
Abstract
Resilience refers to one’s ability to adapt and navigate through challenges in the face of a chronic illness and disability (CID). Originally reported in posttraumatic stress literature, resilience has been studied in various contexts; however, very few studies have been conducted from a virtue perspective. Virtue, in psychological terms, is consistent, everyday action toward a worthwhile pursuit, based on one’s values. From a virtue perspective, resilience is defined as a positive by-product of having endured adversities while transforming them into insightful opportunities for renewal. This article introduces the virtue-based psychosocial adaptation model (V-PAM) and its applicability to the study of resilience. College students with CID (N = 256) were recruited, and their resilience was empirically examined based on the proposed model.
Keywords
The term resilience is defined as “positive adaptation in the face of a traumatic event” (Newman, 2005). This concept has attracted researchers interested in exploring why some individuals who experience overwhelming adversities do not succumb but rather move forward with greater success. Many studies of resilience have focused on the identification of both individual characteristics (e.g., emotional stability, effective communication skills, self-regulatory skills) and environmental characteristics (e.g., formal and informal networks) associated with resilience (Dowrick, Kokanovic, Hegarty, Griffiths, & Gunn, 2008; Edward & Warelow, 2005; Kathryn, Connor, & Jonathan, 2003; Ong, Bergeman, Bisconti, & Wallace, 2006). From these studies, a prototypical profile of resilience has emerged, such as having positive emotions, purpose in one’s life, impulse control, humor, self-acceptance, and supportive relationships (Feder et al., 2013; Fredrickson, 2009; Neenan, 2010). In addition, Reivich and Shatte (2002) agreed that resilience is not an entirely innate or fixed trait. Rather, they suggest that resilience can be learned and developed by actively reframing the challenges and struggles associated with adversities. Arguably, future research in the field of resilience should include a significant emphasis on the malleable aspects of this critical concept (McGrath, 2001; Prigatano, 1989). The present article introduces the virtue-based psychosocial adaptation model (V-PAM; Kim, McMahon, Hawley, & Brickham, 2016a), a new theoretical platform that encompasses the developmental and nurturing aspects of resilience from a virtue perspective, and examines its applicability in the context of resilience studies. As the study of virtue in modern psychology influenced the development of V-PAM, a brief overview is provided. This is followed by an introduction to V-PAM theory and its role in adjustment to chronic illness and disability (CID). Finally, an initial study on the use of the V-PAM as it relates to resilience in students with CID is presented.
Virtue Studies in Modern Psychology
Virtue was a primary area of inquiry in the 19th century, appearing, for example, in studies on citizenship, duty, deeds, and honor (Ross & Nisbett, 1991). However, it fell out of favor with the rise of empiricism, as the moral and philosophical aspects of virtue came to be considered an element of social ethics as opposed to a psychological construct that could be systematically investigated (Adams, 2006; Fowers, 2005). More recently, with the emergence of positive psychology, virtue has regained interest among scholars and has been actively studied in the contexts of thriving, well-being, happiness, and character education. Accordingly, many studies conducted in positive psychology have shown positive correlations between virtue and enhanced mental health (Duan, Guo, & Gan, 2015; Seligman, Steen, Park, & Peterson, 2005).
Positive psychology’s application of virtue-based perspectives to facilitate mental health and well-being helped establish a theoretical differentiation among the constructs of virtue, value, and character. According to Peterson and Seligman (2004), value is what one believes to be important but does not necessarily represent a person’s behaviors or define his or her actions. Virtue, on the contrary, is value in action. Thus, virtue is achieved only through the consistent practice of value. For example, the virtue of honesty can be developed and nurtured through consistent use of honesty in one’s daily actions. Once acquired, a virtue becomes an integral part of one’s character—a behavioral manifestation of one’s virtue—that represents who the individual is.
In research and practice, the theoretical clarification among the constructs of value, virtue, and character prompted the study of character education. One underlying assumption of character education is that it is possible to identify character traits relevant to specific life situations or wellness constructs such as well-being and life thriving, and thus promote the development of such traits (e.g., development of courage). Despite this theoretical contribution, some scholars argue that rehabilitation addresses unique and complex aspects related to CID, and to arbitrarily apply a character education approach may impede the individual’s psychosocial adaptation to CID. To illustrate, Linkins, Niemiec, Gillham, and Mayerson (2015) noted that prescriptive approaches are widespread in character education programs as some strengths are deemed more essential than others. Furthermore, Livneh and Martz (2016) cautioned that many applications of positive psychology focus on character dispositions acquired before the onset of CID and are therefore limited in their ability to explain developmental aspects of the psychosocial adaptation process that occurs as an individual progresses through his or her unique CID experience.
Small v Versus Capital V Virtue Perspective
In modern psychology, the varying virtue perspectives are categorized into small v and capital V. In the small v virtue perspective, emphasis is placed on identifying an individual character strength to recommend its nurturance. One benefit of this approach is that it allows for the scientific study of unique character strengths. For example, it was found that the character strengths of hope, zest, love, gratitude, and curiosity relate substantially to life satisfaction and well-being (Park, Peterson, & Seligman, 2004). Therefore, a recommendation can be made to nurture these strengths within the mental health setting.
Conversely, in the capital V virtue perspective, the focus is not on the identification of one’s character strengths, but rather on their contextual utilization. Unlike the small v perspective that sees one’s characters as strengths, the capital V virtue views one’s characters as assets that can grow as strengths if an individual is able to use these character assets in a contextually wise manner (Adams, 2006; Kim et al., 2016a). In other words, one’s character assets become true strengths only when used in an appropriate manner relative to the situation. The focus of the capital V virtue perspective is to explicate the constituents of virtuous behavior and help the individual use his or her character assets virtuously. The V-PAM is constructed from the capital V virtue perspective. The following sections introduce the V-PAM and discuss its applicability to the study of resilience in individuals with CID.
V-PAM
In applying the capital V virtue perspective to the understanding of psychosocial adaptation to CID, the V-PAM proposes five components that encompass and characterize one’s virtuous pursuit to reach personal excellence in dealing with CID—in other words, psychosocial adaptation. The five components are (a) Courage, (b) Integrity, (c) Practical Wisdom, (d) Committed Action, and (e) Emotional Transcendence.
Courage is one’s ability to face fear. However, it does not simply mean the absence of trepidation, as is implied when we say someone is brave. According to Peterson and Seligman (2004), “courage is an emotional strength that involves the exercise of will to accomplish goals in the face of opposition, external or internal” (p. 29). Courage also addresses one’s “initiative,” a quality that leads to action and is needed to redesign one’s life. To be virtuous, courage provides the power to initiate action despite any fears associated with CID. Thus, virtuous action to prosper with CID requires courage to face the unpredictability of life after the onset of CID, and to initiate a new course of action moving forward.
Integrity is a virtue concept that involves honesty and moral principles. It emphasizes the social, familial, and communal nature of virtue. It is often said that human beings have the right to pursue happiness. However, this is true only when such pursuit does not interfere with the rights of others. Thus, morality is an essential component of integrity. To illustrate, a selfish person can behave cleverly but does not recognize the importance of the common good as he or she seeks self-gratification at the expense of others (Fowers, 2005). In the context of psychosocial adaptation to CID, integrity is particularly important in terms of building harmonious relationships with others involved in the rehabilitation process including family members, medical and health professionals. Collaboration toward a complementary pursuit motivates people to work together, creating a sense of connectedness (Kim et al., 2011), which in this context can support adjustment and adaptation to CID.
Practical Wisdom is another virtue concept and V-PAM component. When adjusting to adversity such as CID, the individual must be able to decide on the best course of action in each specific life circumstance in a way that allows him or her to pursue worthwhile ends (Fowers, 2005). Accordingly, knowledge and experience are important components of Practical Wisdom that generally develop with age. However, continuous and deliberate reflection on actions and outcomes are also critical to the development of Practical Wisdom. Thus, Practical Wisdom goes beyond the simple acquisition and use of knowledge (Swartwood, 2013) to incorporate informed and thoughtful decision making.
Committed Action is the key constituent that leads to virtuous behavior, distinguishing virtue from value. Although the two words are often used interchangeably, value is what one believes to be important, whereas virtue implies consistent and committed action in a manner aligned with one’s values. Virtue is value in action (Adams, 2006; Fowers, 2005; Peterson & Seligman, 2004). To illustrate, most people would agree that honesty is an important value, but not all individuals behave honestly in their daily lives. As a virtue, “honesty” is reserved for individuals whose everyday behaviors and actions reflect the intentional application of honesty. Virtue is an observably consistent, action-oriented term.
Emotional Transcendence is a final constituent of virtuous behavior and the V-PAM. Emotional Transcendence helps individuals create meaning in their lives and reach emotional and mental concordance (Fowers, 2005). Emotional concordance enables individuals to internalize both positive and negative life experiences associated with CID in a synergistic manner. This process generates the authentic motivation needed to move through the challenges associated with CID and move forward with life. Thus, Emotional Transcendence encompasses the ability to infuse new hope into life and transform experiences into insights and renewal, even in the face of adversities (Young-Eisendrath, 1996).
The V-PAM was developed to address the issues in applying virtue study as conceptualized in a small v perspective. The V-PAM does not attempt to classify virtues into categories or assign relative value to virtues. Rather, it provides a framework for pursuing one’s excellence in a virtuous manner in the face of adversities. For instance, as applied in the context of rehabilitation, an individual with CID may recruit the virtue of Courage as a prerequisite to initiate the process of psychosocial adjustment. The individual may then utilize the virtue of Integrity to enhance a collaborative working alliance with the rehabilitation counselor, while concurrently applying the virtue of Practical Wisdom to reflect objectively on CID-related issues or concerns to then formulate a plan of action and make informed decisions specific to different situations or needs. Finally, throughout the course of the individual’s long-term journey with CID, Committed Action and Emotional Transcendence allow the individual to transform illness and disability experiences into insights and renewal that can facilitate growth and adaptation. More detailed information on the dynamics between the five V-PAM constructs can be found in the article titled “Psychosocial Adaptation to Chronic Illness and Disability: A Virtue-Based Model,” published in the Journal of Occupational Rehabilitation (Kim et al., 2016a).
Resilience and V-PAM
Resilience can be inferred or identified in the presence of (a) substantial and overwhelming adversities, such as CID, that stretch one’s coping capacity and (b) the occurrence of positive outcomes (Yates, Egeland, & Sroufe, 2003). For instance, during the process of psychosocial adaptation to CID, when people generate the will and motivation to push through and face adversity with a courageous mind-set, they may derive happiness from transforming challenges into insights and renewal. During this process, they keep their emotions in homeostatic peace, characterized by sound judgments, persistence, conviction, and, ultimately, the ability to celebrate what they have accomplished. In a rehabilitation setting, resilience can be viewed as the constructive navigation through life with CID.
Resilience assists an individual in coping with CID-related challenges by facilitating movement toward attaining goals and achieving success after the onset of CID. Neenan (2010) provided a description of resilience that is not about bouncing back to what was, but enduring hardships and allowing them to reshape oneself for the better: . . . being resilient does not restore the status quo in your life prior to the adversity—springing back to the way it was—but, rather, what you have learned from tackling the adversity changes you for the better and helps you to become more keenly aware of what is important in your life and, as we said, encourages you to pursue it. (p. 17)
In the rehabilitation context, resilient individuals persistently put forth their best effort and positively internalize distress purposefully through self-regulation (Young-Eisendrath, 1996). These aspects of resilience are well aligned with the five virtue constructs of V-PAM. As such, V-PAM holds promise for application in the study of resilience. The purpose of the current study was to empirically explore the applicability of the V-PAM in the context of resilience in individuals with CID.
Method
This study was designed to examine the applicability of V-PAM to resilience research. To carry out this investigation, the researchers (a) recruited 256 college students with CID, (b) grouped participants based on resilience level, (c) compared characteristics between the groups, and (d) tested the contributions of the five V-PAM factors to the observed differences between resilience groups.
Research Questions
Research Participants
Upon institutional board review (IRB) approval, 256 students with CID were recruited from university student disability offices of 10 universities, representing four of the five regions of the United States. Inclusion criteria included the presence of a chronic illness or disability, and age of 18 or older. Eligibility to receive services from a university student disability office (often referred to as Student Disability Services or Resource Center) is determined by medical documentation that proves the existence of disability. To ensure anonymity and confidentiality, the directors of participating student disability offices were responsible for identifying participants who did not meet criteria for inclusion in the present study.
Participants who did not meet the inclusion criteria were excluded by staff at each university’s respective disability resource center. An online platform was created in Survey Monkey that included an introductory information section and consent form, a demographic questionnaire, and self-report questionnaires consisting of three instruments. The estimated amount of time required to complete the online survey was between 30 and 45 min. The link was sent to the directors of participating university disability resource centers for distribution to students who met the inclusion criteria. Three reminders were sent at 10, 20, and 30 days following the initial invitation.
Instruments
Demographic Questionnaire
The demographic information collected in this study included age, gender, race, onset and type(s) of disability, functional limitations, and government benefits status.
Connor Davidson Resilience Scale
The CD-RISC (Connor & Davidson, 2003) is a 25-item measure using a 5-point rating scale (0 = not true at all to 4 = true nearly all of the time) that assesses subjective resilience (i.e., how the respondent has felt on a certain statement over the past month, for example, “able to adapt to change”). The total score ranges from 0 to 100, with higher scores reflecting greater resilience. Internal consistency for the general population is measured at .89 using Cronbach’s alpha. In the current sample, alpha was .92.
Satisfaction With Life Scale
The SWLS (Diener, Emmons, Larsen, & Griffin, 1985) is a five-item measure using a 7-point Likert scale (1 = strongly disagree to 7 = strongly agree) to assess subjective life satisfaction (e.g., “In most ways, my life is close to my ideal”). Alpha coefficients range from .79 to .89, indicating good internal consistency (Pavot & Diener, 2008). The total score ranges from 5 to 35, with higher scores reflecting greater life satisfaction. Test–retest reliability coefficients are between .54 and .84. Finally, the SWLS is significantly related to a single-item, global life satisfaction measure indicating its convergent validity (Van Beuningen, 2012). In the current sample, alpha was .90.
Adapted Inventory of Virtues and Strengths (AIVS)
The AIVS (Kim, Kim, Lee, & Hahm, 2014; Kim, Reid, McMahon, Gonzalez, & Lee, 2016) conceptualizes the five virtue factors of V-PAM in terms of a combination of testing items that reflect one’s character associated with each virtue factor. Using a semantic differential scaling format, individuals evaluate their character by reporting on a 7-point rating system. For example, hateful _ _ _ _ _ _ _ loving. The Courage factor has five items including commanding–submissive, bold–timid, leading–following, courageous–cowardly, and brave–fearful. The Integrity (e.g., trustworthy–untrustworthy) and Practical Wisdom (e.g., openminded–closeminded) factors include 11 items each, the Committed Action factor consists of seven items (e.g., persevering–quitting), and the Emotional Transcendence factor includes 12 items (e.g., forgiving–unforgiving). According to the AIVS development study, 385 adjectives that reflect one’s character and 270 corresponding antonyms were initially created, and then condensed into 64 pairs after a series of panel and expert reviews. Finally, 46 items were retained following factor analysis. The construct validity of the AIVS was examined using correlation analyses between AIVS subscales and measures of psychological well-being (r = .25–.46) and self-esteem (r = .34–.47). Discriminant validity was examined by evaluating the correlation between AIVS factors and a measure of hopelessness (r = −.39 to −.22). The reported alphas of the AIVS subscales in previous studies were .78 for Courage, .78 to .80 for Practical Wisdom, .77 to .79 for Integrity, .81 to .84 for Emotional Transcendence, and .63 to .78 for Committed Action (Kim et al., 2014; Kim et al., 2016b). Alpha coefficients in the current sample were .77, .79, .80, 86, and .79, respectively.
Results
This study employed three statistical analyses: (a) descriptive analysis, (b) cluster analysis followed by univariate analysis of variance (ANOVA), and (c) discriminant analysis followed by ANOVA. Preliminary analyses were also conducted for all variables to examine the distribution, central tendency, and dispersion (i.e., normality) of the data with skewness (≤|2.0|) and kurtosis (≤|4.0|) at a level not exceeding the standard values. All individual cases met the criterion of responding to more than half of the items in every one of the subscales, and the replacement-with-means method was used to handle any remaining missing values. All statistical procedures were carried out using IBM SPSS 21. The results are presented below.
Descriptive Statistics
Descriptive statistics were used to characterize the sample. The sample consisted of 33% male and 66% female participants. The majority of participants were between 20 and 30 (46.9%), and the sample was primarily comprised of White (non-Hispanic, 85.2%) individuals. While 54% of the sample reported their CID as congenital, 42.2% reported it as acquired. Only 30% were receiving government benefits, and the majority reported varying types of functional limitations. Table 1 below provides a summary of these results.
Descriptive Statistics for Participants (N = 256).
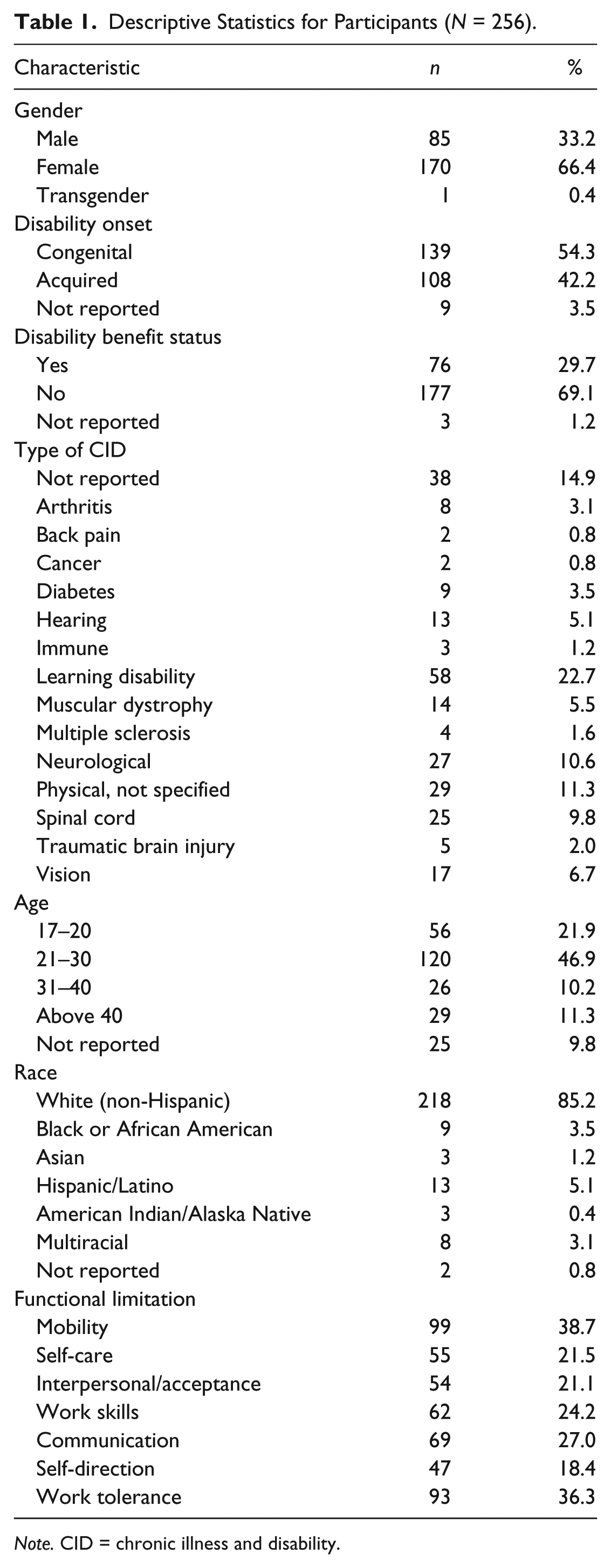
Note. CID = chronic illness and disability.
Cluster Analysis and Follow-Up Univariate ANOVA
To answer the first research question, participants were clustered based on CD-RISC and SWLS total scores using Ward’s minimum variance method (Ward, 1963). Ward’s method minimizes within-group variation and maximizes between-group variation which enabled identification of homogeneous subgroups based on resilience level, as indicated by the mean profile of CD-RISC and SWLS (Aldenderfer & Blashfield, 1984; Berven & Scofield, 1982). To determine the clustering hierarchy, changes in the agglomeration coefficients were examined. Results for the last 10 levels are reported in Table 2.
Changes in Agglomeration Coefficient.
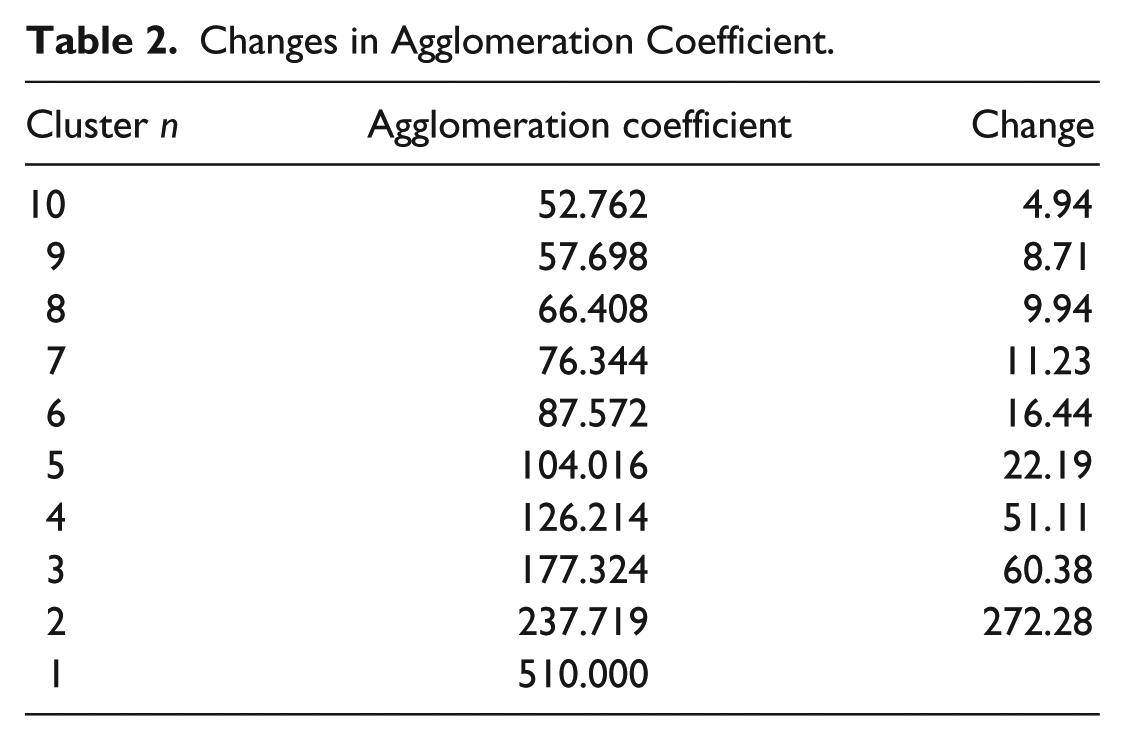
In comparison with relatively little loss in within-cluster homogeneity at preceding levels (60.38 and 51.11), there was a relatively large drop-off in homogeneity for coefficients moving from the first level to the second level (272.28), going from one to two clusters. Examination of these changes in coefficients suggested that the level containing two participant clusters was the optimal partition.
To analyze the unique features of each cluster (Research Question 2), the cluster analysis was followed by ANOVA. Again, because resilience has implications beyond simply dealing with hardships and carries positive connotations within the psychosocial adaptation literature (Limonero, Tomas, Ferandez, GomezRomero, & Aradilla, 2012), resilience was conceptualized in terms of the combined resilience and life satisfaction scores. ANOVA results are described in the following section.
The first group included 133 students with CID whose mean profiles on CD-RISC and SWLS were relatively lower (labeled as the low-resilience group); members of the second group were higher (labeled as the high-resilience group). Table 3 provides a summary of the mean profiles for CD-RISC and SWLS of each cluster. By using ANOVA, significance testing to compare mean differences between groups on these scales was completed. Scores of life satisfaction and resilience were also compared using ANOVA. The homogeneity of variance was tested, and results indicated that the assumption of ANOVA analysis was met, and mean scores on the CD-RISC and SWLS in each cluster were significantly statistically different, F(1, 255) = 282.67, p < .0001, and F(1, 255) = 299.45, p < .0001, respectively.
Descriptive Statistics of V-PAM Factors and Congenital Versus Acquired Disability in Each Cluster.
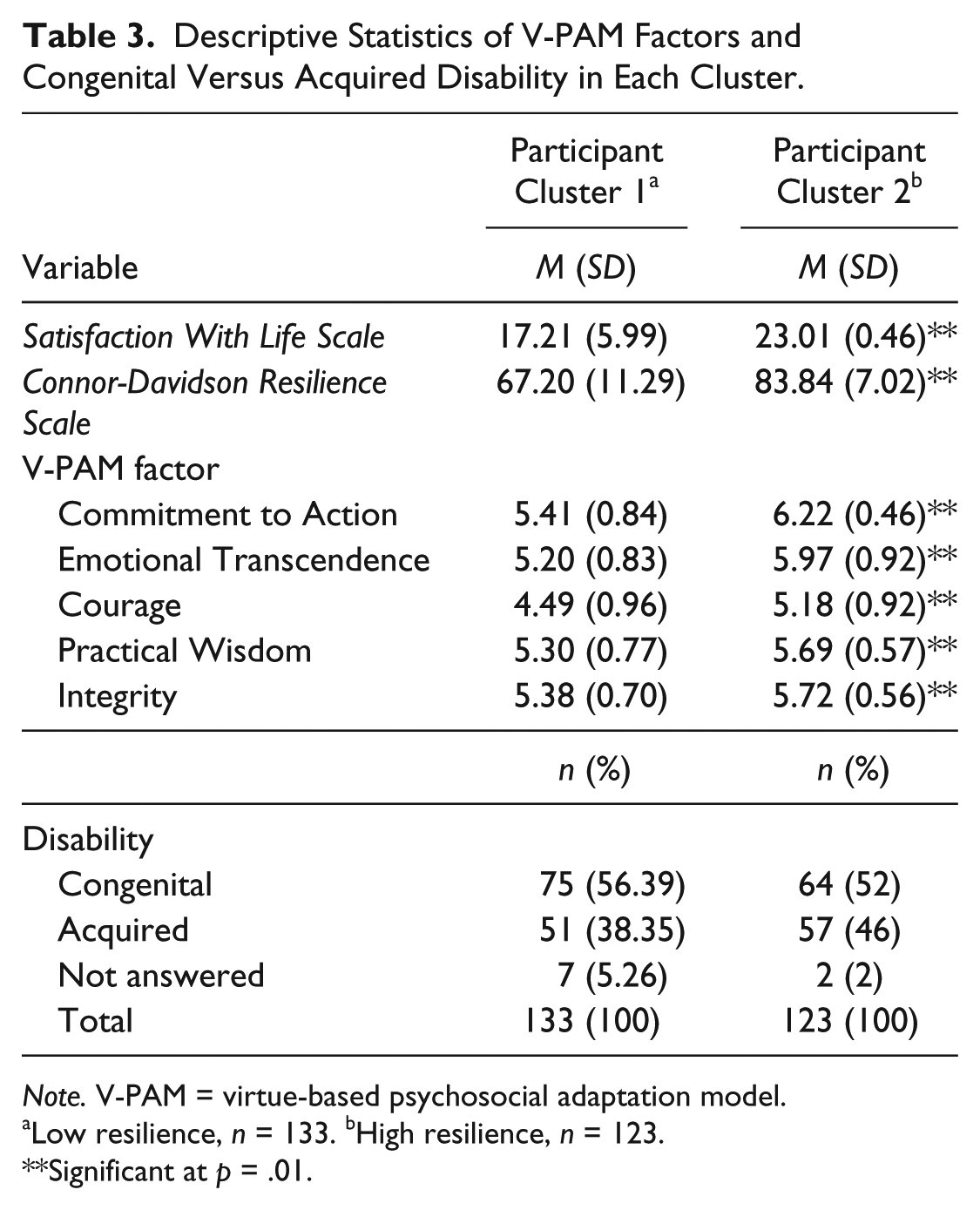
Note. V-PAM = virtue-based psychosocial adaptation model.
Low resilience, n = 133. bHigh resilience, n = 123.
Significant at p = .01.
Discriminant Analysis and Follow-Up ANOVA
To address whether the resilience clusters could be differentiated on the basis of the five virtue factors (Courage, Integrity, Practical Wisdom, Emotional Transcendence, and Committed Action), discriminant analysis was conducted. Resilience cluster memberships served as the group variables, and scores from the AIVS subscales were used as the discriminating variables. The discriminant analysis produced only one significant discriminant function, indicating parsimoniousness of both findings and interpretation, λ = .656, χ2(df = 5, n = 256) = 106.151, p < .0001. The structure matrix table below (see Table 4) provides the correlation between the five virtue factors and the discriminant function. Group centroids along the discriminant function indicated that Cluster 1 (low-resilience group) was located at the negative end (−.694), and Cluster 2 (high-resilience group) was located at the positive end (.751).
Correlations Between Virtue Factors (Structure Matrix).
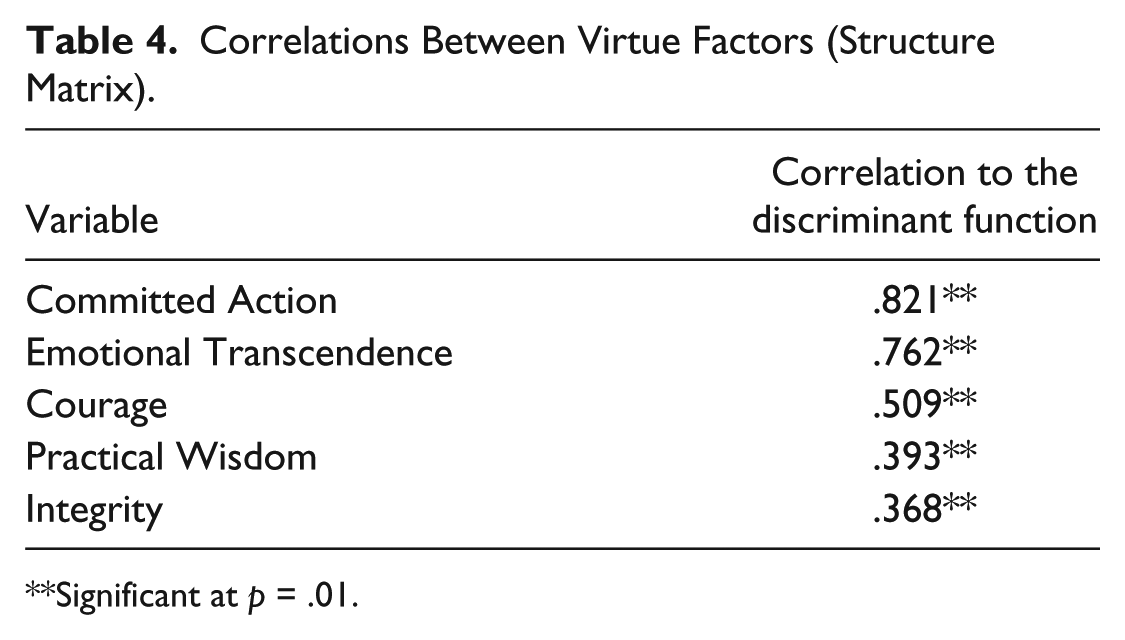
Significant at p = .01.
ANOVA was then performed to determine whether differences between each group’s virtue factors were statistically significant. Results confirmed statistical differences in all five virtue factors and are as follows: Committed Action, F(1, 255) = 89.919, p < .0001; Emotional Transcendence, F(1, 255) = 77.411, p < .0001; Courage, F(1, 255) = 34.555, p < .0001; Practical Wisdom, F(1, 255) = 20.633, p < .0001; and Integrity, F(1, 255) = 18.018, p < .0001. Table 3 provides a summary of the five virtue factors’ mean and standard deviation profiles.
Additional Descriptive and Multiple Regression Analyses
Because only two clusters (high vs. low well-being) were identified and all V-PAM factors were significantly correlated to the discriminant function, two additional statistical procedures were employed. First, descriptive analysis was used to pair resilience cluster memberships with the disability status (congenital vs. acquired), and no discrepancy was identified (see Table 3). Second, multiple regression analysis using simultaneous method was employed to examine the power of the V-PAM factors in predicting resilience. To be consistent with the way resilience in the current study was conceptualized, the scores of the CD-RISC and SWLS were collapsed by multiplying the two scores. The results showed that the multiple regression coefficient (R), using all the predictors simultaneously, was .64 (R2 = .41; adjusted R2 = .40), meaning that 40% of the variance in resilience scores was explained by the V-PAM factors.
Discussion
The present study explored the applicability of the V-PAM, within a resilience framework, for college students with CID. Although resilience is often defined as one’s ability to steer through life’s adversities (Neenan, 2010), resilient people also tend to report relatively high levels of life satisfaction (Cohn, Fredrickson, Brown, Mikels, & Conway, 2009). Thus, a measure of resilience was paired with a measure of life satisfaction to better conceptualize the resilience construct. Results indicated that students with CID can be grouped according to their resilience level as defined by the scores of the CD-RISC and SWLS and that the five virtue factors (i.e., Committed Action, Practical Wisdom, Integrity, Emotional Transcendence, and Courage) explain group differences in resilience levels. Specifically, the first group showed relatively lower resilience and life satisfaction, whereas the second showed higher resilience and life satisfaction.
Resilience cluster memberships were then discriminated based on the five virtue factors of the V-PAM. The results of this analysis were strong and indicated that only one significant discriminant function exists and that all five virtue factors contributed significantly to the distinction between the two groups. The strength of the contribution in differentiating group membership was investigated using the correlation between virtue factors and the discriminant function. The virtue factors in order of strength were Committed Action (r = .821), Emotional Transcendence (r = .761), Practical Wisdom (r = .509), Courage (r = .393), and Integrity (r = .368; see Table 3, structure matrix). ANOVA also provided statistical confirmation that the groups differed on each of the five virtue factors. Based on the finding that all V-PAM factors were significantly correlated with the discriminant function, multiple regression analyses with simultaneous method were followed, indicating that 40% of the variance in resilience can be predicted by V-PAM factors.
Resilience group memberships were paired with disability status (congenital vs. acquired) with an assumption that individuals with congenital disabilities would be more prevalent in the high-resilience group, as studies suggest that people with congenital disability show better adjustment (Bogart, Tickle-Degnen, & Ambady, 2012). For example, VanSwearingen, Cohn, Turnbull, Mrzai, and Johnson’s (1998) study of people with facial paralysis showed high levels of anxiety and depression in the acquired disability group when compared with those with congenital facial paralysis. Similar results were also found in Bogart and Matsumoto’s (2010) study on Moebius syndrome, which compared psychological distress between groups. However, no discrepancy was found in the current study between congenital and acquired disability groups, indicating that resilience in the current study is better explained by virtue than other possible confounding variables. These findings shed light on the utility of the V-PAM in facilitating resilience and life satisfaction in individuals with CID.
Implications for Rehabilitation Counseling
The findings of the present study hold important implications for rehabilitation counselors working with clients with CID. As previously mentioned, resilience can be learned and developed by actively reframing the challenges and struggles associated with adversities such as acquiring and/or living with CID (Reivich & Shatte, 2002). Research further points to the importance of adaptive coping following adversity, and the contribution of therapy in increasing one’s coping skills (Lazarus, 1993). Rehabilitation counselors thus play an important role in assisting clients with CID in developing and maximizing their resilience and life satisfaction through the use of various theories, interventions, and clinical skills. In this section, we discuss how the V-PAM can be incorporated into these existing approaches to better serve clients with CID in their reframing of adversity.
A major emphasis in rehabilitation counseling is on strength-based practice (SBP), defined as “facilitating the discovery and embellishment, exploration, and use of client strengths and resources in the service of helping them achieve their goals and realizing their dreams” (Saleebey, 2012, p. 1). As part of this endeavor, Peterson and Seligman (2004) constructed the Values in Action Inventory of Strengths (VIA-IS), a measure of character strengths that identifies an individual’s top strengths. While this tool is useful, the identification of top strengths does not indicate which strengths are beneficial or ideal for use in a particular context, nor does it assign relative value to strengths as they may apply to different situations (Adams, 2006).
The V-PAM addresses this void by providing a practical framework for the active application of character assets to psychosocial adaptation to CID-related challenges. For example, one’s spirituality may serve to promote Courage; however, if used without Practical Wisdom, the individual may become overly reliant on spiritual healing and may overlook the importance of pursuing necessary medical treatment. By supporting the thoughtful consideration of V-PAM constructs in applying identified character assets, the rehabilitation counselor can guide the client to develop the ability to identify and apply appropriate character assets to support coping in particular situations. Returning to the example above, the rehabilitation counselor may help the client employ Integrity by drawing on the therapeutic alliance and the client’s overall goals to develop a plan of Committed Action. Ongoing counselor-client interactions based on the V-PAM framework can then promote Emotional Transcendence as the client learns to independently identify, apply, and evaluate the use of relevant character assets in diverse challenging situations.
The V-PAM can also be used in conjunction with existing state and federal vocational rehabilitation counseling models. V-PAM factors can be utilized to facilitate candidates’ movement through the vocational rehabilitation process, which includes intake, eligibility determination, individualized plan development, follow-up, and termination. For example, an emphasis might be placed on Courage and Committed Action during the intake and eligibility determination stages; Practical Wisdom during the plan development stage; Committed Action, Practical Wisdom, and Emotional Transcendence during the implementation stage; and Courage and Emotional Transcendence during the follow-up and termination stages.
The V-PAM also aligns well with other therapeutic approaches such as acceptance and commitment therapy (ACT; Hayes, Strosahl, & Wilson, 1999) and cognitive behavior therapy (CBT; Beck, 2010). The V-PAM factors correspond with ACT’s emphasis on both behavior changes and values clarification, gained through mindfulness- and acceptance-based coping strategies. CBT emphasizes identifying and challenging one’s negative thoughts, through which counselors use reframing, cognitive restructuring, and relaxation strategies. V-PAM factors can be used to support constructive reflection on the positive outcomes of the thought-challenging process. For instance, the rehabilitation counselor might draw the client’s attention to how the thought-challenging process helps clarify the situation and make informed decision making possible (i.e., Practical Wisdom) and encourage forward movement and adaptation and success in the face of challenges (i.e., Courage and Committed Action).
Beyond the traditional rehabilitation counseling process, the V-PAM holds promise for application to additional contexts, specific client populations, and patient support networks. For instance, the V-PAM may be well suited for application to people with disabilities and co-occurring substance use disorders (SUD). The V-PAM factors have cross-over capabilities and are already being utilized in the treatment of SUD. For example, within the transtheoretical model (i.e., Stages of Change; Prochaska & DiClemente, 1982) often applied to substance abuse treatment, the V-PAM could be applied to support the behavior change process in clients with SUD and other behavior-dependent conditions. With regard to patient support networks, the V-PAM could be employed to promote communication, cohesion, and resilience in the patient–family, patient–caregiver, or patient–social support network contexts. The V-PAM could serve as a framework for relationship-based interventions that address the challenges associated with handling CID within critical social relationships (e.g., Keitner, 2015).
Virtue-informed rehabilitation and therapeutic services may empower clients to find the courage to cope with challenges as professionals both teach and model virtue-based processes. For instance, the appropriate selection and application of evidence-based treatments requires Practical Wisdom on the part of the professional, while the development of a strong therapeutic alliance models and builds Integrity and promotes an Emotionally Transcendent experience for both parties. Incorporation of a virtue-based perspective such as V-PAM may promote personal and professional success for the client and the professional within the context of the therapeutic relationship.
Implications for Future Research
The findings of the present study are limited by the use of a university student sample, as well as the potential that there could be additional individual and disability-related variables that were not assessed but contribute meaningfully to resilience group membership. Future research should assess factors such as intensity or level of functional impairment, duration and severity of chronic illness or disability, and perceived social support, which could further inform the understanding of low- versus high-resilience individuals. It is also important to note that, although it ensures anonymity and confidentiality of the research participants, the inability to estimate response rate due to the data collection carried out by the multiple participating university offices is a limitation of the current study.
The use of the two primary measures administered could also be considered a limitation in that they may not represent the full spectrum of resilience and life satisfaction constructs and were both self-report measures. The use of additional measures assessing other related constructs such as health-related quality of life may be informative in future studies. The use of observational and multi-informant approaches could also enhance the evaluation of V-PAM’s application to resilience in CID. Replication of this study in additional samples and populations, the collection of additional potentially relevant variables, and the use of alternative measures will help strengthen theoretical support and guide future refinement of V-PAM and any associated interventions.
Future research should examine each of the V-PAM factors individually in rehabilitation contexts. For example, Emotional Transcendence implies that an individual has faced challenges associated with CID and constructed an identity that productively incorporates CID as a part of the self. Thus, this construct can be correlated to disability acceptance and value change (Wright, 1983) within the field of rehabilitation. It is also possible to correlate changes in V-PAM constructs, such as the value placed on Emotional Transcendence over time throughout the rehabilitation process, to better understand the development of resilience following adversity. In addition, considering that the V-PAM emphasizes the positive and constructive interaction effects of its constituent virtue factors, the interaction among virtue factors is another beneficial area of study. Finally, the model warrants further refinement and validation for use with different disability subpopulations.
Conclusion
The purpose of the present study was to investigate the applicability of a virtue-based perspective, the V-PAM, in understanding resilience in individuals with CID. Overall findings indicated that each of the five virtue factors proposed by the V-PAM is highly relevant to the study of resilience within the context of rehabilitation and CID. Specifically, Committed Action was the strongest contributor to resilience, followed by Emotional Transcendence, Practical Wisdom, Courage, and Integrity. The results of the present study capture a more holistic understanding of resilience as it pertains to individuals with CID, and provide insights for incorporating virtue-based perspectives such as the V-PAM into a rehabilitation counseling context.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.