
Abstract
An increase in imported infectious diseases that are unfamiliar to health professionals was expected during the Tokyo 2020 Olympic and Paralympic Games. The National Institute of Infectious Diseases, Japan, therefore developed a pragmatic quantitative methodology to prioritize imported infectious diseases with the greatest implications for medical and public health workers. This approach selected acute-onset infectious diseases recorded in the national surveillance system and defined 2 indicators: absolute caseload and the relative contribution from importations, reflecting potential workload in diagnosis and acute public health responses, and relative importation impact. We prioritized diseases exceeding predefined thresholds for both indicators. The prioritization results, based on simple calculations, identified 15 prioritized diseases and facilitated transparent nationwide public health planning. With increasing global mobility, this method can serve as a useful tool to improve preparedness for mass gatherings and routine public health planning.
Introduction
In 2017 when Tokyo was selected to host the 2020 Summer Olympic and Paralympic Games (hereinafter, Tokyo 2020 Games), 1 millions of visitors from diverse regions were expected to attend. The surge of inbound travelers could increase the likelihood of importing infectious diseases unfamiliar to health professionals, requiring preparedness for this potential public health impact. With a wide range of possible imported infectious diseases, it was essential to prioritize those diseases with the greatest implications for the medical and public health sectors.
Previous approaches to importation risk assessment have applied narrative assessments2-4 and statistical modeling,5-8 whereas disease prioritization relied on Delphi methods,9,10 multicriteria decision analysis,10,11 and qualitative algorithms.10,12 Although these methods have strengths, they generally require substantial resources, including specialized expertise, the involvement of multiple experts, and considerable time for implementation. Because host towns and venues were distributed nationwide, a consistent, comprehensive method readily adopted by individual municipalities was warranted; however, these methods may be challenging for subnational entities to implement. Therefore, a team for surveillance and risk assessment at the National Institute of Infectious Diseases (NIID), Japan, developed a novel approach to prioritize infectious diseases for the Tokyo 2020 Games. Here, we describe this new systematic methodology.
Methods
The overall infectious disease preparedness process for the Tokyo 2020 Games has been previously reported. 13 In that process, infectious disease risks were categorized into 4 types: (1) increased risk of imported cases, (2) increased risk of transmission and a large outbreak, (3) risk of serious outcome, and (4) risk of increased burden on public health responses. The present study focused on the first category: increased risk of imported cases.
Prioritization Procedure
The prioritization procedure comprised 3 steps: (1) selecting candidate acute-onset infectious diseases, (2) defining indicators for prioritization, and (3) identifying high-priority diseases.
Step 1: Selecting candidate acute-onset infectious diseases
Because the Tokyo 2020 Games lasted approximately 3 months, public health concerns focused on acute-onset infectious diseases with relatively short incubation periods. To generate a candidate list of these diseases, we used the case-based notifiable infectious diseases recorded in the National Epidemiological Surveillance of Infectious Diseases (NESID), Japan’s national surveillance system. Under the Infectious Diseases Control Law, 14 clinicians must report notifiable diseases upon diagnosis, often with specific laboratory criteria. Notifications include age, sex, onset date, and presumed/suspected geographic area of infection, facilitating classification as imported or domestic. 15
Of the 87 case-based notifiable diseases, we excluded those with subacute or chronic courses (eg, tuberculosis, syphilis, HIV/AIDS), conditions with nonspecific etiology for notification (eg, acute encephalitis), and antimicrobial-resistant bacteria, given their predominantly nosocomial transmission and limited relevance to community spread during the Tokyo 2020 Games. After these exclusions, 47 acute-onset diseases remained for prioritization.
Step 2: Defining indicators for prioritization
To enable comparison across diseases, we developed quantitative indicators that reflected the potential workload imposed on medical and public health workers.
We first considered the aggregate burden of each disease, representing acute operational workload rather than morbidity or mortality, because the clinical severity was evaluated separately as the risk of serious outcomes within the comprehensive risk assessment outlined previously. 13 For clinicians and laboratory staff, this acute operational workload included clinical assessment, laboratory testing, and case notification; for public health staff, it included case investigation and contact tracing. Because such workload depends largely on disease frequency, we used the total annual number of case notifications as an indicator of “absolute burden,” regardless of place of infection.
We next considered the potential impact of increased international travel on disease importation. While diseases with mostly domestic cases are affected to a limited extent, those with predominantly imported cases may increase substantially, posing additional diagnostic and response challenges, particularly when managing unfamiliar diseases. We therefore defined an “importation index” as the relative frequency of imported cases to domestic cases, representing relative importation impact.

We excluded cases with unknown suspected areas of infection from the calculation. We determined thresholds for both indicators through consultations with epidemiologists at NIID. In the absence of validated benchmarks for this novel framework, we considered expert consensus to be the most appropriate for setting thresholds. With respect to operational workload and epidemiological relevance, we agreed that more than 10 annual notifications represent a meaningful threshold for absolute burden, while the median value represented a reasonable threshold for the importation index, given its wide variation.
Step 3: Identifying high-priority diseases
Using the thresholds defined previously, we identified diseases that have both high absolute burden and high relative importation impact.
Data Applied for Prioritization Method
We applied the prioritization method using data from the NESID Annual Report for 2015, 16 which was the most recent official dataset available at the time of evaluation in 2017. Because Zika virus infection became notifiable in February 2016, we used provisional 2016 data for this disease. 17
Ethical Consideration
All data analyzed are publicly available with no personally identifiable information. Therefore, the Ethics Committee of the Japan Institute for Health Security considered this study not human subjects research because of the lack of interaction with or collection of identifiable information about human subjects and because it was conducted as part of public health surveillance.
Results
Application of the Prioritization Method for the Tokyo 2020 Games
Among the 47 diseases identified in step 1, the importation index could not be calculated for 13 diseases with no imported cases. For the remaining 34 diseases, the median importation index was 0.05 (IQR, 0-0.45).
Fifteen diseases exceeded thresholds for both absolute burden and the relative importation impact (Figure) and were, therefore, prioritized for preparedness.
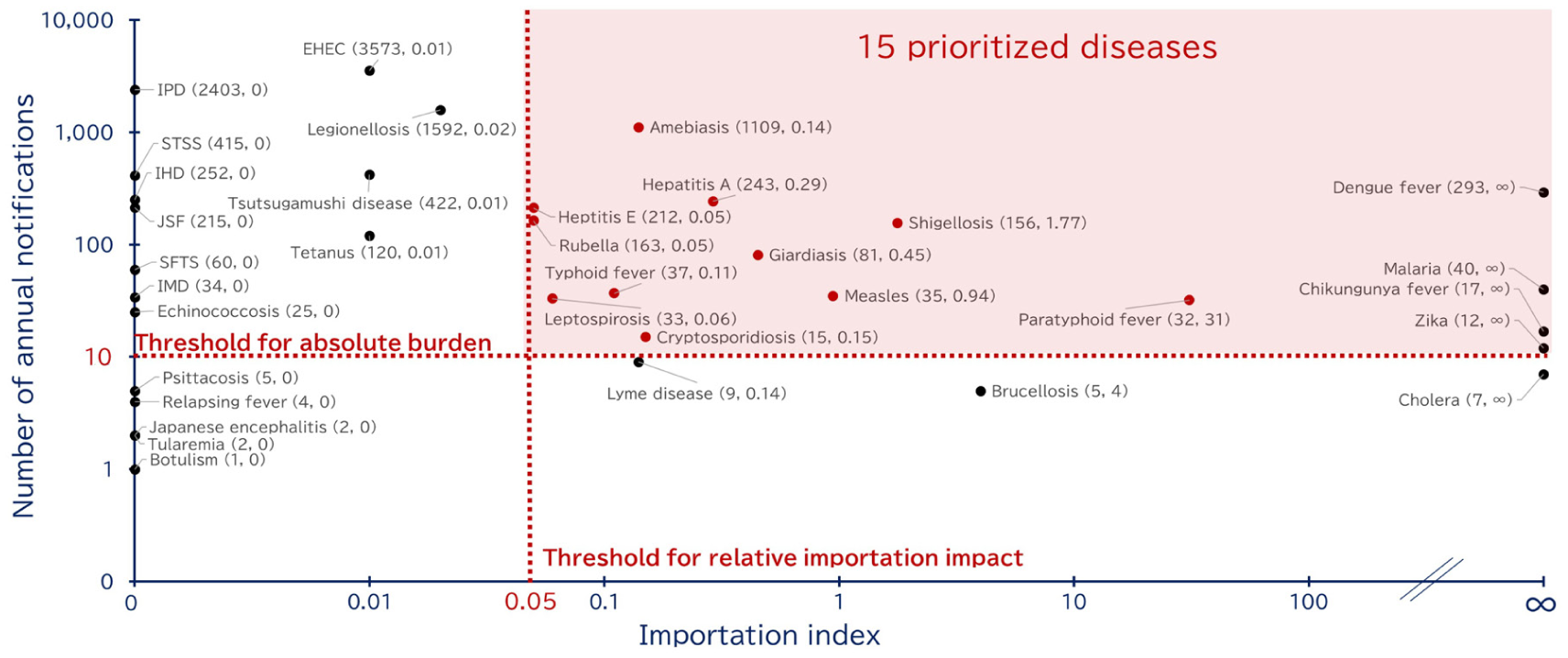
Annual number of notifications and importation index among acute-onset infectious diseases notified to NESID in 2015 (N = 11 624). Abbreviations: EHEC, enterohemorrhagic Escherichia coli infection; IHD, invasive Hemophilus influenza disease; IMD, invasive meningococcal disease; IPD, invasive pneumococcal disease; JSF, Japanese spotted fever; NESID, National Epidemiological Surveillance of Infectious Diseases; SFTS, severe fever with thrombocytopenia syndrome; STSS, severe invasive streptococcal infection; Zika, Zika virus disease. The importation index was not applicable for the following diseases with no notifications: anthrax, avian influenza, diphtheria, Middle East respiratory syndrome, plague, poliomyelitis, Q fever, rabies, severe acute respiratory syndrome, smallpox, viral hemorrhagic fever, West Nile fever, and yellow fever. For the following diseases with no reported domestic cases, the importation index was not calculable because the denominator was 0. However, to express the extent of relative impact, we demonstrated it as “∞”: Dengue fever, malaria, Chikungunya fever, Zika.
Discussion
Preparation Based on the Prioritization Results
The prioritization results directly informed public health planning at both national and local levels. In 2017, NIID disseminated this prioritization framework with its prioritization result, recommending that municipalities apply it within their jurisdictions. 18 Based on the findings, public health authorities could initiate preparedness activities targeting prioritized diseases, including disseminating disease fact sheets, recommending vaccines, and ensuring laboratory resources for testing uncommon pathogens. The early release of prioritization results was critical for enabling such preparation, implemented across various public health entities.
Actual Infectious Disease Events During the Tokyo 2020 Games
Because of the COVID-19 pandemic, the Tokyo 2020 Games were postponed by 1 year and held with a drastic reduction in visitors and exceptionally strict infection control measures. This unique situation likely contributed to the finding that no surges or major events related to the 15 prioritized diseases were observed and that infectious disease cases were mostly limited to sporadic COVID-19 infections. 19
Benefits of This Novel Prioritization Approach
Despite the absence of prioritized infectious disease events or surges during the Tokyo 2020 Games, this novel approach demonstrated distinct benefits.
First, it provided practical guidance. Because the methodology relies on simple calculations using familiar national surveillance data, it was readily accepted by public health personnel. The comprehensive quantitative results facilitated mutual understanding among diverse partners, including policymakers, national authorities, and local health workers, enabling coordinated decision-making.
Second, given consistent high global mobility, this methodology is applicable not only to mass gatherings but also in routine practice. With growing inbound travelers to Japan, periodic assessments would enhance public health planning suited to current circumstances. Furthermore, the underlying concept of this methodology is transferable; in countries or regions with surveillance systems collecting comparable epidemiological information, this framework can serve as a practical tool.
Third, a single figure that simultaneously visualizes absolute and relative indicators enhanced usability. This summary figure can serve as an effective risk communication tool for relevant professionals and the general public, providing clear information on diseases that warrant particular attention before international travel.
Despite clear advantages of this novel prioritization method, we noted several limitations. The first limitation was in the context of application. Because the Tokyo 2020 Games were held under highly unusual circumstances, we were unable to comment on the full potential or generalizability of this prioritization method. Nevertheless, the methodology can be reasonably applied to other settings, and repeated applications can enhance its usefulness and identify potential gaps.
The second limitation stemmed from the nature of the surveillance system and its data. Nonnotifiable diseases could not be assessed, and those with rapidly changing epidemiology, including emerging or reemerging diseases, could have been overlooked. Because this limitation had already been considered in the comprehensive risk assessment, Japanese authorities established an additional system, referred to as the Undiagnosed Serious Infectious Illness Surveillance System. 13 This system was designed to capture severe illnesses that cannot be diagnosed through routine clinical practice at medical facilities, thereby compensating for this limitation. Although complementary tools may be necessary, this methodology can reasonably assess imported diseases by maximizing the use of existing data.
Third, because most imported case patients reported to surveillance are Japanese residents, demographic characteristics and behaviors abroad could differ from those of inbound visitors, potentially leading to an over- or underestimation of the relative impact from importations. Furthermore, traveler distribution during mass gatherings can vary from routine patterns. Therefore, the data used in this prioritization might not fully reflect the risk profile of event-specific inbound travelers. Considering additional information on country-specific inbound travelers and event-related attendance, where available, would enhance the interpretation and contextualization of the prioritization results.
To prepare for the Tokyo 2020 Games, NIID, Japan developed a pragmatic methodology to prioritize imported infectious diseases. With its distinct benefits, this method can serve as a useful tool to prepare for mass gatherings and conduct routine public health planning.
Footnotes
Acknowledgements
The authors appreciate the contributions and support of local public health institutions and medical facilities for national surveillance. We are grateful to Taro Kamigaki, PhD, of NIID/Japan Institute for Health Security for his support to publish this work. In 2025, NIID merged with the National Center for Global Health and Medicine to form the new Japan Institute for Health Security; however, for this study we maintain “NIID” to reflect the name at the time of this project.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by the Health, Labour and Welfare Policy Research Grants (grant no. 24LA2002).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data underlying this article are available in the National Epidemiological Surveillance of Infectious Diseases of Japan Institute for Health Security at https://www.jihs.go.jp/. The datasets were derived from sources in the public domain: ![]() .
.