
Abstract
The purpose of this study was to determine whether personal (caregiving mastery and problem-solving coping) and environmental (social support and professional and community support) caregiver resources mediate the relationship between caregiver perceived burden and quality of life (QOL). The sample consisted of 108 caregivers recruited from support groups who were predominantly White women. The majority of care-recipients had a severe head injury. Measures administered were the Interpersonal Support Evaluation List, the COPE, Family Needs Questionnaire, Modified Caregiving Appraisal Scale, and the World Health Organization Quality of Life–Brief Version. Results showed that social, professional, and community supports mediate the link between perceived burden and QOL. Caregivers of persons with traumatic brain injury frequently face elevated levels of burden, stress, and depression. Positive personal and environmental support, particularly social support, professional/community supports, and mastery, could lessen the negative impact of caregiving burden on QOL of the caregiver.
Keywords
Traumatic brain injury (TBI) is a worldwide public health problem that can result in long-lasting disability (Corrigan, Selassie, & Orman, 2010). In the United States, the prevalence of people living with a disability following hospitalization with TBI is estimated to be 3.2 million (Corrigan et al., 2010). The impact of TBI extends beyond the individual to the family (Degeneffe, Chan, Dunlap, Man, & Sung, 2011; Florian, Katz, & Lahav, 1989; Perlesz, Kinsella, & Crowe, 1999). Family members’ roles and functions are often abruptly and substantially altered, with the daily tasks of caregiving becoming prominent. As a result, family caregivers frequently find themselves facing elevated levels of burden, stress, and depression due to the extensive and chronic nature of TBI care (Degeneffe et al., 2011). Many of these negative caregiver outcomes are associated with poor rehabilitation outcomes for the care-recipient (Rivera, Elliott, Berry, Grant, & Oswald, 2007).
Of particular interest are vocational rehabilitation (VR) outcomes for persons with TBI. Studies suggest that persons with TBI have poorer VR outcomes as compared with those with other types of disabilities (Gordon, O’Neill, & Vandergoot, 2003). One longitudinal study of VR services found that nearly 70% of all consumers achieved employment, whereas those with TBI achieved employment at a rate of only 45% (Hayward & Schmidt-Davis, 2002). In addition, persons with TBI access VR less often than those with other types of disabilities (Bergman, 2002) and comprise a small percentage of VR counselor caseloads (Gordon et al., 2003).
Indeed, TBI is a contemporary disability, and aspects of the VR system along with a lack of TBI services and programs are barriers to successful vocational outcomes for people with TBI (Zuger, Brown, O’Neill, Stack, & Amitai, 2002). Working with families of persons with TBI is one way in which these barriers may be reduced and outcomes improved. Specifically, family members are often the primary source of support for persons with TBI and are typically the navigators of health care and other professional and community support services including VR. As such, rehabilitation counselors need to be prepared to work with both the person with TBI and their family—acknowledging that a family member’s experience may be a facilitator or barrier to effective VR intervention (Degeneffe & Lee, 2015).
Rehabilitation scholars have acknowledged for decades that family is a critical variable that influences rehabilitation outcomes (Dew, Phillips, & Reiss, 1989) and that working with families in the rehabilitation process does not require expertise in family therapy, but an understanding that the family is an integral component of the consumer’s world (Dew et al., 1989). As such, practical assessment techniques and psychosocial interventions based on theory driven caregiver research needs to be included in the rehabilitation counseling context to enhance caregiver functioning and rehabilitation outcomes of care-recipients (Ergh, Rapport, Coleman, & Hanks, 2002).
The World Health Organization International Classification of Functioning, Disability and Health (ICF; World Health Organization [WHO], 2001) that conceptualizes disability as an interaction between functioning (body, activity, and participation) and context (personal and environmental) provides a theoretical framework to facilitate caregiving research and practice. Using this model, caregiver outcomes reflect an interaction between the care-recipient’s functioning and the caregiver’s context. Conceptualizing TBI caregiving from this perspective facilitates research and practice that is ecological and holistic, by considering a broader range of contextual factors that interact to influence the caregiving process. Implicit in this framework is a focus on personal and environmental factors that have the potential to facilitate growth and participation in valued activities and optimal functioning, within the limitations imposed by the deficits (Evans, 2011). Given that many of the deficits associated with TBI cannot be altered, research and practice focusing on positive caregiver personal and environmental resources that contribute to positive outcomes is warranted. Moreover, this line of inquiry is grounded in contemporary and ecological models of health and functioning and is supported by studies that show that psychological growth and positive outcomes do occur for caregivers post TBI (C. A. Cohen, Colantonio, & Vernich, 2002; Parveen, Morrison, & Robinson, 2011). Importantly, the rehabilitation counseling profession has had a tradition of emphasizing the person–environment interaction effect (Chan, Tarvydas, Blalock, Strauser, & Atkins, 2009). Therefore, the evaluation of the WHO ICF framework as a QOL model for caregivers of people with TBI is consistent with the philosophy and professional practice of rehabilitation counseling (Chan et al., 2009; Degeneffe & Lee, 2015; Maki, 2012; Patterson, Bruyere, Szymanski, & Jenkins, 2011) and will provide useful information for integrating family assessment and interventions in VR service delivery practices for people with TBI.
Applying the ICF framework to TBI caregiving, we examined care-recipient functional disability (functioning factor), caregiving mastery and problem-solving coping (personal factors), and social and professional supports (environmental factors). More specifically, we sought to determine whether personal (caregiving mastery and problem-solving coping) and environmental (social support and professional and community support needs) caregiver resources mediate the relationship between caregiver burden and QOL. Currently, there are limited studies using the ICF framework to study these positive personal and environmental factors on the QOL of caregivers of persons with TBI (Reinhard, Given, Petlick, & Bemis, 2008).
We chose to investigate care-recipient functional disability (as perceived by the caregiver) because studies find links between care-recipient functioning and caregiver stress (Oddy, Humphrey, & Uttley, 1978), burden (Allen, Linn, Gutierrez, & Willer, 1994; Brooks, Campsie, Symington, Beattie, & McKinlay, 1987), psychological distress (Kreutzer, Serio, & Bergquist, 1994), marital adjustment (Peters, Stambrook, Moore, & Esses, 1990), and family functioning (Douglas & Spellacy, 2000; Kreutzer et al., 1994). Caregiver mastery and problem-solving coping were investigated because these constructs have been shown to be associated with positive caregiver psychosocial outcomes (e.g., Chronister & Chan, 2006; Degeneffe et al., 2011; Hanks, Rapport, & Vangel, 2007; Rivera, Elliott, Berry, & Grant, 2008). Specifically, caregiving mastery—which involves the sense of control caregivers feel they are able to exercise over the caregiving situation (Struchen, Atchison, Roebuck, Caroselli, & Sander, 2002)—has been linked to QOL (Chronister & Chan, 2006), social support, and family functioning (Hanks et al., 2007). Pearlin and colleagues suggest that caregiver mastery is a critical resource that protects against stress and leads to a reduction in stress associated with role overload, role captivity, and loss of intimate exchange (Aneshensel, Pearlin, Mullan, Zarit, & Whitlatch, 1995). Similarly, we investigated problem-solving coping skills that involves using rational, instrumental problem-solving strategies (e.g., information seeking, taking control) aimed at removing or reducing the cause of the stressor (McLeod, 2010).
According to Rivera and colleagues (2008), higher levels of problem-solving coping enable caregivers to regulate their emotions, maintain a positive attitude (for solving problems), and use rational, instrumental problem-solving strategies, leading to lower levels of caregiver distress. Finally, we chose to examine social and professional supports because of their centrality to the ICF environmental construct (Ergh et al., 2002) and the well documented research literature that shows that social and professional supports alleviate caregiver distress (Ergh, Hanks, Rapport, & Coleman, 2003; Reinhard et al., 2008).
We chose QOL as our outcome measure because prior caregiving research has focused primarily on determining the absence of negative effects versus the presence of a positive outcome (Beach, Schulz, Yee, & Jackson, 2000). Rapp and Chao (2000) suggest that the positive effects of caregiving are conceptually and empirically distinct from the negative effects and should, therefore, be examined separately. Moreover, studies suggest that even with high levels of burden and distress, caregiver life satisfaction can be high (Wells, Dywan, & Dumas, 2005). Indeed, this is an important investigation given that studies suggest that for some caregivers, TBI leads to positive psychological growth and personal satisfaction (C. A. Cohen et al., 2002; Parveen et al., 2011).
Study Aims
This study has two specific aims as follows: (a) to determine if functional disability of the care-receiver with TBI affects the QOL of the caregiver through its effect on perceived burden of providing care and (b) to examine to what extent positive person–environment variables mediate the association between perceived burden and QOL. We proposed the following hypotheses:
Method
Design
In this study, a quantitative descriptive design using hierarchical regression analysis was used to test our mediational hypotheses.
Participants
The sample consisted of 108 caregivers who were predominantly White (83%) and female (74%), with at least some college education. Fifty-two percent were parents and 34% were spouses. The average number of years of caregiving was 8.62, and the majority of care-recipients were described to have a severe head injury (77%) as measured by caregiver self-report of length of loss of consciousness. Demographic information is shown in Table 1.
Descriptive Statistics for Caregivers.

Note. LOC = loss of consciousness; MVA = moving vehicle accident.
Variables
Functional disability
Functional disability was measured by the Patient Competency Rating Scale–Relative Version (PCRS-RV). The PCRS was developed by Prigatano et al. (1986) to assess the functional competency of the care-recipient in activities of daily living, cognitive and interpersonal functioning, and emotional regulation as perceived by the caregiver. The PCRS-RV is comprised of 30 items (e.g., “How much of a problem do they have in preparing their own meals?” “How much of a problem do they have in taking care of their finance?”). Each item is rated on a 5-point Likert-type performance rating scale, ranging from 1 (cannot do) to 7 (can do with ease). In this study, the instrument was used as a measure of functional disability, and the items were reverse-scored with higher scores indicating greater functional disability as perceived by the caregiver. The PCRS-RV was found to be associated with the Glasgow Coma Scale (Sandhaug, Andelic, Berntsen, Seiler, & Mygland, 2012). Test–retest reliability of the PCRS-RV over a 2-week period has been reported to be .92 (Prigatano, Altman, & O’brien, 1990), and an internal consistency estimate of .93 has also been reported (Ergh et al., 2002; Fleming, Strong, & Ashton, 1998). The coefficient alpha for this study was .95.
Perceived burden and caregiving mastery
Perceived burden and caregiving mastery was measured by the Modified Caregiving Appraisal Scale (MCAS). The MCAS was developed by Struchen et al. (2002) to assess a caregiver’s subjective evaluation of his or her present caregiving experience. The complete MCAS is comprised of 41 items and includes four scales: (a) Perceived Caregiving Burden, (b) Perceived Caregiving Mastery, (c) Perceived Caregiving Satisfaction, and (d) Perceived Caregiving Ideology. For our study, we used the first two scales listed above: Perceived Burden and Perceived Mastery. For Perceived Burden, there were 15 items (e.g., “Caring for this individual doesn’t allow me as much privacy as I would like”), and for Perceived Mastery, there were 10 items (e.g., “I feel confident in my ability to care for this individual’s needs”). Each item is rated on a 5-point Likert-type rating scale ranging from 1 (strongly disagree) to 5 (strongly agree). Total scores for each scale are found by summing the raw scores, with higher scores indicating lower burden, more satisfaction, and a higher sense of mastery. Validity evidence is demonstrated by significant correlations between (a) the Perceived Burden subscale and objective burden measures, subjective burden measures, and negative affect measures, and (b) the lack of a relationship of mastery to burden and psychological health measures (Struchen et al., 2002). Internal consistency reliability estimates (Cronbach’s α) for the three scales have ranged from .52 to .91 (Lawton, Kleban, Moss, Rovine, & Glicksman, 1989; Struchen et al., 2002). Test–retest reliability estimates have ranged from .68 to .78 (Lawton et al., 1989). Cronbach’s alpha coefficients in the present study were .89 for perceived burden and .65 for mastery.
Problem-focused coping
Problem-focused coping was measured by the COPE Scale developed by Carver, Scheier, and Weintraub (1989). The COPE assesses the cognitive and behavioral strategies used to cope and is comprised of 60 items including 15 scales with 4 items per scale. For this study, the following two subscales were used to measure problem-focused coping: Active Coping (e.g., “I concentrate my efforts on doing something about it”) and Planning (e.g., “I make a plan of action”), with items extracted from the situational version (e.g., statement tense worded as “I’ve been”) of the COPE. Each item is rated on a 4-point Likert-type scale ranging from 1 (I haven’t been doing this at all) to 4 (I’ve been doing this a lot). Total scores for each scale are found by summing the raw scores, with higher scores indicating more problem-solving coping. Validity evidence is demonstrated by associations between coping and related personality qualities (Carver et al., 1989), and although the COPE has been shown to have a somewhat strong relationship with personality variables, evidence suggests a weak association with social desirability. Internal consistency reliability estimates for the subscales have ranged from .62 to .92 (Carver et al., 1989; Wade et al., 2001). Test–retest reliability of the COPE over a 6- to 8-week period has been reported to range from .48 to .89 (Carver et al., 1989). The Cronbach’s alpha for this study was .77 for problem-solving coping.
Social support
Social support was measured by the Interpersonal Support Evaluation List (ISEL). The ISEL was developed by S. Cohen, Mermelstein, Kamarck, and Hoberman (1983) to measure one’s perceived availability of social support. The ISEL is comprised of 40 items including four scales, with 10 items per scale, counterbalanced for social desirability with half of the items written as positive statements and the other half as negative statements: (a) belonging or companionship support (e.g., “I often meet or talk with family or friends,” “No one I know would throw a birthday party for me”), (b) emotional support (e.g., “There is someone I could turn to for advice about making career plans or changing my job,” “If a family crisis arose, it would be difficult to find someone who could give me good advice about how to handle it”), (c) self-esteem maintenance by social comparison statements (e.g., “ There is someone who takes pride in my accomplishments,” “Most of my friends are more successful at making changes in their lives than I am”), and (d) instrumental or tangible support (e.g., “If I need an emergency loan of US$100, there is someone I could get it from,” “If I were sick and needed someone to take me to the doctor, I would have trouble finding someone”). In this study, the subscales for belonging or companionship support, emotional support, and instrumental or tangible support were used as a measure of perceived social support. Each item is rated on a 4-point Likert-type scale ranging from 1 (definitely true) to 4 (probably false). A total score was found by summing the raw scores, with higher scores indicating higher levels of social support. Validity evidence is demonstrated by a positive link between the ISEL and other measures of social support (.30–.62), self-esteem (.58–.74), and self-disclosure (.40); a negative correlation with psychological symptomatology; no association to social desirability; and the ability to predict depression above and beyond social anxiety (S. Cohen et al., 1983). Internal consistency reliability estimates have ranged from .77 to .91 (Brisette, Scheier, & Carver, 2002; S. Cohen & Hoberman, 1983; S. Cohen et al., 1983). Test–retest reliability estimates for the ISEL over a 2-week period have been reported to be .87 (S. Cohen et al., 1983). The Cronbach’s alpha for this study was .96.
Professional and community support needs
Professional and community support needs was measured by the Family Needs Questionnaire (FNQ). The FNQ was developed by Kreutzer et al. (1994) to assess a perceived family needs following a brain injury. The FNQ is comprised of 40 items including six scales: (a) Health Information, (b) Emotional Support, (c) Instrumental Support, (d) Professional Support, (e) Community Support, and (f) Involvement With Care. We grouped the six scales into three scales that included (a) Health Related Needs consisting of the Health Information and Involvement With Care scales, (b) Professional Support Needs consisting of the Professional- and Community-Based Support scales, and (c) Social Needs consisting of the Emotional and Instrumental Needs scales. Scores indicate the percentage of needs that were important/very important and partly met/met. Higher percentages indicate that a higher number of important/very important needs are met or partly met. See Table 2 for mean scores on the three combined subscales. For the aims of this study, we looked only at the Professional and Community Support subscales. This combined scale included 10 items in total, with 5 professional support items (e.g., “To be told how long each of the patient’s problems is expected to last”), and 5 community support items (e.g., “To have a professional to turn to for advice or services when the patient needs help”). Each item is rated on 4-point Likert-type scale ranging from 1 (not important) to 4 (very important) and a 3-point ordinal scale indicating the degree to which these needs are met ranging from 1(yes, met) to 3 (not met). Validity evidence is demonstrated by correspondence of five of the six factors of this scale with the dimensions of social support (Wortman & Conway, 1985). Internal consistency reliability estimates have been reported as .83 for professional support and .81 for community support network (Serio, Kreutzer, & Witol, 1997). Coefficient alpha in the present study was .89 for health related needs, .91 for professional support needs, and .85 for social needs.
Means and Standard Deviation Scores From Family Needs Questionnaire.

QOL
QOL was measured by the World Health Organization Quality of Life–Brief Version (WHOQOL-BREF). The WHOQOL-BREF was developed by the WHOQOL Group (1998) to assess QOL. The WHOQOL-BREF is comprised of 26 items, shortened from the original longer scale (WHOQOL-100) and includes four subscales: (a) Physical Health, 7 items (e.g., “To what extent do you feel that physical pain prevents you from doing what you need to do?”); (b) Psychological Health, 6 items (e.g., “How often do you have negative feelings such as blue mood, despair, anxiety, and depression?”); (c) Social Relationships, 3 items (e.g., “How satisfied are you with the support you get from your friends?”); and (d) the Environment, 8 items (e.g., “How healthy is your physical environment?”). In this study, the entire scale was used as a measure of the subjective evaluation of the caregiver’s physical health, psychological health, social relationships, and the environment over the last 2 weeks. Each item is rated on a 5-point Likert-type rating scale ranging from 1 (not at all) to 5 (extremely). Total scores are found by summing the raw scores for each subscale, with higher scores indicating better QOL. Validity evidence is demonstrated by comparisons to the WHOQOL-100 (excellent ability to discriminate between ill and well respondents). Internal consistency reliability estimates have been reported to range from .66 to .80. Test–retest reliability of the WHOQOL-BREF over a 2- to 8-week period have been reported to range from .56 to .87 (WHOQOL Group, 1998). The Cronbach’s alpha in this study was .94.
Procedure
A total of 153 mail surveys were distributed, and 76% (117) were returned. Of those returned, 6% (7) did not meet the inclusion criteria, and 2% (2) had incomplete data. The final study sample included 108 caregivers. Participants were recruited from traditional community-based support groups (51%) and web-based support groups (49%) for caregivers of individuals with TBI. Participants recruited from web-based support groups were members of four web-based TBI caregiver support groups. Fifty-two (49%) of the participants were from California, and 51% were from 27 other states, including 6 each from Minnesota, Texas, and Massachusetts; 5 from Indiana; 4 each from Florida and North Carolina; 2 each from Arizona, Wisconsin, Washington, Illinois, Louisiana, Michigan, and New York; and 1 each from Oregon, Pennsylvania, Alabama, Colorado, Maryland, Connecticut, New Hampshire, Washington, D.C., New Jersey, Ohio, and Alaska. Caregivers who expressed an interest in participating were instructed to contact the researcher via e-mail or phone, and those agreeing to participate were mailed a research packet. All participants were informed of the voluntary nature of the research, their rights as a research participant, and the potential negative effects from participating in the study. Caregivers had to meet the following criteria to participate: (a) be at least the age of 18, (b) able to read and understand English (by self-report), (c) consider themselves a primary caregiver (although they could share the responsibilities), and (d) not be a paid, formal caregiver/attendant. The following criteria regarding the care-recipient were also required: (a) the care-recipient had to have been injured no earlier than the 18th year of life, (b) the injury had to have occurred 12 months or more prior to survey completion, and (c) the care-recipient could not be currently living in a residential program.
Data Analysis
Correlational methods were employed to analyze the data. Zero-order correlations for all variables were conducted. Data were also analyzed using multiple regression analysis.
Results
Perceived Burden as a Mediator Between Functional Disability and QOL
Numerous analytic strategies have been developed for testing mediator hypotheses (MacKinnon, Lockwood, Hoffman, West, & Sheets, 2002; Shrout & Bolger, 2002), but the simplest strategy involves a straightforward application of multiple regression and correlation techniques proposed by Baron and Kenny (1986). This procedure involves three steps:
Regress the mediator to the independent variable (IV) to show it is plausible that the two variables can be causally linked.
Regress the dependent variable (DV) to the IV to show a causal relation is plausible as well.
Regress the DV simultaneously to the IV and the mediator to show that the mediator is significantly related to the DV, even when the IV is statistically controlled.
If the regression coefficients for Steps 1 and 2 are significant, and the partial regression coefficient for predicting the DV from the mediator is significant in Step 3, a mediator hypothesis is supported (Baron & Kenny, 1986). Correlations and descriptive statistics for the IV, mediator variables, and DV are provided in Table 3.
Means, Standard Deviations, and Correlations of Variables in Full Model.
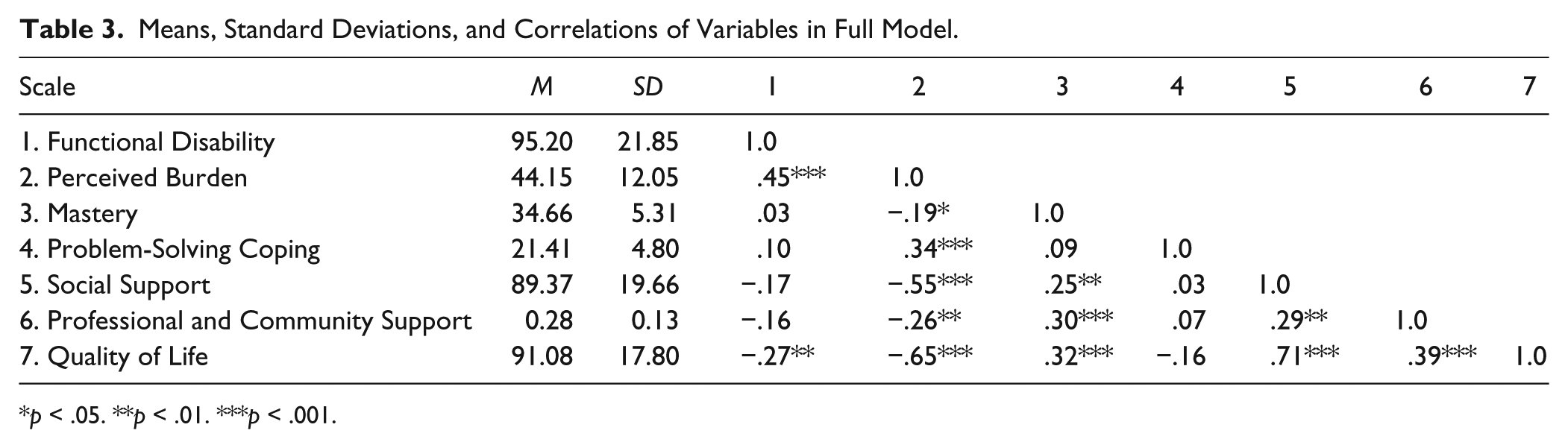
p < .05. **p < .01. ***p < .001.
As expected, the association between functional disability (IV) and QOL (DV; Step 2) was computed to be significant: β (95% confidence interval [CI]) = −.27 [−.45, −.08]. Next, the association between the IV (functional disability) and the mediator (Step 1) was assessed. Functional disability was significantly related to burden β (95% CI) = .45 [.27, .62]. Finally, the mediator (burden) was significantly related to the DV (QOL), β (95% CI) = −.66 [−.82, −.49], while statistically controlling for the IV (Step 3). The model accounted for 60% of the variance in QOL, R = .65, R2 = .42, F(2, 105) = 37.59, p < .001, and is considered a large effect size (J. Cohen, 1988, 1992).
In addition, the association between functional disability and QOL in the final (two-predictor) regression equation was examined. The relationship between functional disability and QOL was no longer significant, β (95% CI) = .02 [−.14, .19] when the mediator (burden) was input into the equation. The β for functional disability was reduced from −.27 to .02 after controlling for the effect of the mediator (burden). To formally test the mediational effect of perceived burden, we computed the bootstrap procedure recommended by Preacher and Hayes (2004). The bootstrapped estimate of the indirect effect, with 3,000 resamples, is similar to the point estimate computed from the conventional regression analysis of the raw data, and the true indirect effect is estimated to lie between −.54 and −.13 with 99% confidence. Because zero is not in the 99% CI, we can conclude that the indirect effect is significantly different from zero, p < .01 (two-tailed).
Positive Person–Environment Factors as Mediators Between Perceived Burden and QOL
Because perceived burden is a modifiable determinant of QOL (vs. functional disability), we conducted a logical follow-up analysis to determine whether specific positive person–environment variables mediate the relationship between perceived burden and caregiver QOL. As expected, the association between perceived burden (IV) and QOL (DV; Step 2) was significant: β (95% CI) = −.65 [−.79, −.50]. Next, the association between the IV (perceived burden) and each of the mediators (Step 1) was assessed. Perceived burden was significantly related to mastery, problem coping, social support, and professional support: βs (95% CIs) = −.19 [−.38, −.01], .34 [.16, .52], −.55 [−.71, −.39], and −.26 [−.45, −.08], respectively. Finally, each of the putative mediators was significantly related to the DV (QOL), while statistically controlling for the IV (Step 3). The relevant analysis was a simultaneous regression of QOL (DV) to perceived burden (IV), mastery, problem coping, social support, and professional support. The mediation model implies that each mediator is uniquely related to QOL (DV), controlling for the other mediators and perceived burden (IV). The model accounted for 64% of the variance in QOL, R = .80, R2 = .64, F(5, 102) = 35.98, p < .001, which is considered a large effect size (J. Cohen, 1988, 1992). Two of the four mediators, social support and professional support needs respectively, were significantly associated with the DV, βs (95% CIs) = .49 [.34, .64] and .15 [.02, .28]. In summary, all three steps were significant as predicted, yielding support for a dual-mediation model. The findings conform to the predictions of a model in which perceived burden is associated with QOL indirectly through its association with social support and professional support needs, each of which is uniquely associated with QOL. In addition, the association between perceived burden and QOL in the final (five-predictor) regression equation was examined. This was also statistically significant, β (95% CI) = −.29 [−.44, −.13]. The β for perceived burden was reduced from −.65 to −.29 after controlling for the effect of the mediators.
The indirect effect for the mediation model was tested using the SPSS INDIRECT macro for conducting bootstrap tests of multiple mediator models downloaded from Kristopher Preacher’s website (http://www.afhayes.com/spss-sas-and-mplus-macros-and-code.html#indirect). For the dual-mediation model, as expected, the unstandardized indirect effects (with 95% CIs derived from bias-corrected and accelerated bootstrap procedures) were products (
Discussion
Consistent with contemporary biopsychosocial approaches to understanding health and disability and the need to integrate family interventions in VR practices for people with TBI, we sought to investigate how functional and contextual variables interact to influence the QOL of those caring for persons with TBI. We were particularly interested in determining the extent to which positive person–environment factors reduce the negative impact of perceived burden on caregiver QOL. Overall, our findings confirmed the role of person–environment variables in facilitating improved QOL among TBI caregivers, supporting the growing body of research that finds appraisals of burden and coping resources and supports to be linked to better caregiver outcomes (Hanks et al., 2007; Hilgeman, Allen, DeCoster, & Burgio, 2007; Rodakowski, Skidmore, Rogers, & Schulz, 2012).
Our first hypothesis sought to determine whether perceived caregiver burden mediates the relationship between care-recipient functional disability and caregiver QOL. Findings revealed that perceived burden significantly mediated the relationship between functional disability and QOL, suggesting that functional disability influences caregiver QOL predominately through caregivers’ appraisal of burden. This finding is consistent with prior research showing that caregiver stress appraisal or perceived burden is a more direct predictor of outcomes than functional status or severity level (Chronister & Chan, 2006; Chwalisz, 1996; Hanks et al., 2007; Rodakowski et al., 2012). Taken together with prior studies, our findings reinforce the importance of addressing caregivers’ distressing cognitive and emotional experiences related to caregiving such as isolation, loss of control, depression, fatigue, role change, and the feeling of being trapped (Arango-Lasprilla et al., 2010; Degeneffe & Lee, 2015; Hanks et al., 2007). Therefore, rehabilitation counselors working with caregivers of people with TBI should carefully assess the perceived burden of these caregivers and be cognizant of how such burden can affect their mental health and well-being. Interventions addressing the emotional response to caregiver burden may improve caregiver mental health, leading to better care for care-recipients with TBI.
Our second hypothesis sought to investigate the mediating properties of positive, person–environment factors (caregiving mastery, problem-solving coping, social support, and professional/community support) on the relationship between perceived burden and QOL. Findings confirmed that social support and professional/community supports partially mediate the relationship between perceived burden and QOL. Our findings are consistent with the large body of literature that suggests social support acts as a buffer against stress (S. Cohen, 2001; S. Cohen, Doyle, Turner, Apler, & Skoner, 2003; S. Cohen & Wills, 1985; Feldman, Cohen, Hamrick, & Lepore, 2004) and the growing body of TBI caregiving literature that suggests social support buffers the negative impact of caregiving stress (Chronister & Chan, 2006; Chronister, Chan, Sasson-Gelman, & Chui, 2010; Chwalisz, 1996; Douglas & Spellacy, 2000; Ergh et al., 2003; Hanks et al., 2007; Harris, Wise, Gallagher, & Goodwin, 2001). Notably, in this study, we measured perceived social support, which refers to the perception of available support if needed in the future; thus, our findings reveal that caregivers’ cognitive and emotional appraisal of potential tangible (e.g., help with transportation, an errand, or house sitting) and emotional support (e.g., having someone to talk to or share experiences with) reduces the negative impact of burden. This clarification is important for intervention; specifically, although a caregiver may appear to have a large network, or family/friends of the caregiver report providing supports, a caregiver’s subjective appraisal of what they believe to be available was found in our study to influence better QOL. In addition, the nature of a caregiver’s social support system may change post TBI, and thus understanding a caregiver’s current perception of what supports are available to them is critical to positively enhancing social support.
Access to and support from professional/community supports are critical to caregiver health and well-being. Unfortunately, there is a lack of comprehensive and integrated post-acute support services for individuals with TBI and their families (Degeneffe & Lee, 2015). As a result, caregivers typically handle care-recipient community living needs alone, without sufficient social and professional supports. This experience, in and of itself, is isolating and likely contributes to significant unnecessary psychosocial strain (Degeneffe & Lee, 2015). Moreover, families want long-term professional support (Bishop, Degeneffe, & Mast, 2006; Degeneffe & Lee, 2015); yet, participation in community support services “is challenged by content, availability, accessibility, quality, and coordination” (Degeneffe & Lee, 2015, p. 164). In light of these barriers, rehabilitation counselors need to pay particular attention to assisting persons with TBI and their family members to find, navigate, and access community supports to insure a continuum of care post injury. Rehabilitation counselors are trained in case management and service coordination; as such, they are in a good position to assist persons with TBI and their families in obtaining professional supports. Training in brain injury and family support (vs. individual support) however, is not common in rehabilitation counseling education programs and may contribute to some difficulties working effectively with persons with TBI and their families (Degeneffe & Lee, 2015). Degeneffe and Lee (2015) discuss best practice approaches for rehabilitation counselors working with persons with TBI and their families by examining environmental resources, innovations, empowerment, and effective professional–family collaborations.
We suggest that rehabilitation counselors use their counseling skills to address and improve family members’ caregiving self-efficacy. Specifically, studies show that TBI caregivers’ self-efficacy or underlying beliefs regarding their ability to provide care, is linked to successful coping and empowerment (Man, 1998). Degeneffe et al. (2011) identified four specific types of self-efficacy relevant to TBI caregiving, including advocacy, community, caregiver, and personal self-efficacy. Advocacy self-efficacy is related to a caregiver’s self-perceived ability to actively participate in the political process to promote services for people with brain injuries; community self-efficacy is a caregiver’s self-perceived ability to access VR services, community resources, legal help, and government benefits; caregiver self-efficacy is related to the ability to modify expectations regarding what can realistically be done, to know the ongoing needs, to select the appropriate health care and rehabilitation services, and to motivate the family member with TBI to engage in work and recreational activities; and personal self-efficacy is characterized by the self-perceived ability to cope with problems, to think positively, to find time for oneself, to manage emotions, and to maintain good physical and mental health (Degeneffe et al., 2011). These four types of self-advocacy skills comprise the Caregiver Empowerment Scale (CES; Degeneffe et al., 2011) and are positively linked to caregiver well-being. Rehabilitation counselors and researchers can use the CES to assess level of perceived self-efficacy among TBI family members as a means to develop more effective rehabilitation planning and intervention for the person with TBI. Indeed, improving a caregiver’s internal and external skills will likely translate into better outcomes for the rehabilitation client with TBI.
Our finding that professional and community support needs partially mediate the link between perceived burden and QOL is also consistent with prior research showing a relationship between TBI family needs and caregiver distress, burden, and QOL (Chronister et al., 2010; Kreutzer et al., 1994; Moules & Chandler, 1999; Nabors, Seacat, & Rosenthal, 2002). Specifically, those who reported, for example, having a professional to turn to for advice, having adequate professional TBI resources, having other family members who understand care-recipient problems, or experiencing care-recipients’ employer, co-workers, or teachers as understanding TBI (Arango-Lasprilla et al., 2010) report better QOL. These findings support the growing body of TBI caregiving literature that affirm the importance of providing professional and community supports for caregivers of TBI. Degeneffe and Lee (2015) discussed that rehabilitation counselors are in an ideal position to help caregivers of people with TBI to become familiar with the VR service delivery system and the complexity of the interactions with many professionals along with the recovery process for individuals with TBI, as they are trained to coordinate the integration of a full range of professional services and care for people with TBI.
On closer look at our second mediation analysis, an interesting finding emerged. Specifically, when social support and professional/community support needs were removed from the regression model, caregiving mastery emerged as a significant mediator between perceived burden and QOL. These results suggest that to reduce the effect of burden on QOL, intervening at the environmental level through social support and professional/community support needs is likely more effective than addressing personal variables such as mastery or coping. However, when environmental resources are not available, addressing a caregiver’s sense of mastery may mediate the negative effects of perceived burden on QOL. Caregiving mastery, or the self-appraised ability to deal with caregiving tasks and demands (Hanks et al., 2007), has been linked to better outcomes in the broader stress process literature as well as in the caregiving literature (Aneshensel et al., 1995; Thoits, 1987), and our study provides some additional evidence for its role in the TBI caregiving process. Moreover, caregiving mastery is essentially task or situation specific self-efficacy, which has been linked to positive outcomes across a wide array of situations with diverse populations (Chronister & Chan, 2006). In our study, mastery emerged as a second level mediator and was also positively linked to QOL, social support, and professional/community support needs in our correlation matrix. Thus, our findings suggest that caregiving mastery does play a role in facilitating positive outcomes, but how it works remains unclear. For example, it may be that caregivers who have more social and community/professional support experience a greater sense of mastery because they are better positioned to be successful with managing caregiving stressors; alternatively, it may be that those who enter the caregiving situation with a higher level of self-efficacy in general, are more apt to seek out the environmental supports needed to manage caregiving tasks. In either scenario, future research in this area is warranted, and facilitating interventions that allow caregivers the opportunity to successfully manage caregiving tasks is justified.
In summary, results of the current study highlight the unique and extensive support service needs of caregivers of people with TBI, including caregiver’s emotional, instrumental, social, professional, and community supports. Rehabilitation counselors are in a position to assess, understand, and provide the necessary family interventions for caregivers and care-recipients with TBI. The education and provision of knowledge about the different phases of rehabilitation, the integration of the varying types of medical and community-based interventions, and empowerment of family members by providing emotional and professional supports for caregivers are among the core functions of what rehabilitation counselors can do, which is consistent with addressing the personal and environmental needs of caregivers of people with TBI.
Limitations
There are several limitations that should be considered in interpreting the results of this study. First, the use of a convenience sample of caregivers attending support groups limits the generalizability of the results to other caregivers who do not attend support groups. The majority of participants were White females with a college education, and 50% had incomes above US$50,000 also limiting the generalizability to those that have a similar demographic pattern. Second, the use of a correlational research design does not allow us to conclude a cause–effect relationship between person–environment variables and QOL. Third, the use of self-report measures can lead to a common response bias inflating the relationship among the constructs in this study.
Fourth, functional disability scores were based on the caregiver’s perception of the care-recipient’s functioning that may be confounded by the caregiver’s emotional experience. Fifth, there are likely other caregiver personal variables such as health or employment status that may contribute to burden and QOL. Finally, although the professional/community support measure was developed specifically for caregivers of persons with TBI, our social support and coping measures were not TBI caregiver specific, and, therefore, may not have tapped into the particular supports or coping skills uniquely relevant to caregiving stressors.
Conclusion
Understanding the personal and environmental resources available to caregivers of persons with TBI is critical to promoting positive outcomes for this population. Indeed, caregivers of persons with TBI frequently face elevated levels of burden, stress, and depression due to the extensive and chronic nature of TBI; yet, our findings suggest that these outcomes can be mediated by positive, personal, and environmental factors, particularly social support, professional/community supports, and caregiving mastery. Unlike care-recipient level of impairment, these person–environmental resources are more amendable to change and have the potential to reduce the level of functional disability for the care-recipient; which in turn, may contribute to better health and well-being for both the caregiver and care-recipient.
Our findings may be more useful to rehabilitation counseling practice with additional research that determines which specific caregiver resources interact with what specific care-recipient activity and participation barriers to reduce the level of disability and improve QOL. In addition, future research is needed that investigates the particular types of social supports that are unique and relevant to caregiver stressors. At present, we have limited knowledge of the types of supports that match the particular types of caregiving stressors—knowledge that is important for social support intervention and assessment. Qualitative and longitudinal research is also sorely needed in this area. Few studies have investigated the phenomenological experience of TBI caregiving, with most TBI caregiving constructs and measures developed a priori, ignoring the experience of those providing the caregiving. Finally, caregiving is a dynamic process that changes over time, and to better understand the changing personal–environmental support needs of caregivers long-term, longitudinal research is needed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.