
Abstract
Peer support groups are the most utilized form of treatment for individuals recovering from substance abuse and substance dependence. This study examined an understudied peer support program (Self-Management and Recovery Training [SMART] Recovery), which is distinct from traditional 12-step models. Although treatment planning for substance use disorders is not the primary focus of vocational rehabilitation (VR), persons with disabilities are at increased risk for these disorders. Due to the bio-psycho-social nature of substance use disorders, VR counselors must consider ethical treatment recommendations for clients who demonstrate need for supplemental treatment. This descriptive-survey study investigated two samples of member and facilitator characteristics, motivations, and recovery goals among the SMART Recovery community. Implications for VR counselors making best practice recommendations for clients with substance use disorders are discussed.
Keywords
The rate of substance use disorders in the United States presents a serious public health concern. According to the Substance Abuse and Mental Health Services Administration (SAMHSA; 2011), 8.7% of the U.S. population was classified with substance dependence or substance abuse. The National Institute on Drug Abuse (NIDA; 2011) noted that nearly 9% of Americans reported using illegal drugs; these results have continued to climb over the last decade. For persons with disabilities, the rates are even more concerning. According to the National Association on Alcohol, Drugs and Disability (NAADD; 2013), persons with a disability are 2 to 4 times more likely to experience substance abuse compared with the nondisabled population. Abuse rates among persons with disabilities vary considerably depending on the nature of the disability. Acquired versus lifetime disability status also impacts abuse patterns, with higher abuse and dependence rates among those living with acquired disabilities (Radnitz, Tirch, Vinciguerra, & Moran, 1999). Within the disability community, approximately half of all persons with spinal cord injury, traumatic brain injury (TBI), and psychiatric disability experience substance use disorders (NAADD, 2013). Persons with physical disabilities and limited activity levels were found to be at increased risk for substance use disorders (Turner, Lloyd, & Taylor, 2006).
Among persons who acquire TBI, nearly half were found to be intoxicated at the time of injury, and up to a third continued to abuse substances postinjury (Radnitz et al., 1999). Prior to spinal cord injury resulting in disability, 65% indicated problem drinking before an accident or injury, and 62% of those with spinal cord injury were found to be intoxicated at the time of injury. Most (68%) continued to abuse substances after release from a rehabilitation hospital (Radnitz et al., 1999). Another study (Radnitz et al., 1996) found that the lifetime prevalence rates for dependence was significantly higher (37.6%) among spinal cord injury survivors compared with the nondisabled population.
The reasons for the disproportionate rates of abuse and dependence among persons with disabilities are likely complex, but some of the reasons include the unique risk factors for groups of people with disabilities, including medical, social, psychological, and financial risk factors (Radnitz et al., 1999). Living with multiple stigmas may serve as an additional barrier to treatment seeking, and having to take medications that both contribute to patterns of abuse, as well as hinder traditional “sobriety only” models of treatment likely contribute to increased risk. In addition, persons seeking traditional rehabilitative services may not be screened for substance abuse, and VR counselors may not be trained to assess or refer clients at risk for treatment needs. Furthermore, many who meet criteria for abuse or dependence may not have financial resources for treatment costs. Given the lower employment rates for people with disabilities, many people may be without health insurance that could cover outpatient treatment. Another factor unique to this group is the use of prescribed medications to alleviate symptoms. For instance, some medications to treat psychiatric symptoms (including those for attention-deficit/hyperactivity disorder [ADHD], anxiety disorders, and depression) have abuse potential, which can complicate treatment. Many people with musculoskeletal disabilities also live with chronic pain, which is often treated with prescribed narcotic pain medications (Falvo, 2013). These medications have high potential for abuse and dependence. Nearly half of all people who were prescribed pain medications for spinal cord injury and chronic pain reported abusing their medications (Radnitz et al., 1999). In addition, those with both spinal cord injury and chronic pain who viewed alcohol or pain medications as a way to cope with lack of sleep, mood swings, and social isolation, were more likely to abuse substances (Radnitz & Tirch, 1995). The increased availability and affordability of legal drugs with abuse potential presents a unique risk factor for onset of abuse and dependence for this subpopulation. The risk may be even greater for those who also view drugs and alcohol as a viable coping mechanism to alleviate physical and social symptoms of their conditions.
Treatment Options
Access to care for substance abuse disorders is a problem. Only 7.9% of those who need treatment for a substance use disorder receive it at a specialty facility (i.e., hospital, drug or alcohol rehabilitation or mental health center; SAMHSA, 2011). Inability to afford treatment, lack of health insurance, employer and community stigma, lack of education regarding treatment options, and lack of time for treatment are primary contributors to low rates of treatment access (SAMHSA, 2011). For individuals with disabilities, the added complications of adjusting to a disability and navigating the unique risk factors for this group may result in even more barriers to treatment compared with those living without a disability. For instance, meeting spaces for peer support groups are often held in available community spaces such as churches or nonprofit agencies, which do not always provide wheelchair accessibility. Furthermore, according to the Bureau of Labor Statistics (2014), addictions and behavioral disorder counselors are not required to have any knowledge or training about disabilities. In many cases, education beyond a high school diploma is not required for certification and employment in these settings.
One option for individuals with disabilities is vocational rehabilitation (VR) counseling services. VR services focus on the physical and psychosocial adjustment to disability, with a primary emphasis on vocational and career goal setting. Treatment for substance abuse is not an explicit focus of VR services nor is it typically a primary goal of VR services. Despite this, many clients who are eligible for VR services are at risk for abuse (NAADD, 2013). To supplement VR services, rehabilitation counselors can screen clients who are at increased risk and provide ethical recommendations for additional treatment services. Depending on the nature of the primary disability or illness, clients may be eligible to receive inpatient or outpatient treatment for substance abuse. Even for those who are eligible to receive funding for additional counseling services, the time commitment and additional stigma may be significant barriers to seeking these types of treatments. An alternative, supplemental, and free option is available in the form of peer support groups. These programs continue to be the most predominant method of treatment for substance abuse disorders. Of the 4 million persons who received treatment for substance abuse in 2011, 2.1 million received treatment exclusively at a peer support group (SAMHSA, 2011). Research supports peer support group attendance in conjunction with professional treatment (Humphreys et al., 2004) as these groups are best viewed as a form of continuing care to prevent relapse.
Support groups provide a recovery-oriented, social support network that focuses on achieving and maintaining abstinence from abused substances. Peer support programs are free, available to voluntary participants on a daily or weekly basis in many communities, and serve as a source of general support for individuals who wish to recover from addictive behaviors (Moos, 2007). Rigorous research over many years supports the notion that social support and supervision from peer groups enhances the process of remission (Beattie, 2001; Bond, Kaskutas, & Weisner, 2003; Moos, 2007; Project MATCH Research Group, 1998). Project MATCH Research Group (1997) noted that 12-step facilitation helped clients to disengage from social networks supportive of drinking and encouraged them to invest in a network that supported abstinence. Project MATCH Research Group (1998) found that clients who participated in 12-step treatment conditions had higher percentage of days abstinent and a lower number of drinks per drinking day 3 years after the initial study than clients who received the cognitive-behavioral treatment or motivational therapy conditions. Participation in an external peer support group was associated with this effect.
Reduction in peer support group involvement has been shown to reduce the likelihood of abstinence (Bond et al., 2003). Beattie (2001) found that higher levels of social support increased positive results for substance abusers by 22% in a meta-analysis of literature concerning substance abuse treatment outcomes. The support received from a recovery group is distinct in its provision of consistent contact with other individuals who share a common goal and who encourage substance use reduction (Bond et al., 2003). Support groups also teach and model refusal skills, provide specific suggestions for avoiding situations in which relapse is likely, have accessible meeting times, and engage in sponsorship relationships. These different types of support provide a foundation for present and future abstinence (Kaskutas, Bond, & Humphreys, 2002).
12-Step Models: Principles, Philosophy, and Mechanisms for Change
A majority of the literature supporting the efficacy of peer support programs pertains to 12-step groups (Branscum, 2010; Galanter, 2008; Knack, 2009; McKellar, Stewart, & Humphreys, 2000; Project MATCH Research Group, 1997; Ye & Kaskutas, 2009). Alcoholics Anonymous (AA) is the most popular and most accessible 12-step program (Branscum, 2010). Membership exceeds one million members in the United States alone (White & Madara, 2002). There are no fees for membership; the organization is self-supporting through its own contributions. The AA and other 12-step approaches are typically based on the belief that substance dependence is a spiritual and a medical disease (Ferri, Amato, & Davoli, 2006). The only requirement for 12-step program membership is a desire to stop using substances. AA follows a 12-step model that suggests ways in which the person may develop a satisfying life without alcohol. Foundational premises of AA include (a) persons with alcohol dependence cannot manage their lives, (b) persons with alcohol dependence cannot stop drinking alone, and (c) to stop drinking and manage life, surrender to a higher power is necessary (AA World Services, 1939). By admitting and accepting a lack of control or powerlessness, one gains control according to the program’s philosophy. The program emphasizes the reliance on a “higher power” to restore sobriety. The 12-step model has been adopted for other substances, including narcotics, cocaine, and other substances and behaviors.
SMART Recovery: Principles, Philosophy, and Mechanisms for Change
Self-Management and Recovery Training (SMART) is a peer support, recovery program that focuses on helping members recover from all types of addiction and addictive behaviors. The program focuses on the following: building and maintaining motivation; coping with urges; managing thoughts, feelings, and behaviors; and teaching members to live a balanced life (SMART, 2012). SMART Recovery groups provide an interactive structure for planned discussion (Horvath & Velten, 2000). Meetings are facilitated by a nonprofessional volunteer who has undergone an online training course providing the required knowledge of the program’s foundations (Horvath & Velten, 2000). As of 2012, 698 SMART meetings operated in the United States, Canada, Australia, and Great Britain (Allwood & White, 2013).
SMART Recovery groups are distinct from traditional 12-step models, and may be more aligned with current rehabilitation counseling practices in several ways. First, 12-step models often require total abstinence as a requirement for membership. This can be problematic for many people with disabilities who take prescribed, narcotic pain medications, or other medications with abuse potential, as part of their treatment and rehabilitation plan. SMART Recovery does emphasize the importance of abstinence, but does not require it as a goal for members. The SMART philosophy emphasizes harnessing individual empowerment using cognitive-behavioral and rational emotive techniques to foster change in abuse patterns (SMART, 2012). In contrast, traditional 12-step programs emphasize a dependence on a higher power and working through 12 steps to reach sobriety. SMART Recovery meetings utilize trained facilitator-led structured discussions, rather than peer-led storytelling based on the 12 steps. Furthermore, membership in SMART Recovery is considered finite and available on an as-needed basis compared with a lifetime membership commitment for sobriety and access to one’s higher power through AA. These distinguishing features highlight SMART Recovery’s alignment with the rehabilitation field’s emphasis on independent and autonomous living, and a consideration for each individual’s unique needs as he or she adjusts to a disability in the context of facilitated support. For these reasons, SMART Recovery peer groups may be a good fit for many people with disabilities seeking supplemental support for their recovery from addiction and who choose not to participate in12-step programs.
Little research exists to date that supports the efficacy of SMART Recovery (Horvath & Yeterian, 2012; Humphreys et al., 2004). A few studies (Horvath & Velten, 2000; Humphreys et al., 2004) have focused on explaining the program’s philosophy and providing conceptual support for the program. Li, Feifer, and Strohm (2000) highlighted philosophical differences between SMART Recovery members when compared with members of AA. Results indicated that individuals in SMART Recovery demonstrated more of an internal locus of control and less dependence on a higher power when it came to regulating drinking (or drug)-related behaviors compared with 12-step members. Hester, Lenberg, Campbell, and Delaney (2013) found that individuals who attended SMART Recovery meetings, and Overcoming Addictions (a web application based on the SMART Recovery program), demonstrated an increase in percentage of days abstinent, reduction in substance related issues, and a reduction in drinks per drinking day. Penn and Brooks (2000) mentioned no statistically significant differences in outcome for 12-step and SMART Recovery participants on the Addiction Severity Index Scale (ASI), alcohol, drug, psychiatric, legal, and employment composites, though statistical data were not reported. A. J. Brooks and Penn (2003) also found that individuals with co-occurring mental health and substance use diagnoses had positive outcomes as a result of attending both 12-step and SMART Recovery meetings. No research was found outlining SMART Recovery members with disabilities. Clearly, more research is needed on SMART Recovery communities.Rehabilitation counselors have a duty to be aware of the high rate of substance use disorders among persons with disabilities, as well as the barriers individuals may encounter when considering suitable treatment opportunities. Familiarization with the treatment options that exist for this population will also assist providers in making informed and ethical referrals when necessary. Research shows that peer support group involvement reduces substance abuse (Humphreys et al., 2004). Much of the research that exists has centered on traditional 12-step programs such as AA or Narcotics Anonymous. Humphreys et al. (2004) suggested that these findings will likely extend to other peer support organizations; however, little research exists to date that supports this assumption. A greater understanding of other, nontraditional models (such as SMART Recovery) may prove useful to rehabilitation counselors as they collaboratively design treatment plans with their clients.
Because of the limited research conducted on SMART Recovery groups, the current study aimed to provide preliminary information on SMART Recovery, an understudied recovery group that may be a fit for people with disabilities who are in need of supplemental peer support for addiction disorders. A two-sample, exploratory descriptive-survey approach was utilized to investigate the characteristics, motivations, and recovery goals of SMART Recovery members and facilitators, with the intention of determining the referral potential for this resource when working with clients who live with a disability and substance abuse disorder. The results from this study can be used to inform subsequent research questions that will likely benefit the disability and rehabilitation communities. The following research aims guided the current study: Describe members of the SMART Recovery community, including the percentage of members with a disability, and description of the disability categories. Describe participants’ motivations for membership in the community. Describe SMART facilitators and their educational and training backgrounds that prepared them for facilitation. Provide rank ordering of members’ recovery goals. Provide rank ordering of facilitators’ recovery goals.
Method
Participants
Sample 1 consisted of 81 participants. They were all self-selected and voluntarily participated in meetings. Inclusion criteria required that all participants were 18 years or older and had been attending SMART Recovery meetings for least 3 months. Participants’ attendance at SMART Recovery meetings ranged from 3 months to 10 years, with a mean of 1.58 years (SD = 1.81). Participants ranged in age from 18 to 72 years, (M = 48.1; SD = 13.1). Most participants were male (66.7%). Most reported having a disability (65%). See Table 1 for full participant demographic data.
Demographic Characteristics of SMART Recovery Members.

Note. Percentages may not total 100 due to rounding. SMART = Self-Management and Recovery Training.
Sample 2 consisted of 42 SMART Recovery facilitators. Facilitators ranged in age from 20 to 76 years, (M = 52.4; SD = 13.79). Facilitators reported a range of years as a SMART Recovery facilitator from less than 1 year to 23 years (M = 5.95; SD = 5.877). The mean number of SMART Recovery meetings facilitated per month was 3.42 (SD = 2.96). See Table 2 for full participant demographic data.
Treatment Characteristics of SMART Recovery Members.
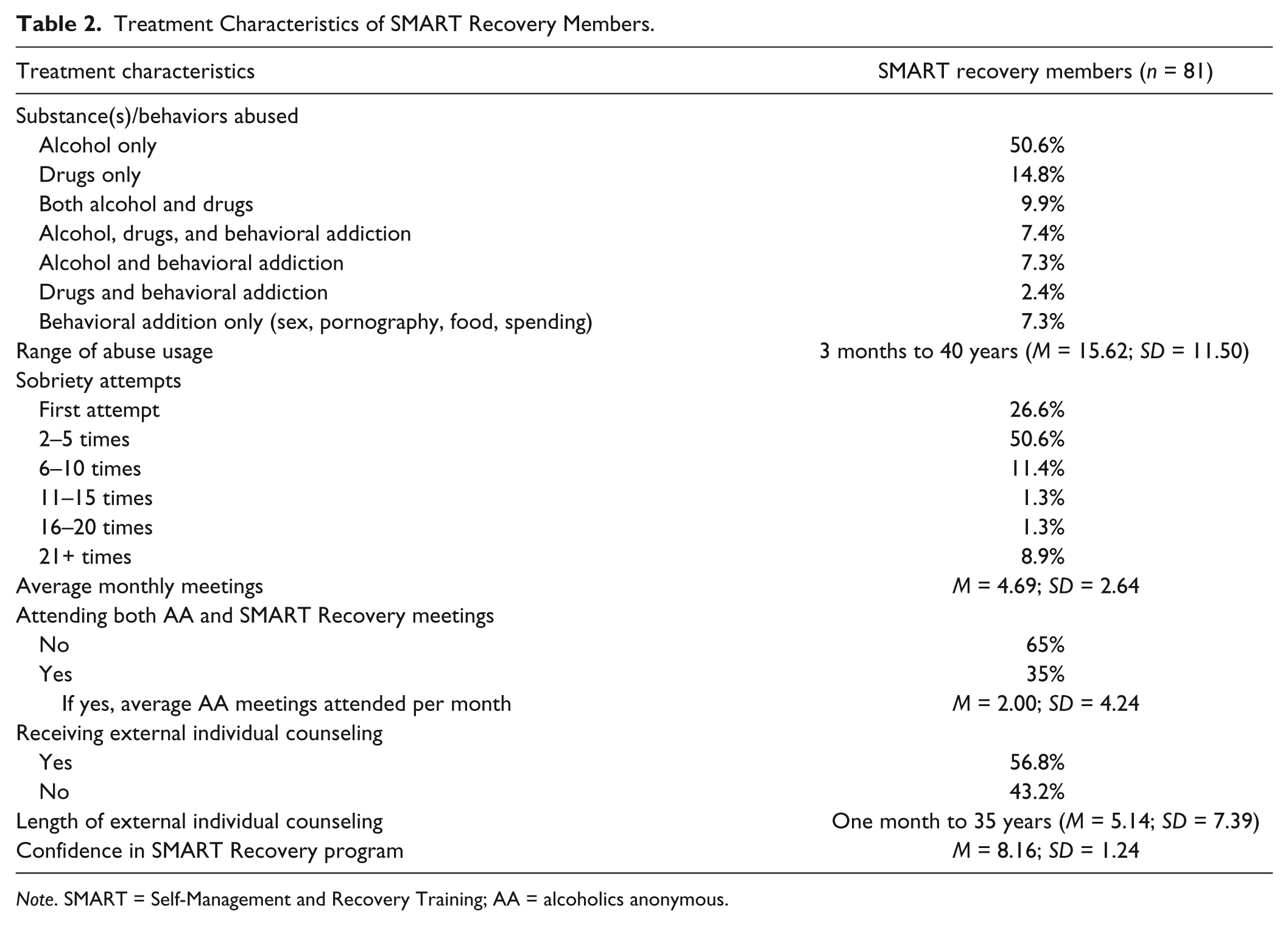
Note. SMART = Self-Management and Recovery Training; AA = alcoholics anonymous.
Procedures
Administrative personnel in SMART Recovery were contacted about this research project and agreed to provide contact information. Emails were sent to 55 SMART Recovery facilitators asking them to distribute research packets to participants in their groups who met eligibility criteria for the research project. From these 55 emails, 14 SMART Recovery facilitators were identified as being willing and able to distribute packets to eligible group members who met inclusion criteria. All research participants were informed in writing that their participation was voluntary and they were free to withdraw from the study at any time without penalty. Participants were given a US$10 gift card to a national retail chain as compensation for their time. A total of 150 packets were distributed. Eighty-one completed packets were returned to the lead investigator for a final response rate of 54%. The Institutional Review Board at the primary investigator’s participating institution approved this study.
The same 55 SMART Recovery facilitators were recruited to participate via a second email approximately 6 to 8 months later. Emails contained informed consent, outline of research project, and a link to an electronic survey via SurveyGizmo. All participants were informed in writing that their participation was voluntary and they were free to withdraw from the study at any time without penalty. No compensation was given to these participants. Out of the 55 SMART Recovery facilitators contacted to complete the survey, 42 completed the online surveys for a final response rate of 76.4%.
Instruments
A 47-item survey designed to investigate the research aims was sent to a pilot sample of 27 SMART participants. The items asked participants to respond to a range of demographic items as well as specific questions pertaining to addiction and recovery, including rank ordering recovery goals. In addition, two open-ended questions asked participants to explain their motivations for belonging to SMART Recovery and explain their motivations for switching groups if applicable. Two of the authors generated a list of potential items after determining research questions. This list of potential items was brought to a group of three faculty members in the department, for which the lead investigator teaches, who served as research advisors on this project. This group along with the lead investigator determined the final items to be piloted. The data from the pilot sample revealed a need to revise some items for clarification. The survey was revised and sent out to a larger sample that yielded the 81 participants in Sample 1 used in the current analysis. Example items included a 9-point Likert-type question: “How much confidence do you have in the SMART Recovery program to help you with your recovery goals?” Also, a six-option multiple-choice item: “How many times in your lifetime have you made the decision and taken action to get sober/clean?” The survey for the facilitators contained 12 items, mostly demographic in nature, with one rank ordering item pertaining to recovery goals. Several items were open-ended questions asking participants to describe their motivations for becoming facilitators and the preparation they felt was most useful to them in this role. Participants in both samples were provided a list based on a range of recovery goals from the counseling literature, AA philosophy, and stated SMART goals. Members were given 7 goals to rank and facilitators were given 11 goals to rank. Both groups had the opportunity to provide additional goals not included in the lists. The lists of goals were a mix of research findings on successful factors for recovery, factors specific to disability adjustment, specific SMART principles, and specific 12-step principles. As the items for Sample 2 were standard demographic items or were similar to items that had been piloted by the participants in Sample 1, this survey was not pilot tested.
Data Analysis
To determine the percentage of the sample who reported having a disability, a frequency count was done in IBM SPSS version 22. Frequency counts were also completed to determine the remaining percentages of the participants’ demographic information, excluding age and length of facilitation. Means and standard deviations were calculated for items pertaining to confidence in the program, ages, number of meetings attended, and the lengths of external counseling, substance usage, and SMART Recovery facilitation. The percentages pertaining to the treatment characteristics of SMART Recovery members, including substances abused, sobriety attempts, external counseling, and the attendance of both AA and SMART Recovery, were calculated via frequency counts. In addition, members ranked the importance (1 = highest importance, 7 = lowest importance) of factors for their recovery and facilitators ranked the program’s goals. A frequency count was used to calculate the percentage of each response ranked within participants’ top three most important factors.
Content analysis was applied to describe the SMART Recovery members’ and facilitators’ responses to open-ended questions in a systematic and triangulated manner (Denzin, 1978; Elo & Kyngäs, 2008; Krippendorff, 1980, 2012). Although typically used with denser text, content analysis can still be used with sparser text, such as open-ended survey questions, and is often utilized over other types of code-based approaches (Jackson & Trochim, 2002). The organization of the content analysis followed the outlined steps presented by Elo and Kyngäs (2008), which includes open coding, creating categories, and abstraction. Three of the four researchers independently read all participants’ transcribed responses to develop investigator triangulation (Denzin, 1978; Elo & Kyngäs, 2008). Each researcher openly coded the data by developing concepts to represent the content of the data (Elo & Kyngäs, 2008). Once this was completed, all three researchers publicly reviewed and compared the generated concepts. Consensus of the concepts was reached through discussion and negotiation, and the data were recorded before identifying the categories. Each researcher then conducted an individual list of categories from the concepts generated. Consensus of categories was reached by the team through discussion and negotiation. Categories were then consolidated and formally created when consensus was reached (Elo & Kyngäs, 2008).
The members’ responses to the open-ended question for membership motivation generated six categories that were consolidated to four categories. The facilitators’ responses to facilitation motivation were consolidated from five categories to four. Responses for facilitation preparation were consolidated from four categories to three. Categories were generated, as opposed to themes, due to the sparse text content and to align accurately with Elo and Kyngäs’s (2008) outlined steps. Abstraction and direct quotation of the participants’ responses, cited in the Results section, were identified as those that best illustrate the overall categories (Elo & Kyngäs, 2008; Wolcott, 2009).
Reflecting and presenting the participants’ responses to the open-ended questions was established by following four criterion constructs of trustworthiness: (a) credibility, (b) dependability, (c) transferability, and (d) confirmability (Lincoln & Guba, 1985). Multiple researcher involvement established investigator triangulation and enhanced the credibility of the findings through the convergence of the investigators’ perspectives (Denzin, 1978; Lincoln & Guba, 1985). Abstraction and direct quotation of participants’ responses developed transferability by providing descriptive evidence that supports the data analysis and helps to determine the degree to which the analysis can be discerned to other contexts (Lincoln & Guba, 1985). Dependability was established by rigorously following the outlined protocol explicitly detailed in the method of data collection and its analysis to act as a guideline for future replications (Lincoln & Guba, 1985). An audit trail of detailed records was kept that included verbatim transcriptions and original copies of all participants’ responses to provide confirmability (Charmaz, 2006; Lincoln & Guba, 1985). In addition, an ongoing reflexivity process was completed verbally by three of the four coding members to deconstruct their own thoughts and beliefs that may bias the research (Shenton, 2004).
Results
Sample 1
SMART Recovery participants reported attending an average of 4.69 SMART Recovery meetings per month (SD = 2.64). As shown in Table 3, SMART Recovery participants reported abusing a variety of substances. These participants reported abusing the substance and/or engaging in the behavior they were seeking help with for a range from 3 months to 40 years (M = 15.62; SD = 11.50). When asked how much confidence (out of 10) they had in the program to help them meet their recovery goals, participants reported a mean of 8.16 (SD = 1.24).
Demographic Characteristics of SMART Recovery Facilitators.
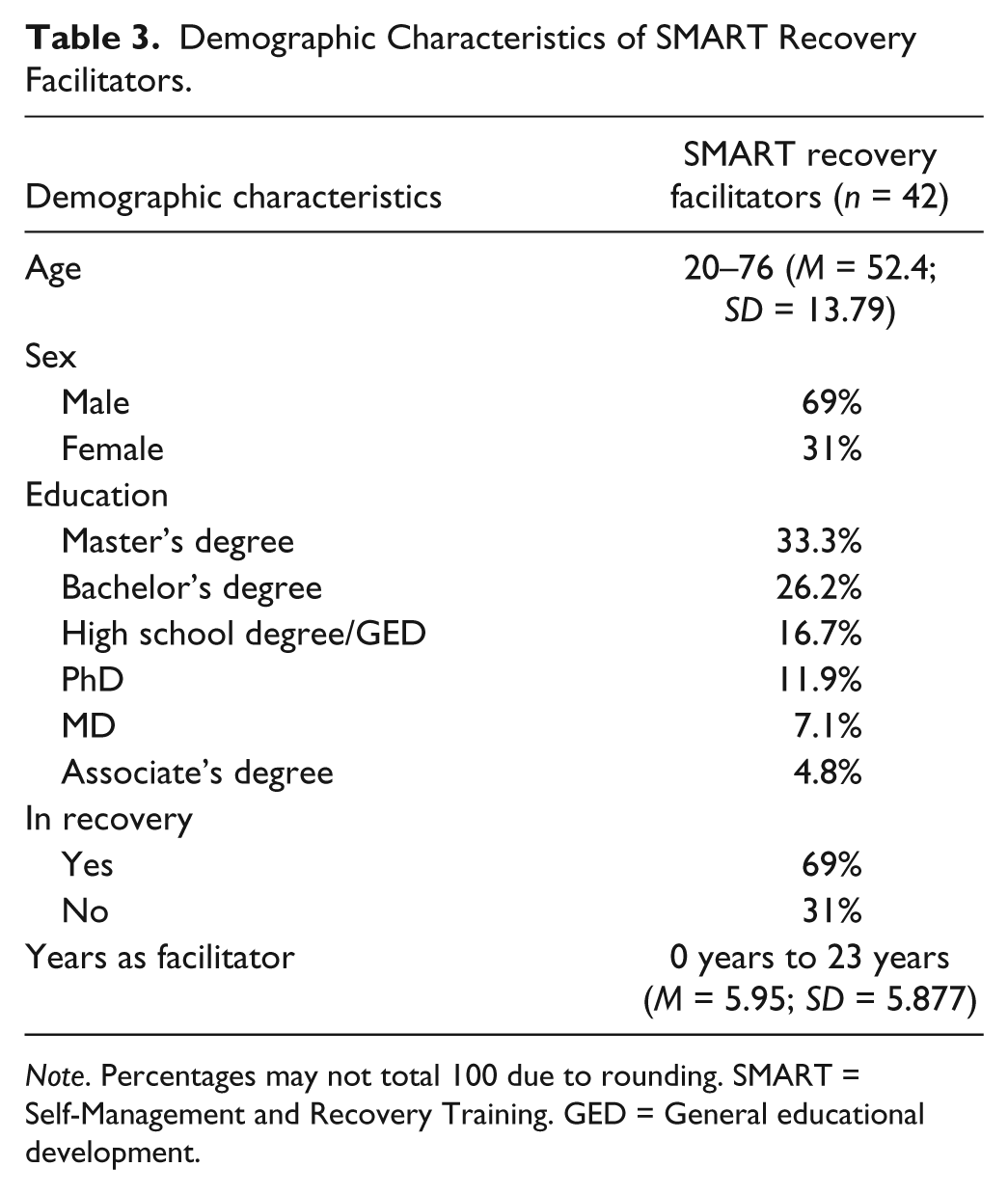
Note. Percentages may not total 100 due to rounding. SMART = Self-Management and Recovery Training. GED = General educational development.
Participants ranked the importance (1 = highest importance, 7 = lowest importance) of seven factors for their recovery and their top three ranked responses were calculated (see Figure 1). Participants had the opportunity to provide other factors not included in the list. No participants, however, provided any qualitative responses for this question.
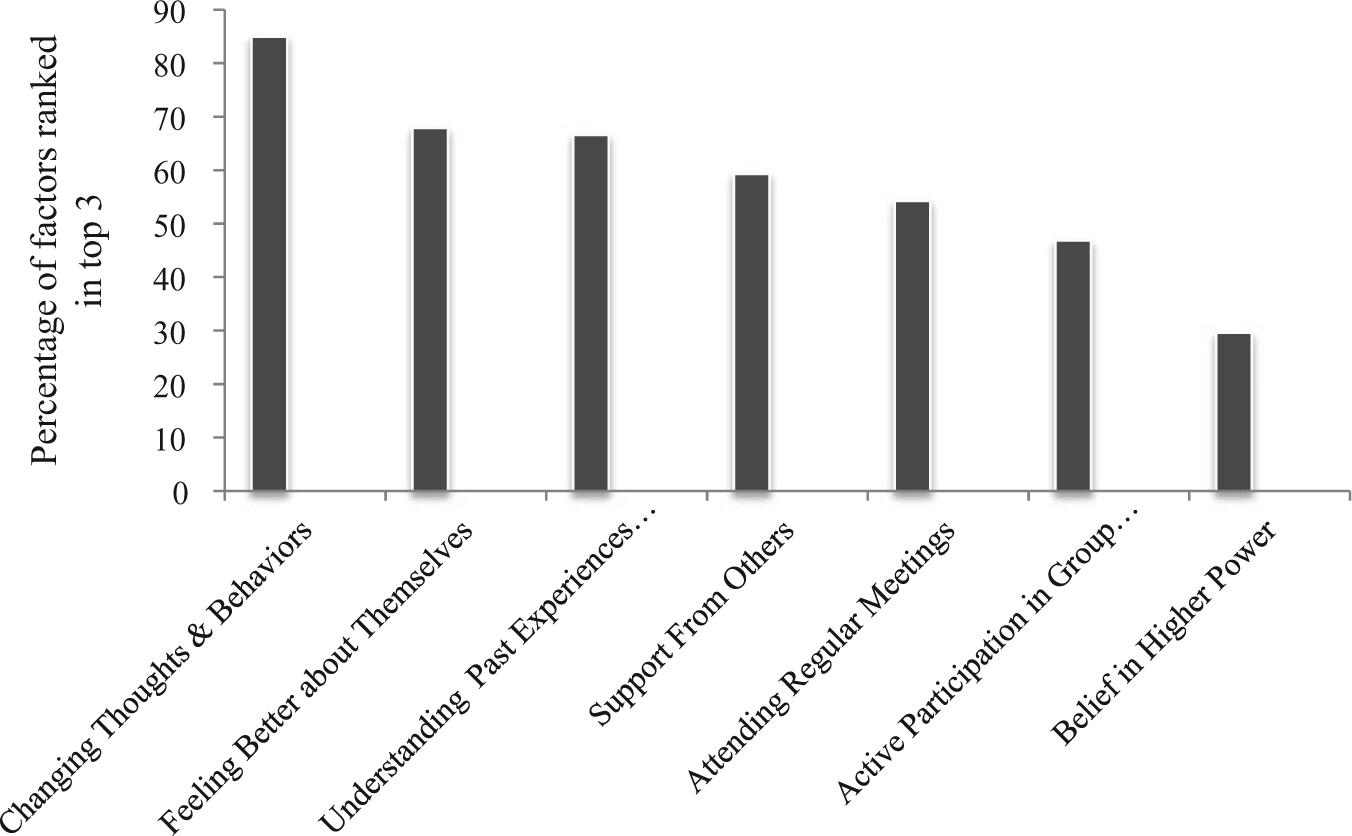
Members’ rank order of recovery goals.
Reasons You Started Attending SMART Recovery Meetings
SMART Recovery members were asked if they had attended another type of recovery group program. Out of the 81 total participants, 64 reported that they had attended another type of recovery meeting and provided reasons for switching to SMART Recovery. Four overarching categories emerged from analyzing the participants’ responses.
Alignment with SMART Recovery program’s philosophy, principles, and format.
Difficulties with surrendering to religious affiliations, such as a higher power, and the adoption of a powerlessness identity.
Still attending both 12-step meetings and SMART Recovery meetings.
Outlier responses.
Alignment with SMART Recovery program’s philosophy, principles, and format
Thirty-three participants (51.6%) stated the benefit of connecting with SMART Recovery philosophy, principles, and format as compared with 12-step models. The cognitive-behavioral approach used in SMART Recovery is a foundational appeal for some SMART Recovery members. This essence was captured in one participant who stated, “I’ve had good results with [cognitive-behavioral therapy]. I sometimes see the rituals of 12-step programs as obstacles.” In addition, some participants reported being attracted to the SMART Recovery program’s format of having trained facilitators leading discussion. A participant reported, What attracted me to SMART were the trained facilitators and the conversation—I feel much more support using reason—makes a lot more sense to me then [sic] 12-steps which you have to rely on an addict to help you through.
Difficulties with surrendering to religious affiliations, such as a higher power, and the adoption of a powerlessness identity
Seventeen participants (26.6%) reported switching as a result of viewing the low utility for a higher power and an aversion to adopt a powerlessness identity. One participant reported, I am not a 12-stepper and I don’t believe that a belief in a “higher power” has any utility for me. If there is a God, it does not intervene in human affairs. Admitting that you are powerless against addiction, and need divine intervention to overcome that addiction is not a constructive mind-set.
Participants also reported not connecting with 12-step programs due to their lack of religious affiliation and, consequently, switching to the SMART Recovery program. One participant stated, “I’m not religious.” Another participant reported, “Don’t agree with giving up to a higher power. Like the idea I have the choice of what to do when the urge comes . . .”
Still attending both 12-step meetings and SMART Recovery meetings
Twelve participants (18.8%) provided responses regarding their reasons for membership in both SMART Recovery and traditional 12-step communities. One participant reported that he or she is “currently doing both. With a ‘home group’ for SMART Recovery and a separate one for [Alcoholics Anonymous].” Another participant reported, “I haven’t switched. I find different perspectives valuable.”
Outlier responses
Researchers discovered two participants’ (3.1%) statements that did not clearly fit into any category. All three researchers could not unanimously agree on the meanings of these statements and, therefore, decided to develop a separate category for these responses to give space for these responses and avoid making unfounded inferences about their meanings by placing them in one of the other three categories. The first statement is “I like the variety.” It was unknown to researchers if the enjoyment of variety was due to wanting to try another program, the variety of people who attend SMART Recovery, or because of the philosophy of the SMART program. Because this statement could be interpreted in several different ways, this statement was not included with the previously mentioned three categories. The second response included in this outlier category is “My dedication to sobriety.” Like the previous statement in this category, this too could be interpreted in different capacities. This response, therefore, was also separated from the other categories that readily emerged.
Sample 2 Results
SMART Recovery facilitators ranked the importance (1 = highest importance, 11 = lowest importance) of the program’s goals intended to help members with recovery. These program goals include abstinence, identifying and correcting irrational thoughts and behaviors, learning how to cope with urges, reduced use of addiction, increase in self-awareness, increase in motivation, establishing balance in life, identification of relapse triggers, understanding the purpose of one’s life, decrease in stigma, and incorporating spirituality into one’s life. Facilitators’ top three ranked responses were calculated (see Figure 2).

Facilitators’ rank order of recovery goals.
Reasons for Becoming a Facilitator
Four overarching categories emerged from analyzing the participants’ (n = 38) responses regarding reasons for becoming a SMART Recovery facilitator. These four categories include
To give back by helping others
Personal benefit for their own recovery.
Accidental Facilitator.
To provide an alternative recovery group.
To give back by helping others
Sixteen participants (42.1%) reported becoming a SMART Recovery facilitator was a means of giving back the SMART Recovery program because it helped with their personal recovery. One participant reported he or she became a facilitator to “give back for all the help the program gave me.” Another participant echoed this response by stating, “SMART helped me in many ways and I wanted to pay it forward.”
Personal benefit for their own recovery
Eight participants (21.1%) reported their reason for becoming a facilitator was to benefit their own recovery process. One participant reported that being a SMART Recovery facilitator “enhances my commitment to recovery . . .” Another participant reported it “helps keep myself on track, to participate in the community, and share my experiences and insights with others while hearing others.”
Accidental facilitator
Eight SMART Recovery facilitators (21.1%) found themselves becoming a facilitator due to chance or being asked to facilitate a meeting. One participant reported, “Back then, the facilitator’s wife got pregnant . . . So I stepped in on an emergency basis. We alternated after he returned. Then he started two new meetings. I took over our meeting . . .” Another participant reported, “I was asked by another facilitator to do it,” while another participant paralleled this statement by stating he or she “ . . . was asked to be a facilitator.”
To provide an alternative recovery group
Six participants (15.8%) reported they became a SMART Recovery facilitator to help provide an alternative recovery group. One participant reported he or she became a facilitator “To help make alternative recovery available to others like me who only had 12-step in my area.” Another participant reported becoming a SMART Recovery facilitator was a means “to provide an alternative option to others who did not think 12-step was the answer.”
What Prepared You to Be a Facilitator?
Three overarching categories emerged from analyzing the participants’ (n = 35) responses to what prepared them to be a SMART Recovery facilitator. These three categories included
SMART Recovery training materials and resources.
Additional resources outside of SMART Recovery materials.
Formal training and education.
SMART Recovery training materials and resources
Twenty-one participants (60%) reported utilizing the SMART Recovery training materials and its resources as a means to be prepared as a facilitator. One participant reported using “the SMART Handbook, the SMART website, and the SMART booklist” as a guide for becoming a facilitator. Another participant stated becoming a facilitator by the “Facilitator training and continuous training via the SMART recovery website . . .”
Additional resources outside of SMART Recovery materials
Nine participants (25.7%) reported either looking for outside readings, mentors, or referencing their own life experience as resources to help prepare themselves as facilitators. One participant reported using “Outside reading, the three or four 12-step meetings I attended over the years, suggestions and observations from meeting attendees.” Another reported, “Experience with my own recovery,” was a way to develop as a facilitator.
Formal training and education
Five participants (14.3%) reported referencing their own formal training and education to help prepare them as a facilitator. One participant reported his or her “undergrad studies in psychology, sociology, philosophy, and humanities as well as graduate religious studies and graduate counselor education degree program,” as instrumental in preparation. Another facilitator reported using his or her “experience as a physician for 30 years in the emergency department, including many persons with addiction problems . . .” as a means to prepare for meeting facilitation.
Discussion
Both samples were mostly male, White, and well educated. These membership demographics align with 12-step meeting membership demographics (AA, 2012). This article provides the first known report of SMART Recovery facilitator demographics. On average, members attended meetings weekly, and approximately one third reported attending both SMART Recovery and traditional 12-step meetings. The high percentage of people reporting a disability highlights the importance for rehabilitation counselors to be aware of the increased preponderance of substance use disorders for people with disabilities. The results of this study are aligned with other reports indicating that people with disabilities are at increased risk for substance use disorders (NAADD, 2013).
The majority of facilitators reported being in recovery from addiction themselves. One study investigating the working alliance among clients and substance abuse counselors noted that clients perceive a stronger working alliance if their counselor is also in recovery (Meier, Donmall, Barrowclough, McElduff, & Heller, 2005). It is not known if SMART members shared this view of the working alliance. It is also not known if SMART members value the formal education of their facilitators, but responses from members indicate that the format and facilitator training were valued by at least some of the members surveyed; both are areas for further research.
Facilitators’ responses reflect their motivations for involvement as being important in their own recovery, as a way to give back to others, and as a way to provide alternative support for those who desire it. Giving back to others and facilitation as a means to support their own recovery process is aligned with sponsor comments in 12-step traditions (AA, 2012). The third theme of providing alternative support reflects a desire among many facilitators to fill a perceived gap in the recovery community for those who desire a different model from the traditional 12-step model.
Members ranked their recovery goals and were given the opportunity to provide narrative responses as well. More than 80% of members ranked changing thoughts and behaviors as critically important to recovery, followed by feeling better about self, and connecting past events to current life situations. The members in this sample reflected an understanding of recovery as a cognitive-emotional process for which people have agency to administer change in their lives. Changing thoughts and behaviors as a top priority for recovery aligns with cognitive-behavioral theory (CBT; Beck, 1993) and rational emotive behavioral theory (REBT; Ellis, 1957). Given that the SMART Recovery philosophy is partly based on CBT and REBT, it is not surprising that so many members ranked this as being important for recovery. The other two top priorities are also aligned with counseling theory. Specifically, the notion that feelings about oneself reflect behavioral motivations and coping strategies, is a core counseling tenet (Corey, 2009). Negative self-feelings contribute to reduced efficacy, which can impact behavioral change related to addiction (Bandura, 2004). Connecting past events to present circumstances is also central to many counseling theories, including psychodynamic theory, Adlerian theory, and Erikson’s psychosocial developmental theory, all of which promote the exploration of past events and interpretation of how these events translate to current motivations (Corey, 2009). Rehabilitation counselors working with clients who attend SMART Recovery meetings can explore their clients’ recovery goals and provide augmented support for these goals using one or more appropriate theoretical frameworks. This approach of aligned messages from multiple treatment sources may be preferable not only to clients but also to counselors who are trained to use appropriate theoretical tenets in their work with clients.
No free reply responses from members indicated adjustment to disability as important for successful recovery. Surprisingly, support from others was ranked fourth highest among members. Social support has been found to be a very good predictor of long-term recovery rates, and many researchers believe a necessary ingredient for recovery (Beattie, 2001; Bond et al., 2003; Moos, 2007). Given the importance of this factor, it may benefit members to increase their awareness of this factor as being important for recovery. It may also be that individuals entering recovery have lost or abandoned previous social groups due to triggers and use. Therefore, increasing early education and experiences around building new social networks is advisable.
Belief in a higher power was ranked as the least important recovery goal by members. This finding is congruent with prior research findings indicating far fewer SMART members identified as being spiritual compared with AA members (Li et al., 2000). The rank ordering of recovery goals is aligned with the members’ response themes and quotes, which reflected a preference for cognitive approaches over spiritual ones, and a preference for the structure and format of SMART meetings. It is important to note that approximately one third of members in our sample reported attending both traditional 12-step meetings as well as SMART Recovery meetings and that this particular group may be more open to multiple ways to find support and strategies for their recovery.
When asked about their overall confidence in SMART Recovery, members reported a mean rating of 8.16 (out of 10), indicating high levels of confidence in the program. This is congruent with qualitative statements provided by members as well as the rank ordering of recovery goals, which align with SMART Recovery philosophy. Taken together, these data imply that members from this sample not only indicated general confidence in the program but also could articulate their reasons for this confidence. Participants further reflected a prioritizing of personal recovery goals that are consistent with the program’s goals, as well as counseling theories and rehabilitation principles of autonomy, independent living, and personal agency. Most members reported a past or current active participation in individual counseling in addition to peer support group meetings. This involvement in individual counseling may account for members’ reasons for rank ordering recovery goals as they did.
The top ranked recovery goal among facilitators was abstinence, which reflected the more traditional 12-step model of absolute sobriety. Abstinence as a goal is supported by literature on recovery (F. Brooks & McHenry, 2009) but does not take into account the specific challenges to recovery for those learning symptom management through use of prescription medications. Rehabilitation counselors may need to discuss the importance of taking medications as prescribed, and the abuse potential for certain prescribed drugs, as they work with their clients who are dealing with this particular challenge. The mixed messages from physicians, rehabilitation providers, and recovery support persons could lead to confusion, low efficacy to implement changes, and feelings of frustration. Rehabilitation counselors can help their clients prevent or cope with this experience by continuing to discuss these challenges while reinforcing the importance of adhering to the rehabilitation plan as outlined by the rehabilitation team. Rehabilitation counselors can also discuss ways that clients can introduce this challenge in support meetings with the goal of increasing awareness and enhancing understanding in the group.
Over half of facilitators ranked correction of irrational beliefs and subsequent behaviors (second highest priority) as being critically important for recovery. This recovery goal aligns with the SMART Recovery philosophy based on REBT, and is congruent with members’ ranking of changing thoughts and behaviors as a top recovery goal. Facilitators ranked incorporation of spirituality as being least important for recovery. This is not surprising given the SMART Recovery training materials and overall REBT- and CBT-based philosophy. This rank ordering aligns with many qualitative responses from facilitators regarding their motivations to provide an alternative support group and aligns with member rank ordering of higher power as the least important factor for recovery.
Facilitators’ rankings of recovery goals indicated the second and third top goals are aligned with counseling principles and SMART Recovery principles, and that the fourth highest (reduced use) reflected a sensitivity to reduction of use as being a corrective step for some, or a necessary behavioral modification for others who may not be able to completely abstain due to medical circumstances (i.e., prescription medications). No facilitator indicated that adjustment to disability was important for recovery, and very few indicated that stigma reduction was important. This was somewhat surprising as most facilitators identified being in recovery from a diagnosable psychiatric disability (substance dependence), yet did not indicate that adjustment to living with this disability and the accompanying stigma as being of primary importance for successful recovery. Given that stigma has been found to be a significant barrier to treatment for people seeking services, employment, and housing for people with substance dependence and other stigmatized disabilities (Corrigan, 2006), increased awareness of how stigma manifests for people in recovery, and how it is a double burden for people with disabilities in recovery, could benefit discussions and complement existing CBT/REBT interventions.
Implications for Rehabilitation Counseling
Rehabilitation counselors can use this information to discuss important elements of peer support groups when exploring options with their clients who are seeking this form of support. The results support other research findings, which indicate the high comorbidity rate for people living with a disability and substance dependence. Our sample reported a range of disabilities, and confirmed previous findings of the high comorbidity rates for people with psychiatric disabilities and substance dependence. Surprisingly, no one in our sample reported spinal cord injury or TBI. As a result, rehabilitation counselors may need to screen for substance abuse more systematically and make referrals for treatment and support groups as needed for people with these disabilities. Our study did not investigate the accessibility of meeting spaces. Low accessibility may have prevented people with spinal cord injury and TBI in wheelchairs from attending meetings.
An explanation that others in attendance at meetings are likely to have a disability may be reassuring to many clients, and this may lead to improved attendance rates. Rehabilitation counselors can discuss the recovery goals that are prioritized in the different recovery communities, including SMART Recovery. Discussion of the different styles of meetings, the focus of meetings, availability of meeting times, and the format of peer support meetings with their clients is one way rehabilitation counselors can work to find the best fit. As social support has been shown to be critical for long-term recovery rates (Beattie, 2001), clients who feel supported by peers with shared goals and similar perspectives are likely to attend meetings regularly and thus benefit from support as a result. It is important for rehabilitation counselors to be aware of their clients’ current support systems, including peer support and additional counseling both in the past and present. One important consideration may be to process discrepancies experienced by the client as he or she seeks support from multiple sources.
Our sample reflected mostly White, employed, and educated men. White men are particularly likely to be diagnosed with substance dependence (NIDA, 2011). This discrepancy exists in many treatment settings, so that female clients and clients of other ethnicities may feel excluded. Helping clients process these feelings of exclusion with the aim of relating in other ways, or expressing this in meetings, may be an important counseling goal for some. Persons with disabilities are less likely to benefit from the highest levels of education, compared with nondisabled people, and are less likely to be employed (U.S. Department of Labor Bureau of Labor Statistics, 2013). Helping clients relate to their peers despite potential discrepancies in education and employment may also benefit clients. Essentially, helping clients focus on shared values and experiences versus differences may result in increased feelings of equity and competence within the group setting.
Overall, the members’ recovery goals align with rehabilitation counseling principles, as well as the principles and recovery philosophy published by SMART Recovery (SMART, 2012). This alignment of rehabilitation principles with SMART Recovery members’ goals may be useful for clients adjusting to disability and seeking services from peer support groups and a VR counselor. VR counselors should be aware of the different philosophies and recovery goals common to peer support groups so they can process discrepancies that may arise, and provide continuity of treatment goals when possible.
Much of the research on peer support groups focuses on 12-step models. Very little research has been conducted on alternative models. It is important to find applicable treatment options for clients who do not adhere to the 12-step principles, or for whom total abstinence from all substances as a required tenet of membership is not feasible. The results of this article provide initial evidence for the demographic characteristics and prioritization of recovery goals among SMART Recovery community members and facilitators. Empirical evidence supports the cognitive approach that this program subscribes to (Butler, Chapman, Forman, & Beck, 2006), but little is known about the efficacy of the program as a whole. It would be helpful for the counseling profession to identify the types of clients who may benefit from SMART Recovery community.
As adjustment to disability is not a focus of SMART Recovery, rehabilitation counselors should be prepared to discuss the health and disability complications that can result from abusing alcohol and drugs, including bladder management, worsening of TBI symptoms, increased likelihood for depression, potential to further injure while intoxicated, contraindications with other medications, and greater risk for unemployment/underemployment (Compton, Thomas, Stinson, & Grant, 2007; Falvo, 2013). The psychological challenges of adjusting to a disability and working toward recovery from addiction, taking medications for symptoms, and managing the dual stigma of disability and substance dependence is worthy of ongoing exploration with clients in the counseling context. In addition, rehabilitation counselors who are knowledgeable about the different recovery communities will be better able to discuss the options with their clients as they collaborate and design treatment plans.
Limitations and Future Directions
Both samples were small and nonrandomly selected, and therefore cannot be generalized to the entire SMART Recovery community. Only descriptive data were provided in the current study, and as such, no conclusions can be made about the efficacy of the program or recovery rates for the current sample. The purpose of the current study was to identify future research aims and describe the characteristics of the SMART Recovery community so as to provide information to rehabilitation counselors for treatment planning purposes. Future studies should aim to investigate the recovery rates for people in this community. Comparative studies investigating the efficacy rates for a range of recovery communities and peer support groups would be useful when discussing available options with clients. The scope and purpose of this investigation did not permit comparison of 12-step member characteristics. As much of the existing literature on peer support groups focuses on 12-step models, rehabilitation counselors are advised to read the existing literature for comparison purposes when helping clients choose a recovery community. Future studies should aim to confirm the accessibility of meeting spaces given the percentage of people with disabilities in the current sample and previous research findings on substance abuse rates for people with spinal cord injury.
Given the 60% relapse rate among the general population (NIDA, 2013), future studies should aim to confirm the relapse rates among people with disabilities who participate in peer support groups, such as SMART Recovery. If, or when a participant does relapse, a structured support system may provide a softer landing and thus reduce the amount of time spent in a state of relapse. Relapse with healthy support is preferable to relapse without support. The format of the SMART Recovery groups may enhance attendance and accountability due to smaller group sizes led by trained facilitators. Participants and facilitators may be more inclined to have expectations for attendance in this type of format, compared with 12-step meetings where group sizes vary, and lack of facilitation and structure may prevent accountability for regular attendance. Follow up studies should include investigation of this hypothesis.
Conclusion
Peer support groups are an important aspect of treatment for individuals recovering from substance use disorders. It is essential for rehabilitation counselors who work with clients at risk for these disorders to have knowledge of the variety of continuing care options that are available. Due to the high prevalence of substance use disorders in the disability community, it is particularly vital that VR counselors have a working knowledge of treatment options that suit their clients’ individual needs. This study presented information on SMART Recovery community member and facilitator characteristics, motivations, and recovery goals. Further research is still needed to fully examine the functions, accessibility, and effectiveness of these groups. SMART Recovery philosophy aligns with rehabilitation counseling philosophy and is a viable option to consider for clients resistant to more traditional 12-step models.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.