
Abstract
The purpose of this article is to examine the results of the certified rehabilitation counselor (CRC) knowledge validation study conducted in collaboration with the Commission on Rehabilitation Counselor Certification (CRCC). The research design for the present study includes both descriptive and ex post facto approaches. Three hundred ninety-four CRCs completed the Knowledge Validation Inventory–Revised (KVI-R) survey. Factor analysis results revealed six knowledge domains: (a) rehabilitation and mental health counseling, (b) employer engagement and job placement, (c) case management, (d) medical and psychosocial aspects of chronic illness and disability, (e) research methodology and evidence-based practice, and (f) group and family counseling. The findings of this study provide important information for CRCC to examine and develop test and item specifications that will guide future versions of the CRC examination. The findings also inform the description of the knowledge base underlying the practice of rehabilitation counseling and contribute further empirical evidence regarding the knowledge domains identified in this replication and extension of the previous study completed in 2012.
Keywords
Among the different counseling disciplines, the certified rehabilitation counselor (CRC) credentialing process is the oldest and most reputable certification mechanism in the United States (Leahy, Chan, Sung, & Kim, 2013; Leahy & Holt, 1993). The application of scientific research to develop the test and item specifications has been the hallmark of the CRC certification examination (Leahy et al., 2013). Rubin and colleagues (1984) conducted the first national role and function study of the CRC, and provided the test specifications for refining the content of the certification examination and the item pool. Since 1985, the Commission on Rehabilitation Counselor Certification (CRCC) has been conducting role and function and knowledge validation studies regularly to ensure the relevance and validity of the Certified Rehabilitation Counselor Examination (CRCE, Leahy et al., 2013). Findings from these studies were also used by the Council on Rehabilitation Education (CORE) to develop curriculum standards for master’s program in rehabilitation counseling. With the merger of CORE to the Council for Accreditation of Counseling and Related Educational Programs (CACREP), CRC role and function study becomes even more important for integrating rehabilitation counseling contents in the CACREP curriculum standards for the rehabilitation counseling specialty area.
Leahy and colleagues (2013) conducted a CRC study with a representative sample of CRCs to examine the major job functions and knowledge domains required for the professional practice of rehabilitation counseling. They found that rehabilitation counseling practice and the service delivery environments are changing swiftly, and rehabilitation counselors are practicing in diverse clinical settings. Their study was conducted with a goal to revise and update the test specifications for the CRCE. Specifically, three major rehabilitation counselor job functions and four knowledge domains were identified (see Table 1; Leahy et al., 2013).
Job Functions and Knowledge Domains Identified by Leahy et al. (2013).
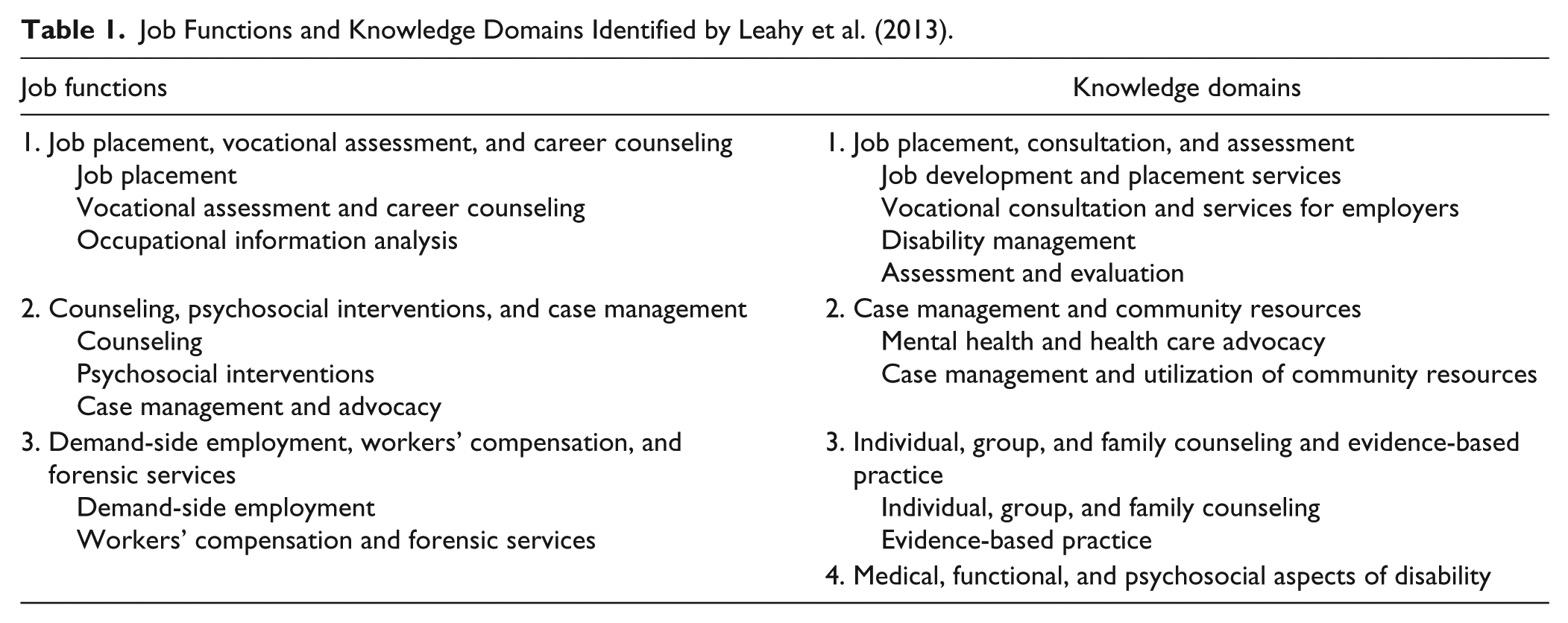
Findings from the Leahy et al. (2013) study provided a strong empirical support for the certification processes as well as information to guide the development of test specifications for the CRCE process. However, more than 5 years have passed since the most recent study completed in 2012 (Leahy et al., 2013). Over the past several years, enormous changes have taken place in the rehabilitation counseling profession, including the merger between CORE and CACREP on July 1, 2017 (CACREP, 2015). Clinical settings for the professional practice of rehabilitation counseling have continued to diversify, and the delivery of services has continued to evolve to address the physical and mental well-being and employment needs of people with disabilities (Chan et al., 2017). Recognizing these changes in the field and consistent with the accreditation requirements that CRCC regularly studies and reviews the test and item specifications used to guide the CRCE process, a new study was undertaken in 2016 to examine the major knowledge domains of rehabilitation counseling practice in diverse practice environments. The findings and specific data from this study have recently been used by the CRCC to examine and develop test specifications for future versions of the CRCE as well as for the continued accreditation of the CRCC. The purpose of this article is to report the results of the CRC knowledge validation study conducted by the CRCC in 2016.
Research Design and Research Questions
The research design for the present study includes both descriptive and ex post facto approaches. Specifically, factor analysis was used to examine major knowledge domains underlying the professional practice of rehabilitation counseling. The ex post facto portion of the study includes comparisons of knowledge domain scores across rehabilitation practice settings and counselor licensure status. The research questions addressed in the present study are as follows:
Method
Participants
A sample of CRCs was randomly selected from the CRCC database, and data were collected from August 24, 2014, through October 10, 2014. In addition to the initial email request to participate, potential participants received three additional follow-up email requests before the end of the data collection process to increase overall response rate. Three hundred ninety-four out of 1,809 CRCs who received email completed the KVI-R survey, for a usable response rate of 21.8%. Of the 394 participants who submitted KVI-R survey questionnaires, 317 provided responses with less than 5% missing at the item level.
Respondents included 69.9% women and 30.1% men, with mean age of 48.09 years (SD = 12.53 years). They had an average of 14.83 years (SD = 11.15 years) of experience since receiving their CRC credential. In addition to being a CRC, 88 participants (27.8%) indicated that they are also an LPC. For the purpose of this study, LPCs refer to licensed professional counselors, licensed clinical professional counselors, and licensed mental health counselors. The majority of the respondents identified themselves as Caucasian/non-Hispanic (82.4%), followed by African Americans (10.1%), Hispanic/Latino Americans (3.6%), Asian Americans (1.6%), American Indian/Native Americans (0.3%), and Other (2.0%). Most respondents have master’s degree (81.3%) for their highest degree earned followed by doctoral degree (13.0%), bachelor’s degree (1.6%), and other (4.1%). Academic majors of the participants included (a) rehabilitation counseling (71.3%), (b) other counseling specialty (7.6%), (c) rehabilitation psychology (4.1%), (d) psychology (4.1%), (e) other rehabilitation specialty (2.5%), (f) social work (0.9%), and (g) other (9.5%). Rehabilitation practice settings reported by the participants included (a) public vocational rehabilitation agencies (34.1%), (b) private/proprietary rehabilitation companies (24.0%), (c) schools and universities (15.1%), (d) medical/psychiatric facilities (10.4%), (e) nonprofit rehabilitation facility/organizations (6.3%), and (f) other (10.1%). The demographics of the current study sample was reflective of the actual overall population demographics for CRCs.
Measures
KVI-R
The KVI-R developed by Leahy et al. (2013) was used as the primary instrument for the study. The current version of the KVI-R was first carefully reviewed and revised through a Delphi study with a panel of subject matter experts before being distributed for the study. In addition, a Demographic Questionnaire was used to collect demographic information (e.g., gender, age, race/ethnicity, years of experience, job settings, job titles, and LPC credentials) from the CRC participants.
Delphi study
To validate and revise the KVI-R, the Delphi method was used to obtain consensus of a panel of practitioners, educators, and researchers who are experts in the professional competencies of rehabilitation counseling. Twenty-one experts were nominated by members of the CRCC Examination and Research Committee. Nine agreed to participate. The expert panel comprised five men and four women, with mean age of 42.75 years (SD = 11.02 years). Seven were Caucasians and two were Asian Americans. Two of the expert panel members reported having a disability. The majority of the respondents have either a master’s degree (44.4%) or a doctoral degree (44.4%). The job titles reported by the participants include (a) professor (44.4%), (b) vocational rehabilitation counselor/specialist (22.2%), (c) administrator/manager/owner (11.1%), (d) supervisor (11.1%), and (e) transition specialist (11.1%). They rated (a) relevancy of the 91 original KVI-R items to the contemporary practice of rehabilitation counseling using a yes/no format and (b) the importance of 25 new knowledge items using a 5-point Likert-type importance rating scale (1 = not important, 2 = somewhat important, 3 = important, 4 = very important, and 5 = extremely important). Findings from the panel of experts indicated that most KVI-R items are still highly relevant for contemporary rehabilitation counseling practice. Only one item from the original scale and three new items met the threshold of concern in terms of low mean importance ratings. After a careful review of the descriptive statistics and contents of the items, two items were eliminated from the instrument before subjecting the KVI-R for an exploratory factor analysis due to low means on the importance of the items to practice and outcomes. These two items are (a) concepts and principles of organizational development and stakeholder management and (b) life-care planning and life-care planning services.
Knowledge Validation Inventory–Revised–Final version
The final version of the KVI-R for this study is a 114-item survey instrument. Respondents were asked to rate the importance of each knowledge item using a 5-point Likert-type scale (1 = not important, 2 = somewhat important, 3 = important, 4 = very important, and 5 = extremely important) related to the professional practice of rehabilitation counseling.
Data Analysis
An exploratory factor analysis using principal axis factoring (also known as common factor analysis) was performed to identify the underlying dimensions of the KVI-R scores important for the professional practice of rehabilitation counseling (Clark & Watson, 1995; Costello & Osborne, 2005; Floyd & Widaman, 1995). A MANOVA was computed to test the differences among rehabilitation counselors who worked in different practice settings on the linear combination of the major rehabilitation counseling knowledge domains derived from factor analysis. When a multivariate effect was found, a follow-up univariate ANOVA was computed for each dependent variable.
Results
RQ1: What Are the Underlying Dimensions of the KVI-R Scores?
The Kaiser–Meyer–Olkin measure of sampling adequacy for the KVI-R items was .95, which exceeded the minimum criteria of .50, suggesting the sample was factorable (Costello & Osborne, 2005). The Bartlett’s test of sphericity, which tests the null hypothesis that the correlation matrix is an identity matrix, was found to be significant, χ2(6,441, N = 317) = 28,858.14, p < .001, indicating that correlations in the data were appropriate for factor analysis. Finally, the communalities were all above .3, confirming that each item shared some common variance with other items. Initially, the Kaiser–Guttman rule (eigenvalue greater than 1) was used to determine how many factors should be retained (Nunnally & Bernstein, 1994). A 21-factor solution was indicated. Cattell’s scree test was used as an alternative method to determine the number of factors to retain (Cattell, 1966; Gorsuch, 1990). Using the scree test, a six-factor solution (accounting for 51.3% of the variance) was indicated and it was rotated to simple structure using promax rotation. Next, items with factor loadings equal to or greater than .35 were retained for further analyses. The final six-factor solution was found to be parsimonious, meaningful, and interpretable. For three of the larger factors, additional factor analyses were performed to identify subdomains to increase the homogeneity and interpretability of the item clusters. The mean importance rating, the factor loading, and the communality for each knowledge item in each of the six knowledge domains are presented in Table 2. In addition, the subdomains for the first three knowledge domains are presented in Tables 3 to 5.
Means, Standard Deviations, and Factor Loadings for the Six Knowledge Domain Factors.
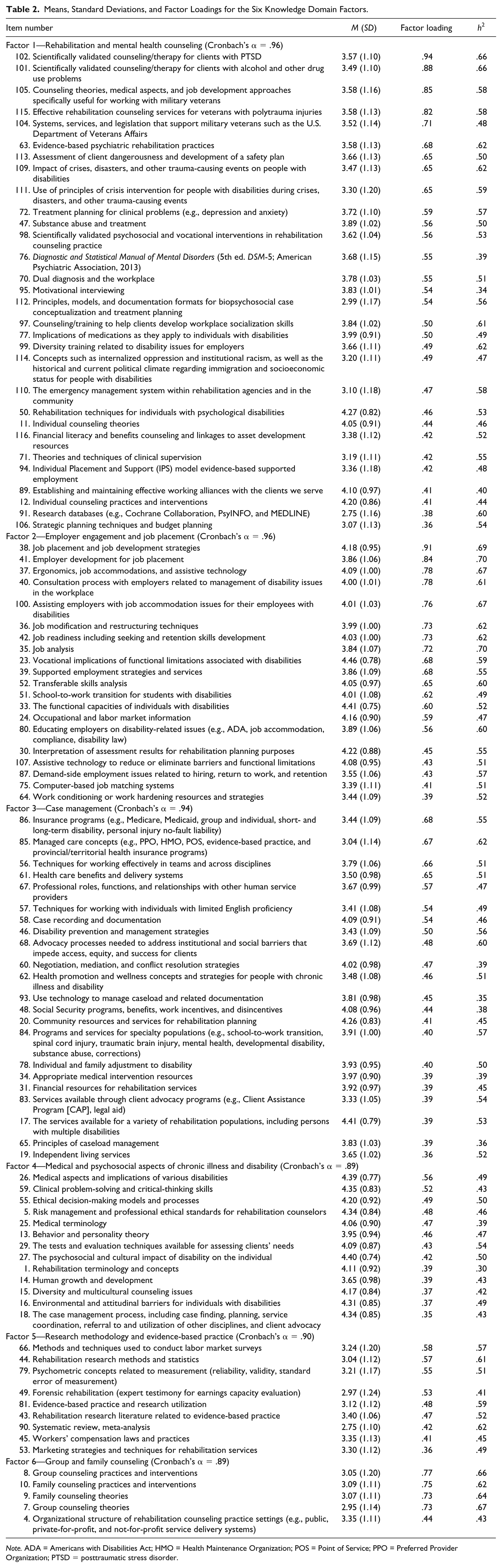
Note. ADA = Americans with Disabilities Act; HMO = Health Maintenance Organization; POS = Point of Service; PPO = Preferred Provider Organization; PTSD = posttraumatic stress disorder.
Means, Standard Deviations, and Factor Loadings for Subdomains in Factor 1.
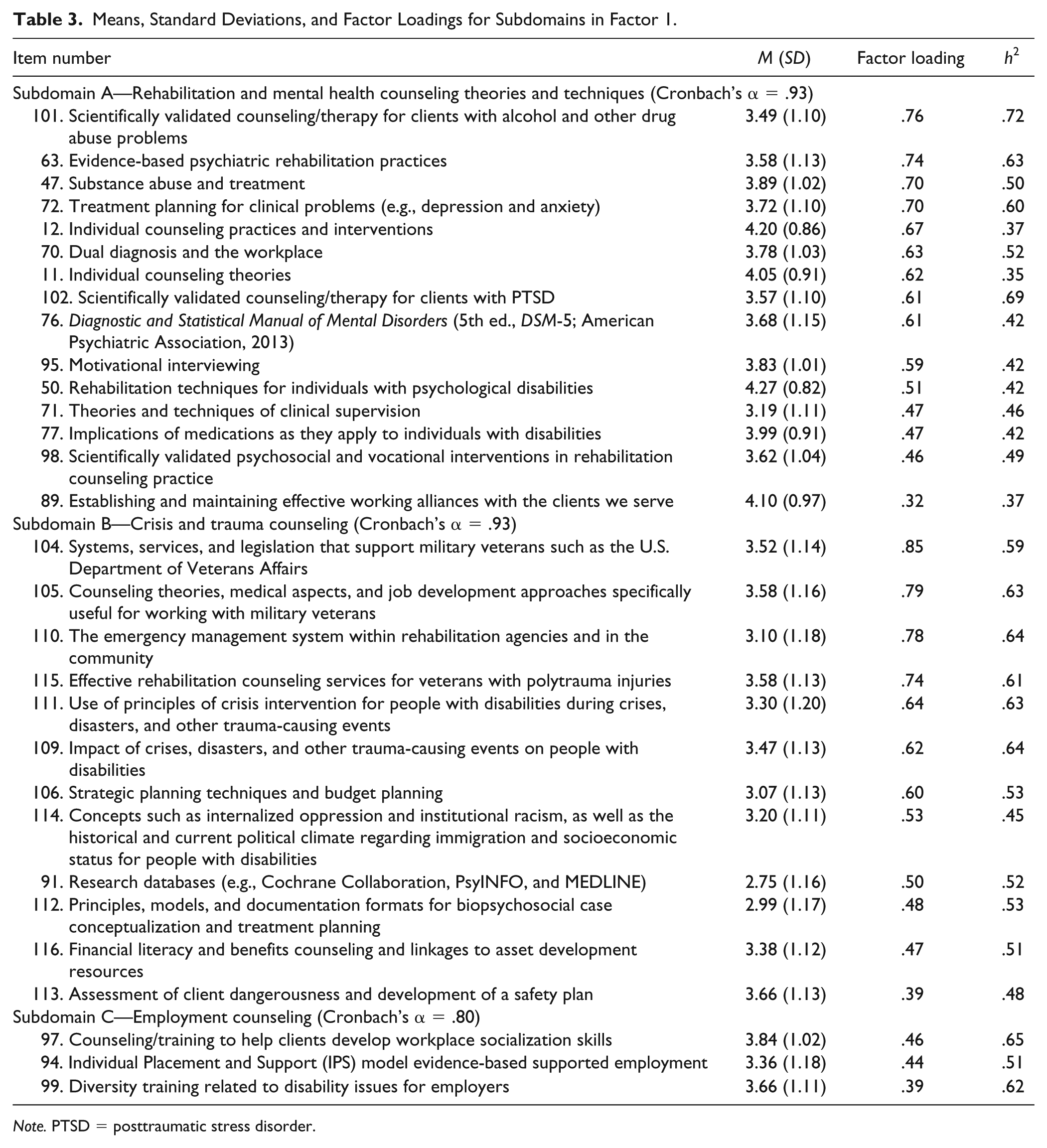
Note. PTSD = posttraumatic stress disorder.
Means, Standard Deviations, and Factor Loadings for Subdomains in Factor 2.
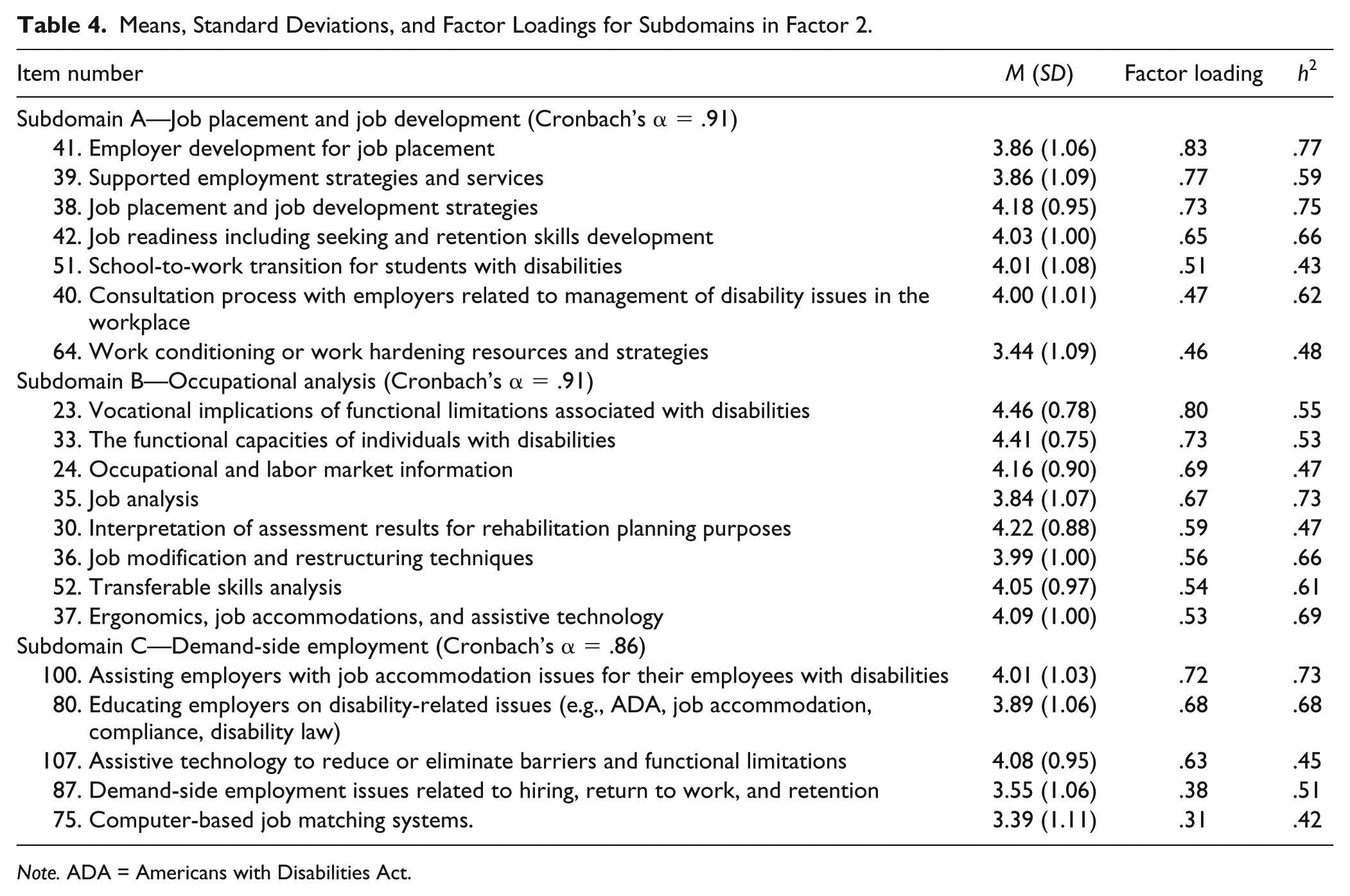
Note. ADA = Americans with Disabilities Act.
Means, Standard Deviations, and Factor Loadings for Subdomains in Factor 3.
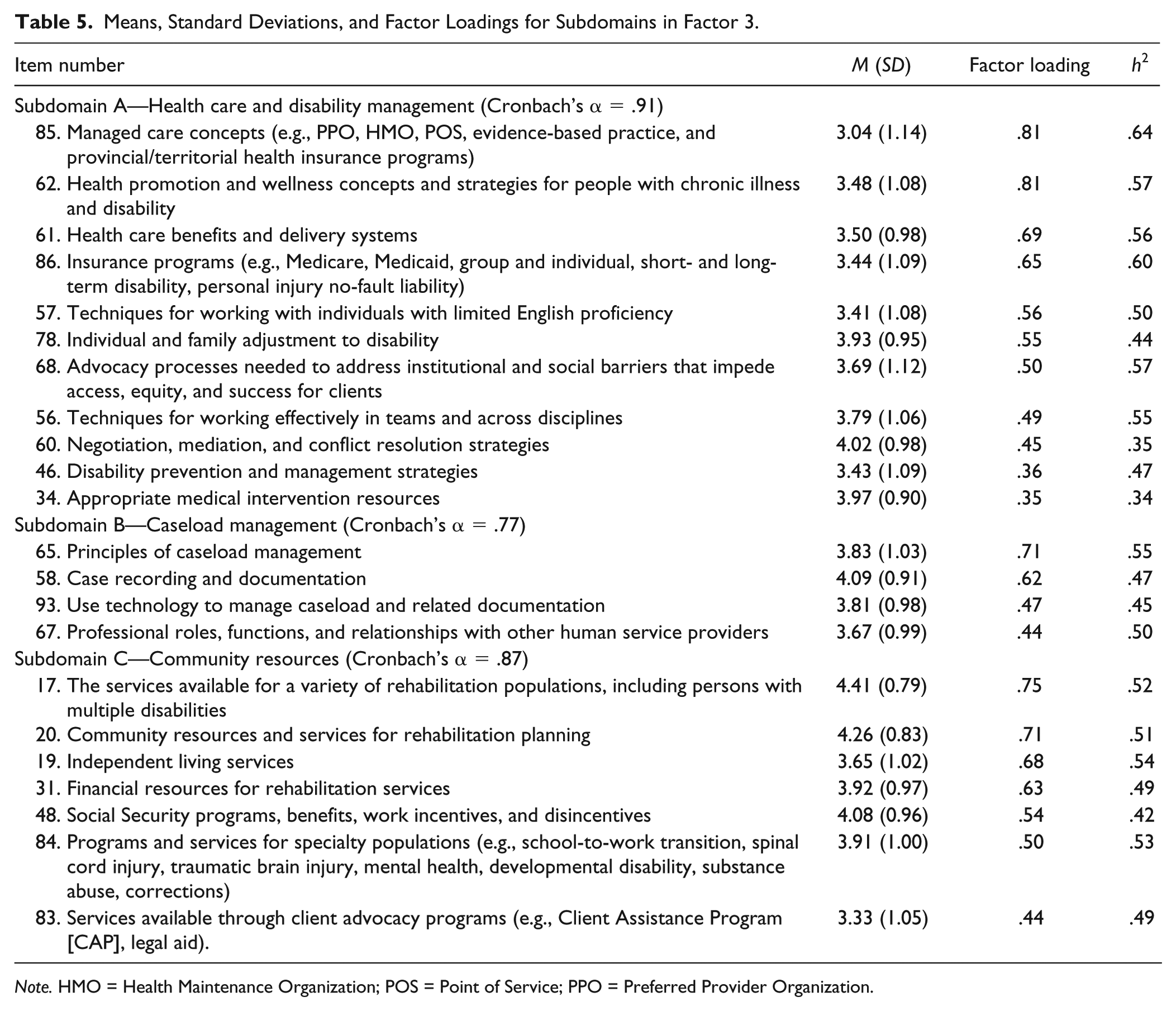
Note. HMO = Health Maintenance Organization; POS = Point of Service; PPO = Preferred Provider Organization.
Factor 1—Rehabilitation and mental health counseling
This factor includes 30 knowledge items that are important to rehabilitation and mental health counseling intervention activities. Subsequent factor analysis of these 30 items revealed the items can be further organized to three subdomains: (a) rehabilitation and mental health counseling theories and techniques, (b) crisis and trauma counseling, and (c) employment counseling. The internal consistency reliability coefficient (Cronbach’s α) for this knowledge domain related to counseling interventions was computed to be .96. The Cronbach’s alpha for the three subdomains were .93, .93, and .80, respectively.
Factor 2—Employer engagement and job placement
This factor consists of 20 knowledge items that are important to employment intervention activities. Subsequent factor analysis of these 20 items revealed the items can be further organized into three subdomains: (a) job placement and job development, (b) occupational analysis, and (c) demand-side employment. Cronbach’s alpha for this knowledge domain related to employment interventions was computed to be .96. The internal consistency reliability coefficients for the three subdomains were .91 .91, and .86, respectively.
Factor 3—Case management
This factor comprises 22 knowledge items that are important to case management–related activities. Subsequent factor analysis of these 22 items revealed the items can be further organized to three subdomains: (a) health care and disability management, (b) caseload management, and (c) community resources. Cronbach’s alpha for this knowledge domain related to case management activities was computed to be .94. The internal consistency reliability coefficients for the three subdomains were .91, .77, and .87, respectively.
Factor 4—Medical and psychosocial aspects of chronic illness and disability
This factor includes 13 knowledge items related to medical and psychosocial aspects of chronic illness and disability. Cronbach’s alpha for this knowledge domain was computed to be .90.
Factor 5—Research methodology and evidence-based practice
This factor comprises nine knowledge items related to rehabilitation research methods and evidence-based practices. Consistent with previous CRC knowledge validation studies, this knowledge domain also included two items related to forensic rehabilitation. One plausible explanation is because forensic rehabilitation practice requires searching research database to evaluate the effectiveness of medical and vocational rehabilitation interventions. Cronbach’s alpha for this knowledge domain was computed to be .90.
Factor 6—Group and family counseling
This factor comprises five knowledge items related to family and group counseling. Cronbach’s alpha for this knowledge domain was computed to be .89.
RQ2: How Important Are These Knowledge Domains for the Professional Practice of Rehabilitation Counseling?
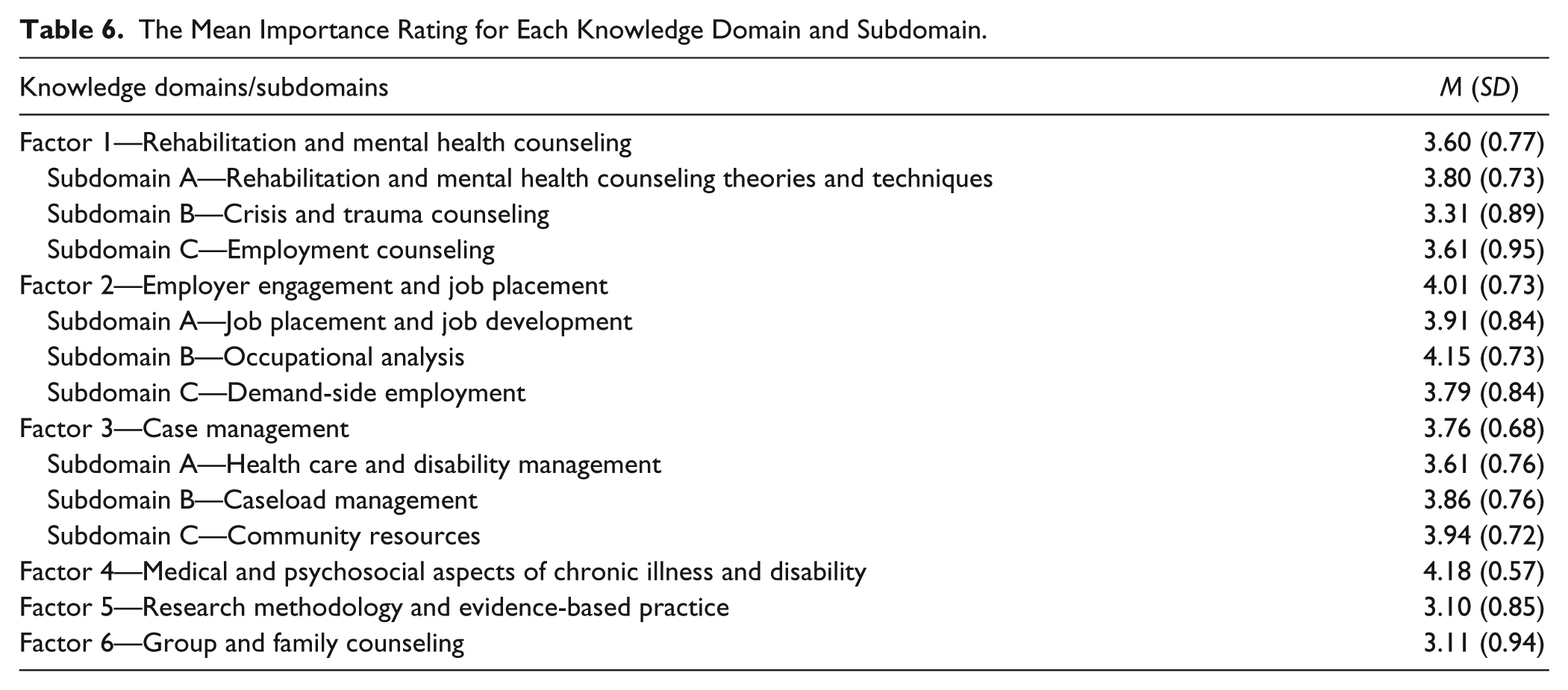
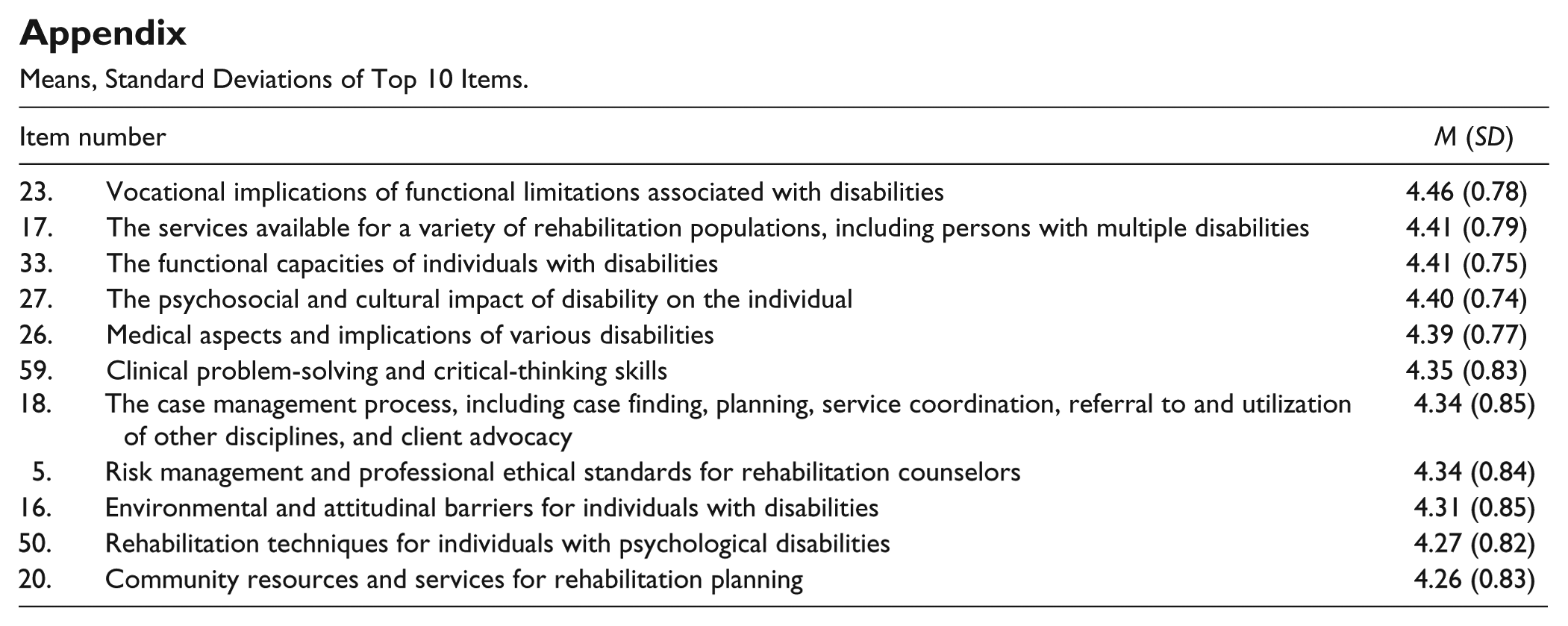
The mean importance rating of each domain is summarized in Table 6. The mean importance rating for rehabilitation and mental health counseling domain was 3.60 (SD = 0.77), 4.01 (SD = 0.73) for employer engagement and job placement domain, 3.76 (SD = 0.68) for case management, 4.18 (SD = 0.57) for medical and psychosocial aspects of chronic illness and disability, 3.10 (SD = 0.85) for research methodology and evidence-based practice, and 3.11 (SD = 0.94) for group and family counseling. “Medical and psychosocial aspects of chronic illness and disability” was the most important knowledge domain as rated by the CRCs who participated in this study. However, the domain of “research methodology and evidence-based practice” as well as “group and family counseling” were rated by CRCs who participated in this study as the least important knowledge domains. See the appendix for means and standard deviations for the top ten rated items.
The Mean Importance Rating for Each Knowledge Domain and Subdomain.
RQ3: Do CRCs From Different Practice Settings Vary in Their Perceptions of the Relative Importance of Knowledge Domains Required for Rehabilitation Counseling Practice?
A MANOVA was computed to test the differences among rehabilitation counselors who worked in different practice settings on the linear combination of the six major rehabilitation counseling knowledge domains. MANOVA revealed a significant multivariate effect, Wilks’ lambda = .71, F(30, 1,226) = 3.61, p < .001, η2 = .069; the partial η2 of .066 indicates that the effect for group differences in our MANOVA accounted for 6.6% of the group differences. A follow-up univariate ANOVA was computed for each dependent variable. The alpha level was divided by six for each pair-wise comparison to control for Type I error (α = .05/6 = .0083). Rehabilitation counselors across employment settings rated case management and psychosocial and medical aspects of chronic illness and disability as similarly important. The ANOVA results indicated CRCs in the six practice settings differed significantly on two of the six knowledge domains: (a) rehabilitation and mental health counseling, F(5, 311) = 3.50, p = .003, η2 = .053, indicating the effect of group differences accounted for 5.3% of the variance in rehabilitation and mental health counseling; and (b) group and family counseling, F(5, 311) = 5.34, p = .001, η2 = .079, indicating the effect of group differences accounted for 7.9% of the variance in group and family counseling.
Post hoc comparisons using the Tukey’s procedure indicated that rehabilitation counselors who work in not-for-profit rehabilitation organizations (M = 3.95, SD = 0.66) and school and university settings (M = 3.76, SD = 0.73) rated rehabilitation and mental health counseling knowledge as more important than practitioners who work in proprietary rehabilitation settings (M = 3.33, SD = 0.82). Practitioners who work in school and university settings (M = 3.58, SD = 0.85) also rated group and family counseling knowledge as more important than practitioners in public vocational rehabilitation agencies (M = 2.91, SD = 0.96) and proprietary rehabilitation settings (M = 2.90, SD = 0.96).
RQ4: Do CRCs With the LPC Credential Vary in Their Perceptions of the Relative Importance of Knowledge Domains Required for Rehabilitation Counseling Practice Compared With CRCs Without Counsel or Licensure?
Hotelling’s T2 was used to analyze the data to answer this research question. Hotelling’s T2 test revealed a significant multivariate effect, Hotelling’s T2 = .055, F(6, 310) = 2.85, p < .05, η2 = .052; the partial η2 of .052 indicates that the effect for group differences accounted for 5.2% of the group differences. A follow-up univariate t test was computed for each dependent variable. The results indicated significant differences on one of the six knowledge domains related to rehabilitation counseling practice. CRCs with the LPC credential rated group and family counseling as significantly more important (M = 3.35, SD = 0.91) than CRCs without counselor licensure (M = 3.02, SD = 0.94).
Discussion
The results of this study provide a new empirical evidence of the knowledge base underlying the professional practice of rehabilitation counseling for CRCs across all clinical practice settings. These findings are intended for use by the CRCC to examine and develop the new test and item specifications for future versions of the CRCE.
The sample randomly drawn from the CRCC database for the KVI-R study was carefully constructed to ensure that the sample was reflective of the overall CRC population characteristics (N = 16,259). This was especially important because we anticipated that we would achieve a response rate, based on other studies using an electronic survey platform (e.g., Leahy et al., 2013; Phillips & Leahy, 2012), of somewhere around 20%. As can be observed, the response rate for the KVI-R study was 21.8%. The research sample was clearly similar to the current overall population demographics for CRCs.
In the process of conducting this study, the KVI-R was revised to include content that reflects new knowledge requirements for rehabilitation counselors in today’s complex human service delivery environments. These newer areas were developed based on expert opinion of the Delphi panelists (subject matter experts) and a review of contemporary literature in these areas. As a result of the Delphi study, we were able to confirm and validate the items in KVI-R and modify and revise a number of the items based on panelist recommendations, eliminate any dated or redundant items, and create new items based on their recommendations of what appeared missing in the instrument.
These results also provide further validation of the importance of those more traditional knowledge areas (e.g., job development and job placement, personal and group counseling, and case management) associated with the role of the rehabilitation counselors that have been empirically described in previous studies (e.g., Leahy, Chan, & Saunders, 2003; Leahy, Muenzen, Saunders, & Strauser, 2009; Leahy, Szymanski, & Linkowski, 1993; Rubin et al., 1984). The results of this study differ somewhat in organizational structure from the current knowledge domain solution (Leahy et al., 2013) that CRCC uses to guide the test specifications for the CRCE. These differences, however, are primarily related to a greater degree parsimony achieved in the overall description and additional depth and range within each of the knowledge domains that were identified.
An analysis on the impact of employment settings on the perceived importance of knowledge domains was also performed. The results of this analysis provided additional evidence that the instruments performed as one would have anticipated in relation to clinical setting differences. The results, for the most part, are also very consistent with previous research (Leahy et al., 2003; Leahy et al., 2013; Leahy et al., 2009; Leahy et al., 1993) related to differences in relation to the practice setting of respondents. Although differences exist in importance level of a few knowledge domains (e.g., rehabilitation and mental health counseling and group and family counseling), there is significant agreement about the commonality of the knowledge domains across employment settings (e.g., case management, and medical and psychosocial aspects of chronic illness and disability), which further supports the use of these findings in setting the new test specifications.
One of the research questions asked whether CRCs with counselor licensure (LPC) varied in their perceptions of the relative importance of different rehabilitation counseling knowledge areas required for rehabilitation counseling practice compared with CRCs without counselor licensure. The analysis of the data for this question indicated that there was only one statistically significant difference in relation to knowledge importance (group and family counseling), indicating that these two subgroups are highly similar.
Over the years, empirical findings on the role, function, and knowledge requirements were systematically utilized by the CORE to assist in establishing their curriculum standards for academic program accreditation in rehabilitation counseling at the master’s degree level. As indicated earlier in the article, with the merger of CORE and CACREP and the emergence of rehabilitation counseling among the specialty areas now accredited by CACREP, it is highly recommended that these studies continue to be used to provide empirically validated knowledge requirements in the specialty standards for rehabilitation counseling within CACREP accreditation process.
Mapping the Blueprint of the New CRCE Test Specifications From the Empirical Findings
The findings from the final version of the KVI-R that identified the knowledge domains and subdomains, along with individual knowledge areas were selected as the primary data to establish the new organizational structure, and map out the new blueprint, of test specifications for the CRCE. In terms of organizational schema, the CRCC Standards and Examination Committee (the Committee) and the research team decided to use the new structure from the KVI-R for the knowledge domains. They also decided that the knowledge items would be organized under a combination of factors and subdomains (as was done in 2013) to increase the homogeneity of the individual knowledge areas included, and to improve the interpretability of the blueprint of test specifications.
For the most part, the original structure of the KVI-R findings reported earlier in this article was used in the design of the new CRCE test specifications. The Committee reviewed each of the factors from the study and decided to utilize a 12-domain structure of the specifications. In addition, during this part of the review, some of the knowledge domains were relabeled to better reflect domain content. The Committee also carefully examined each of the knowledge items within the 12 domains. Two items were subsequently eliminated from the blueprint as a result of low mean importance ratings and 13 items were added to the blueprint. These additional items were originally part of the KVI-R but did not load high enough (<.35) on any of the factors to be included in the final structure. These items were also rated relatively high in terms of importance ratings (>3.0), and the Committee felt they should be included in the blueprint. It should also be noted that four of these items were excluded during this part of the analysis as a result of redundancy of content. Finally, there were a number of knowledge items that were moved by Committee consensus to alternative domains within the structure to better reflect homogeneity of content within domains and improve interpretability of the blueprint. As part of this process, four additional items were removed from the specification due to the specificity of population and practice setting. It was also believed that the content of these more specific items was already reflected in the specifications. Once these changes were made, the research team and the Committee agreed that each of the knowledge domains and subdomain items attained a level of empirical importance sufficient to be included in the test specifications for future versions of the CRCE. See Table 7 for the final layout of the final test specifications, including the percentage of items selected for each examination in each knowledge domain. Finally, the Committee voted to approve these specifications for future examinations. The new test specifications were then presented to the CRCC Board that approved and adopted the new examination structure for implementation in October 2017.
Test Specification for the CRC Examination.
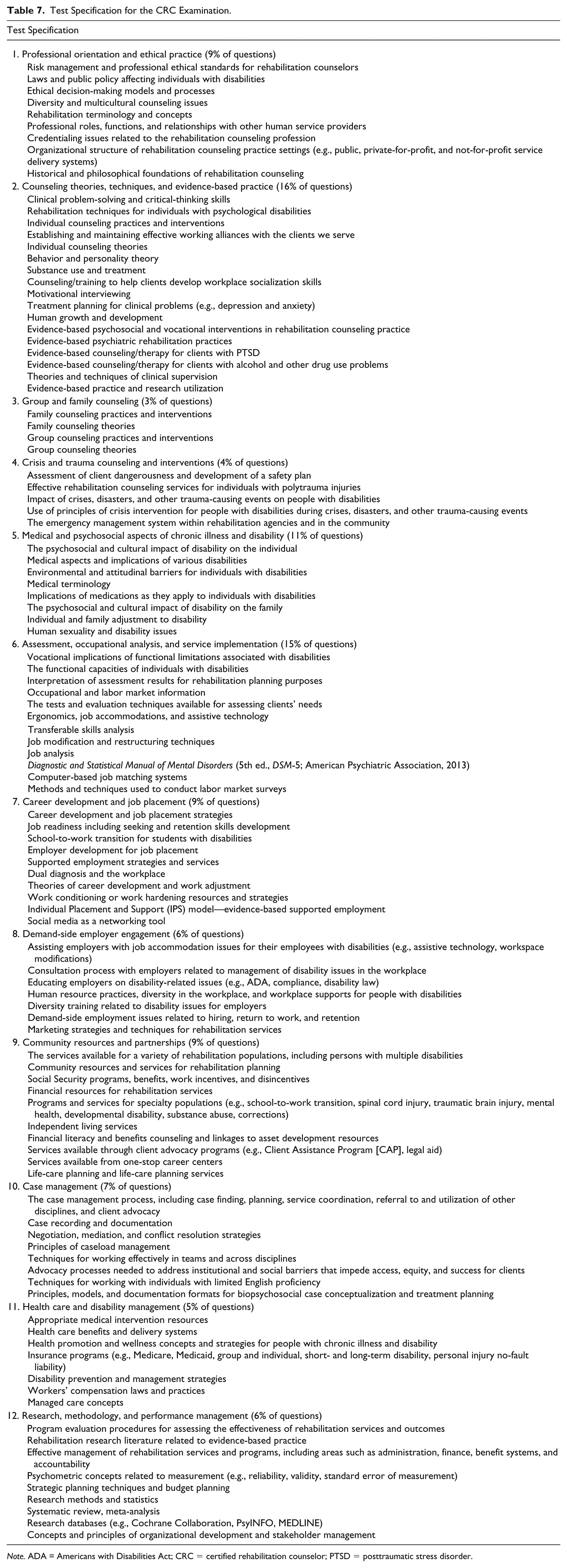
Note. ADA = Americans with Disabilities Act; CRC = certified rehabilitation counselor; PTSD = posttraumatic stress disorder.
Limitations
The findings from this study should be viewed and applied within the context of several limitations. Although random selection of participants strengthened the generalizability of these findings, only individuals who were currently credentialed by CRCC were selected for the sample, and no further information was available related to how effective these practitioners were in relation to practice other than certification/licensure status. In addition, about one third of the participants worked in state Vocational Rehabilitation (VR) agency settings and less than 10% worked for community-based rehabilitation organizations. The overrepresentation of state VR counselors may affect the generalizability of the results. Although the response rate would be viewed as generally acceptable in relation to these types of survey research applications, a limitation is nevertheless noted. Another classic limitation imposed by the research methods employed in this study relates to the reliance on self-report in assessing the importance of various knowledge domains associated with effective practice. Finally, another limitation of the study is noted in relation to the time between data collection and article preparation, which was the result of the time required to analyze the data, prepare a final report, and have the CRCC Standards and Examination Committee examine the findings to officially set and approve the new test specifications for the CRCC examination.
Conclusion
The results of this study provide empirical support for the description of the knowledge base underlying the professional practice of rehabilitation counseling, and contribute further empirical evidence in relation to the content and construct validity of the knowledge domains identified in this replication and extension of the most recent study completed in 2012 (Leahy et al., 2013). The focus of this study was to identify and examine the major knowledge domains required for effective rehabilitation counseling practice to revise and update the test specifications for the CRCE. These findings can also be used to empirically validate the specialty standards for rehabilitation counseling within the current CACREP accreditation requirements.
Over the past 25 years, including the present study, there have been five, large-scale national research initiatives (Leahy et al., 2003; Leahy et al., 2013; Leahy et al., 2009; Leahy et al., 1993) that have identified and defined the specific competencies important to the professional practice of rehabilitation counseling and the achievement of positive outcomes with the consumers they serve. These last five national studies have sampled the same population of interest and used parallel definitions of variables, research questions, and research instruments. Each successive replication and extension of this line of inquiry has added to the evidence-based (DePalma, 2002) foundation of underlying knowledge dimensions essential for rehabilitation counseling practice. These studies and prior research have provided the discipline with consistent empirically based evidence of an established and mature discipline that is able to respond appropriately to the evolutionary demands and pressures of a dynamic human service field.
Footnotes
Appendix
Means, Standard Deviations of Top 10 Items.
| Item number | M (SD) | |
|---|---|---|
| 23. | Vocational implications of functional limitations associated with disabilities | 4.46 (0.78) |
| 17. | The services available for a variety of rehabilitation populations, including persons with multiple disabilities | 4.41 (0.79) |
| 33. | The functional capacities of individuals with disabilities | 4.41 (0.75) |
| 27. | The psychosocial and cultural impact of disability on the individual | 4.40 (0.74) |
| 26. | Medical aspects and implications of various disabilities | 4.39 (0.77) |
| 59. | Clinical problem-solving and critical-thinking skills | 4.35 (0.83) |
| 18. | The case management process, including case finding, planning, service coordination, referral to and utilization of other disciplines, and client advocacy | 4.34 (0.85) |
| 5. | Risk management and professional ethical standards for rehabilitation counselors | 4.34 (0.84) |
| 16. | Environmental and attitudinal barriers for individuals with disabilities | 4.31 (0.85) |
| 50. | Rehabilitation techniques for individuals with psychological disabilities | 4.27 (0.82) |
| 20. | Community resources and services for rehabilitation planning | 4.26 (0.83) |
Acknowledgements
The authors extend their great appreciation to Ms. Cindy Chapman, CEO of Commission on Rehabilitation Counselor Certification (CRCC), for her exceptional assistance and financial support in carrying out this study. They would also like to thank all the members of the CRCC Examination and Research Committee for their help and support. This research was also supported in part by funding from the Council on Rehabilitation Education (CORE), which merged with the Council for Accreditation of Counseling and Related Educational Programs (CACREP) effective July 1, 2017.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was commissioned and funded by the Commission on Rehabilitation Counselor Certification (CRCC).