
Abstract
Objectives:
Mental health screening platforms can be used to identify students in mental distress and can connect students to mental health services during disruptive events such as campus closures. We examined college students’ utilization of a mental health screening platform in the year before and after COVID-19–related campus closures.
Methods:
We analyzed 12 239 students across 31 US institutions who used the Interactive Screening Platform (ISP) in the 1 year before and after the COVID-19–related campus closure on March 15, 2020. We analyzed 3 outcomes: the monthly number of participants at each college, the proportion of participants who entered a dialogue with a mental health counselor, and the proportion of participants who sought a referral through the platform. To determine whether students sought a referral to mental health services, we used natural language processing methods to analyze messages between students and counselors. We used 2-sample t tests to test for differences in means and χ2 tests to determine differences in proportions, with P < .05 indicating significance.
Results:
We found no significant differences in the mean number of participants before and after March 15, 2020 (14.4 vs 16.0 participants per month, respectively), the proportion of participants who participated in a dialogue with a counselor (22.9% [1327 of 5806] vs 23.3% [1501 of 6433]), or the proportion of participants who sought a referral (11.2% [649 of 5806] vs 10.9% [698 of 6433]).
Conclusions:
Student use of the ISP was sustained after the COVID-19–related campus closures, suggesting that the ISP can continue to engage with students during disruptions to campus life. The ISP is a tool that campus leaders can consider using during future disruptive events.
Keywords
In tandem with the mental health crisis among young people, 1 the mental health of college students has been an increasing concern during the past decade.2,3 In response, colleges and universities have expanded their efforts to support students’ mental health through clinical mental health services and prevention programming.4,5 Clinical telehealth services and digital mental health programs are increasingly being used to supplement campus services. 6 Although digital or online mental health programs vary, such programs have been shown to reduce symptoms of anxiety and depression among college students.7,8 Some programs serve as a portal to clinical services delivered by a mental health professional, some deliver self-guided therapeutic content or psychoeducation, and some seek to connect students to care.
Student mental health, which was already worsening before the COVID-19 pandemic, was affected by the pandemic; campus closures, which ended in-person classes and forced students to leave campus, abruptly disrupted college students’ routines.9,10 During the pandemic, students had difficulty understanding how to access clinical mental health services.11,12
Information on how students connected to online mental health services could guide strategies to support their mental health should campuses close again. Future campus closures are not out of the question, given that the risk of another pandemic might be increasing. 13 Since the onset of COVID-19, online mental health interventions have been effective in mitigating anxiety, depression, and social functioning in young people. 14 However, what has not been investigated is (1) the use of online mental health interventions among college students during disruptive events and (2) whether mental health screening platforms, such as the Interactive Screening Program (ISP), can identify students in mental distress and connect them to mental health services during such periods.
Program Description
The ISP is an online platform developed by the American Foundation for Suicide Prevention (AFSP) that focuses on reaching students who are in mental distress and seeks to connect them to professional mental health care.15,16 Previous studies have described the ISP in detail,5,15-17 and additional information is provided (eSection 1 in Supplemental Material). Briefly, the AFSP developed the ISP in the early 2000s to identify students experiencing mental distress and to connect them to care. Since its inception, approximately 60 campuses have used the ISP. The ISP includes an initial questionnaire that asks questions about mental health symptoms in various domains, which serves to characterize risk. A mental health professional who works at the student’s campus reviews the questionnaire responses and gives feedback to the student, which often includes immediate empathic support and information about seeking professional care. The student then has the option to continue to exchange messages with the mental health professional through the “dialogue” feature. The dialogue aims to catalyze the student’s connection to professional mental health services.
Importantly, the ISP aligns with existing models for suicide prevention strategies. The cascade of care model, adapted from the HIV cascade of care model, stipulates 5 stages: (1) identification and characterization of risk, (2) immediate intervention, (3) linkage to professional care, (4) further prevention and treatment, and (5) recovery and resilience. 18 The ISP facilitates stages 1 through 3 of the cascade of care model for suicide prevention.
One pathway to implementing the program is through federal funds, such as the Garrett Lee Smith Campus Suicide Prevention Grant. For example, Johns Hopkins University implemented the program after receiving a Garrett Lee Smith award and decided that its benefits merited retaining the program after federal funding expired. 5
The ISP offers an important opportunity to study digital health interventions for college students during a disruptive campus event for several reasons. First, the ISP is one of the earliest digital screening programs used in the college campus context and can offer data for at least 1 year before the campus closures related to the COVID-19 pandemic, allowing us to control for seasonal variations in patterns of student use. Second, the ISP is multi-institutional and can provide insights beyond specific institutional, sociodemographic, or geographic contexts. Third, to our knowledge, the ISP is one of the most utilized platforms that facilitates text dialogues between higher education students and mental health professionals. These rich data offer an important opportunity to examine students’ engagement patterns and help-seeking behaviors during disruptions to campus life. Given the scope of the ISP data, the supervised use of natural language processing (NLP) methods with appropriate testing and careful oversight provides a powerful tool to process unstructured text data 19 that would take hundreds of thousands of hours of human work.
Purpose of the Evaluation
We used 3 aims to evaluate utilization of the ISP during the COVID-19 pandemic. For aim 1, we compared ISP utilization by students in the year before and after March 15, 2020, when campuses closed because of the COVID-19 pandemic. For aim 2, we compared the proportion of participants engaging in a dialogue with a mental health professional in the year before and after the March 15, 2020, campus closures. For aim 3, we compared the proportion of participants who sought a referral through the ISP before and after the March 15, 2020, campus closures.
We used the 3 aims to evaluate the ISP’s performance on the numerically corresponding stage of the cascade of care model. For example, aim 1 sought to evaluate the number of participants who used the ISP, which can characterize risk for suicide by asking questions about depressive symptoms, substance use, and suicidal thoughts and behaviors. This corresponds with stage 1 of the cascade of care model, which seeks to characterize risk.
Methods
Study Design
We used data from students participating in the ISP for this cross-sectional study. The Johns Hopkins Medicine Institutional Review Board acknowledged this secondary analysis of deidentified data (under application 00326442) as exempt from human studies research review and deemed that consent from participants was not required. We conducted the analysis in accordance with the ethical standards outlined in the 1964 Declaration of Helsinki.
Data Sources and Sample
We obtained the ISP data from the AFSP. We decided to select the cutoff for the pre– and post–COVID-19 closure periods as Sunday, March 15, 2020, the date by which more than one-half of US postsecondary institutions had transitioned to virtual learning.20,21 The transition happened quickly. As of March 8, only 2 institutions had closed. By March 18, >85% of institutions had transitioned to virtual learning. 20 To control for differences in seasonal variation, we established the time frame for the analysis as 1 full year before and after March 15, 2020. We included students at institutions who were using the ISP continuously between March 16, 2019, and March 15, 2021. We defined continuous use as at least 1 student at their institution completing the questionnaire in periods that correspond to months when a school would be in session (eSection 1 in the Supplement).
Outcome Measures
We examined the following utilization outcomes: (1) the number of participants per month per institution, (2) the proportion of participants who participated in a dialogue, and (3) the proportion of participants who sought a referral to care. We counted dialogue participation as yes (vs no) when the student had sent a message to the mental health counselor after completing the survey, and we calculated the proportion by using the denominator of ISP participants during the same pre– or post–COVID-19 closure period.
We used NLP methods to analyze the content of the dialogue entries and to determine whether a student sought a referral to care. We calculated proportions by using the denominator of all ISP participants during the same pre– or post–COVID-19 closure period. Before analysis, one author (C.A.) deidentified the text data by using established NLP methods for deidentifying personal health information. 22 To mitigate the possibility of bias and strengthen reliability, we implemented a rigorous 4-step process to determine the outcome of seeking a referral to care: (1) we established a standardized definition for seeking a referral to care, (2) we manually coded a test set of dialogues using the standardized definition, (3) we trained and validated the NLP models on the manually coded test set, and (4) we applied the NLP models to the rest of the dataset.
For step 1, we drafted a definition for seeking a referral to care and applied the definition to a random sample of 10 dialogues by having 4 to 6 authors code each dialogue as yes or no for seeking a referral to care. We discussed disagreements in coding and revised the definition of seeking a referral to care through a consensus-building process. We executed this process on sets of 10 randomly sampled dialogues and assessed interrater agreement, as measured by Randolph κ. Randolph κ is an alternative to Cohen κ when there are >2 coders. 23 We obtained a Randolph κ of 0.93 for seeking a referral to care after we coded 70 unique dialogues.
For step 2, we randomly sampled a test set of 200 dialogues and assigned random combinations of 3 authors from a 6-author coding team to code each dialogue. The majority vote among the 3 coders determined whether a dialogue was coded yes or no for seeking a referral to care. We determined that the interrater agreement for seeking a referral to care was still satisfactory in this 200-dialogue test set (0.78).
For step 3, an author with expertise in NLP (C.A.) tested various NLP model settings and prompts for GPT-4o (OpenAI) on 50 of the 200 dialogues to identify the best-performing model. The author then applied the highest-performing settings and prompt to the full 200-dialogue test and checked against the manual coding. We determined that GPT-4o achieved an accuracy score of 90.2% and a Cohen κ of 0.80 on this 200-dialogue test set.
After we achieved these robust performance scores, for step 4, we allowed GPT-4o to assign yes or no for seeking a referral to care to the rest of the dialogues. Likely for safety reasons, GPT-4o refused to evaluate 281 dialogues (many of which contained language about self-harm). Two authors (S.L. and A.M.W.) coded those dialogues (achieving 89% agreement). A third coder (J.A.) coded the remaining 31 dialogues for which the 2 authors had disagreed. We considered students who did not enter any dialogue text as not having sought a referral. Additional details about the NLP methods are included in eSection 3 of the Supplement, such as the codebook definition for seeking a referral, the model settings tested, and the final model settings and prompt.
Predictor
The predictor was a binary variable representing the pre– and post–COVID-19 closure periods for the 1 year before and after the end of the day on Sunday, March 15, 2020, with the former serving as the reference group.
Covariates
We collected sociodemographic measures from self-reported student data. Each institution selects which sociodemographic variables to collect, leading to variability in the availability of certain variables. Adopting a threshold used in prior work with ISP data, we included only sociodemographic variables that had no more than 30% missing data. 24 Retained sociodemographic variables included age (5.0% missing data), gender (2.6% missing data), and race and ethnicity (19.2% missing data). The survey obtained age as a numerical entry. An open-ended question assessed gender with categorical responses in a “select all that apply” format and coded as female, male, transgender, genderqueer (which included people who identified as gender nonconforming), and other (which included people who selected self-describe, nonbinary, gender agnostic, agender, third gender, other, or ≥1 response). Similarly, an open-ended question queried race and ethnicity with categorical responses that included White (some institutions used the descriptors Caucasian/European/White), American Indian or Alaska Native, African American/Black (some institutions used African/Afro-Caribbean), Hispanic/Latin(x), multiethnic, Asian/Pacific Islander, Arab/Middle Eastern, other, and prefer not to answer.
Analysis
We used RStudio version 2023.12.1+402 (Posit PBC) for our analyses. We calculated descriptive statistics for sociodemographic characteristics of participants in the year before and after March 15, 2020, as well as the total number of users, mean monthly users, and proportion of users participating in the dialogue and seeking a referral. We calculated the mean monthly participation per institution as the total number of participants completing a questionnaire per institution (determined by the survey time stamp) in each of the pre– and post–COVID-19 closure periods divided by 12 (to get a monthly average). Of note, to calculate mean monthly participation, we combined participation in the 2 half-months on either end of the pre–COVID-19 year (March 16-31, 2019, and March 1-15, 2020) to create 12 total months, and we did the same for the following year. We used 2-sample t tests to test for differences in the mean monthly users before and after March 15, 2020, and Pearson χ2 tests to determine differences in proportions.
We developed 4 pairs of regression models: an unadjusted model and an adjusted model for each outcome. For each model, we used the closure period (pre– vs post–COVID-19) as the predictor and 95% CI for its coefficient to test the hypothesis that utilization was different before and after March 15, 2020. For the first pair, we used Poisson regression to model the outcome of participation count per institution in each calendar month. The adjusted model included institution, calendar month, the proportion of female respondents at an institution in that month, and the proportion of White respondents at an institution in that month. We chose female and White respondents because they were the largest categories of gender and race and ethnicity. For the second and third pairs, we used logistic regression to model the outcomes of engaging in a dialogue and seeking a referral, respectively. Both adjusted models included each participant’s institution, gender, and race and ethnicity, as well as the month of participation. For the fourth model pair, we used Poisson regression to execute an interrupted time-series analysis of the participation count per institution in each month. 25 The interrupted time-series equations are shown here.
The monthnumber (0-24 in the 2-year time series) and the interaction term between monthnumber and period (pre- vs postclosure) distinguished the time-series models from the first pair of Poisson models described previously. Of the 2 interrupted time-series regressions, the first included a term (monthname) to adjust for monthly variation in participation. All Poisson regressions used the number of days in each calendar month as the exposure, and 95% CIs were generated by robust SEs given overdispersion in the data.
We conducted 8 post hoc sensitivity analyses (eSections 6-9 in the Supplement). The first 3 analyses assessed whether the findings were driven by particular groups of institutions by excluding 3 groups of schools from the analysis (low-utilization schools, schools with inconsistent participation, and schools in the top and bottom deciles of utilization). The next 3 analyses examined how handling the safety-flagged dialogues in 3 ways affected our results. For the seventh, given the rollout of vaccines in December 2020, 26 we investigated how restricting the comparison periods to March 16 to December 31 of 2019 and 2020 affected the results. Eighth and last, we checked for trends in ISP utilization across gender and race subgroups.
Results
A total of 16 630 students across 58 institutions used the ISP from March 16, 2019, through March 15, 2021. After excluding institutions that did not have ISP participation in each academic term in the year before and after March 15, 2020, our sample included 31 institutions and 12 239 students. Of the 31 institutions, most were public (n = 23) and almost half (n = 15) enrolled ≥10 000 students (eSection 4 in the Supplement).
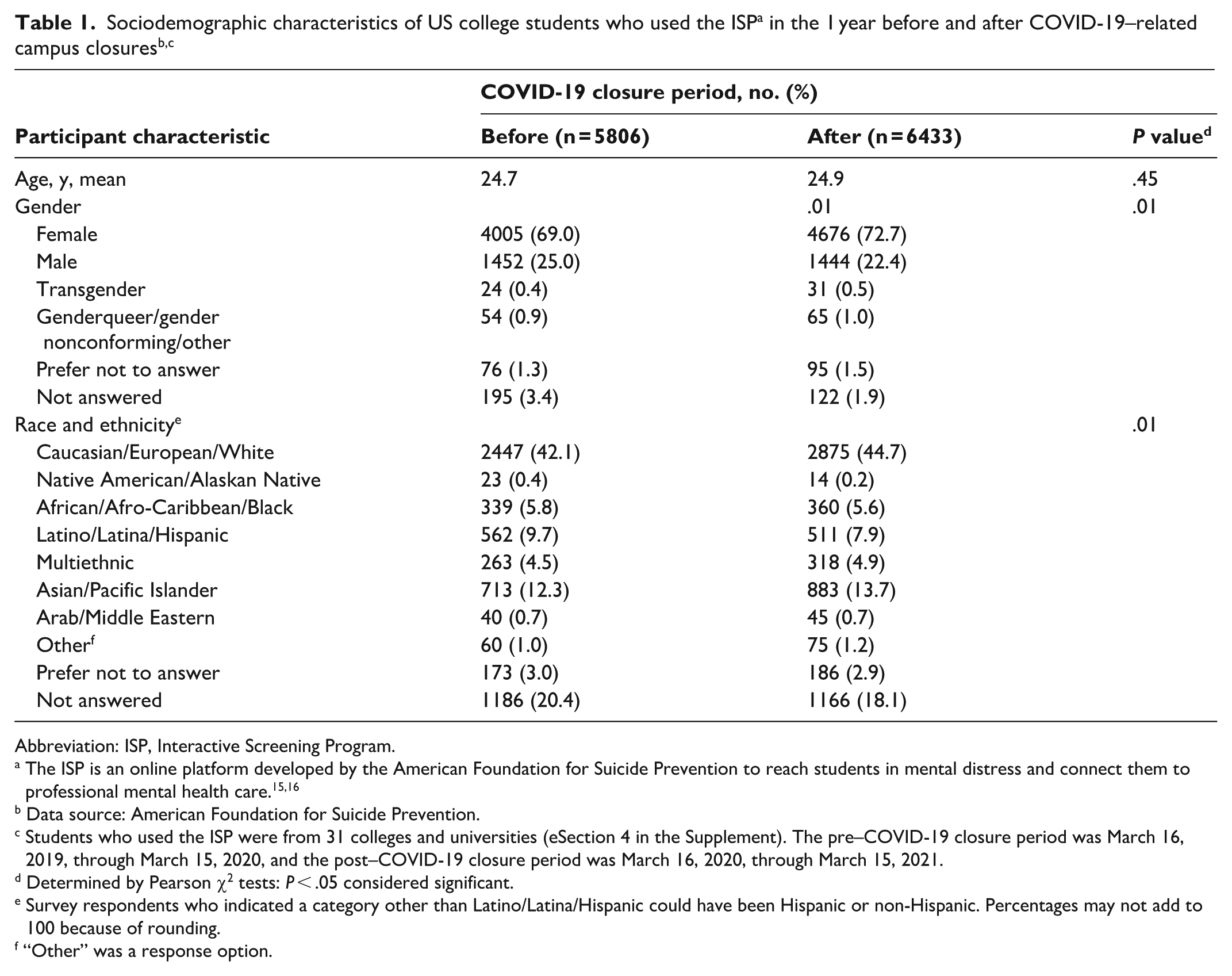
We found some differences in the sociodemographic characteristics of students who participated in the ISP in the year before and after March 15, 2020 (n = 5806 and n = 6433, respectively) (Table 1). The mean age of participants in both groups neared 25 years (t11 417 = –0.75; P = .45). The 2 groups differed significantly in terms of gender (χ24 = 14.9; P = .01). A greater percentage of pre–COVID-19 participants than post–COVID-19 participants identified as male (25.0% [1452 of 5806] vs 22.4% [1444 of 6433]) and a lower percentage identified as female (69.0% [4005 of 5806] vs 72.7% [4676 of 6433]). The 2 groups differed significantly in terms of the distribution of race (χ28 = 23.2; P = .01). The pre–COVID-19 group had a lower percentage of White students (42.1% [2447 of 5806] vs 44.7% [2875 of 6433]) and a higher percentage of Latin(x)/Hispanic students (9.7% [562 of 5806] vs 7.9% [511 of 6433]) than the post–COVID-19 group.
Abbreviation: ISP, Interactive Screening Program.
The ISP is an online platform developed by the American Foundation for Suicide Prevention to reach students in mental distress and connect them to professional mental health care.15,16
Data source: American Foundation for Suicide Prevention.
Students who used the ISP were from 31 colleges and universities (eSection 4 in the Supplement). The pre–COVID-19 closure period was March 16, 2019, through March 15, 2020, and the post–COVID-19 closure period was March 16, 2020, through March 15, 2021.
Determined by Pearson χ2 tests: P < .05 considered significant.
Survey respondents who indicated a category other than Latino/Latina/Hispanic could have been Hispanic or non-Hispanic. Percentages may not add to 100 because of rounding.
“Other” was a response option.
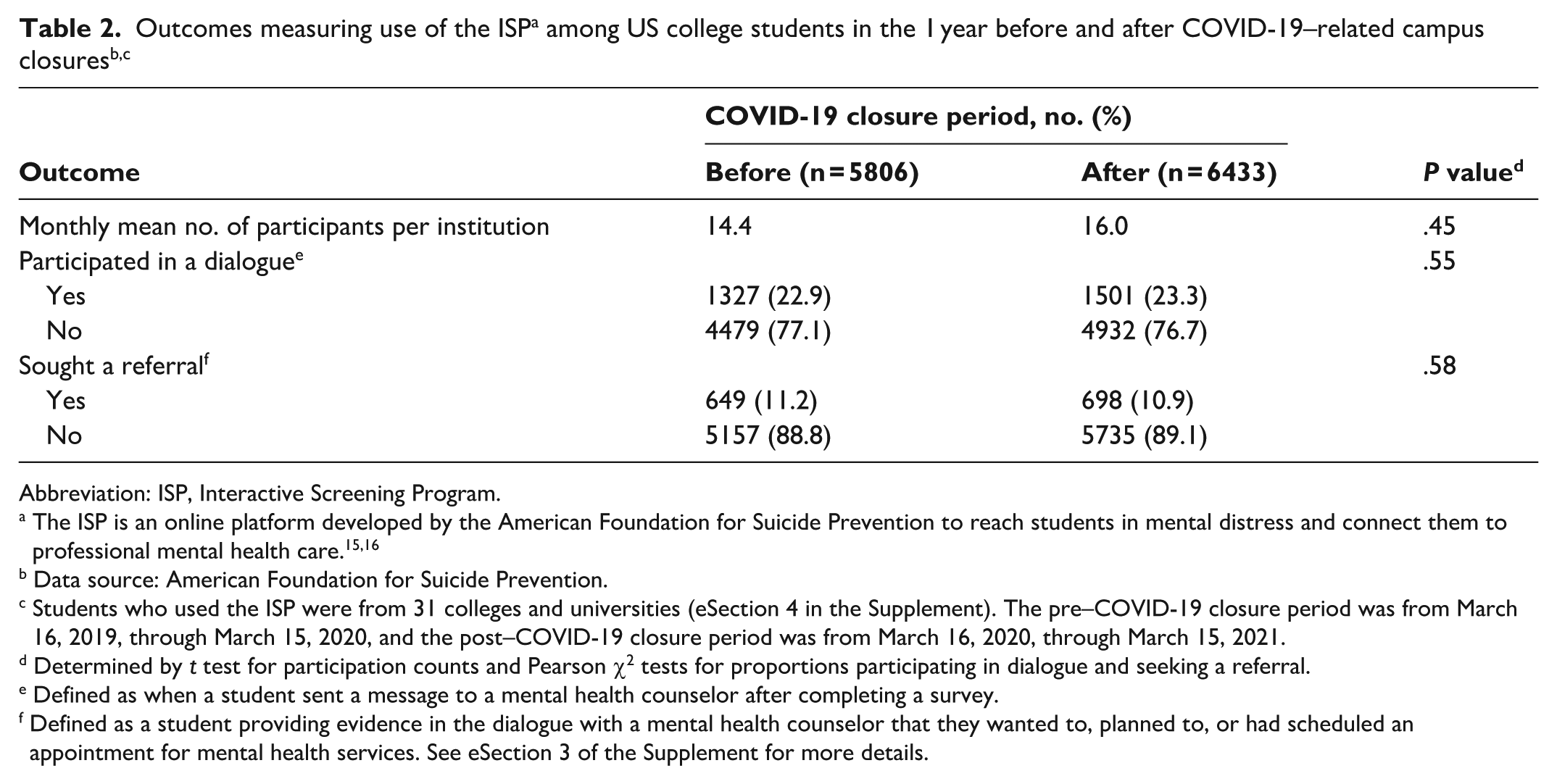
Mean monthly participation at each institution was lower—but not significantly different—in the year before March 15, 2020, as compared with the year after (14.4 vs 16.0 participants per month at each institution; t801 = 0.76; P = .45) (Table 2). Comparing the years before and after March 15, 2020, revealed no differences in the proportions of students participating in a dialogue (22.9% [1327 of 5806] vs 23.3% [1501 of 6433], respectively; χ21 = 0.36; P = .55) or seeking a referral (11.2% [649 of 5806] vs 10.9% [698 of 6433]; χ21 = 0.30; P = .58).
Abbreviation: ISP, Interactive Screening Program.
The ISP is an online platform developed by the American Foundation for Suicide Prevention to reach students in mental distress and connect them to professional mental health care.15,16
Data source: American Foundation for Suicide Prevention.
Students who used the ISP were from 31 colleges and universities (eSection 4 in the Supplement). The pre–COVID-19 closure period was from March 16, 2019, through March 15, 2020, and the post–COVID-19 closure period was from March 16, 2020, through March 15, 2021.
Determined by t test for participation counts and Pearson χ2 tests for proportions participating in dialogue and seeking a referral.
Defined as when a student sent a message to a mental health counselor after completing a survey.
Defined as a student providing evidence in the dialogue with a mental health counselor that they wanted to, planned to, or had scheduled an appointment for mental health services. See eSection 3 of the Supplement for more details.
The unadjusted and adjusted regression models for each of the 3 utilization metrics did not detect significant differences between the years before and after March 15, 2020 (Table 3). The monthly predictions from the interrupted time-series regression models showed similar utilization in both years, with a general increase in participation from March to March each year and annual peaks in October and February (Figure; eSection 5 in the Supplement).
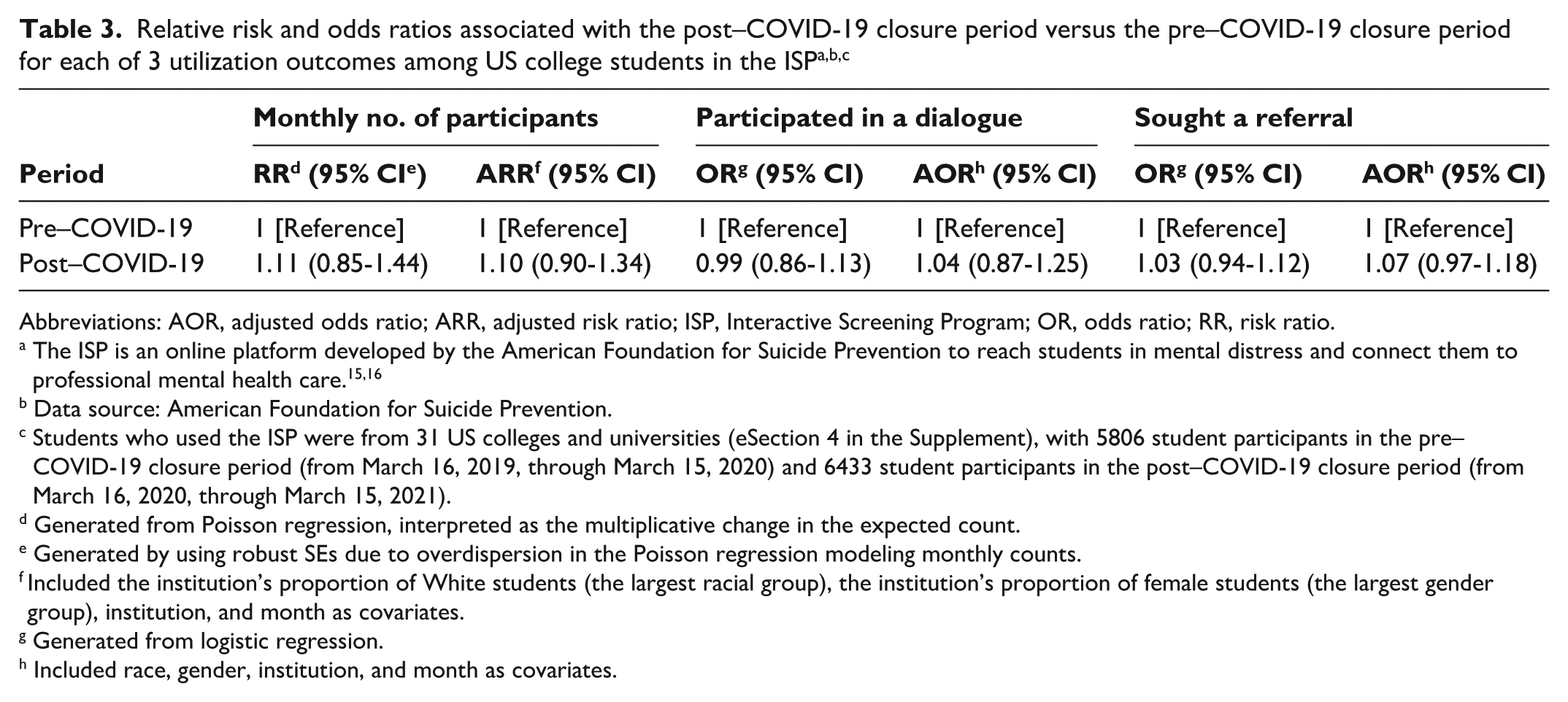
Abbreviations: AOR, adjusted odds ratio; ARR, adjusted risk ratio; ISP, Interactive Screening Program; OR, odds ratio; RR, risk ratio.
The ISP is an online platform developed by the American Foundation for Suicide Prevention to reach students in mental distress and connect them to professional mental health care.15,16
Data source: American Foundation for Suicide Prevention.
Students who used the ISP were from 31 US colleges and universities (eSection 4 in the Supplement), with 5806 student participants in the pre–COVID-19 closure period (from March 16, 2019, through March 15, 2020) and 6433 student participants in the post–COVID-19 closure period (from March 16, 2020, through March 15, 2021).
Generated from Poisson regression, interpreted as the multiplicative change in the expected count.
Generated by using robust SEs due to overdispersion in the Poisson regression modeling monthly counts.
Included the institution’s proportion of White students (the largest racial group), the institution’s proportion of female students (the largest gender group), institution, and month as covariates.
Generated from logistic regression.
Included race, gender, institution, and month as covariates.
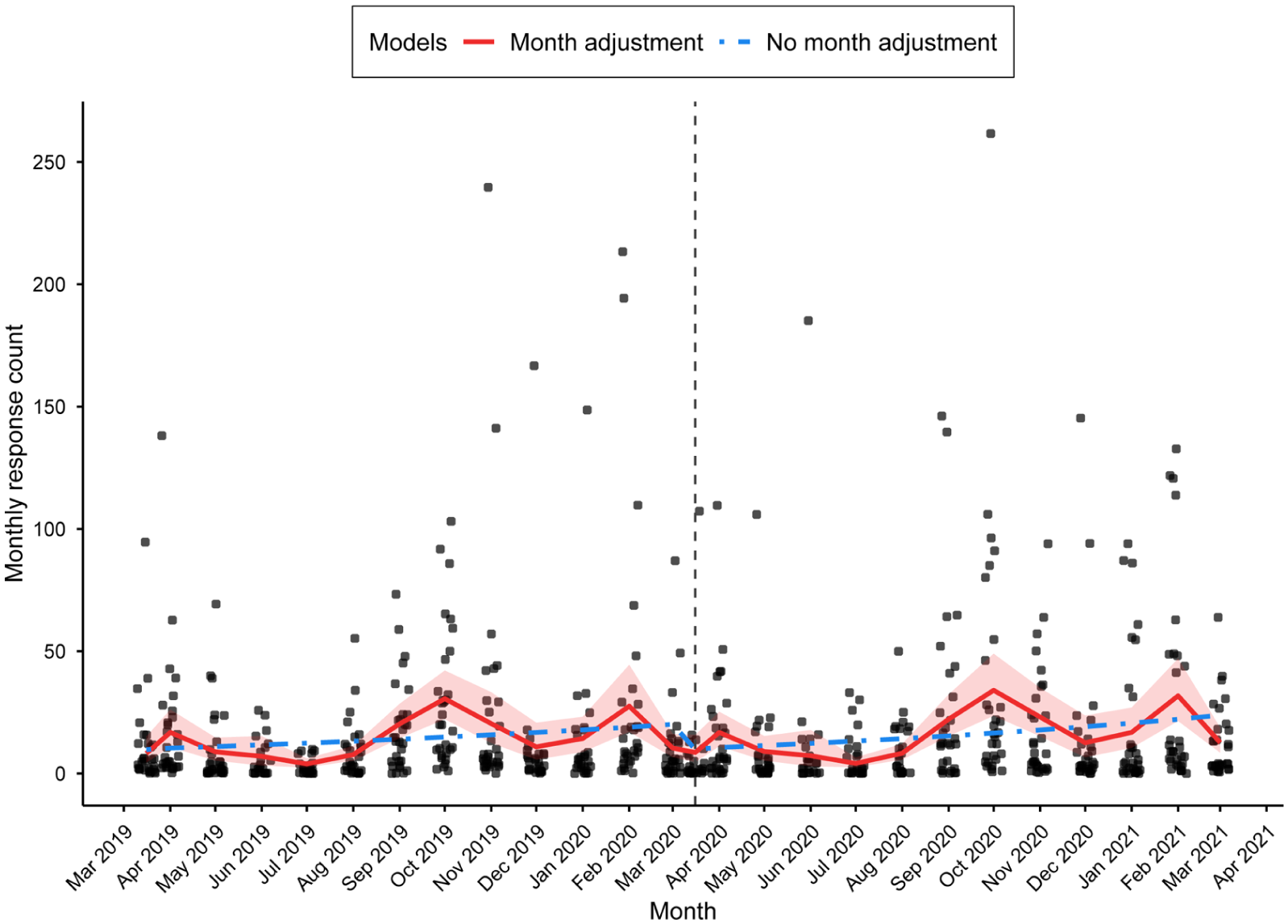
Monthly participation counts in the Interactive Screening Program (ISP) from March 16, 2019, through March 15, 2021, in interrupted time-series regression models with and without adjustments for month effects. The ISP is an online platform developed by the American Foundation for Suicide Prevention to reach students in mental distress and connect them to professional mental health care.15,16 Vertical dashed line indicates COVID-19–related college closures on March 15, 2020. Dots indicate each institution’s count of ISP participants in that month. Shading indicates 95% CIs for the month-adjusted time-series regression, which were generated by using robust SEs due to overdispersion in the data. Data source: American Foundation for Suicide Prevention.
In the sensitivity analyses, excluding institutions with (1) low ISP utilization, (2) inconsistent ISP utilization, or (3) ISP utilization in the top or bottom decile found only 1 difference (eSections 6-9 in the Supplement). After we removed data from institutions in the top or bottom participation count decile, the proportion seeking a referral in the year after campus closures dropped from 11.8% to 10.1% (χ21 = 5.95; P = .01). The sensitivity analyses examining various ways of handling the safety-flagged dialogues did not change the results. Restricting the analysis to March 16 to December 31 of both years (2019 and 2020) resulted in a lower proportion of students seeking a referral in the postclosure period (10.8% vs 12.3%; χ21 = 4.53; P = .03). Finally, when stratifying by race and gender subgroups, we found a higher proportion of Hispanic/Latinx students participating in a dialogue and seeking a referral in the postclosure period.
Lessons Learned
ISP utilization—as measured by mean questionnaire completion per college per month, proportion of participants participating in a dialogue with a counselor, and proportion seeking a referral to care—did not change in the year after March 15, 2020. Overall, our findings suggest that the utilization of the program can be sustained during disruptive periods, such as campus-wide closures.
We believe that our study is the first to evaluate a digital mental health program at multiple institutions using data from periods before and after the COVID-19 campus closures. It advances the literature on digital mental health programs on college campuses by showing that the ISP was able to sustain student engagement and catalyze referrals to care during campus closures. This finding suggests that the ISP could be used to connect students to care during future campus closures caused by a pandemic or other disasters by helping them progress through the first 3 stages of the cascade of care model.
Our findings might encourage use of the ISP even outside the context of campus closures for reaching students located off campus, such as commuter students or students who leave campus during academic breaks. Institutions that pursue such a strategy would want a plan for referring students who are located out of state or out of the country and, thus, might have difficulty using campus services due to state-based licensure. One such option would be to obtain an institutional subscription to a third-party telehealth service that offers mental health care in multiple states.
The sociodemographic differences in ISP utilization before and after the COVID-19 pandemic deserve scrutiny. We found minor shifts to more student participants identifying as female and White. This finding might be explained by differences in how sociodemographic groups experienced the COVID-19 pandemic. One systematic review of longitudinal studies of college students during the pandemic noted that female students reported more severe anxiety, depression, stress, and loneliness than male students. 27 That same review also found differences in trends of various psychiatric symptoms among racial subgroups. Alternatively, differences in access to technology needed to access the platform might explain differences in race. 28 Our subgroup analysis found that Hispanic/Latinx students were more likely to participate in a dialogue and seek a referral in the postclosure period than in the preclosure period. However, the reason for their increased engagement is unclear.
Our sensitivity analyses suggest some nuances in the ability to support seeking a referral to care. First, after the largest and smallest schools were excluded, the proportion who sought a referral to care was significantly lower in the postclosure period than in the preclosure period. One possible explanation is that high-utilization schools were best able to develop a pandemic strategy to support students seeking a referral. If utilization is an indication of school size, those schools might have also been better resourced. Second, a lower proportion of participants sought a referral to care through the ISP during March 15 to December 31, 2020, than during the same period in the prior year. Vaccines 26 were rolled out in late December 2020; perhaps, students were less likely to seek referrals before then and institutions were less likely to offer them.
Limitations and Strengths
This study was limited by several factors. First, differences could not be assessed in the implementation of the program before and after the campus closures (eg, the number of students invited and how they were contacted), which might have influenced utilization metrics. The lack of difference in overall utilization before and after March 15, 2020, might not truly indicate equivalent rates of participation. For example, if institutions considerably ramped up email invitations to participate in the ISP after March 15, 2020, but utilization did not change, this would mean that the proportion of students participating actually decreased. Second, our “seeks referral” variable was based on student-reported interest in connecting to mental health care services, but we lacked data to determine whether students actually connected to such services. Third, limited and variable assessment of students’ socioeconomic characteristics gave us little ability to disentangle factors, such as financial means, that might have influenced differences in utilization among racial groups. Fourth, it is not clear how many students were invited to participate in the ISP, whether invitation procedures differed among institutions, and whether recruitment after the campus closures would have differentially affected students who stayed near campus versus those who returned home.
Strengths of this study included the use of a large dataset from multiple institutions, as well as NLP methods with robust performance metrics to analyze a large amount of text from several thousand participants and infer referral-seeking behaviors.
Conclusions
The ISP’s utilization and function of catalyzing referrals to care did not decrease in the year after the campus closures precipitated by the COVID-19 pandemic. The ISP’s ability to help students progress through the stages of the cascade of care model did not appear to be negatively affected by campus closures. This study provides preliminary evidence that the ISP could support student mental health during potential future campus disruptions.
Supplemental Material
sj-docx-1-phr-10.1177_00333549261453012 – Supplemental material for Mental Health Screening Before and After the 2020 COVID-19 Closures of US College Campuses: A Cross-Sectional Comparison Using Natural Language Processing
Supplemental material, sj-docx-1-phr-10.1177_00333549261453012 for Mental Health Screening Before and After the 2020 COVID-19 Closures of US College Campuses: A Cross-Sectional Comparison Using Natural Language Processing by James Aluri, Susanna Lewis, Ashley M. Witmer, Carlos Aguirre, Zoena Howland, Lida King, Susan Han, Mark Dredze and Holly C. Wilcox in Public Health Reports®
Footnotes
Acknowledgements
The AFSP and the ISP Statistics Jurisdictions were the source of the data files used in this analysis. We acknowledge AFSP staff who assisted with providing data for these analyses.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: J.A., S.L., A.M.W., C.A., Z.H., L.K., S.H., and H.C.W. received funding for this research through a data contract with the AFSP. A.C.W. receives funding from the National Institute of Mental Health (Psychiatric Epidemiology Training Grant T32MH0145920).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J.A. receives research funding from the AFSP. H.C.W. serves on the board of the AFSP and AFSP’s Scientific Council. M.D. receives consulting fees from Good Analytics Inc and Bloomberg LP.
Disclaimer
The funding sources had no role in the study design; collection, analysis, and interpretation of data; drafting of the article; or decision to submit the article for publication. The AFSP reviewed the article for factual accuracy of the description of the ISP program and the acknowledgments of its role in the provision of data.
Data Availability Statement
The AFSP and the ISP Statistics Jurisdictions were the source of the data files used in this analysis. These data are not publicly available.
Supplemental Material
Supplemental material for this article is available online. The authors have provided these supplemental materials to give readers additional information about their work. These materials have not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.