
Abstract
Objective:
Few studies have examined the mental health burden faced by working parents. We assessed the prevalence of fair or poor self-reported mental health and identified desired workplace improvements among US working parents.
Methods:
We conducted a descriptive analysis of the 2024 SummerStyles survey, a nationally representative web-based panel survey of US adults aged ≥18 years. Working parents were defined as adults employed full- or part-time with ≥1 child aged <18 years. We calculated weighted percentages and 95% CIs to characterize mental health status and workplace priorities across demographic and occupational groups.
Results:
Among 1201 working parents, 15.3% (weighted n = 126) reported fair or poor mental health. The prevalence of self-reported fair or poor mental health was higher among women than among men (20.0% vs 11.4%), among those with lower annual household income (<$25 000: 31.6%) versus higher annual household income ($25 000-$49 999: 20.1%; $50 000-$99 999: 19.6%; >$100 000: 10.0%), among those with less versus more educational attainment (high school graduate or less: 20.2%; some college: 20.0%; ≥bachelor’s degree: 10.9%), and among those with retail/stores/shopping jobs (26.8%) versus jobs in other industries (health care: 20.4%; education and tutoring: 8.0%; professional, scientific, technical, and business services: 11.4%; finance, banking, and health insurance: 10.2%). Desired workplace improvements included increased paid leave (20%), ability to work remotely/telework (20%), and flexible work schedules (19%), with differences by demographic and occupational characteristics.
Conclusions:
Tailored workplace policies, such as flexible scheduling and expanded leave benefits, may support the mental health of US working parents. Additional research should explore industry-specific nuances of preferred workplace flexibilities among US working parents to guide work-based interventions.
Research has independently documented the mental health burdens experienced by parents 1 and workers, 2 including elevated stress, anxiety, and burnout. Workers in high-stress industries (eg, health care) face increased risks of anxiety and depression, while parents often report elevated stress potentially due to caregiving demands, highlighting the need to investigate how these roles intersect in the lives of contemporary working parents.3,4 This dual role often creates compounding stressors, exacerbating mental health challenges for individuals who must balance overlapping responsibilities.
Research on work-related psychosocial exposures has consistently linked factors such as job strain, low autonomy, and lack of support with adverse mental health outcomes. 5 Within this body of literature, the experience of working parents is often touched upon through the lens of work–family conflict, a well-established concept defined as “a form of interrole conflict in which the role pressures from the work and family domains are mutually incompatible in some respect.” 6 While some studies control for parental status7-9 or examine it as a moderating variable,10,11 few studies have characterized the mental health burden faced by working parents. This gap in the literature is critical because understanding working parents as a distinct population is essential for developing targeted interventions and supportive workplace policies.
This gap in understanding is especially relevant in the wake of the COVID-19 pandemic, which intensified household–career conflicts and highlighted the need for flexible, family-supportive work environments.12,13 Prior studies show that job flexibility, paid leave, and supportive culture can improve employee well-being,14-16 but less is known about how working parents prioritize these options. Furthermore, little nationally representative data exist to describe mental health status or workplace needs among working parents across industries and income groups.
In August 2024, the US Surgeon General issued an advisory on mental health and well-being among parents, highlighting the critical need to address mental health challenges faced by this population and underscoring the importance of workplace flexibilities and support systems to mitigate these challenges. 17 Addressing this need requires timely, detailed data on the experiences and preferences of working parents.
We conducted a descriptive analysis of data from the 2024 SummerStyles survey, 18 estimated the prevalence of fair or poor self-rated mental health among working US adults, and identified the single workplace change working parents would consider most beneficial.
Methods
We analyzed data from the 2024 SummerStyles survey, 18 a web-based survey administered in English to a nationally representative panel of US adults aged ≥18 years. The panel is recruited and maintained by Porter Novelli via Ipsos’ KnowledgePanel, which uses address-based sampling to ensure national representativeness. 18 Survey weights adjust for sex, age, race and ethnicity, education, and annual household income based on US Census Current Population Survey benchmarks. 19 Data were collected in June 2024, and the response rate was 76.3%. The SummerStyles dataset is proprietary but can be made available to academic or public health researchers through a data-use agreement with Porter Novelli.
Of 4371 survey respondents, we excluded participants who reported they were not employed full- or part-time (n = 1606) and who did not report parental status (n = 3). The final analytic sample included 2762 employed respondents, comprising 1201 working parents (defined as adults employed full- or part-time with ≥1 child aged <18 y in the household) and 1561 nonparent workers. The primary analyses focused on working parents; however, we made comparisons between parent and nonparent workers to contextualize the findings. We excluded respondents who selected “I am not a working parent” from the analysis of desired workplace improvements, which was limited to working parents.
We included 2 survey questions in the analysis. A total of 1201 working parents were asked, “What would be the most beneficial change at your workplace?” Response options included access to affordable, on-site childcare; ability to work remotely/telework; flexible work schedule (days and/or times); fewer work hours (part-time, 35-hour week); more paid time off; and a more supportive workplace culture. All participants were asked, “In general, how would you rate your mental health, including your mood and your ability to think?” Response options were excellent, very good, good, fair, or poor. For analysis, we categorized self-reported mental health into fair or poor and good/very good/excellent.
We performed descriptive analyses for all outcomes stratified by sex (male, female), age group (18-29, 30-44, 45-49, ≥60 y, missing/refused), race and ethnicity (Hispanic, non-Hispanic Black, non-Hispanic ≥2 races, non-Hispanic White, non-Hispanic Other), marital status (married, not married, missing/refused), education level (high school graduate or less, some college, bachelor’s degree or higher, missing/refused), annual household income (<$25 000, $25 000-$49 999, $50 000-$99 999, ≥$100 000), industry (health care; education and tutoring; professional, scientific, technical, and business services; retail/stores/shopping [including online retail]; finance, banking, and health insurance; missing/refused), and age of youngest child (≤6, >6 y). We calculated weighted percentages and 95% CIs using SAS version 9.4 (SAS Institute Inc). We designed this analysis as a descriptive, hypothesis-generating study. Rather than modeling relationships between variables, we sought to summarize subgroup patterns in mental health status and workplace needs among US working parents. We did not conduct hypothesis tests or multivariable models to avoid the risk of overinterpreting exploratory comparisons as causal. 16 The study objective was to summarize patterns across subgroups and highlight potential disparities in self-reported mental health and workplace needs, providing a foundation for future inferential studies. This activity was reviewed by the Centers for Disease Control and Prevention, deemed not research involving human subjects, and was conducted consistent with applicable federal law and Centers for Disease Control and Prevention policy (see eg, 45 CFR part 46, 21 CFR part 56; 42 USC §241[d]; 5 USC §552a; 44 USC §3501 et seq).
Results
Population Characteristics
Among 1201 working parents who participated in the 2024 SummerStyles survey, approximately 47.1% were male and 46.2% were female (eTable 1 in the Supplement). Most respondents were aged 30 to 44 years (56.5%), non-Hispanic White (55.9%), married (72.2%), and held a bachelor’s degree or higher (52.1%). More than half (53.9%) reported an annual household income of ≥$100 000. A greater proportion of working parents reported having children aged >6 years versus ≤6 years (51.3% vs 48.0%). The largest proportion of working parents worked in the health care industry (14.6%), followed by education and tutoring (11.1%), and professional, scientific, technical, and business services (10.7%). Overall, 15.3% (n = 162) of working parents reported their mental health as fair or poor (Table 1).
Prevalence of fair or poor self-reported mental health among workers (N = 358), by parental status (parent vs nonparent) and selected demographic characteristics, Porter Novelli SummerStyles, United States, 2024 a
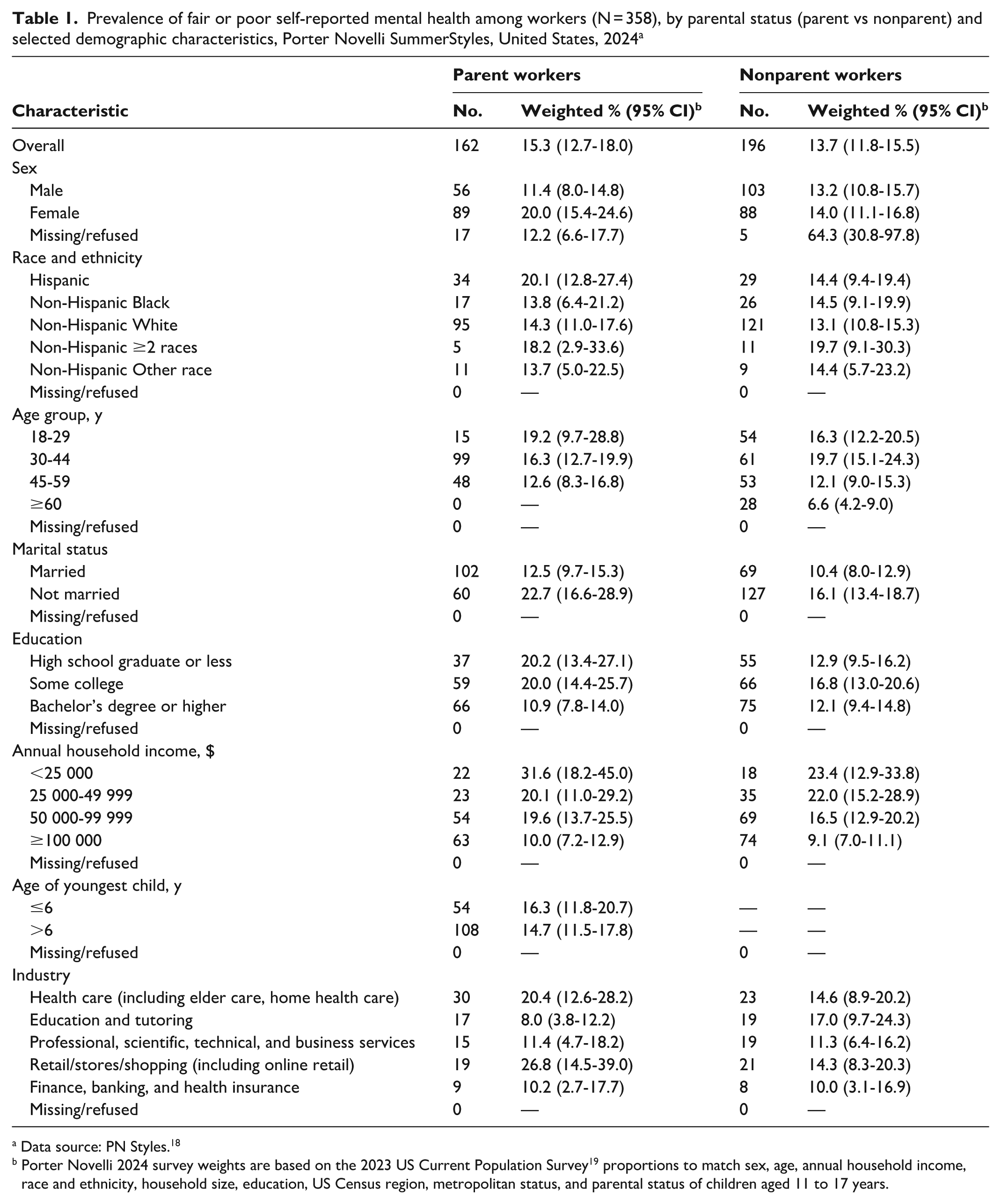
Data source: PN Styles. 18
Porter Novelli 2024 survey weights are based on the 2023 US Current Population Survey 19 proportions to match sex, age, annual household income, race and ethnicity, household size, education, US Census region, metropolitan status, and parental status of children aged 11 to 17 years.
Self-Reported Mental Health by Demographic and Occupational Characteristics
Among working parents, the prevalence of fair or poor mental health was higher among women (20.0%; 95% CI, 15.4%-24.6%) than among men (11.4%; 95% CI, 11.1%-16.8%) (Table 1). The prevalence of fair or poor mental health was also higher among working parents with lower annual household income (<$25 000: 31.6%; $25 000-$49 999: 20.1%) than among parents with higher annual household income (≥$100 000: 10.0%).
By industry, the prevalence of self-reported fair or poor mental health was highest among working parents in the retail/stores/shopping industry (26.8%), followed by parents in health care (20.4%), and professional, scientific, technical, and business services (11.4%) (Table 1).
The prevalence of self-reported fair or poor mental health was similar between parent workers (15.3%) and nonparent workers (13.7%) overall, as well as across most selected demographic characteristics (Table 1). However, female parent workers had a higher prevalence of fair or poor mental health (20.0%) than male parent workers (11.4%), whereas among nonparent workers, the difference by sex was smaller (14.0% among women vs 13.2% among men). Similarly, working parents with the lowest educational attainment reported a higher prevalence of fair or poor mental health (≤high school graduate: 20.2%) than working parents with the highest educational attainment (≥bachelor’s degree: 10.9%). By contrast, among nonparent workers, the prevalence of self-reported fair or poor mental health was more similar by education level (12.9% for ≤high school graduate and 12.1% for ≥bachelor’s degree).
Desired Workplace Improvements
More paid time off (20%), the ability to work remotely/telework (20%), and flexible work schedules (19%) were the most identified beneficial workplace changes among working parents (Table 2). More paid time off was the most selected option among female working parents (21%), whereas the ability to work remotely/telework was the most selected by male working parents (23%). Working parents with annual household incomes <$50 000 reported a greater need for flexible work schedules (27%) and more paid time off (28%) than working parents with annual household income ≥$100 000 (flexible schedules: 17.2%; paid leave: 16.4%).
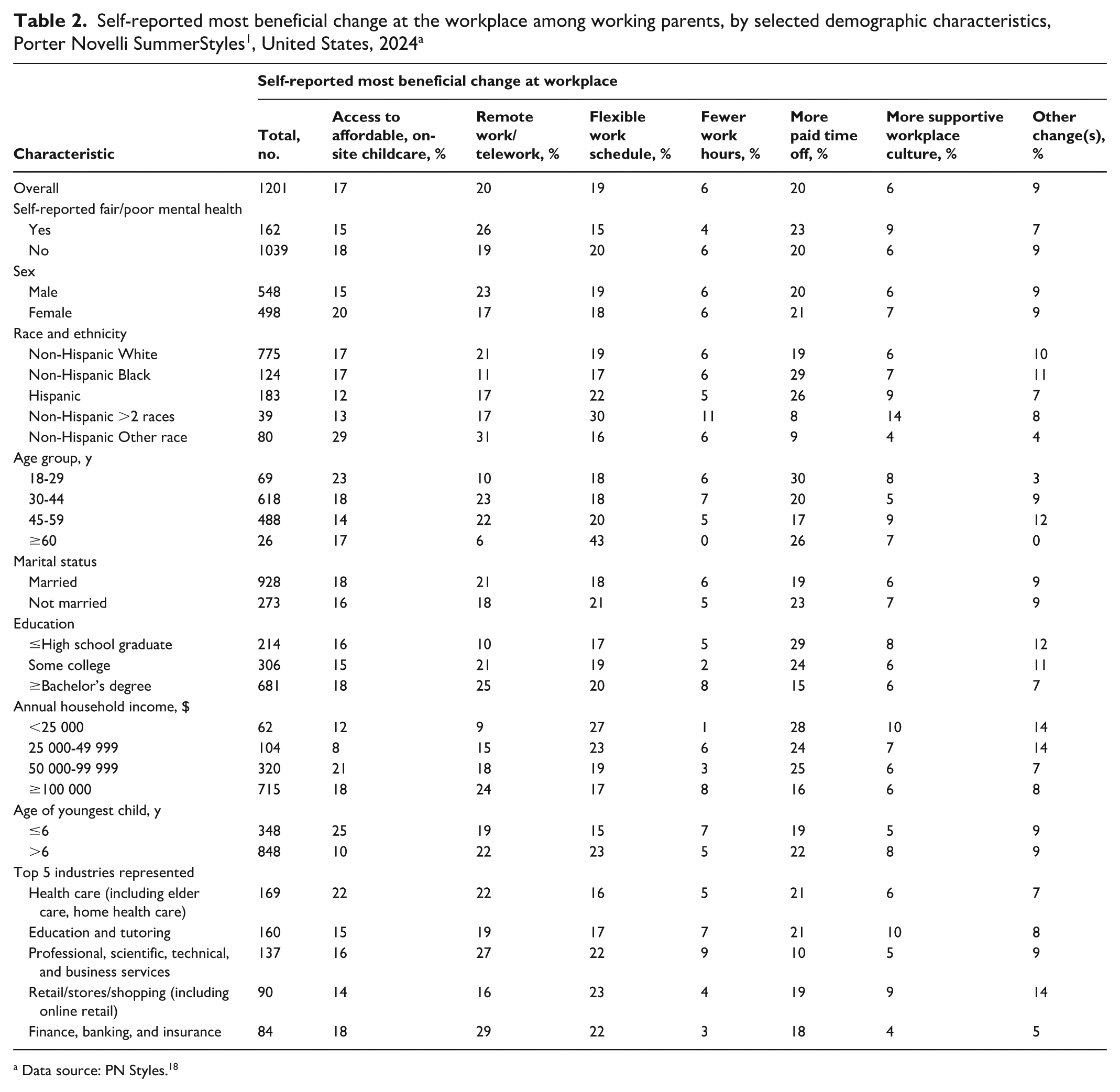
Data source: PN Styles. 18
Working parents with children aged ≤6 years (vs children aged >6 y) identified access to affordable, on-site childcare as the most beneficial workplace improvement (25% vs 10%) (Table 2). Working parents in professional, scientific, and technical services prioritized the ability to work remotely/telework (27%), while those in retail/stores/shopping jobs emphasized flexible work schedules (23%). Parents working in the health care sector identified access to affordable, on-site childcare (22%) and the ability to work remotely/telework (22%) as their top priorities.
Among working parents, preferences for workplace changes varied by self-reported mental health status (Figure). Working parents who reported fair or poor mental health (vs good/very good/excellent mental health) were more likely to prioritize the ability to work remotely/telework (26% vs 19%) and more paid time off (23% vs 20%). Access to affordable, on-site childcare was desired by both groups, although slightly more among working parents with good/very good/excellent mental health than among working parents with fair or poor mental health (18% vs 15%). In contrast, working parents with good/very good/excellent mental health (vs working parents with fair or poor mental health) more frequently endorsed a flexible work schedule (20% vs 15%) and a more supportive workplace culture (9% vs 6%). Only a small proportion of respondents in either group cited fewer work hours as their top desired change.
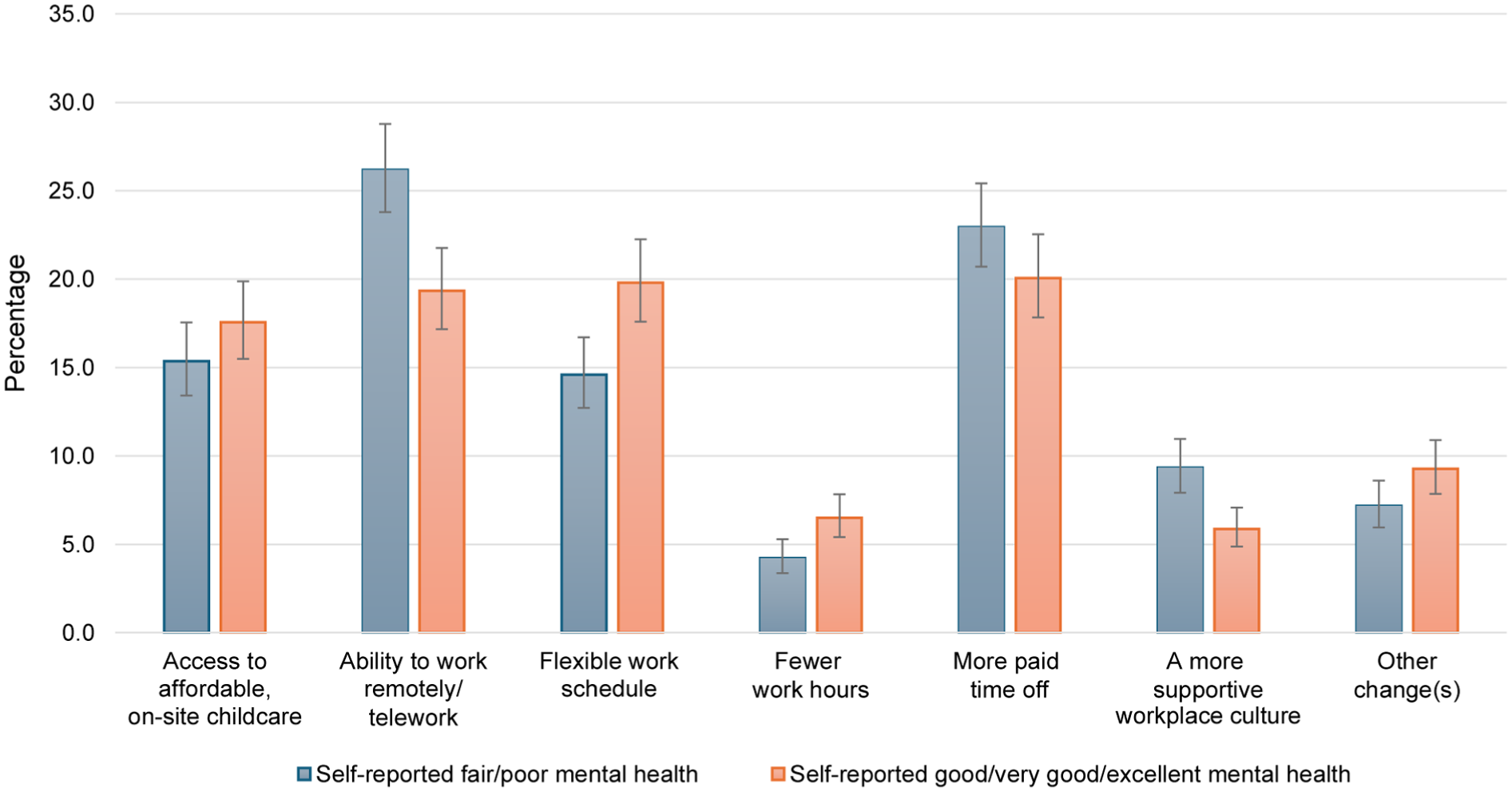
Self-reported most beneficial change at the workplace among working parents, by mental health status, Porter Novelli SummerStyles, United States, 2024. Data source: PN Styles. 18
Discussion
In this nationally representative sample of US adults, approximately 1 in 6 working parents reported fair or poor mental health. Working parents’ self-reported preferences for the most beneficial workplace changes differed meaningfully by sex, annual household income, child age, and—importantly—mental health status, highlighting the need for nuanced and responsive workplace policies.
Differences in mental health status by sex align with existing evidence 20 that caregiving responsibilities disproportionately affect working women. Among working parents in our sample, women were more likely than men to report fair or poor mental health and less likely to prioritize working remotely/teleworking as the most beneficial workplace change. This pattern is consistent with studies showing that remote work during the COVID-19 pandemic was associated with increased psychological distress among women but not men. 21 These differences may reflect the unequal distribution of unpaid household and caregiving labor, 20 which can compound with occupational demands to increase the incidence of fair or poor mental health status among female workers.
Working parents with fair or poor mental health were more likely to prioritize structural supports—such as remote work (26%) and paid leave (23%)—while those reporting good/very good/excellent mental health were more likely to select more supportive workplace culture. This divergence may reflect differences in baseline stress levels and perceived job control. Parents experiencing greater mental health challenges may require more substantive changes to manage work and caregiving demands, while other parents may benefit from optimizing existing supports.
Additionally, contextual factors not captured in this analysis, such as partner status (eg, single vs partnered) and partner employment, should be considered. These factors can influence both mental health outcomes and workplace preferences among working parents, shaping the dynamics of support systems and stressors they encounter. Future research should aim to incorporate these variables to provide a more nuanced and comprehensive understanding of the diverse factors affecting the well-being and workplace needs of this population. Previous research shows the importance of structural supports in enhancing mental health. For example, access to paid parental leave has been linked to lower psychological distress, improved overall well-being, and increased job satisfaction among working parents. 22 These supports can be especially critical for single parents and parents with lower-wage jobs, who may have fewer informal resources to buffer against the stress of balancing work and caregiving responsibilities than parents with partners or higher-wage jobs. Workers without access to paid sick leave are more likely than workers with access to paid sick leave to report anxiety and depression, 23 and parental access to leave has been associated with improved health care use and reduced stress. 24 Access to affordable childcare—more commonly prioritized by parents with younger children—has also been linked to reduced burnout and improved emotional well-being. 25
Importantly, robust structural supports have downstream implications for children’s health and development. Poor parental mental health (particularly persistent depression and anxiety) has been linked to adverse child outcomes, including emotional and behavioral difficulties, lower academic achievement, and impaired social functioning.26-28 Conversely, workplace policies that alleviate parental stress and enhance well-being may indirectly foster more stable and supportive home environments, which are associated with better developmental outcomes for children. 29 This intergenerational perspective highlights that improving workplace conditions for parents can produce long-term societal benefits that extend beyond the immediate workforce.
Differences in mental health outcomes and workplace priorities across industries likely reflect differing work conditions such as long shifts, unpredictable hours, or limited flexibility.30-32 Notably, compared with working parents in other industries, working parents in retail and health care sectors reported higher levels of fair or poor mental health and were more likely to prioritize paid sick leave and schedule flexibility. These findings suggest that industry-specific strategies are essential, particularly in customer- and patient-facing roles where certain workplace changes may be hard to implement.
Limitations
This study had several limitations. First, mental health was measured by using a single self-reported item, which may have introduced measurement error; however, such items have shown strong correlation with validated mental health screening tools. 33 Second, the cross-sectional design limited causal inference. Third, while survey weights improve generalizability, results may not reflect the experiences of all working parents, particularly those without reliable internet access or who are underrepresented in online panels. Fourth, our findings were based on a single dataset, which may limit the generalizability of our results. Studies using other national datasets or longitudinal studies could be used to assess the consistency and robustness of our results. Finally, because this was a descriptive, exploratory analysis, we did not conduct multivariable modeling to assess associations and, therefore, could not draw causal conclusions about our findings. Future research may benefit from hypothesis-driven inferential approaches that test associations between mental health and workplace priorities while adjusting for potential confounders or exploring effect modification.
Conclusion
This descriptive analysis provides timely insights into the mental health and workplace needs of US working parents. By identifying key disparities and worker-identified solutions, this study can inform equitable and targeted interventions. Future research should explore how workplace policies such as paid leave, childcare access, and flexible scheduling affect parent mental health.
Supplemental Material
sj-docx-1-phr-10.1177_00333549261451182 – Supplemental material for Self-Reported Mental Health and Desired Workplace Improvements Among Working Parents, United States, 2024
Supplemental material, sj-docx-1-phr-10.1177_00333549261451182 for Self-Reported Mental Health and Desired Workplace Improvements Among Working Parents, United States, 2024 by Kristen Van Buren, Eric W. Lundstrom, Amel Omari, Kristin J. Marks, Candice Y. Johnson and Dallas S. Shi in Public Health Reports®
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the National Institute for Occupational Safety and Health, Centers for Disease Control and Prevention. Use of trade names and commercial sources is for identification only and does not imply endorsement by the US Department of Health and Human Services.
Supplemental Material
Supplemental material for this article is available online. The authors have provided these supplemental materials to give readers additional information about their work. These materials have not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.