
Abstract
This study aimed to analyze factors associated with resilience among persons with spinal cord injury (SCI). An integrative review was conducted. Electronic databases including PubMed, ProQuest, Cumulative Index of Nursing and Allied Health Literature, and Web of Science were searched using relevant search terms and keywords. A total of two qualitative and nine quantitative studies were included in the review. Psychosocial factors such as social support, self-efficacy, spirituality, post-traumatic growth, life satisfaction, adaptive coping strategies, psychological strength, and being a role model were associated with higher resilience. Stress, anxiety, depression, external locus of control, and attachment avoidance correlated with lower resilience. Inconsistent results were reported for demographic and injury-related variables such as the age of the participants, gender, pain, and functional independence. The integrative review reported a number of factors associated with resilience in people with SCI. Rehabilitation counselors working with this population can design rehabilitation interventions targeting these variables to enhance the resilience of people with SCI. Consideration of cultural and contextual influences on resilience, as well as the design of effective interventions, are important directions for future research.
Spinal cord injury (SCI) is a chronic neurological condition that affects approximately 250,000 to 500,000 people around the world every year (World Health Organization [WHO], 2013). SCI is a life-altering disability that profoundly impacts the physical, psychological, social, and financial aspects of a person’s life (Crew & Krause, 2009). In addition, SCI can result in long-term physical (e.g., immobility, spasticity, chronic pain, pressure ulcers), and psychosocial issues. Psychosocial problems, such as depression, anxiety, post-traumatic stress disorder, social withdrawal, divorce, and unemployment are prevalent among persons with SCI, and further affect their well-being and rehabilitation outcomes (Craig & Perry, 2014). Because SCI can impact multiple aspects of an individual’s life, adaptation to SCI poses a significant challenge and requires abundant psychosocial resources (Martz et al., 2005). Despite the negative consequences of SCI, previous studies have reported that some persons with SCI are resilient enough to experience positive adjustment and high quality of life (Bonanno et al., 2012; Guest, Craig, Tran, & Middleton, 2015; Kilic et al., 2013). Understanding factors that affect resilience can help in the development of rehabilitation interventions that can positively impact the quality of life in persons with SCI.
Resilience in SCI
Resilience is a psychological construct within the positive psychology research paradigm that emphasizes the strengths or positive characteristics of a person (Seligman & Csikszentmihalyi, 2000). Resilience is defined as the personal ability to cope with adversity (Connor & Davidson, 2003), or the process of adapting well while confronting adversities or stressful events (American Psychological Association, 2010). Richardson (2002) states that a person’s reaction to a stressful event is determined by his or her level of resilience. Following an event, the person may undergo four different paths as follows: (a) resilient integration characterized by finding new interests and meaning in life; (b) reintegration to homeostasis (balance in life; c) reintegration with loss (e.g., unemployment or social isolation); or (d) dysfunctional reintegration characterized by depression or low quality of life. A longitudinal study found that 68% and 66% of participants with SCI reported high resilience at discharge and after 6 months of living in the community, respectively. Other participants demonstrated low resilience, which is likely to interfere with successful integration into the community (Guest, Craig, Tran, & Middleton, 2015).
The current literature suggests that higher resilience among persons with SCI is associated with adaptive adjustment, effective coping, and better quality of life (Bonanno et al., 2012; Tansey et al., 2017). Resilience appears to mitigate the negative effects of pain on adaptation outcomes and to buffer the occurrence of depressive symptoms among persons with SCI (Bonanno et al., 2012; Min et al., 2014). On the contrary, low resilience is likely to result in poor adjustment, behavioral disengagement, and psychological distress, including depression (Bonanno et al., 2012; Kilic et al., 2013). A resilient individual possesses a strong sense of self-efficacy, perceived social support, and stable mood which can help them to adapt successfully despite the disability-related consequences of SCI (Guest, Craig, Tran, & Middleton, 2015; Kilic et al., 2013). Resilience has a vital role in achieving adjustment following SCI (Kornhaber et al., 2017). Overall, the current evidence suggests that persons with SCI who have greater resilience overcome adversity more successfully than those who have lower resilience (Guest, Craig, Tran, & Middleton, 2015; Tansey et al., 2017; White et al., 2010).
Research on Factors Associated With Resilience in SCI
The literature shows that resilience in people with SCI is influenced by multiple psychosocial, demographics, and injury-related variables (Bhattarai et al., 2018; Bonanno et al., 2012; Guest, Craig, Tran, & Middleton, 2015; Kilic et al., 2013). Kumpfer (1999) stresses that resilience results from the interaction of personal, environmental, and situational factors. Richardson (2002) pointed out that a person can be moved from dysfunctional reintegration to resilient integration with appropriate interventions. Consideration of factors related to resilience is essential while planning or designing interventions in rehabilitation settings. To date, a few systematic reviews have been conducted which examine personal psychological factors that influence the quality of life and adjustment in persons with SCI (e.g., Peter et al., 2012; van Leeuwen et al., 2012). Several outcomes have been analyzed in terms of adjustment to SCI, such as quality of life, life satisfaction, well-being, physical health, mental health, activity and participation, anxiety, depression, post-traumatic stress, and emotional distress (Peter et al., 2012; van Leeuwen et al., 2012). However, none have investigated resilience as an outcome.
Although resilience has not yet been systematically reviewed as a measurement outcome in persons with SCI, a systematic review was conducted to explore factors related to resilience among people with chronic physical illnesses (Stewart & Yuen, 2011). The review included 52 studies that were carried out among people with cardiovascular diseases, stroke, HIV/AIDS, diabetes, cancers, rheumatoid arthritis, hip fracture, and multiple sclerosis. The outcomes in the review were resilience and related constructs such as hardiness, benefit-finding, positive adaptation, and positive behavior. Psychosocial factors including self-efficacy, self-esteem, internal locus of control, optimism, mastery, hope, self-empowerment, social support, spirituality, and active coping were found to be associated with resilience (Stewart & Yuen, 2011). SCI is a chronic disability that can have a substantial impact similar to some other chronic illnesses such as dementia, multiple sclerosis, cerebral palsy, and diabetes (WHO, 2013), and as such factors of resilience are important to explore in SCI as well.
The understanding of factors contributing to resilience will help rehabilitation researchers and practitioners to develop effective rehabilitation programs to enhance resilience in persons with SCI. Improving overall well-being by utilizing one’s resources, including resilience, is one of the major goals of rehabilitation services. As rehabilitation counselors have a central role in the rehabilitation process of persons with SCI, their understanding of how they can support their clients in developing and strengthening resilience is fundamental. Although people with SCI may not recover from their physical condition (e.g., paralysis), assisting them to enhance resilience may enable those individuals to achieve optimum functioning.
Therefore, the present review was conducted to analyze the available evidence regarding demographic, injury-related, and psychosocial factors that are associated with resilience in persons who have sustained a SCI. The review question addressed in the present analysis is: What demographic, injury-related, and psychosocial factors are associated with resilience in persons with SCI? A summary of current findings on factors can provide a basis for a better understanding of how persons with SCI can effectively adjust to the negative consequences of SCI.
Method
An integrative review was undertaken, as this approach allows for the combination of diverse methodologies to provide a comprehensive understanding of a particular phenomenon (Whittemore & Knafl, 2005). The stages of the integrative review include problem identification, literature search, data evaluation, data analysis, and presentation/results (Whittemore & Knafl, 2005).
Problem Identification
The review question was formulated using the PICO abbreviation (Joanna Briggs Institute, 2014), where P (population) = persons with SCI, I (exposure of interest) = factors influencing resilience, C (context) = rehabilitation center or community setting, and O (outcome) = level of resilience. PICO is a format that helps to structure the research question in terms of a specific population’s problem and aids in finding clinically relevant evidence in the literature. This helps the researcher to formulate the search strategies by identifying the key concepts that need to be in the identified articles.
Literature Search
In December 2018, a comprehensive and systematic search was conducted in the following electronic databases: PubMed, ProQuest, Cumulative Index of Nursing and Allied Health Literature (CINAHL), and Web of Science. The search terms and keywords were formulated according to PICO. The keywords used to search population were “spinal cord injury,” “SCI,” “paraplegia,” and “quadriplegia.” The keywords for factors included “indicators,” “factors,” “determinants,” “predictors,” and “correlates,” and the keywords for outcomes included “resilience” and “resiliency.” Boolean connectors AND, OR, and NOT were used to combine search terms. Each resulting factor (e.g., social support, self-efficacy, stable mood, spirituality) was also searched together with the key terms of resilience and SCI.
Inclusion and exclusion criteria
Both qualitative and quantitative studies that examined factors of resilience among adults with SCI living in a rehabilitation center, community setting, or both were included in the review. The review was limited to empirical research published in the English language between 2007 and 2018 in scientific journals. Case studies, reviews, or studies conducted in children or other populations were excluded. Studies that measured the adjustment process or quality of life rather than resilience as the major outcome were not included in the review.
Data Evaluation
The titles and abstracts of the studies that came up in the database searches were screened and the relevant studies were retrieved to evaluate in detail. The references of the selected articles were further examined to identify more relevant articles for inclusion. As an integrative review includes diverse empirical and theoretical sources or research designs, evaluating and interpreting the quality of studies is complex. Therefore, quality appraisal of selected studies may not be considered as essential in the integrative review (Whittemore & Knafl, 2005). In this review, all studies that met the inclusion criteria, regardless of methodological quality, were included in an effort to glean all evidence related to factors of resilience in this population.
Data Analysis
From each qualifying study, information related to authors, published year, country, sample size, setting, study design, and associated factors or determinants were extracted and traced into matrix-evidence tables. Then, the findings were synthesized and summarized. Factors of resilience were identified based on results from correlation and regression analyses. Therefore, outcomes from correlation and regression analyses demonstrate the association between resilience and related factors (see Table 3). A p value of less than .05 was considered to be a statistically significant association.
Results
The search strategy revealed a total of 291 studies (see Figure 1). After removing duplicates and irrelevant studies, a total of 11 studies were included for the final review. Of the 11, nine were quantitative studies and two were qualitative phenomenology studies.

Search process and search result.
Characteristics of the Selected Studies
All of the studies were conducted in developed countries, including Australia (Guest, Craig, Nicholson Perry, et al., 2015; Guest, Craig, Tran, & Middleton, 2015; Kilic et al., 2013), the United States (Dodd et al., 2015; Driver et al., 2015; Machida et al., 2013; Monden et al., 2014; White et al., 2010), Canada (Catalano et al., 2011), and South Korea (Min et al., 2014), with the exception of one study conducted among people with earthquake-related SCI in Nepal (Bhattarai et al., 2018). The studies were carried out in community settings, rehabilitation centers, or both. All quantitative studies used bivariate or multivariate statistical analyses. Sample sizes ranged from 12 to 28 in the qualitative studies and 37 to 255 in the quantitative studies. Of the nine quantitative studies, five were descriptive cross-sectional in design. All of the studies used convenience sampling techniques to recruit participants. The characteristics of these studies are presented in Table 1.
Characteristics of the Selected Studies.

The nine quantitative studies analyzed for this review were homogeneous in terms of the measurement of resilience. All of these studies used the Connor-Davidson Resilience Scale (CD-RISC), either the 25-item original version (Bhattarai et al., 2018; Catalano et al., 2011; Guest, Craig, Nicholson Perry, et al., 2015; Guest, Craig, Tran, & Middleton, 2015; Min et al., 2014; White et al., 2010) or the 10-item short version (Dodd et al., 2015; Driver et al., 2015; Kilic et al., 2013). The instruments that were used to measure resilience and resilience factors identified in the selected studies are presented in Table 2. From the review of the 11 studies, a total of 26 independent variables were identified which can be considered as factors of resilience based on the resilience literature. Factors identified from the review were grouped into two primary categories: psychosocial factors and demographic and injury-related factors, as most of the reviewed studies categorized and investigated factors in terms of these two groups. The factors that showed significant associations with resilience are presented in Table 3.
Measurement Instruments of Resilience and Factors in the Selected Studies.
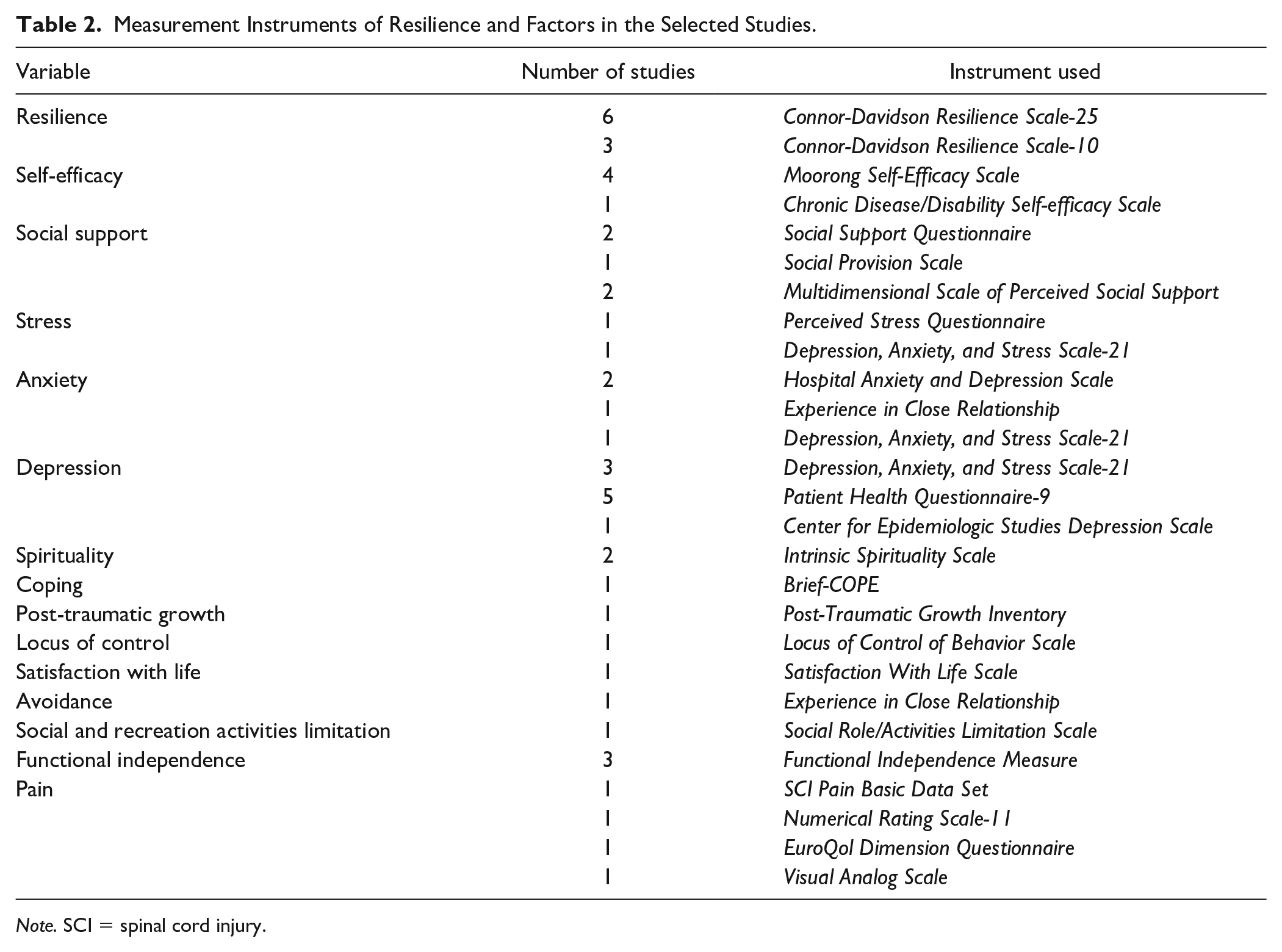
Note. SCI = spinal cord injury.
Factors and Their Associations With Resilience in Persons With Spinal Cord Injury.

Note. *p < .05; **p < .01.
Psychosocial Factors
Self-efficacy
Overall, five studies examined the effect of self-efficacy on resilience. Bandura (1986) defines self-efficacy as people’s judgments of their capabilities to organize and execute courses of action required to attain designated types of performance. Self-efficacy in the studies was referred to as confidence in performing functional, social, leisure, and vocation activities following SCI (Guest, Craig, Tran, & Middleton, 2015; Kilic et al., 2013). The relationship between self-efficacy and resilience was found to be statistically significant in all of the studies with effect sizes (r) ranging from .50 to .68. A higher self-efficacy was associated with higher resilience in persons with SCI (Bhattarai et al., 2018; Driver et al., 2015; Guest, Craig, Nicholson Perry, et al., 2015; Guest, Craig, Tran, & Middleton, 2015; Kilic et al., 2013).
Social support
Perceived social support from family, friends, or significant others was found to be consistently associated with resilience in people with SCI in five studies. Persons with SCI with higher social support were likely to be highly resilient, and those with low social support appeared to have lower resilience scores (Bhattarai et al., 2018; Catalano et al., 2011; Dodd et al., 2015; Guest, Craig, Nicholson Perry, et al., 2015; Guest, Craig, Tran, & Middleton, 2015). Similarly, in qualitative studies, participants reported that social support received from family, friends, caregivers, rehabilitation staff, and peer mentors helped to enhance their resilience (Machida et al., 2013; Monden et al., 2014).
Stress, anxiety, and depression
Two studies found a strong negative correlation between stress and resilience (Catalano et al., 2011; Kilic et al., 2013). Similarly, four studies reported a significant negative association between resilience and anxiety (Dodd et al., 2015; Guest, Craig, Nicholson Perry, et al., 2015; Guest, Craig, Tran, & Middleton, 2015; Kilic et al., 2013). Also, eight studies assessed the relationship between resilience and depression and reported a significant negative association between these two variables (Bhattarai et al., 2018; Catalano et al., 2011; Dodd et al., 2015; Guest, Craig, Nicholson Perry, et al., 2015; Guest, Craig, Tran, & Middleton, 2015; Kilic et al., 2013; Min et al., 2014; White et al., 2010). The studies noted that persons with SCI who had high stress, anxiety, and depressive symptoms tended to report lower resilience.
Spirituality
Spirituality, faith, or making meaning in a stressful situation emerged as a positive factor related to resilience in one quantitative study (White et al., 2010) and one qualitative study (Monden et al., 2014). Spirituality in the quantitative study was defined as one’s relationship to God or whatever she or he perceives to be a higher power or transcendence (Bhattarai et al., 2018; White et al., 2010). A higher spirituality in persons with SCI was found to be related to higher resilience (White et al., 2010). In the qualitative study, participants reported that their spirituality or faith had a positive influence on their ability to cope (Monden et al., 2014). However, a study conducted among people with earthquake-related SCI reported a nonsignificant relationship between spirituality and resilience (Bhattarai et al., 2018).
Coping strategies
One quantitative and two qualitative studies examined and reported a positive relationship between problem-focused, adaptive coping strategies, and resilience among persons with SCI (Catalano et al., 2011; Machida et al., 2013; Monden et al., 2014). Coping was operationalized as cognitive and behavioral strategies used by persons with SCI to manage the demands of life (Catalano et al., 2011). In one qualitative study, participants indicated that adaptive coping strategies such as having a sense of humor, setting a goal, seeking education, listening to music, and journaling contributed to their ability to adapt (Monden et al., 2014). Similarly, Machida et al. (2013) reported that behavioral and cognitive strategies were helpful in increasing resilience among persons with SCI.
Miscellaneous factors
Besides the aforementioned factors, a few studies reported other factors associated with resilience. Post-traumatic growth, or positive changes that occurred after experiencing a traumatic event, was positively associated with resilience (Min et al., 2014). A strong negative association was found between resilience and external locus of control, in that persons who believe that they are not responsible for their behavior or do not have control over their life tended to report lower resilience (Kilic et al., 2013). Life satisfaction was significantly associated with resilience, reflecting that persons with SCI who were satisfied with their life experience were likely to obtain higher scores in resilience (White et al., 2010). Furthermore, an avoidant attachment style, which means discomfort with closeness and depending on others, was negatively correlated with resilience (Dodd et al., 2015). Also, one qualitative study identified psychological strength, perspective, and being a role model as positive contributors to resilience (Monden et al., 2014).
Demographic and Injury-Related Factors
Age of the participants
There were inconsistent results regarding the correlation between age of participants and resilience. In one out of five studies, older age was significantly associated with higher resilience (Driver et al., 2015); however, a nonsignificant association was identified in the other studies (Bhattarai et al., 2018; Dodd et al., 2015; Guest, Craig, Nicholson Perry, et al., 2015; Min et al., 2014).
Pain
A significant negative correlation was found between pain and resilience in three studies (Driver et al., 2015; Guest, Craig, Tran, & Middleton, 2015; Min et al., 2014). However, a nonsignificant association between pain and resilience was found in one study (Kilic et al., 2013).
Functional independence
Three studies examined the relationship between functional independence and resilience (Driver et al., 2015; Guest, Craig, Tran, & Middletone, 2015; White et al., 2010). Functional independence was conceptualized as the ability of a person with SCI to independently perform activities in four areas: (a) self-care; (b) bladder and sphincter control; (c) mobility; and (d) locomotion. Only one study found a significant association between functional independence and resilience, with results reflecting higher resilience in persons with SCI who were less dependent or more independent in performing those activities (Guest, Craig, Tran, & Middletone, 2015).
Employment
Three studies examined the association between resilience and employment status (Bhattarai et al., 2018; Driver et al., 2015; Min et al., 2014). Of the three, two studies found a significant positive correlation between resilience and employment (Bhattarai et al., 2018; Min et al., 2014).
Miscellaneous factors
Some of the reviewed studies also examined other demographic and injury-related factors (Bhattarai et al., 2018; Driver et al., 2015; Guest, Craig, Nicholson Perry, et al., 2015; Kilic et al., 2013; Min et al., 2014). Only the study conducted in Nepal demonstrated a gender-related effect, with higher resilience in males than in females with SCI (Bhattarai et al., 2018). In addition, that study also reported the influence of current living location on the resilience of individuals with SCI, with those who were living in urban areas reporting higher resilience than those living in rural areas. A nonsignificant association was found between resilience and marital status, educational status (Guest, Craig, Nicholson Perry, et al., 2015), secondary complications, length of stay at a rehabilitation center (Driver et al., 2015), time since injury (Kilic et al., 2013; Min et al., 2014), level of injury, completeness of injury (Guest, Craig, Nicholson Perry, et al., 2015; Kilic et al., 2013), and social and recreational activities (Driver et al., 2015).
Discussion
The purpose of this review was to examine the existing evidence related to factors associated with resilience in persons with SCI. The empirical studies reviewed suggested that resilience is an attribute that can be enhanced or diminished. Those who have high resilience are generally more able to cope with the negative consequences of SCI and have a good quality of life (Driver et al., 2015; Kilic et al., 2013; Tansey et al., 2017). Numerous factors associated with resilience in persons with SCI were identified in this review. Most of these factors are consistent with factors that were previously explored in a systematic review of studies related to chronic physical illnesses (Stewart & Yuen, 2011). The present review revealed some consistent and inconsistent factors related to the resilience of people with SCI.
Self-efficacy and social support were found to be the most consistent factors associated with resilience. A sense of self-confidence to perform a particular behavior is likely to enhance resilience (Guest, Craig, Tran, & Middleton, 2015; Kilic et al., 2013). Similarly, perceived support from family, friends, or others helps an individual to change negative thoughts and seek resources to manage stress (Catalano et al., 2011; Guest, Craig, Tran, & Middleton, 2015). The incongruent findings related to spirituality in one study could be due to the different context in which the study was conducted. The study was conducted in a developing Asian country and included participants who faced dual traumatic events: earthquake and SCI. The authors argued that the traumatic events could lead to an alteration in participants’ spiritual beliefs and that the dynamic nature of spirituality is difficult to capture in a cross-sectional study (Bhattarai et al., 2018).
Depression or depressive symptoms were found to be associated with lower resilience among people with SCI in almost all of the reviewed studies (Bhattarai et al., 2018; Catalano et al., 2011; Dodd et al., 2015; Guest, Craig, Nicholson Perry, et al., 2015; Guest, Craig, Tran, & Middleton, 2015; Kilic et al., 2013; Min et al., 2014; White et al., 2010). Immediate and long-term consequences of SCI such as immobility, functional limitations, dependency, chronic pain, unemployment, and other medical complications could result in depression. Furthermore, depression is likely to reduce self-efficacy to manage daily life stressors and seek social support. Therefore, people with SCI who have depression or depressive symptoms are likely to experience lower resilience (Bhattarai et al., 2018).
There were inconclusive findings regarding the contribution of demographic and injury-related factors to resilience. Age of participants, gender, pain, and functional independence were inconsistent determinants of resilience. The discrepancies in the findings could be attributed to different reasons such as study setting, cultural differences, measures of constructs, characteristics of samples, sample size, and operational definitions of some variables. For example, Kilic et al. (2013) measured neuropathic pain using a 10-point scale, and Driver et al. (2015) measured overall pain (could be either neuropathic or musculoskeletal pain) using a 10-point scale. However, Min et al. (2014) used a 3-point scale to measure pain. In terms of characteristics of participants, some studies included only people with traumatic SCI (Driver et al., 2015), whereas others included people with traumatic as well as nontraumatic SCI (Kilic et al., 2013; Min et al., 2014). In a study conducted by Kilic et al. (2013), 98% of the participants were Caucasian, whereas other studies included different ethnic groups.
With regard to gender, the study conducted in Nepal, a developing Asian country, found that male participants were likely to have higher resilience scores than female participants. The authors argued that the cultural context of the country could have resulted in this discrepancy. In a patriarchal society, males, even those with a disability, are considered to be authority figures; whereas, females are considered to be subordinates. Males are also more likely to obtain higher levels of education and employment as compared with females. Consequently, males in these contexts may have higher self-esteem or confidence which could contribute to greater resilience. A study conducted in India also supported the finding that males with SCI were more resilient than their female counterparts (Ahum et al., 2016). Bhattarai et al. (2018) also found that the people living in rural areas with inaccessible health care, rehabilitation services, and transportation facilities reported lower resilience scores than those living in urban areas.
A number of design strengths and weaknesses were identified. All of the studies were similar in terms of the measurement outcome and measurement tool for resilience. Some of the studies included an adequate sample size (Catalano et al., 2011; Dodd et al., 2015; Monden et al., 2014) and longitudinal design (Driver et al., 2015; Guest, Craig, Tran, & Middleton, 2015; White et al., 2010). However, weaknesses such as small sample sizes (Driver et al., 2015; Min et al., 2014; White et al., 2010), lack of clear inclusion/exclusion criteria (Monden et al., 2014), and inclusion of only male participants (Machida et al., 2013) were noted in some studies. Furthermore, participants were recruited using convenience sampling techniques in all of the studies.
Limitations and Future Research
The current review extends the knowledge of factors related to resilience in person with SCI. However, some limitations to this review suggest areas for future research. First, the generalizability of the findings should be considered. The review included only recent studies published between 2007 and 2018; therefore, the review might have missed some factors investigated in earlier research. In addition, only studies published in English were included in the review, which might have resulted in the exclusion of other relevant studies in other languages. Furthermore, most of the studies reviewed were carried out in developed/Western countries, except for one study. As resilience is considered to be a dynamic construct that varies among cultures (Gunnestad, 2006), studies in other cultures or minority populations should be conducted. As noted, only the study conducted in a developing Eastern context found resilience to differ by gender and current living location (Bhattarai et al., 2018). This illustrates the need to conduct further studies focusing on how collectivist and individualistic societies, social network systems, and other environmental factors (e.g., accessibility of transportation, health care) can influence the development and maintenance of resilience in different ways among persons with SCI.
Second, the present review identified factors mainly based on descriptive studies. Out of 11, only one intervention study related to resilience was conducted among persons with SCI, and the intervention (cognitive-behavioral therapy) did not yield significant changes in resilience (Guest, Craig, Nicholson Perry, et al., 2015). Therefore, there is not enough evidence to demonstrate the causality or directionality of the relationship between resilience and its associated factors. More intervention studies targeting the specific factors (e.g., self-efficacy, social support, effective coping, employment) are imperative to enrich the resilience of persons with SCI. Randomized controlled trials and longitudinal studies are indicated to support the effectiveness of resilience-related interventions utilizing these contributing factors.
Third, the review included both qualitative and quantitative studies; therefore, it is not possible to establish the statistical associations between resilience and variables themes, particularly from qualitative studies. Conducting a future review more systematically using a formal systematic review process or meta-analysis design will help to establish the most accurate factors related to resilience. The authors of this review included all the available studies meeting the inclusion criteria, regardless of the quality of the studies. Therefore, it is recommended to use a numeric rating appraisal tool to critically appraise the quality of articles in the future.
Implications for Rehabilitation Practice
The findings of the current study may be helpful for rehabilitation counselors to provide effective interventions to people with SCI to enhance their resilience, quality of life, and ultimately, overall well-being. The goal of rehabilitation is to minimize the impact of disabilities and improve individuals’ functioning and well-being. This can be achieved by delivering resilience-strengthening interventions, with consideration to the aforementioned modifiable and non-modifiable factors (Bhattarai et al., 2018; Min et al., 2014). Kumpfer (1999) noted that the interaction between various personal and environmental or social factors is likely to result in resilience. Therefore, mobilizing and strengthening the individual’s strengths such as self-efficacy, social support, spirituality, coping strategies, and employment, and minimizing barriers (e.g., anxiety, depression, low self-efficacy, maladaptive coping, unemployment) may help to enhance resilience.
The review consistently identified self-efficacy and social support as the most significant positive contributors to resilience; therefore, interventions targeting these resources may be beneficial to promote resilience. For example, involving the individual in care planning and setting specific and realistic goals is fundamental in promoting self-efficacy. Interventions that enhance self-efficacy during the rehabilitation process may allow people with SCI to engage in work or community participation in the future (Driver et al., 2015). Motivating an individual to perform specific tasks of daily life (e.g., personal care, relationships, school, mobility, household chores) by setting small achievable goals may increase their sense of achievement and independence, which may further contribute to resilience (Kornhaber et al., 2017).
Most people with SCI require some degree of physical and emotional support from caregivers during the early rehabilitation process. As research suggests that attachment avoidance is related to low resilience (Dodd et al., 2015), rehabilitation counselors who understand attachment styles of clients may be better able to help the clients effectively move toward secure relationships. Similarly, improving the social skills of clients is likely to affect their resilience (Bonanno et al., 2012). Also, engaging family, friends, or significant others during the rehabilitation process can enhance the client’s sense of attachment and security. Rehabilitation professionals can also help clients to build supportive social networks in outpatient settings as well because resilience has been found to be lowered after discharge from the rehabilitation unit (Driver et al., 2015).
Rehabilitation counselors can also plan early vocational rehabilitation interventions for people with SCI. Rehabilitation counselors can act as liaisons between the client and the employer by contacting and providing information regarding the injury, potential limitations, available workplace supports or incentives available to the employer, and discuss the availability of suitable work for the client (Bloom et al., 2017). Consequently, achieving employment may enhance the resilience and overall quality of life of people with SCI. Although some of the factors identified in this review are non-modifiable (e.g., gender, age), identifying people in those risk groups and considering early and tailored interventions will be beneficial.
Conclusion
This review summarized and synthesized the factors that have been found to be associated with resilience among people with SCI. Many factors were identified. Some of those factors are modifiable; hence, rehabilitation counselors can design intervention strategies to promote the resilience of people with SCI. The review also revealed that resilience can be influenced by individuals’ cultural or social environments. Therefore, these factors need to be considered while developing interventions. Research on determinants of resilience is mostly limited to developed countries; future studies to explore this issue among persons with SCI in developing and/or Eastern countries are indicated. Overall, the current review serves as a guide for rehabilitation counselors to include factors contributing to resilience in clients’ rehabilitation plans. This will help to promote the effectiveness of rehabilitation services and effectively reintegrate the persons with SCI into their communities. Further intervention studies considering these factors are also needed.
Footnotes
Acknowledgements
The authors would like to acknowledge Faculty of Nursing, Prince of Songkla University, Thailand.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.