
Abstract
From 2010 to 2023, the Smoking Cessation Leadership Center partnered with the Substance Abuse and Mental Health Services Administration to launch the State Leadership Academies (hereinafter, Leadership Academies) to address tobacco use in populations with behavioral health conditions in the United States. The Leadership Academies were a facilitated convening of leaders in tobacco control, behavioral health, and public health who were tasked with creating action plans to reduce the high rates of tobacco use in populations with behavioral health conditions in their states. State partners convened for a 2-day summit between 2010 and 2023, created an action plan, and, in the subsequent 3 to 5 years, implemented and evaluated the action plan in the areas of data, systems, education, or policy. Using a multimethods evaluation approach, we describe short-term outcomes (collaborations), intermediate outcomes (examples of integration of tobacco treatment and policy), and long-term outcomes (decline in tobacco use prevalence) of the Leadership Academies, focusing on 4 state case studies. The case studies highlighted unique partnerships, impactful strategies, the harnessing of state-level infrastructure, and the importance of political will to achieve state-level reductions in tobacco use in populations with behavioral health conditions. The 4 states showed a mean decline of 5.2% in smoking prevalence among people with frequent poor mental health and 6.2% among people with heavy drinking during their Leadership Academy tenure. The case demonstrated the importance of cross-sector collaboration, leadership buy-in, and the creation of sustainable funding structures to support the scaling up of promising projects. Leadership Academies were an effective engagement model to reduce the prevalence of tobacco use in populations with behavioral health conditions.
Keywords
In 2021, an estimated 28.3 million people in the United States (11.5%) reported current smoking,1,2 contributing to more than 490 000 deaths annually. 2 Tobacco use is disproportionately concentrated among people with behavioral health conditions (ie, mental health and/or substance use disorders).3-5 Almost half (>200 000) of deaths due to tobacco use occur among people with behavioral health conditions, making this population, which already has a reduced lifespan,2,5 in need of further support to alleviate the physical and behavioral health burden of tobacco use. 5
Mental health and substance use disorders are widespread in the United States. In 2022, 23.1% of adults aged ≥18 years had any mental illness, 17.3% had a substance use disorder, 32.9% had either a mental illness or a substance use disorder, and 8.4% had both. 6 Data from the 2006-2019 National Survey on Drug Use and Health showed that rates of past-month cigarette smoking were nearly double among those with major depressive episodes than among those without major depressive episodes (30.5% vs 18.7%). 4 The differences in rates were even more drastic among those with substance use disorders: 58% of people with substance use disorders versus 19% of people without substance use disorders reported smoking in the last month. 4 During this same 15-year period, past-month cigarette smoking declined from 37.3% to 24.2% among those with a major depressive disorder and from 46.5% to 35.8% among those with a substance use disorder. 4
Although rates of smoking are declining in the population with behavioral health conditions, 4 the absolute difference in smoking rates between people with and without behavioral health conditions has not narrowed significantly. 4 Even among people with behavioral health conditions, further gaps exist by socioeconomic status, race and ethnicity, educational attainment, and involvement with the criminal/legal system. 7 Differences exist by sociodemographic characteristics and by state. The prevalence of adults with any mental illness ranged from 11.7% in Utah to 42.1% in Louisiana, with a median of 24.7% in South Carolina. 7 These individual and population trends in tobacco use in populations with behavioral health conditions highlight a need for renewed efforts to promote cessation and cessation-focused tobacco control policies. 7
Several myths have perpetuated the use of tobacco in populations with behavioral health conditions. The “self-medication hypothesis” posited by the tobacco industry suggested that people with behavioral health conditions smoke to alleviate their mental health symptoms. 8 The tobacco industry has consistently funded research to support these and other findings that quitting smoking is detrimental to patients’ mental health. 5 These theories were subsequently perpetuated by health care providers who believed that tobacco use was beneficial in treating their patients’ mental health conditions.5,9 In addition to targeted marketing and health care provider beliefs, systems-level barriers to tobacco cessation (eg, lack of access to tobacco treatment) exist among behavioral health populations. 10 In 2023, only 14 states had enacted laws to support policies on tobacco treatment and tobacco-free grounds in mental health and substance use treatment facilities. 10
The elevated smoking rates among populations with behavioral health conditions and the importance of addressing tobacco use to improve behavioral health prompted the Smoking Cessation Leadership Center (SCLC) to develop the State Leadership Academies (hereinafter, Leadership Academies) model.11,12 Implemented in 25 states, the Leadership Academies were launched to create collaborations in individual states among mental health, substance use, and public health departments as well as tobacco control groups to reduce tobacco use among their populations with behavioral health conditions.11,12 With support from the Substance Abuse and Mental Health Services Administration (SAMHSA), SCLC hosted 2-day Leadership Academy summits between 2010 and 2023 that used the performance partnership model, 13 which provided a framework for states to (1) identify the current state of tobacco use, (2) develop goals for reducing tobacco use, (3) identify strategies to achieve these goals, and (4) determine outcomes and process measures to evaluate their success.11,12 The approach, impact, and evaluation of the Leadership Academies model are described elsewhere. 11 In this article, we describe 4 case studies that provide shared lessons for cross-collaboration across behavioral health, public health, and tobacco control to reduce tobacco use in populations with behavioral health conditions.
Purpose
The purpose of these case studies is to share lessons learned from collaborations among state mental health and substance use treatment services, tobacco control programs, and public health to reduce the state prevalence of tobacco use in populations with behavioral health conditions.
Methods
Leadership Academies Procedures
The Leadership Academies began as a joint effort in 2010 between SAMHSA and the SCLC. 12 With funding from SAMHSA combined with the SCLC’s experience with leading leadership summits, expertise in tobacco technical assistance, and wide-ranging curricula and toolkits, SCLC convened Leadership Academy summits in 25 states from 2010 through 2023 (Figure 1). 11 SCLC funded the Leadership Academies until 2018. From 2018 to 2023, SCLC was awarded funding from SAMHSA to be the first National Center of Excellence for Tobacco-Free Recovery. 11 We highlight 4 states as case studies to share lessons on reducing tobacco use prevalence in populations with behavioral health conditions. These case studies exemplified the partnerships, strategies, state-level infrastructure, and political will necessary to achieve state-level reductions in tobacco use in populations with behavioral health conditions. The project was considered exempt by the University of California Institutional Review Board (IRB) because this work did not involve collecting identifiable information from study participants and because it was conducted as part of a large public health project (IRB no. 23-39017).
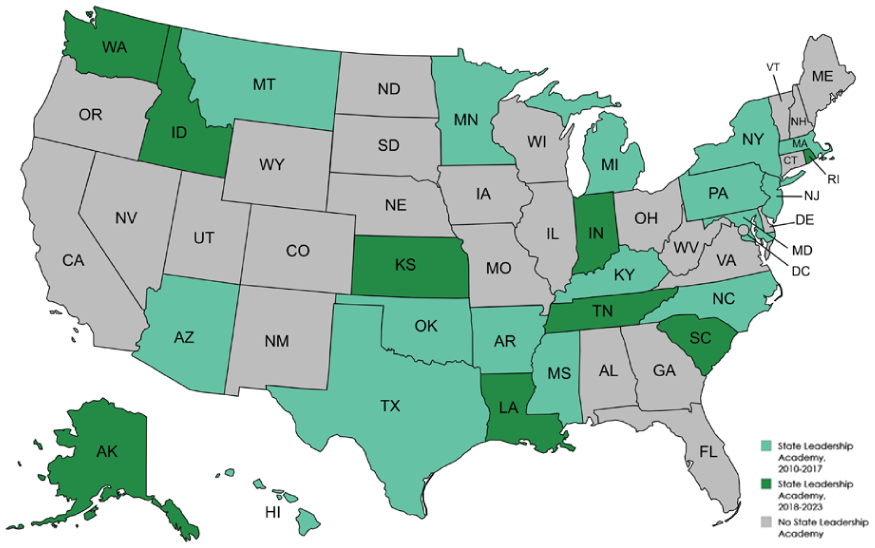
States with and without State Leadership Academies, United States, 2010-2023. From 2010 to 2023, the Smoking Cessation Leadership Center partnered with the Substance Abuse and Mental Health Services Administration to launch the State Leadership Academies to address tobacco use in populations with behavioral health conditions in the United States.
Implementation Framework for the Leadership Academies
We invited states to apply to be a Leadership Academy state and selected states that had a high prevalence of tobacco use and leadership support to expand their tobacco control efforts. 12 Each Leadership Academy summit involved a diverse group of 30 to 40 officials from state public health, mental health, and substance use; health care; and government agencies that had not previously collaborated.11,12 Throughout the 2-day summit, we used the performance partnership model to support Leadership Academy states to develop an action plan to reduce tobacco use for their state. Action plans focused on the domains of health systems change to promote tobacco treatment, policies to reduce tobacco use, educational resources for the tobacco treatment workforce, and data to monitor progress and roadblocks. 11 The performance partnership model, a leadership action model, involved taking a group through 4 simple questions: (1) Where are we now (baseline)?, (2) Where do we want to be (target)?, (3) How will we get there? (action plan with multiple strategies), and (4) How will we know we are getting there? (the impact and measurement plan). 13 To operationalize this model, we asked Leadership Academy participants to work through a 4-step process to identify (1) the baseline prevalence of behavioral health conditions and tobacco use in their state, (2) their target reduction in tobacco use among their population with behavioral health conditions, (3) an action plan to achieve the goal, and (4) ways to quantify the impact of the strategies implemented. 11 The Leadership Academy state planning committees used data from the Behavioral Risk Factor Surveillance System (BRFSS) to evaluate their baseline prevalence of tobacco use among people with behavioral health conditions. States then used BRFSS data to identify 5-year target reductions in tobacco use prevalence in 2 populations: those with frequent poor mental health and those with heavy drinking. 14
In addition to hosting the 2-day Leadership Academy summit, SCLC supported states to implement their action plans by providing administrative support and technical assistance through curricula, assessing roadblocks, monitoring progress, and facilitating collaborations. 12 SCLC provided telephone, online, and in-person technical assistance to states for up to 3 years after the summit. SCLC maintained an active website of resources, toolkits, and webinars. 11 An SCLC website dashboard provided a view of state-level progress on reducing the prevalence of cigarette smoking relative to their set target and to other states.
Data Sources
We used a multimethods approach, including narrative progress surveys from state Leadership Academy participants and BRFSS tobacco use prevalence estimates, to evaluate the Leadership Academy model. 11 The populations under study included both Leadership Academy participants and the populations with frequent poor mental health and heavy drinking in each of the 4 case study states. Our short-term process outcome in the first 2 years of the summit was the total number of new cross-sector collaborations. Intermediate outcomes within 2 to 4 years of the state summit were initiatives in systems change, policy implementation, educational efforts, or the use of data to reach priority populations. The long-term outcome for the 5 years after the summit was a reduction in the prevalence of tobacco use among those with heavy drinking and frequent poor mental health, as demonstrated by BRFSS data.
Data Analysis
We reported proportions for process outcomes. We provided a narrative description of intermediate outcomes using data from the narrative progress surveys related to systems change, policy implementation, or educational efforts for each case study. We used BRFSS data to report the unadjusted, population-weighted prevalence of tobacco use at baseline and 5-year follow-up for each state. We reported the mean decline in smoking prevalence between baseline and 5-year follow-up.
Outcomes
Short-Term Outcomes
During the duration of the project, SCLC facilitated collaborations among 2773 organizations in the 25 Leadership Academy states that coordinated and/or shared resources because of the grant. Among the 7 states that hosted a Leadership Academy summit during the 5-year SAMHSA grant, attendees represented the following areas: 16.5% in tobacco control, 32.4% in public health, 30.2% in mental health, 14.4% in substance use, and 6.5% in government.
Intermediate Outcomes
Case study 1: Gap nicotine replacement therapy project
Prior to the summit, case study 1 had adopted policies on tobacco-free grounds in its behavioral health facilities and had leadership support from the Department of Mental Health and Substance Use Services to move toward a wellness-focused policy on tobacco use. The state used the momentum from the summit, including new partnerships among behavioral health departments, public health departments, and state quitlines, to promote systems-level access to tobacco treatment. Case study 1 implemented and evaluated a program to increase nicotine replacement therapy (NRT) coverage in residential drug treatment programs. A project that had initially started in 14 residential drug treatment programs expanded to all residential drug treatment programs in the state by the end of the Leadership Academy’s 5-year program. The gap NRT project enhanced tobacco treatment support in crisis and inpatient programs as well as residential treatment programs, with the goal of integrating these services into existing substance use programming. This state added a new data measure on tobacco use for residents in residential drug treatment programs at intake, during treatment, and at discharge. By providing access to NRT, they also increased referrals to the state telephone quitline and addressed delays in accessing treatment after discharge. The State Tobacco Settlement funds paid for this initiative, and these funds were allocated to state mental health and substance use services, allowing them to purchase NRT to cover residents when they first entered the facility and after discharge into the community. The state evaluation of the initiative between 2018 through 2019 demonstrated that it was able to reach 2032 clients in residential drug treatment, and of those, 772 (38.0%) residents attempted to quit or reduce tobacco use, and 642 (31.6%) residents self-reported they were able to quit completely.
Case study 2: State tobacco-free mental health clinics
Case study 2 obtained information on organizational priorities for addressing tobacco use among state behavioral health facilities and identified tobacco-free policies as a focus for the state. It worked with the state Department of Mental Health to implement and support a tobacco-free campus for all its statewide community mental health clinics. State leaders established champions in community mental health clinics, setting a target timeline for policy implementation. Mental health clinic leadership was involved at all levels of the policy change, providing treatment resources and incentives to quit smoking for staff, promotional materials, and signage for each facility. Patients in mental health clinics were linked with resources for cessation through their state quitline and offered free NRT (patches, gum, lozenges). Case study 2 also linked tobacco treatment with the State Opioid Response grant program in counties that had a high prevalence of tobacco use and opioid use disorder through a pilot program that made NRT available in those county facilities.
Case study 3: Expansion of tobacco cessation services and policies in managed care organizations
Following its Leadership Academy summit, case study 3 expanded its tobacco-free campus policies and tobacco treatment services among Medicaid managed care organizations (MCOs). These efforts began with a policy restricting the use of any tobacco in any state-operated health facility. To support policy implementation, the state launched the Change for Life: Tobacco Free Recovery Initiative Campaign, a collaboration between local behavioral health and public health leaders. From 2016 through 2023, 15 agency-wide tobacco-free policies were adopted, covering more than 100 000 clients and staff in state MCOs. In 2022, tobacco-free campuses were required in most Medicaid provider contracts, covering most behavioral health providers in the state. MCOs were also mandated to provide screening, promotion, training, and referrals to quitline services. This state worked with organizations such as the National Alliance on Mental Illness to bring about awareness on addressing tobacco use and behavioral health, increasing the promotion of fax referrals to state quitline services.
Case study 4: State interagency collaboration to create a funding program for state behavioral health facilities
At the time of the Leadership Academy Summit, case study 4 had already established a Tobacco Prevention and Cessation Commission in response to high rates of tobacco use in its populations with behavioral health conditions and a state focus on substance use prevention and treatment. Case study 4 formalized a memorandum of understanding between the state tobacco control program and its mental health and addiction services to foster ongoing collaboration. The behavioral health department created a funding program and released a request for applications to fund and support state behavioral health facilities to adopt tobacco treatment and tobacco-free policies in their facilities. The state tobacco program offered technical assistance to those facilities selected for funding and provided guidance on metrics as well as resources to provide tobacco treatment and tobacco-free grounds policies.
Long-Term Outcomes
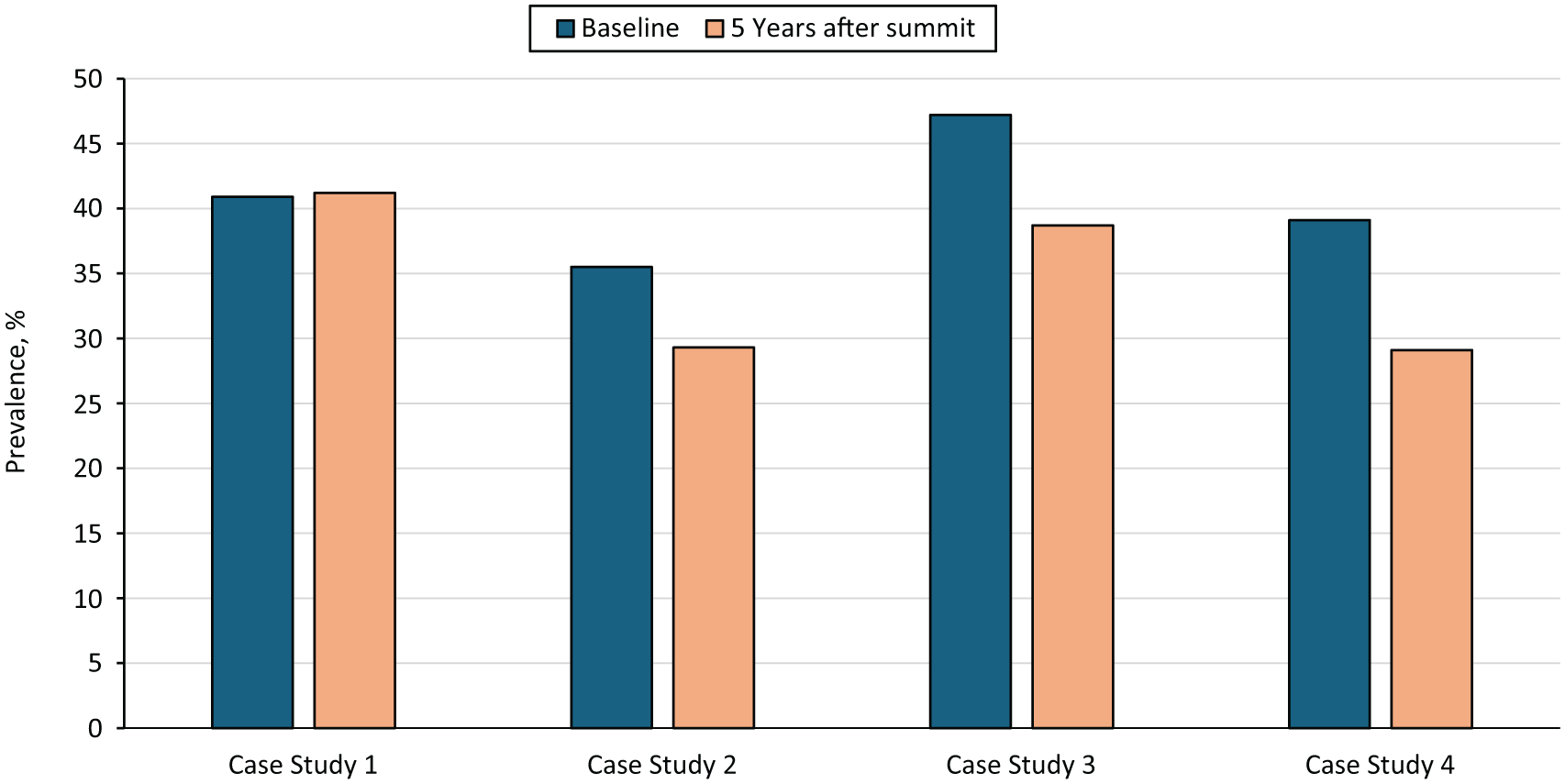
The 4 states showed a mean decline in smoking prevalence among adults with frequent poor mental health and heavy drinking during their Leadership Academy tenure. Across states, the mean unadjusted decline in tobacco use prevalence among adults with frequent poor mental health was 5.2 percentage points (Figure 2), and the mean unadjusted decline in tobacco use prevalence among adults with heavy drinking was 6.1 percentage points (Figure 3). Case study 4 had a 10.4 percentage-point decline in smoking prevalence among adults with frequent poor mental health and a 10.0 percentage-point decline among adults with heavy drinking during the study period. In case studies 2 and 3, the percentage-point decline in cigarette smoking among adults with heavy drinking was larger than among adults with frequent poor mental health. Case study 1 did not see a percentage-point decline in the prevalence of smoking among adults with heavy drinking.

Prevalence of cigarette smoking among people with frequent poor mental health at baseline and 5 years after the State Leadership Academy Summit, Behavioral Risk Factor Surveillance System, 2010-2023. 14 From 2010 to 2023, the Smoking Cessation Leadership Center partnered with the Substance Abuse and Mental Health Services Administration to launch the State Leadership Academies to address tobacco use in populations with behavioral health conditions in the United States.
Prevalence of cigarette smoking among people with heavy drinking at baseline and 5 years after the Leadership Academy Summit, Behavioral Risk Factor Surveillance System, 2010-2023. 14 From 2010 to 2023, the Smoking Cessation Leadership Center partnered with the Substance Abuse and Mental Health Services Administration to launch the State Leadership Academies to address tobacco use in populations with behavioral health conditions in the United States.
Lessons Learned
The Leadership Academy model supported states to bridge gaps in access to tobacco treatment, expanded tobacco-free policy implementation in state behavioral health facilities, and yielded important lessons. However, we acknowledge a limitation. We were unable to draw causal inferences between participating in the Leadership Academies and declines in the state prevalence of tobacco use. Declines could have been due to secular trends. 11
Collaboration Across Disciplines
The model supported and fostered cross-sector collaboration between tobacco control and behavioral health officials, raising awareness of the high rates of tobacco use in the population with behavioral health conditions and mobilizing state resources to reduce the prevalence of tobacco use. The 4 case studies demonstrated that these cross-sector collaborations led to sustained implementation of projects that supported the delivery of tobacco treatment and/or implementation of tobacco-free policies in health care and behavioral health settings. These collaborations were particularly important for leveraging shared resources, including staff and funding resources for the integration of tobacco treatment in behavioral health and primary care settings.
Need for Leadership Buy-in and Champions
Leadership buy-in and state champions were essential components to advance state tobacco control initiatives, particularly in the face of competing funding priorities, political shifts, and staff and leadership turnover in state public health and behavioral health agencies. The Leadership Academies’ 2-day summits were often launched by senior public health and behavioral health state officials, signaling the importance of reducing tobacco use as a state priority. The leaders also normalized and championed the link between tobacco use and behavioral health, setting the agenda and tone for the meeting, which was a motivating factor for frontline staff leading tobacco control efforts in facilities.
Sustainability
Through this work, we recognized the importance of building sustainable systems that can support ongoing efforts to reduce the state-level prevalence of tobacco use, even in the face of shifting political priorities, limited funding, and changes in staffing or leadership. The case studies presented in this article serve as models of successful implementation of tobacco treatment and tobacco control programs, particularly in states that are facing challenges to prioritizing tobacco control efforts.
Footnotes
Acknowledgements
The University of California, San Francisco, Smoking Cessation Leadership Center thanks its state partners; officials from state public health, behavioral health, tobacco control, health care, and government; and participants for their contribution to this work during the past 13 years.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Robert Wood Johnson Foundation and the Substance Abuse and Mental Health Services Administration (grant no. H79SM080950). A version of this work was presented at the Annual Society of General Internal Medicine Conference, Hollywood, Florida, May 2025, and at the National Conference on Tobacco or Health, Chicago, Illinois, August 27, 2025.