
Abstract
Existing research has indicated an association between resilience and psychosocial adjustment to disability. The purpose of this study was to validate the Brief Resilience Scale (BRS) in a sample of vocational rehabilitation (VR) consumers. Participants were 277 individuals with disabilities receiving state VR services. Findings support the identification of two factors in the BRS, labeled succumbing and resilience by the researchers. The succumbing factor was positively associated with reporting of depression while the resilience factor was associated with well-being. Implications for practice in state VR agencies are provided.
Rehabilitation counseling incorporates many aspects of positive psychology, including the focus on human strengths, health, and subjective well-being, in its professional practice knowledge base (Chou, Chan, Phillips, & Chan, 2013; Seligman & Csikszentmihalyi, 2000). Resilience, a major construct in positive psychology, has received increased attention in rehabilitation counseling research as empirical support for the association between resilience and psychosocial adjustment, especially for individuals with traumatic disabilities, has been demonstrated (Catalano, Chan, Wilson, Chiu, & Muller, 2011; Chou, Lee, Catalano, Ditchman, & Wilson, 2009; Fujikawa et al., 2013).
Resilience is considered an individual’s ability to “bounce back” from adversity (Dyer & McGuinness, 1996). According to Yates, Egeland, and Sroufe (2003), resilience can be inferred when there are two major judgments involved: (a) exposure to significant adversity (e.g., a traumatic disability) and (b) a positive developmental outcome occurs. An outcome is considered positive when there is a level of psychosocial adjustment that is better than expected given exposure to extreme circumstances (Luthar, Cicchetti, & Becker, 2000).
The Brief Resilience Scale (BRS) was developed to provide a brief measure of resilience (Smith et al., 2008). In previous research examining the psychometric characteristics of the BRS with undergraduate students and cardiac patients, the measure was found to be reliable and reported resilience as a unitary construct (Smith et al., 2008). In addition, resilience was positively related to other positive psychology constructs such as optimism, social relations, coping, and health, and negatively related to anxiety, depression, perceived stress, negative affect, and physical symptoms (Smith et al., 2008). The purpose of the current study was to investigate the psychometric qualities of the BRS in a sample of vocational rehabilitation (VR) consumers.
Method
Participants
Participants in this study included 277 VR consumers recruited from Alaska, Kentucky, Florida, Michigan, New Mexico, Texas, Utah, and Wisconsin. Average age of the participants was 37.72 years (SD = 12.80). Forty-three percent of the participants were White, 10% Black, 41% Hispanic, 4% American Indian or Alaska Native, and 1% Asian; 61% were women; 24% were married or cohabitating; and 40% had at least some postsecondary education. Forty-three percent of participants had physical and sensory disabilities, 35% had mental health disabilities, and 22% had developmental disabilities. One hundred participants were randomly selected for exploratory factor analysis (EFA), and 177 participants were used for confirmatory factor analysis (CFA).
Measures
The BRS was developed by Smith et al. (2008) to assess resilience as the ability to bounce back from adverse events. It is composed of three positive valence items (Items 1, 3, and 5) and three negative valence items (Items 2, 4, and 6) rated on a 5-point Likert-type scale ranging from 1 (strongly disagree) to 5 (strongly agree). Negative valence items are reverse scored; the six items are summed so that high total scores indicate higher levels of resilience. Internal consistency reliability coefficients (Cronbach’s alpha) of the BRS were reported to range from .80 to .91. Test–retest reliability of the scale was reported to range from .61 to .69 (Smith et al., 2008).
The Patient Health Questionnaire–9 Items (PHQ-9) asks individuals to rate how often depressive symptoms had bothered them during the previous 2 weeks using a 4-point Likert-type intensity scale. Cronbach’s alpha for the PHQ-9 was reported to range between .86 and .89 (Kroenke, Spitzer, & Williams, 2001), and .91 for the current study.
The Satisfaction With Life Scale (SWLS) is a five-item measure constructed by Diener, Emmons, Larsen, and Griffin (1985) to assess life satisfaction using a 7-point Likert-type agreement scale. Cronbach’s alpha for the SWLS was reported to range between .61 and .81 (Diener et al., 1985), and .79 for the current study.
Procedure
Recruitment flyers were posted in the field offices of state VR agencies in eight states and distributed to rehabilitation counselors working in those offices. After reviewing the flyer and consent form, participants met with a researcher at the state VR office to complete the survey.
Data Analysis
Both EFA and CFA were used to evaluate the measurement structure of the BRS. In addition, Pearson product–moment correlation coefficients were computed to provide evidence of construct validity for the BRS based on its relationship with resilience-related constructs.
Results
The BRS was subjected to a principal components analysis (PCA) with oblique rotation. The Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy was .79 (>.50), and the Bartlett’s test of sphericity was significant, χ2(15, N = 100) = 257.54, p < .001, indicating suitability for factor analysis. Contrary to findings reported by Smith et al. (2008), both the Kaiser–Guttman “eigenvalues greater than one” criterion and Cattell’s scree test (Cattell, 1966; Nunnally & Bernstein, 1994) indicated a two-factor solution, accounting for 75% of the total variance. Component 1 is composed of the three negative valence items (labeled succumbing), and Component 2 is composed of the three positive valence items (labeled resilience). All items loaded significantly onto their respective factors (loadings ranging from .83 to .92). The correlation between resilience and succumbing was moderate (r = −.49, p < .001). Table 1 presents the means and standard deviations for each of the items on the BRS, as well as factor loadings, eigenvalues, and percentage of variance explained.
Means and Standard Deviations for Each of the Items on the BRS Scale, Factor Loadings, Eigenvalues, and Percentage of Variance Explained by Each Factor (N = 100).
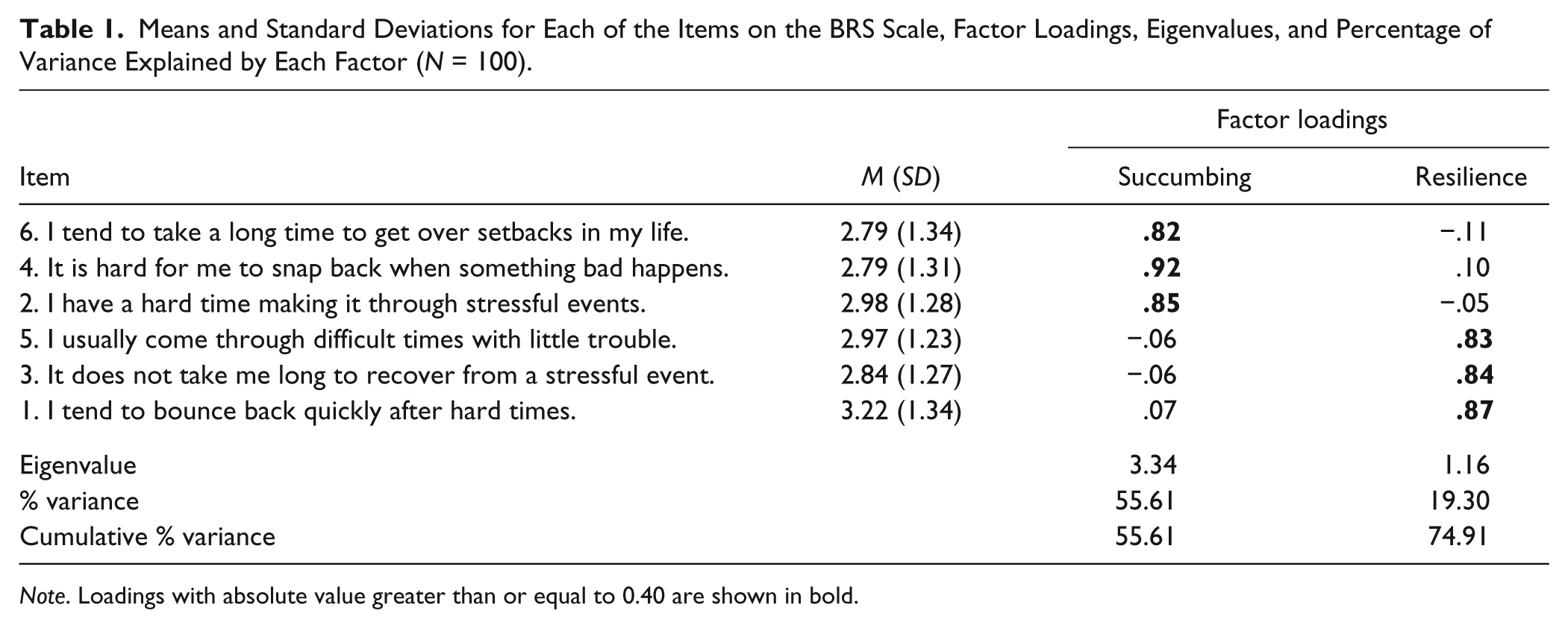
Note. Loadings with absolute value greater than or equal to 0.40 are shown in bold.
The two-factor measurement structure was cross-validated using CFA (Byrne, 2001). Two CFA models were evaluated: (a) the one-factor model (to evaluate the BRS as a unidimensional measure) and (b) the two-factor intercorrelated model (to confirm our EFA result). CFA indicated a poor fit for the one-factor model: χ2(9, N = 177) = 133.57, p < .001; χ2/df = 14.84, comparative fit index (CFI) = .66; and the root mean square error of approximation (RMSEA) = 0.28, 90% confidence interval (CI) [0.23, 0.32]. The chi-square test of model fit for the two-factor intercorrelated model is also significant, χ2(8, N = 177) = 15.58, p < .05; however, χ2/df = 1.95 is less than 3, CFI of .98 is greater than .95, and RMSEA of 0.07 (90% CI [0.00, 0.12]) is below the value of 0.08; all these indexes meet the criteria of good model fit (cf. Weston, Gore, Chan, & Catalano, 2008). In addition, significant chi-square differences (χ2diff = 117.99, dfdiff = 1, p < .01) between the models and reduction in the Bayesian information criterion (BIC) index from 195.68 for the one-factor model to 82.87 for the two-factor model confirmed that the two-factor model explained data better than the one-factor model (Kaplan, 2000). All items in the two-factor model significantly loaded on their respective factors ranging from .66 to .78 for the succumbing factor and from .69 to .87 for the resilience factor.
Mean of the average item scores for the succumbing and resilience factors were 2.76 (SD = 1.07) and 3.08 (SD = 1.03), respectively. Internal consistency reliabilities (Cronbach’s alpha) for the succumbing and resilience components were .83 and .79 respectively. The succumbing factor was positively associated with depression (r = .59, p < .001) and negatively associated with life satisfaction (r = −.42, p < .001), whereas the resilience factor correlated negatively with depression (r = −.33, p < .001) and positively with life satisfaction (r = .26; p < .001). The succumbing factor had a higher correlation with both depression and life satisfaction than the resilience factor.
Discussion
The objectives of this study were to examine the factorial structure of the BRS in a sample of VR consumers and the concurrent validity of the BRS with depression and life satisfaction measures. A two-factor model comprised of a resilience factor and a succumbing factor provided the best fit with the data. The internal consistency reliability of the BRS was within acceptable ranges. Examination of concurrent validity revealed a moderate positive association between negative valence factors and depression; positive valence factors were associated with life satisfaction. Of interest, the succumbing factor had a higher correlation with depression and life satisfaction indicators than with the resilience factor. The higher correlations between the succumbing factor and these external correlates are consistent with the existing literature regarding negative valence detection and response bias in that individuals detect negative valence verbal information with both higher accuracy and sensitivity (Nasrallah, Lavie, & Carmel, 2009). The perceptual sensitivity for negative valence items may be an adaptive characteristic. The preferential processing of potentially threatening information benefits attentiveness activities as they relate to self-preservation (Nasrallah et al., 2009). Alternatively, models of adjustment to chronic illness and disability suggest that persons with disabilities may be prone to negative self-evaluation and display a heightened sensitivity to negative environmental cues (Livneh & Antonak, 2005). Given the sample under consideration in this study, understanding the effect of the experience of disability on perceptual processing is an area requiring further research. Respectively, a limitation of this study is that it did not include analysis of the sample group member’s type of disability, length of disability, or measurement of disability acceptance.
Rehabilitation Implications
Overall, this study demonstrated that the BRS measures two related factors that are appropriate for use by rehabilitation counselors to identify and assess resiliency among individuals receiving VR services. In the VR process, knowledge of client characteristics or factors promoting resilience such as optimism, active coping, and social support may provide counselors valuable insights into the needs of service recipients and suggest strategies to implement more successful rehabilitation plans and interventions. The BRS features questions in plain language, and the time required to administer and score the BRS suggests that it would be a simple, brief, and reliable measure for rehabilitation counselors to incorporate in their assessment and planning efforts. Moreover, BRS administration could be a useful part of the client screening and admission processes of both state VR and community-based rehabilitation agencies by providing a discrete measure of psychosocial functioning and well-being.
Footnotes
Authors’ Note
The ideas, opinions, and conclusions expressed are those of the authors and do not represent recommendations, endorsements, or policies of the U.S. Department of Education.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The contents of this article were developed with support from the Rehabilitation Research and Training Center on Evidence-Based Practice in Vocational Rehabilitation (RRTC-EBP VR) at the University of Wisconsin–Madison and the University of Wisconsin–Stout and with funding provided by the U.S. Department of Education, National Institute on Disability and Rehabilitation Research (Grant H133B100034).