
Abstract
From January 5 through April 4, 2025, and July 14 through October 10, 2025, the US Public Health Service Commissioned Corps conducted the largest reported deployment in response to a syphilis outbreak in US history. During two 90-day periods, 67 US Public Health Service officers were deployed in 30-day rotations across 9 Tribal areas within the Indian Health Service Great Plains Area and 3 urban centers in South Dakota and North Dakota to support ongoing outbreak activities. Overall, the deployment identified 139 people newly diagnosed with syphilis through screening 2913 people. By 30 days after deployments for the syphilis outbreak response, 126 (90.6%) people with newly diagnosed syphilis had started treatment. This case study highlights the effective coordination among the Indian Health Service, the US Public Health Service Commissioned Corps, state health departments, Tribal health agencies, the Great Plains Tribal Leaders Health Board, and other partners. Prioritized activities of the response included contact tracing, health care provider education, community-based screening events, and field-based administration of treatment. We describe the roles of culturally sensitive public health practice, interagency collaboration, and rapid clinical response in responding to sexually transmitted infection outbreaks. Experience gained in South Dakota and North Dakota may provide insightful direction for future large-scale infectious disease campaigns.
From 2019 through 2023, the United States experienced a 58% increase in reported adult syphilis cases. 1 From 2021 through 2023, South Dakota had the highest rate of adult primary and secondary syphilis cases in the country, with a 50.7% increase during the period. 1 Since 2021, approximately 85% of early syphilis cases in South Dakota have been among American Indian or Alaska Native people.2,3
North Dakota and South Dakota have 12 federally recognized Tribes, 14 Indian Health Service (IHS) units, and 2 South Dakota Urban Indian Health Centers. Great Plains Tribal Leaders Health Board (GPTLHB) is a Tribal organization that is a consortium of 17 federally recognized Tribes in North Dakota, South Dakota, Nebraska, and Iowa. GPTLHB began syphilis outbreak response efforts in 2022 through the Great Plains Tribal Epidemiology Center (GPTEC), 4 which included requesting support from federal agencies. At the request of GPTEC and Tribes, staff from the Centers for Disease Control and Prevention (CDC) deployed to South Dakota to provide epidemiology and case investigation support in July 2023 and again in April 2024.5 -7 In February 2024, GPTLHB and Tribal leaders asked the US Department of Health and Human Services secretary to make a public health emergency declaration under section 319 of the Public Health Service Act8,9 to increase resources to address the syphilis outbreak, including deployment of a US Public Health Service (USPHS) Commissioned Corps.
In response, USPHS Commissioned Corps headquarters received funding for deployment and worked with IHS Great Plains Area staff to establish mission objectives and coordinate the syphilis response in South Dakota. Sixty-seven officers from the USPHS Commissioned Corps were deployed for six 30-day rotations from January 5 through April 4, 2025, and again from July 14 through October 10, 2025.
Purpose
This case study describes activities of the deployed US Public Health Service officers, including data describing the number of people screened for syphilis, people with syphilis identified, and treatment outcomes. We offer lessons learned from conducting a large-scale syphilis outbreak response across a large geographic area spanning multiple Tribal and urban communities. We share 4 key elements that made this deployment successful, which may inform future syphilis outbreak responses, especially in Tribal and rural areas where infrastructure constraints and health inequities are major obstacles to disease control measures.
Methods
Communication, Coordination, and Community Engagement
Deployment of the USPHS Commissioned Corps followed Tribal leaders’ request for personnel to support syphilis outreach, diagnosis, and treatment9 -11 and was informed by national data. 12 Prior to deployment, weekly coordination meetings were conducted with the Office of the Assistant Secretary for Health and IHS. Initial discussions included the IHS Area Office, IHS service units, CDC consultants from prior deployments, GPTLHB, and South Dakota Department of Health (SDDOH) to coordinate response activities.
Formal notification letters were sent to Tribal leaders detailing the objectives and scope of the response and the support designated for the Great Plains Area, particularly focusing on regions with the highest syphilis incidence rates. Given the diversity of participating sites, which included various Tribal and urban communities, engagement strategies were tailored locally to fit the needs, priorities, and contexts of each community in collaboration with Tribal and IHS partners. Local adaptations included selection of outreach locations, communication channels, and engagement approaches that aligned with local community norms, resources, logistics, and public health priorities.
During the deployment, weekly meetings were conducted with the IHS Area Office, IHS service unit staff, and the deployed US Public Health Service officer in charge and often included North Dakota Health and Human Services (NDHHS), SDDOH, and GPTLHB. Deployed officers met virtually on a weekly basis to address any concerns that the officer in charge elevated to partners as needed.
Officer Deployment and Training
US Public Health Service officers were deployed in 30-day rotations to South Dakota and North Dakota in 6 groups for two 90-day periods in 2025: 15 officers in January, 15 in February, 13 in March, 8 in July, 9 in August, and 7 in September. Officers represented various clinical disciplines, including licensed physicians, physician assistants, nurse practitioners, registered nurses, pharmacists, and laboratory technicians, from 11 federal agencies. All officers received mission orientation at the start of their deployment. Orientation included national and regional syphilis epidemiology; an overview of screening, diagnosis, and treatment recommendations; training on rapid point-of-care tests; and guidance on contact-tracing procedures, case interview techniques, cultural competency, trauma-informed care, and surveillance data collection and reporting processes.
This activity was reviewed by IHS, deemed not research, and conducted consistent with applicable federal law and IHS policy (see eg, 45 CFR part 46.102[l][2], 21 CFR part 56; 42 USC §241[d]; 5 USC §552a; 44 USC §3501 et seq).
Prioritized Outbreak Response Activities
Deployment teams were assigned to areas with high syphilis incidence rates and conducted response activities in North Dakota and South Dakota at 10 IHS units and 2 Urban Indian Health Centers. Activities were guided by IHS13,14 and CDC 15 sexually transmitted infection recommendations and included augmenting existing case finding and contact-tracing efforts through household visits; conducting community events for syphilis screening, treatment, and education; focused screening and field treatment in high-risk institutional settings; and delivering health provider education. Contact tracing for pregnant women, women of childbearing age, and their partners was prioritized to reduce the risk of congenital syphilis.
Multiagency Coordination
Coordination among agencies was a cornerstone of this response. Orientation training and response activities were coordinated by IHS and hosted by GPTEC. SDDOH and NDHHS provided surveillance record search capacity to ensure prompt review of prior diagnosis and treatment to guide appropriate management of people who had a positive test result for syphilis and their contacts. Tribal health directors and IHS public health nursing staff facilitated community engagement, education, screening events, and door-to-door outreach. Officers worked with corrections staff to develop mass screening protocols in correctional facilities. The US Department of Health and Human Services supported response funding and provision of benzathine penicillin and rapid syphilis test kits.
Syphilis Screening Events
Community-based response outreach, education, and screening activities occurred at community events, grocery stores, homeless shelters, drug rehabilitation centers, county and Tribal correctional facilities, and private homes. Teams established testing areas in emergency department waiting areas, dental clinics, and outpatient clinics and provided education at health fairs, schools, and clinic settings.
The availability of syphilis testing at community events was advertised in multiple forms in English, the primary spoken language. Fliers and calendars were created and disseminated in communities, uploaded onto social media sites, and distributed with medications in pharmacy bags. Local radio stations hosted IHS staff, who promoted upcoming community-based events where syphilis testing would be available.
During voluntary testing events, every opportunity was taken to update demographic information in medical and surveillance records, including residence history and a list of contacts to ensure adequate clinical follow-up. Consent for testing or treatment was obtained per IHS or partnering clinical facilities’ procedures. Minor differences in processes were present across deployment sites. Most were associated with the source of test result data or public health contact-tracing processes (local or IHS area) and use of testing and treatment supplies.
Treatment of Individuals and Their Contacts
Syphilis was treated with intramuscular benzathine penicillin injections in people without penicillin allergies or those who were pregnant. Those nonpregnant people with reported or documented penicillin allergy received oral doxycycline. Medications were administered by licensed USPHS Commissioned Corps, IHS, or Tribal health center providers according to stage of syphilis infection based on CDC 2021 sexually transmitted disease treatment guidelines 15 in clinic and field-based settings.
Data Collection
US Public Health Service officers recorded all officer–patient activities by using a standard form (Supplemental File). Officers documented screenings and treatment of individuals in both paper and electronic versions. Site leads compiled this information and collaborated with IHS and Tribal public health nurses, GPTEC, and state public health staff to update diagnoses and treatment status, submitting data weekly to the IHS response data lead. Submitted data included information on outreach events, test outcomes, treatment details, case status, and staging efforts in which officers participated.
IHS sites used either traditional or reverse syphilis testing algorithms, 16 per site protocols. Positive test results were considered indicative of a potential new syphilis infection only when the nontreponemal rapid plasma reagin and a treponemal test (Treponema pallidum particle agglutination or other rapid treponemal test) were reactive.
In instances where the rapid plasma reagin and T pallidum particle agglutination were reactive, additional clinical evaluation and surveillance record review determined whether the test result reflected a new syphilis infection or a previously identified and treated individual. This strategy included medical record review and patient history assessment in collaboration with NDHHS and SDDOH disease intervention specialists to verify prior syphilis titers, stage, and treatment history to clarify case classification. This process differentiated among newly acquired infections, serofast status 17 (stable nontreponemal titer after adequate treatment), or reinfections, each requiring different clinical and public health management.
Data Analysis
IHS Area Office staff consolidated weekly data into an aggregate dataset in Microsoft Excel for analysis. Pending laboratory results were promptly updated as results were received, and individuals who received a positive test result were cross-checked against the SDDOH disease management system to validate case classification. Data were cleaned to remove duplicate entries of individuals who were screened more than once within each 90-day period.
Outcomes
During the deployments, 2913 people were screened for syphilis in the community at 10 IHS facilities and in 3 urban areas in South Dakota and North Dakota. Among those screened, 51.1% (n = 1489) were female (Figure). The average age was 39 years (range, 13-87 y), with a median age of 38 years for both sexes. Among females screened, 67.5% (n = 1005) were of childbearing age (15-44 y).
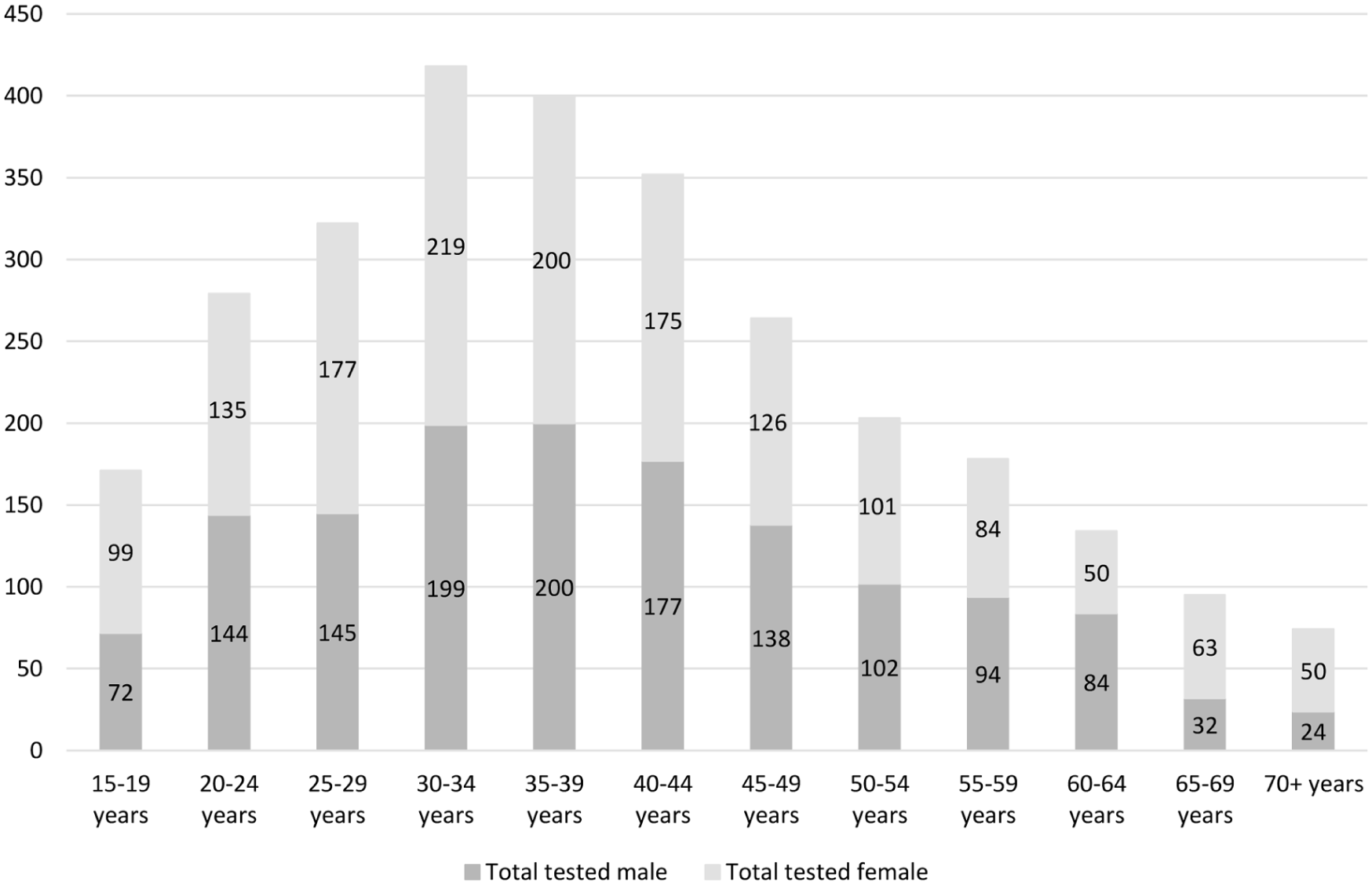
Reported syphilis screenings by age and sex, South Dakota and North Dakota, January 5–April 4 and July 14–October 10, 2025 (N = 2913). Screenings for those aged 0 to 14 years and unknown age are not included due to small numbers. This discourages misinterpretation of unstable data and protects patient confidentiality.
A total of 139 people with newly identified syphilis were observed during the deployment through routine screening events, yielding a syphilis incidence rate of 4.8%. Among females of childbearing age, 6.1% (61 of 1005) presented as newly diagnosed. The average age of people with syphilis was 34 years (range, 17-66 y), with a median age of 33 years for females and 34 years for males.
Among people identified, syphilis staging was available for 84.9% (118 of 139). Approximately two-thirds (61.9%; n = 86) were late or unknown duration, 16.5% (n = 23) were early nonprimary/nonsecondary stage, and 6.5% (n = 9) were primary and secondary syphilis. Treatment was initiated with penicillin or doxycycline in 126 (90.6%) patients. USPHS officers and other field staff referred individuals not treated during the deployment period for treatment through IHS, Tribal health centers, NDHHS, or SDDOH.
Lessons Learned
Four key components of this USPHS Commissioned Corps deployment facilitated response efforts and helped make the deployment successful.
Need for USPHS Commissioned Corps Deployment
Before officer deployments in January 2025, local, state, federal, and Tribal partners had been collaborating on syphilis outbreak response efforts for 3 years. Although robust, efforts had been hindered due to high clinical staff vacancy rates 18 and limited surge capacity to respond to large outbreaks. Officer deployment was initially proposed in a 2023 resolution from the GPTLHB because clinical staff were needed to provide direct clinical care, such as syphilis testing, test interpretation, and treatment, as the scope of the current syphilis outbreak exceeded the capacity of these local systems. As one of the nation’s uniformed services, the mission of the USPHS Commissioned Corps “is to protect, promote, and advance the health and safety of the nation.” 19 Officers provide surge capacity of clinical staff to communities to mitigate public health threats and respond to emergencies when local capacity is overwhelmed. The historic presence of deployed US Public Health Service officers demonstrates responsive federal support and a sustained commitment to curbing syphilis increases in Tribal settings.
Multijurisdictional Collaboration
Multiagency collaboration is vital to any outbreak response efforts but is particularly important and challenging in Tribal settings.20 -23 Overlapping jurisdictions and roles necessitate close coordination of staff, resources, and activities to ensure efficient use of resources. Monthly and weekly meetings between key partners supporting the work of the deployment teams included staff from IHS, GPTLHB (including GPTEC and Oyate Health Center, a Tribally operated health center that receives funding from IHS under the 638 Compact), 24 Tribal public health authorities, NDHHS, and SDDOH. Officers were able to build on existing partnerships and response activities to guide efforts. Each partner played an important role in the deployment: IHS and GPTLHB provided strategic guidance on overall goals, helped identify high-priority communities, and supplied resources; Tribal and IHS staff facilitated officer education, access to and use of clinical facilities and materials, and navigation of local communities. IHS, SDDOH, and NDHHS managed data that helped to locate people with syphilis and their contacts, enabled disease staging, guided treatment recommendations, and contributed staff for field teams.
Readily Available Testing and Treatment Resources
Rapid identification and prompt treatment of individuals with syphilis and their contacts were prioritized to prevent ongoing community-level transmission. To reach as many people as possible and align with IHS’s federal obligation and responsibility to American Indian or Alaska Native people, 25 all testing and treatment were provided at no cost to individuals. Clinical staff and officers conducted laboratory testing through venous blood draws using IHS, Tribal, and private laboratories, depending on local resources, to ensure quick laboratory test results and subsequent treatment. Point-of-care testing was used selectively, especially during community events or in remote settings without readily accessible laboratory services. In accordance with national guidelines, 15 benzathine penicillin was the preferred treatment. IHS was able to provide an adequate supply of benzathine penicillin for people with diagnosed syphilis, despite shortages from a voluntary recall and relatively high cost.
Community-Based Response
Community participation in the syphilis response was essential to the success of these events because they provided local knowledge, such as when and where to hold events. USPHS officers were embedded with local public health staff (Tribal, IHS, and state). This type of community input enhanced the officers’ work and allowed the deployment to be tailored to local needs. For example, patient incentives in the form of gift cards were available for some screening events and appeared to encourage screening participation. 4 Additionally, officers planned and conducted large-scale syphilis screenings in a county jail, homeless shelters, and a drug rehabilitation center in Rapid City, an urban area in South Dakota included in this response.
This case study highlights the importance of community involvement, interagency coordination, and culturally sensitive practices in a large-scale public health deployment. The response, which deployed 67 US Public Health Service officers in 2025 across a large rural area, extended and expanded the ongoing outbreak response activities previously implemented by Tribal, IHS, and local public health partners. These USPHS Commissioned Corps–supported efforts produced notable public health results, with nearly 3000 people screened and 139 newly identified with syphilis. Provisional data from SDDOH for 2025 showed a 41.5% decrease in early syphilis cases as compared with 2024.3,26 These decreases suggest that interventions are resulting in overall declines in syphilis rates.
Mission objectives informed by cultural awareness and context related to the environment and communities where the response efforts occurred were foundational to a successful response in these Tribal areas. The successful establishment of trust between community members and response partners for the delivery of syphilis outbreak response activities was important and may have led to the large number of people presenting for syphilis testing. Historical trauma and mistrust pose major challenges for health engagement in many American Indian or Alaska Native communities. 27 A united and collaborative partnership supported a multiagency response pairing essential skill sets with a united approach. Finally, ensuring that officers and supporting partners understood the syphilis-related clinical and public health interventions necessary to perform the mission objectives was essential to provide appropriate care to community members. Lessons learned from this response can inform approaches in other areas facing increases in the number of syphilis cases. Although these results are encouraging, ongoing support is needed to continue response efforts to identify undiagnosed syphilis cases to end the syphilis outbreak in Tribal communities and jurisdictions in the Great Plains Area.
Supplemental Material
sj-docx-1-phr-10.1177_00333549261453011 – Supplemental material for A US Public Health Service Commissioned Corps Response to a Syphilis Outbreak in Tribal Communities in South Dakota and North Dakota, 2025
Supplemental material, sj-docx-1-phr-10.1177_00333549261453011 for A US Public Health Service Commissioned Corps Response to a Syphilis Outbreak in Tribal Communities in South Dakota and North Dakota, 2025 by Kaitlin A. Gonzales, Meghan Curry O’Connell, Melanie M. Taylor, Tai-Ho Chen, Tyler Broghammer, Michelle VanderMay, Christopher Peltier and Natalie F. Holt in Public Health Reports®
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for GPTLHB participation in these response efforts was provided by the Indian Health Service, US Department of Health and Human Services (U1B11IHS00007, NU121HS0029).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention or the Indian Health Service.
Supplemental Material
Supplemental material for this article is available online. The authors have provided these supplemental materials to give readers additional information about their work. These materials have not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.