level of support from the workplace, the negative impact of SA on job satisfaction can be mitigated. The following hypothesis was proposed:
H2: Work support will moderate the relationship between SA and job satisfaction where a high level of work support will weaken the negative relationship.
The Moderating Role of Family Support
Some scholars have argued that the different roles of social support depend on whether it is independent of stress sources (Blau, 1981). In general, family support, such as emotional concern and instrumental aid (Alcover et al., 2018), has been revealed to be a key factor in causing feelings of being controlled or feeling intruded upon (Brock & Lawrence, 2009, 2014), as well as feelings of loss of autonomy and crossing the boundaries of intimacy (Newsom & Schulz, 1998; Rafaeli & Gleason, 2009). This is true especially of women who account for the majority of nurses (Feng, et al., 2019). Compared to men, women are more embedded in their family network; they are more likely to be exposed to adverse network events either through the exposure to stressors, or conflicts that are experienced in intimate relationships (Walen & Lachman, 2000). Several studies indicate that more family connection is not always better for women because their personal subjectivity (thoughts, feelings, and behaviors) is more extremely depleted (Schoenbach et al., 1986). When employees engage in SA, perceived family support may accelerate the impairment of their psychological needs.
To be specific, first, under high family support, when nurses experience SA, they would have stronger desire to put up with it, work harder and more persistently to benefit their family (Menges et al., 2017). At the same time, the sense of autonomy restriction becomes stronger. Empirical studies have demonstrated that employees’ perception of support from family members may cause distress due to impaired autonomy (Brock & Lawrence, 2009, 2014). Second, a high degree of family support without boundaries results in perceptions of over-protection and personal defeat, since this support is sometimes attributed to lack of competence or efficiency (Newsom & Schulz, 1998). Therefore, receiving support passively may not enhance one’s self-worth but actually threaten it (Uy et al., 2016) and may reduce a person’s attention to the task because the family support may be not useful (Ehrhardt & Ragins, 2019). Furthermore, although family members can provide support concerning work experience, interaction with them could also arouse feelings of tension, anxiety, and other undesired emotions, along with more resistance to work demands regarding emotion, eroding employees’ relatedness needs (Lim & Lee, 2011). Therefore, we propose that when employees perceive high family support, the negative impact of SA on job satisfaction is accelerated. The following hypothesis is proposed:
H3: Family support will moderate the relationship between SA and job satisfaction where high level of family support will accelerate the negative relationship.
A Moderated Mediation Model
As discussed above, it seems that nurses perceiving different types of social support may have distinct responses to the negative effects of SA. It can also be inferred that the strength of the indirect relationship between SA and PWB through job satisfaction is likely to vary under different levels of social support, showing a moderated mediation model (Edwards & Lambert, 2007). In particular, when employees engage in SA, high support from the workplace may compensate their psychological needs, helping transform controlled motivation into autonomous motivation. Therefore, the negative relationship between SA and job satisfaction may be relieved, resulting in a weaker negative indirect effect on employees’ PWB. However, when employees engage in SA, high family support may fuel their perception of controlled motivation, facilitating the negative relationship between SA and job satisfaction, ultimately exerting a stronger negative indirect effect on employees’ PWB.
By integrating the SDT, we proposed a moderated indirect effect model in which SA affects PWB through job satisfaction, varying with two types of social support. Therefore, the following hypotheses were proposed:
H4. The indirect effect of SA on employees’ PWB via job satisfaction is weaker for those with high work support.
H5. The indirect effect of SA on employees’ PWB via job satisfaction is stronger for those with high family support.
Methods
Sample and Procedures
For 2 weeks, data of nurses working in a tertiary hospital in central China were collected. The hospital is the largest general medical institution in the region and undertakes medical rescue tasks in the surrounding provinces and cities. The hospital employs over 3500 personnel, of which 1500 are clinical front-line nurses. One of the authors working at the department of science and training in the hospital could reach out to every nurse. An online questionnaire link was generated after the survey content was uploaded onto the online platform “Questionnaire Star.” The link was sent to WeChat working groups to ensure that all of the nurses (500+) could access it. The inclusion criteria were employees working as a registered nurse for 1 year or more, and nurses who were on duty in the last 2 weeks. Nurses who did not directly participate in the care of patients (e.g., training position) and part-time nurses were excluded. Participants were invited to complete the online questionnaire while ensuring confidentiality and anonymity of their responses and identity. Two weeks later, all completed questionnaires were collected and analyzed. A total of 386 questionnaires were completed. After eliminating invalid responses due to missing responses, the final sample consisted of 342 responses, with a response rate of 88.6%.
Of the 342 respondents, the average age was nearly 35 years, 89.5% were female, 89.8% had a bachelor’s degree, work experience ranged from less than 3 to more than 20 years with an average tenure of 14.7 years, 49.1% had a junior professional title; 83.3% were ordinary nurses, and 44.7% nurses additionally do the housework. This was consistent with the overall population structure of all nurses in the hospital.
Measures
To ensure the reliability and validity of variable measurement, the scales used in this study are all well-established scales that are widely used in the mainstream literature at home and abroad. At the same time, to improve the effectiveness of western scales in localization research in China, the measures were translated and back-translated from English into Mandarin Chinese to ensure accuracy, except for the measure of PWB subscale because it had a Chinese version with good reliability and validity (Brislin, 1980). Specially, the scale in this study was processed as follows: Firstly, the bilingual researchers conducted two-way translation on the English scale, and on this basis, the sentences with great differences from the original scale were corrected. Then, experts and scholars in related fields and enterprise employees were invited to evaluate and test the scale items, respectively. Finally, according to the feedback, the questions were further improved to form a Chinese version with both rigor and readability. All measures were rated using a six-point Likert scale ranging from 1 (strongly disagree) to 6 (strongly agree) to reduce the central tendency.
Surface acting: We utilized a five-item scale developed by Grandey (2003). Considering that the service target of nurses was patients, “customers” in the original scale was replaced by “patients” to suit the context. An example item is “I just pretend to have the emotions I need to display in my job.” Previous studies have provided evidence of the structural validity of the SA scale, with Cronbach’s α = .94 (Yam et al., 2016). In this study, Cronbach’s α for this scale was .86.
Perceived work support and family support: Zimet et al. (1988) developed a multidimensional scale of perceived social support, and differentiated three sources of it: family, friends, and a significant other. The family, friends, and significant others subscales demonstrated Cronbach’s α of .86, .84, and .80, respectively (Tonsing et al., 2012). Given that the working setting of the respondents, work and family support are the nurses’ primary sources of support, a sub-scale of “significant other” and family were applied in the study. A four-item scale of support from “significant other” was used to measure work support, and “significant other” in the original scale was replaced by “supervisor and coworker” to fit the context. An example item is “At work, there are supervisors and coworkers around when I am in need.” In this study, Cronbach’s α for the work support subscale was .91. A four-item scale of support from family was used to measure family support and included items such as “I get the emotional help and support I need from my family.” In this study, Cronbach’s α for the family support subscale was .89.
Job satisfaction: Job satisfaction was measured using Liu et al.’s (2007) three-item scale, one of which was reverse-scored. An example is: “In general, I do not like my job.” Research has demonstrated good internal consistency for the job satisfaction with Cronbach’s α = .82 (Liu et al., 2007). In this study, Cronbach’s α of the scale was .82.
Psychological well-being: We selected a six-item scale of PWB, a subscale of employee well-being developed by Zheng et al. (2015) to estimate nurses’ PWB, which was tested in the Chinese context and demonstrated good internal consistency and construct validity (Cronbach’s α = .88). It included items such as “In general, I am positive about myself and have self-confidence.” In this study, Cronbach’s α of the scale was .90.
Control variables: We controlled for several demographic variables as previous literature revealed that age, sex, professional title, position title, and family happiness are likely to influence individual PWB (Magee, 2015). In addition, the psychological sense of control was demonstrated to be associated with PWB (Brown, 2007); thus it was controlled.
Sense of control: A three-item scale, a subscale of Resilience scale developed by Connor & Davidson (2003), was used to measure employees’ psychological sense of control. Resilience is viewed as a measure of stress coping ability, and includes five subscales: personal competence, positive acceptance of change, sense of control, and other factors. An example item of sense of control is “I feel in control of my life.” Previous research has demonstrated good internal consistency for the personal sense of control with Cronbach’s α = .72 (Anderson & Bang, 2012). In this study, Cronbach’s α of the scale was .78.
Analytical Strategy
First, since our data was collected from one source (i.e., employees’ self-report), common method bias was thought to be a danger to our research conclusion. Thus Harman’s single factor analysis and confirmatory factor analysis (CFA) were conducted to examine the construct validity of the proposed model. Second, the structural path-analysis model (Figure 2) and the hypotheses were tested and analyzed using Mplus Version 7.4 (Muthén & Muthén, 2010). To probe for mediation and mediated moderation effects (i.e., H1, H4, and H5), we utilized the 95% bias corrected bootstrap confidence interval (CI) analyses with 5000 bootstrap samples to further inspect the statistical significance. Standardized parameter estimates for the full SEM model.
Single Factor Test
Before CFA, Harman’s single factor test was performed using SPSS 22.0 to examine whether common method bias existed in our study (Podsakoff et al., 2003). The results showed that the first factor accounted for 35.85% (far below the 50% mark), indicating common method bias was not a serious problem.
Confirmatory Factor Analysis
Confirmatory Factor Analysis of Study Factors.
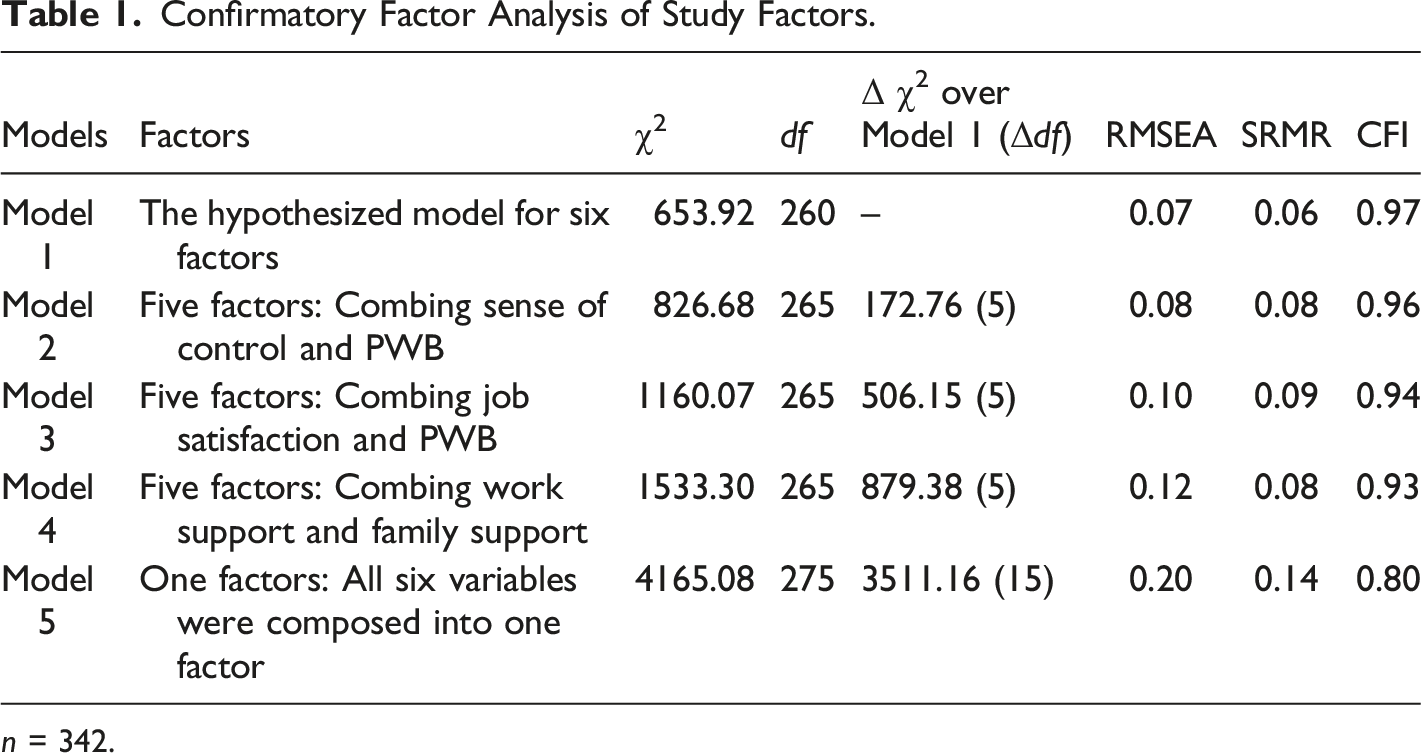
n = 342.
Results
Description
Means, Standard Deviations and Correlations.
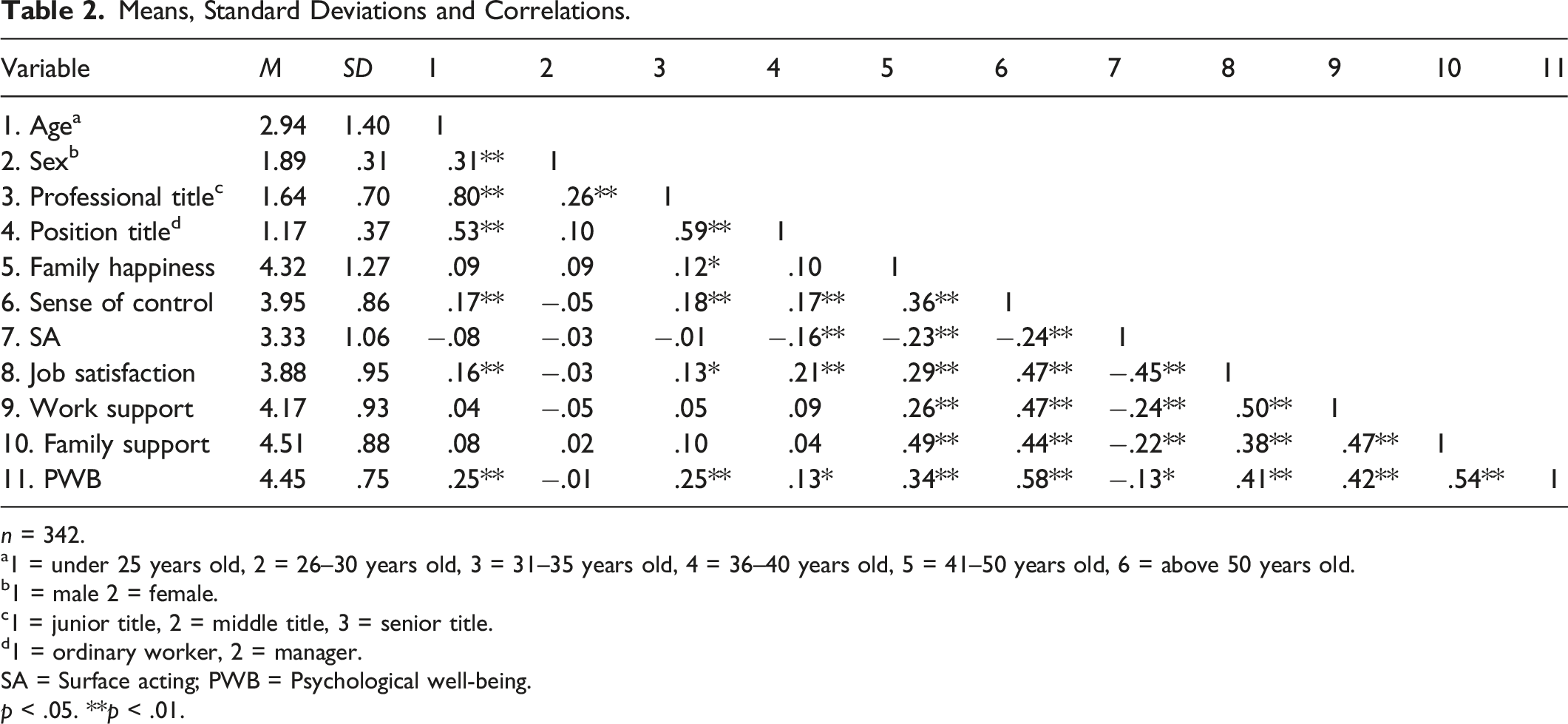
n = 342.
a1 = under 25 years old, 2 = 26–30 years old, 3 = 31–35 years old, 4 = 36–40 years old, 5 = 41–50 years old, 6 = above 50 years old.
b1 = male 2 = female.
c1 = junior title, 2 = middle title, 3 = senior title.
d1 = ordinary worker, 2 = manager.
SA = Surface acting; PWB = Psychological well-being.
p < .05. **p < .01.
Hypotheses Testing
The Mediation Effect of Job Satisfaction.

n = 342. *p < .05, **p < .01 SA = surface acting; JS = job satisfaction; PWB = psychological well-being.
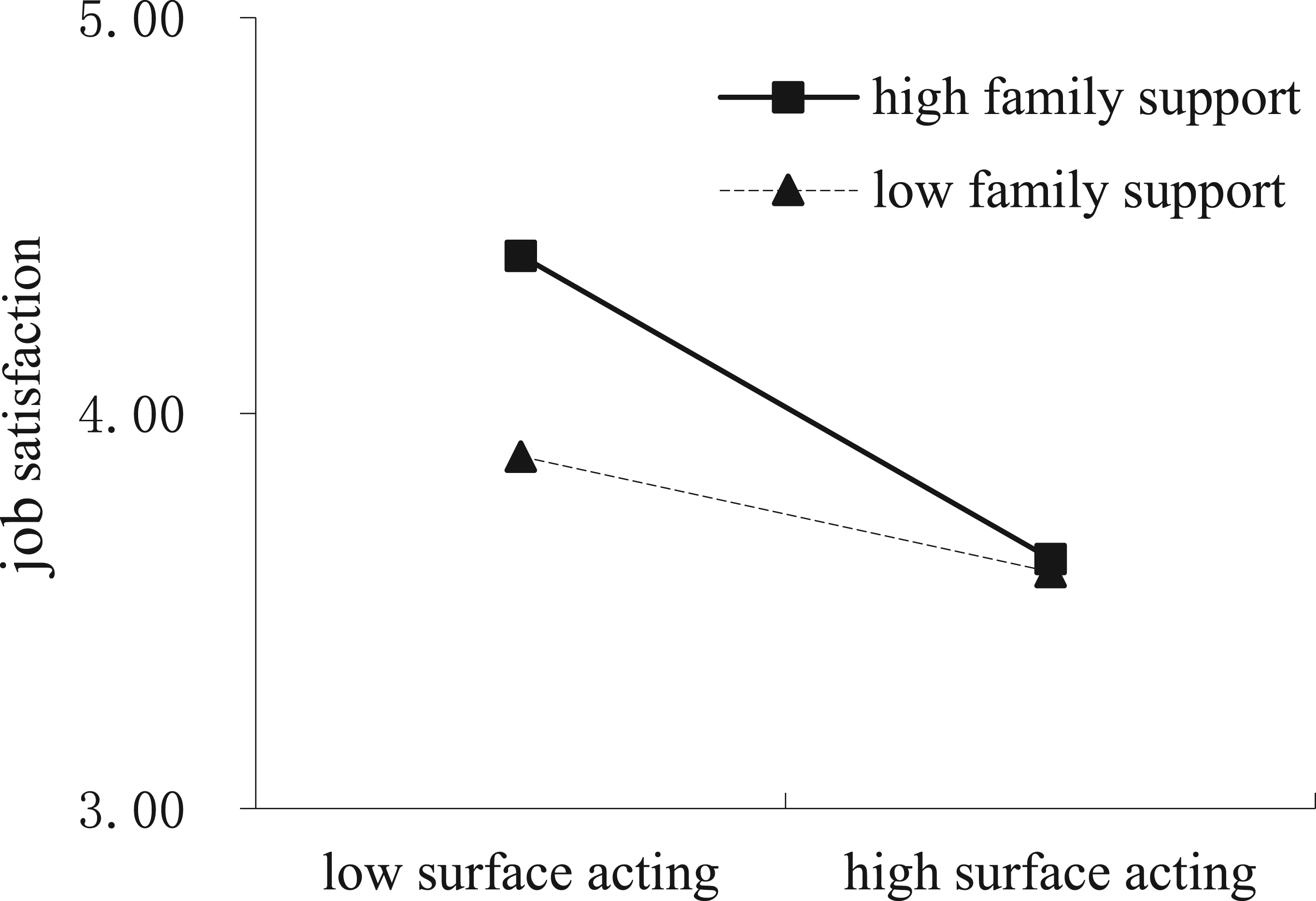
H2 and H3 proposed that work support and family support would moderate the relationship between SA and job satisfaction in different directions. Figure 2 provided the standardized coefficients in the moderated model. The results demonstrated that the negative relationship between SA and job satisfaction became significantly mitigated with the increase of work support (γ = .093, p < .05), and deteriorated with the increase of family support (γ = −.125, p < .05). The simple slopes displayed in Figures 3 and 4 further demonstrate it. That is, the relationship between SA and job satisfaction became stronger under low work support conditions (γ = −.371, p < .001) than high level of it (γ = −.185, ns), whereas it became weaker under low family support (γ = −.153, p < .05) rather than high family support conditions (γ = −.403, p < .001). In other words, work support and family support worked in opposite directions regarding the moderating role on the association between SA and job satisfaction. Then, the hypothesis 3 and 4 were fully supported. Moderating effect of work support on surface acting and job satisfaction. Moderating effect of family support on surface acting and job satisfaction.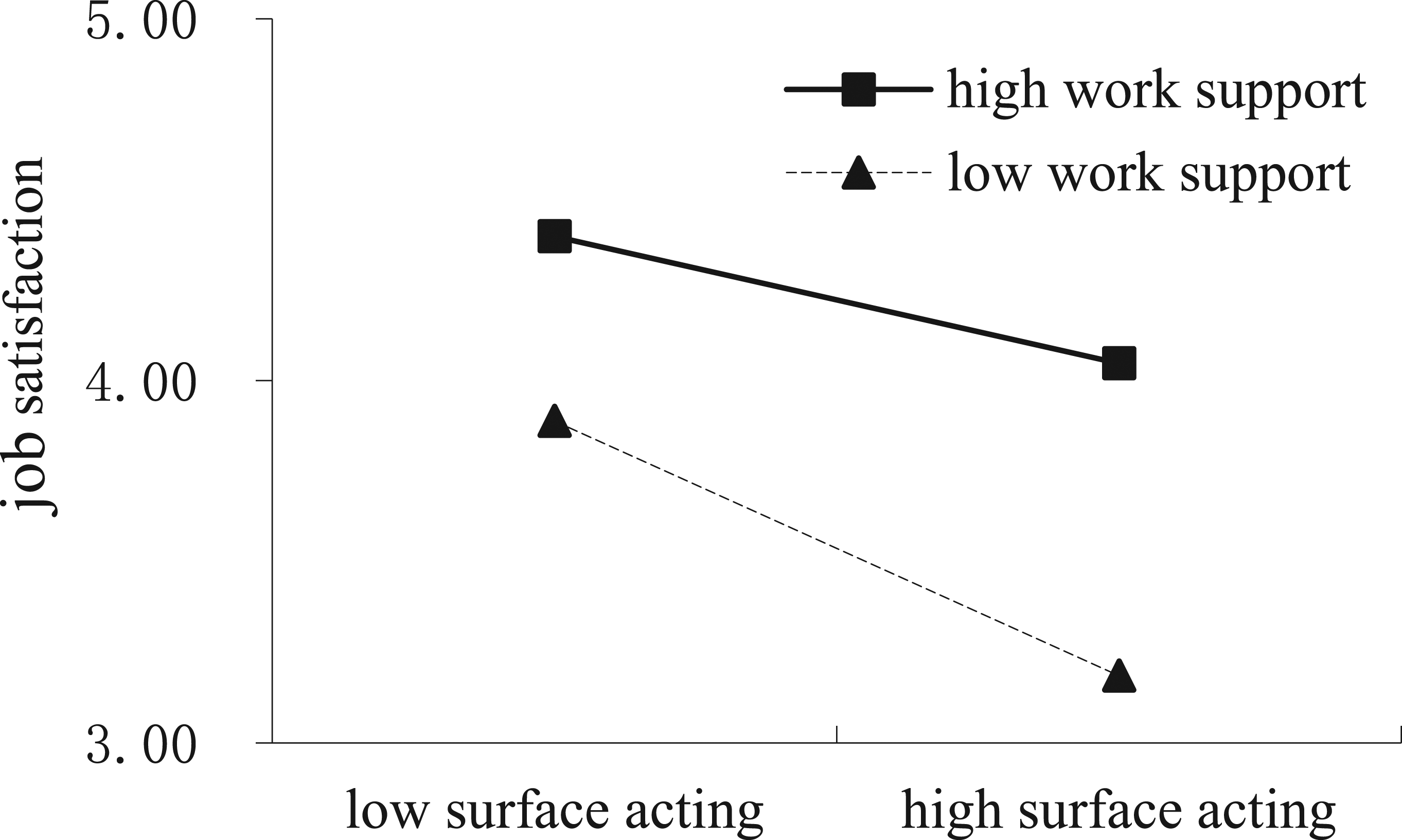
Conditional Effects of SA on PWB Through Job Satisfaction at Different Levels of Social Support.
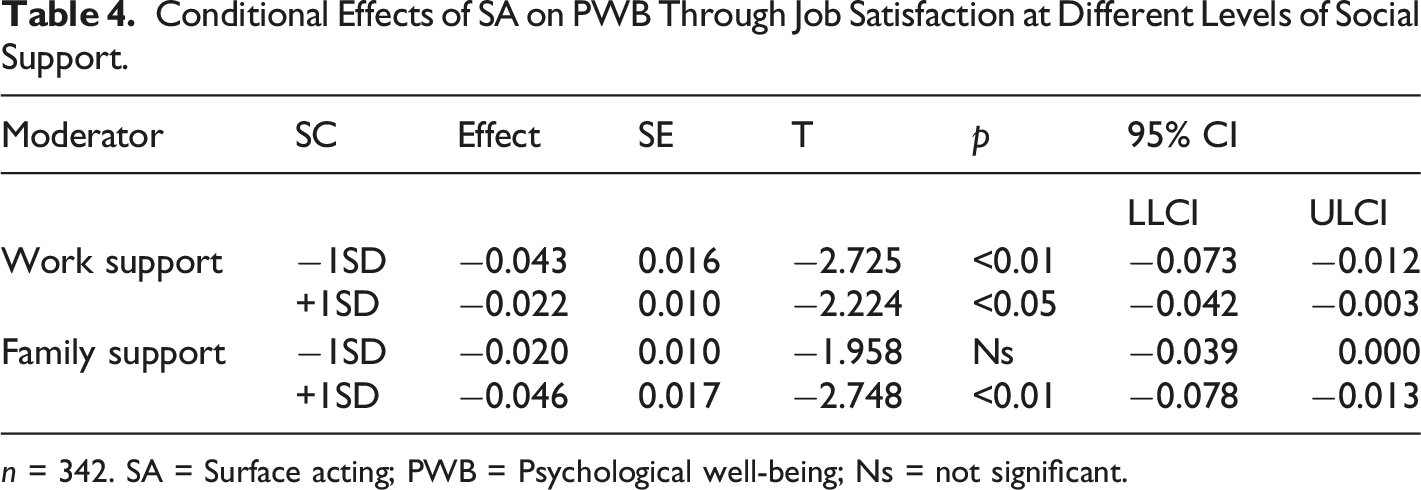
n = 342. SA = Surface acting; PWB = Psychological well-being; Ns = not significant.
Discussion
With SDT as the theoretical basis, SA was proved to exert negative influence on nurses’ PWB through their job satisfaction and such effects could be mitigated by work support and worsened by family support. The current study makes numerous important theoretical and practical contributions pertaining to how SA impacts job satisfaction and PWB and sheds light on how two types of social support could alleviate or aggravate the negative impacts.
Theoretical Implications
This study offers three theoretical contributions to the existing research.
First, by utilizing the self-determination perspective of emotional labor and employee outcome, this study explored how SA could impact PWB via job satisfaction. Prior research largely focused on resource-based theories to explore the negative effects of SA on employees’ well-being (Grandey & Melloy, 2017; Kinman et al., 2011; Uy et al., 2016); however, our research takes a person-centric perspective and verifies it in working nurses, in response to the appeal of the scholars to understand employees lived-through experiences from a subjective stance. Moreover, by examining the mediating role of job satisfaction, this study implies that PWB stems from satisfaction states of self-determination experienced by an individual at work that leads to life satisfaction, potential development, and personal growth.
Second, by integrating social support as a contextual element into the process of SA, job satisfaction and PWB, this study found the “double-edged” nature of social support. Specifically, the current study verified that the negative association between SA, job satisfaction, and PWB was weakened via work support and strengthened by family support. The positive role of work support between SA and outcomes has received wide support (Duke et al., 2009; Grandey & Melloy, 2017), and the negative role of family support was found in a few studies (Alcover et al., 2018; Lim & Lee, 2011). Our study has examined the different roles of work and family support simultaneously, and our findings provide empirical evidence for an in-depth exploration of these roles.
Finally, the current study disclosed the negative impact of family support among female nurses in China. In our study sample, female nurses accounted for nearly 90%, and 55.3% nurses reported that their family members did the housework, which may explain the stronger adverse effects of family support. One explanation may be that Chinese women are deemed to have the responsibility to undertake housework and care for their family whether they work outside the home or not (Judge & Livingston, 2008). Thus, more support from family would arouse their feelings of guilt for failing to fulfill family obligation and stimulate feelings of loss of psychological needs. The current study uncovered the dark side of family support, contributing to this area of the social support.
Practical Implications
Current study findings have important practical implications for management in organizations. First, nurses do not merely perceive, feel, and respond to their work passively, but actively shape their experiences from their own standpoint, thus managing employees’ perception that “self-determination is the key.” Since SA in the nurse’s work environment is inevitable, managers can adopt some strategies to compensate the perception of autonomy, competence, relatedness needs in other ways, such as providing more chance of self-expression, more training for job skill or emotional management ability, or more activities to enhance team bonding. Second, establishing a supportive or mutual assistance culture within the workplace, such as including instrumental and emotional supportive skills in training courses for managers and employees, plays an important buffering role when nurses experience high SA. Finally, for nurses, too much family support is not helpful to resist the negative influence of SA on PWB. In order to reduce the adverse effect of family support, some measures might be taken, such as maintaining a balance between work and family demands or keeping family support within a reasonable range. Moreover, when providing necessary support, it is important to offer support as equals, and help rather than act in a controlling or hijacking way, so employees could get substantial help from family members without their psychological needs being threatened.
Limitations and Future Directions
The current study has some limitations. First, this study collected homologous cross-sectional data at a certain time mode, which cannot precisely explain the dynamic causal process by which SA affects employees’ PWB through job satisfaction with varying social support. However, common method bias is not a serious problem because the results of the implementation of Harman’s single test and CFA results indicate good validity of the data from this study. Repeated validation can be performed in the future, using longitudinal studies or data from different sources. Second, in this study, SDT was used to explain the hypothesized mechanisms between SA and PWB, and yet, employees’ perception of self-determination has not been measured directly in this study. In the future, the perception of self-determination or the three types of psychological needs could be directly investigated to examine the changes after engaging in SA, and other mediating and moderating mechanisms could be explored more deeply. Third, the moderating role of social support should be further examined. In the current study, family support was found to fuel the negative relationship between SA, job satisfaction, and PWB; future research should investigate the role of family support with regard to different occupations, male respondents, and other cultural contexts.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.