
Abstract
The present study aimed to investigate the indirect effect of appraisal of disability on the relationship between basic hope and coping strategies in women with long-term spinal cord injury (SCI), taking into account the moderating role of general self-efficacy. A cross-sectional study with 187 women with paraplegia in Poland was conducted. Main outcome measures, the Coping Orientations to Problems Experienced (COPE), the Basic Hope Inventory (BHI), Appraisals of Disability Primary and Secondary Scale (ADAPSS), and General Self-Efficacy Scale (GSES), were used. Our study showed that the strategies most commonly used by participants are seeking emotional support, religion, and acceptance. More than 45% of the respondents revealed average levels of basic hope, 58.82% revealed high levels of general self-efficacy, and most of them assessed their disability as determined resilience while noticing its negative aspects. The indirect effect of disability appraisal on the relationship between basic hope and coping strategies (denial, focus on emotions, seeking emotional support, religion, and acceptance) was confirmed. The moderating role of general self-efficacy in this analysis of mediating was also confirmed. General self-efficacy plays a significant role in explaining the relationship between basic hope and coping strategies mediated by appraisals of disability in women with long-term SCI.
Keywords
Spinal cord injury (SCI) is associated with numerous physiological, psychological, and social consequences, determining a wide range of challenges and stressful situations (Dickson et al., 2008; Post & van Leeuwen, 2012). The literature shows that gender is a factor differentiating everyday life with SCI (Anderson et al., 2008). Because SCI affects men more often, many areas of female functioning are overlooked in research (Samuel et al., 2007). Several studies have shown that women with SCI are in a much worse situation than men (Beigi & Cheng, 2010; Terrill & Molton, 2019) as a consequence of double discrimination, both on the basis of sex and experienced physical disability. The difficulties experienced by women with SCI are mainly related to their “assumed societal” gender roles such as mother or wife. They are also caused by structural barriers in society such as social exclusion, stereotypes related to their asexuality, and the inability or lack of competence to perform certain life roles (Lappeteläinen et al., 2017; Miller, 2009). However, previous research with women with SCI also shows there are positive aspects of their functioning, including effective coping and experiencing constructive posttraumatic changes (Byra, 2017a).
Understanding the role of disability, and especially long-term disabilities, in the lives of women is crucial to explain and enhance the overall quality of their lives (Coyle et al., 2000). Long-term SCI in women reveals some unique issues and concerns (Pentland et al., 2002) also related to coping. Women with SCI must deal not only with the permanent effects of SCI but also with age-related secondary health complications such as pain, fatigue, and skin problems (McColl et al., 2004), as well as possible developmental crises at different life stages associated with difficulties in fulfilling professional, parental, or social roles (Craig et al., 2015). For example, studies have shown women-specific challenges to living with neurogenic bladder and bowel (Nevedal et al., 2016). Despite the extensive knowledge of coping in people with disabilities, coping strategies in people with long-term disabilities, and specifically women, have not yet been analyzed sufficiently. The growing number of people with long-term disabilities in the population also justifies the need for analyzing how they adapt and cope with stress (Kennedy, Lude, et al., 2010; Molton & Yorkston, 2017). As research shows, the specificity of problems, the perception of functional changes (Amsters et al., 2005), coping, and adaptation (de Ruijter et al., 2018;) are related to the duration of SCI and may be specific for people with long-standing SCI (Cijsouw et al., 2017; Jőrgensen et al., 2017; Lundstrőm et al., 2017).
The theoretical background explaining coping and adaptation to long-term SCI is reflected, among others, in the SCI Adjustment Model (SCIAM) created by Craig et al. (2017) and Middleton and Craig (2008). According to this model, adjustment to SCI is “a complex process, multi-factorial in nature involving non-linear adaptation over time” (Craig et al., 2017, p. 124). This model was created to show and explain all aspects of adjustment to SCI, including the way individuals cope with stress and challenges involved in adjusting. It also explains how multiple factors lead to dynamic coping with adaptive or maladaptive outcomes of this adjustment. The definition of coping in this model is taken from Lazarus and Folkman (1984), who see it as “constantly changing cognitive and behavioral efforts to manage specific external and/or internal demands that are appraised as taxing or exceeding the resources of the person” (p. 141). Coping is the central element of the model. It is a product of combined predisposing factors including relatively stable personality traits and mediating factors (the importance of appraisal and perceptions). Physical aspects, psychological resources, and social factors can act as moderators of the relationship between appraisal and coping. Among psychological factors, generalized beliefs, such as general self-efficacy, play an important role. Importantly, sex and time since injury combine with moderators and mediators in this process as well (Craig et al., 2017).
Coping
The SCIAM explains coping as strategies that are determined by the specificity of difficult situations. Literature shows that people cope differently with the consequences of SCI (Buunk et al., 2006). Kennedy et al. (2000) have found that many individuals with SCI cope well after injury. In addition, Pollard and Kennedy (2007) have shown that coping strategies used by individuals with SCI remain relatively stable over time. They have found that early coping is very important because it helps to reduce the number of psychological problems after acquiring SCI, which is important especially for women who have higher levels of anxiety and depression than men (Rotarou & Sakellariou, 2018). Mazur et al. (2019) note that the ability to cope after a sudden loss of mobility differs among women and men with SCI. Women prefer more emotion-oriented coping and use less avoidance coping than men. Also, Livneh and Wilson (2003) and Byra (2011) have shown that women with physical disabilities use emotion-oriented coping more often than men. In reference to the SCIAM, coping strategies are determined by personal factors including relatively stable personality traits and cognitive functions, such as hope.
Hope as a Predictor
Hope is usually defined as future orientation (Snyder et al., 2006) and, according to researchers (Lohne & Severinsson, 2004; Parashar, 2015), is central to recovery after SCI. It is the force that spurs individuals. Hope was important to all participants of the research, providing energy and power for future recovery after SCI (Dorset et al., 2017; Lohne & Severinsson, 2006). In people with SCI, hope positively correlates with life satisfaction, positive coping styles, and self-reported adjustment (Felter et al., 2017; Kennedy et al., 2009; McDonald et al., 2018). Hope also negatively correlates with life problems and negative coping strategies (Livneh & Martz, 2014). In explaining coping with stress, basic hope is particularly important—it is a relatively stable personality trait and at the same time a psychological resource that shapes the individual’s response to new and difficult situations that require adaptation. Basic hope is a fundamental belief in two features of the world: its order and sense and general positivity toward humans (Trzebiński & Zięba, 2004). Basic hope positively correlates with disability acceptance, (Byra, 2014) posttraumatic growth, (Byra, 2018a), problem-solving coping (Byra, 2016), self-efficacy, and negatively with avoidance and emotion-focused coping in people with SCI (Byra & Ćwirynkało, 2018). Previous studies have shown a significant correlation between basic hope and coping strategies in people with long-term SCI (Byra, 2016). This relationship has not yet been tested separately among women, though. Furthermore, according to the SCIAM, the association between personality factors (here basic hope) is not direct and may be mediated by appraisal.
Appraisal of Disability as a Mediator
Appraisal of disability is generally understood here following Lazarus and Folkman’s (1984) assumptions about primary and secondary cognitive appraisal. Research has shown that individuals’ responses to SCI first result from the situation they are in (primary appraisal) and second, from the individual’s resources and coping strategies related to the situation (secondary appraisal; Kaiser & Kennedy, 2011). These appraisals are significant for the way individuals with SCI cope because they shape their choice of strategies (Kennedy et al., 2009). Differences have been noted in the configurations of coping styles and strategies after including disability appraisal as a challenge, loss, or a threat in people with physical disabilities (Byra, 2012). Appraisal as a loss or threat was found to be associated with using maladaptive coping strategies, and appraisal as a challenge was associated with active coping strategies in individuals with SCI (Byra, 2018b). There are few studies focused on the appraisal of SCI. McDonalds et al. (2018) note that despite the central role of cognitive appraisal for adjustment after injury, only recently has SCI-specific appraisal been highlighted as a key element in the experiences of individuals with SCI. Therefore, there is a need for further research into the role of primary and secondary appraisals following injury, especially in women, because there is a notable lack of research in this area.
Self-Efficacy as a Moderator
Self-efficacy refers to a personal belief or the degree to which a person is confident to perform a particular task and reach goals in specific situations (Bandura, 1977). In the SCIAM, general self-efficacy is a determining factor in the process of specific disability appraisal and consequently the choice of coping strategies. Therefore, it can be considered a factor moderating the relationship between basic hope, appraisal of disability, and coping strategies. Self-efficacy in people with SCI is negatively correlated with depression, anxiety, and stress (Craig et al., 2013; Geyh Sz Kunz et al., 2016) and positively correlated with well-being (De Roon-Cassini et al., 2009) and mental health (Peter et al., 2012). In addition, low levels of self-efficacy can be a primary risk factor for maladaptive adjustment in people with SCI (Craig et al., 2013). General self-efficacy is also an important determinant of coping with the encountered challenges (Bhattarai et al., 2018; Byra & Ćwirynkało, 2018; Umucu et al., 2016). Women with SCI have been found to have lower general self-efficacy than men (Byra, 2011). Referring to the SCIAM, general self-efficacy is a trait that does not change much over time and may be important for the relationship between basic hope, disability appraisal, and coping. These associations have not yet been tested in women with long-term SCI.
The Purpose of the Study
The current study aimed to investigate the mediating effect of appraisal of disability on the relationship between basic hope and coping strategies in women with long-term SCI, taking into account the moderating role of general self-efficacy. This research goal not only results directly from the assumptions of the SCIAM (Craig et al., 2017; Middleton & Craig, 2008) but also refers to relationships that are part of a more complex explanation of the relationships between factors in this model. Based on the assumptions of this model and earlier research, the following hypotheses were posited:
The assumed relationships between these variables are presented in Figure 1.
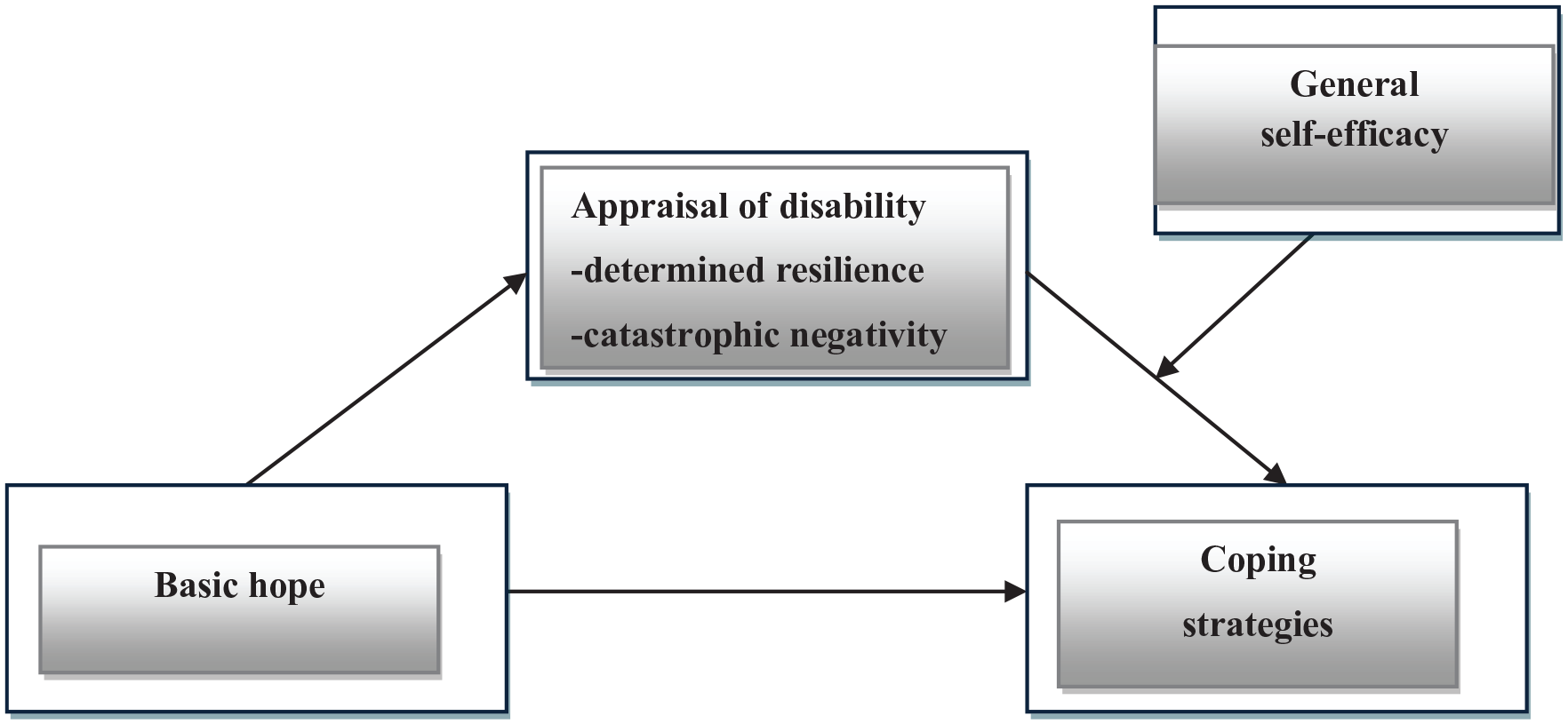
A conceptual model of relationships between variables.
Method
Participants and Procedure
In total, 210 women with paraplegia were selected for the study out of which 15 declined to participate. Eight sets of questionnaires were rejected due to incomplete data. Finally, 187 women with paraplegia participated in the study. Inclusion criteria included being an adult (≥18 years) woman with paraplegia. Women with diagnosed cognitive or communication impairment, anxiety-depressive disorders, neurological diseases, addiction to psychoactive substances, or after cerebral hemorrhages were not qualified for the study. Participant characteristics are presented in Table 1.
Sociodemographic Characteristics of Participants.
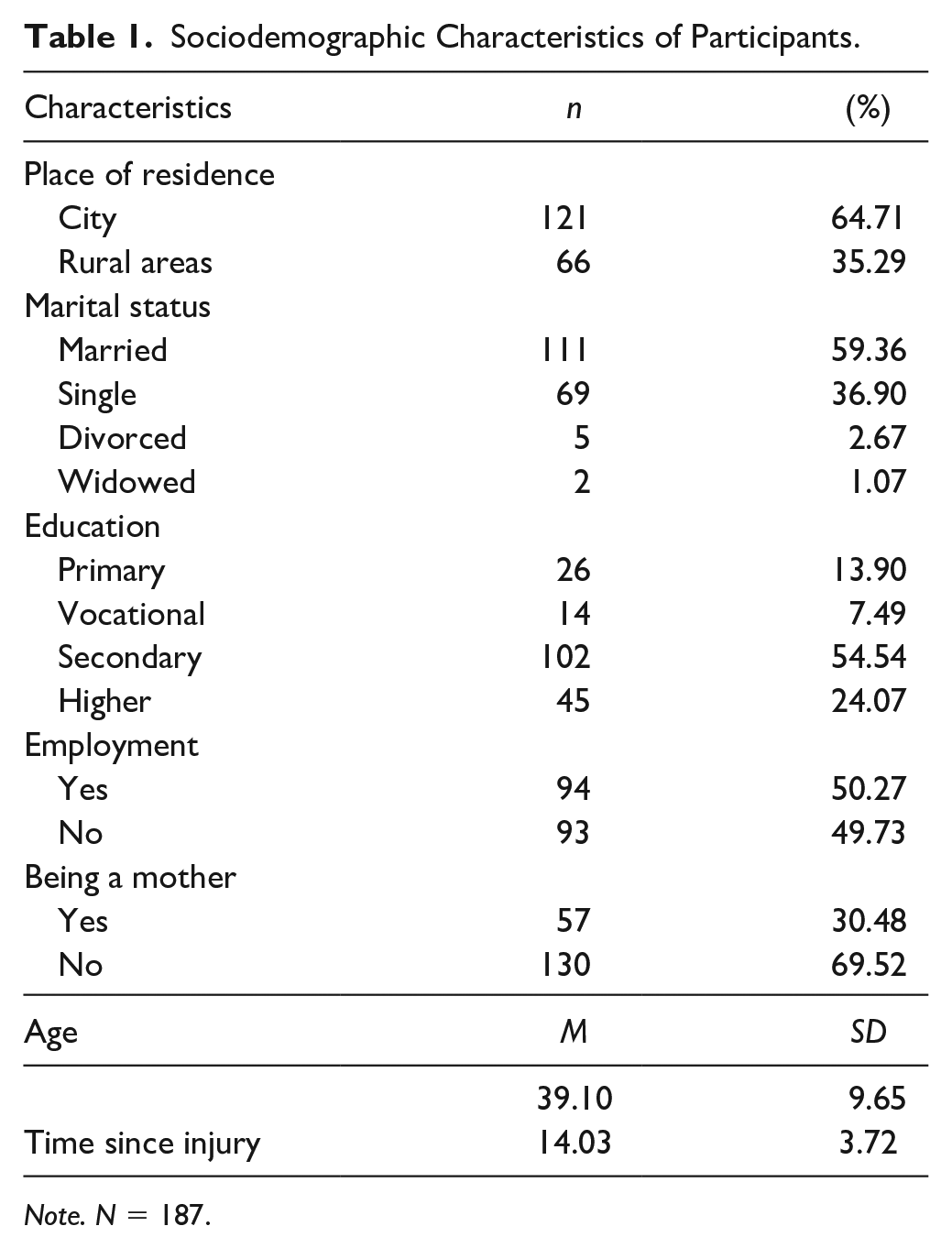
Note. N = 187.
Women with long-term SCI (>10 years) were invited to the study group through contacts with institutions employing persons with physical disabilities, associations, and foundations in Poland. These institutions engage clients in voluntary activities and provide support to women with SCI. The participants were approached when they were at the institution or foundation and were asked to complete a paper booklet of questionnaires. They gave consent to participate in the research without remuneration. The measurements were administered in person by the authors of this study. We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research. The research was a cross-sectional study based on self-reports. The paper-and-pencil procedure was used.
Instruments
The Polish version of the Coping Orientations to Problems Experienced (COPE) developed by Wrześniewski is a 60-item scale determining the frequency of applying the following strategies: focus on the problem (PRO), denial (D), focus on/venting of emotions (EM), seeking emotional support (SUP), acceptance (AC), religion (REL), humor (HUM), and alcohol/drug use ideation (ALK). Respondents reply to each statement using a 4-point scale, where 1 = I’ve never done that and 4 = I almost always did. Higher scores indicate more frequent use of particular strategies by the respondent. The Polish version of COPE showed good validity and reliability (Wrześniewski, 1996). In the present sample, Cronbach’s alpha of the individual subscales ranges from .65 to .92.
The Basic Hope Inventory (BHI) by Trzebiński and Zięba contains 12 statements evaluated by respondents on a 5-point Likert-type scale. It is used to determine the general level of basic hope manifested in personal beliefs about the world, its order, meaning, and positive nature. Higher scores imply greater basic hope. The psychometric properties of the instrument are satisfactory: Cronbach’s alpha = .70 (Trzebiński & Zięba, 2003). In the current study, Cronbach’s alpha was .83.
Appraisals of Disability Primary and Secondary Scale (ADAPSS) is a 32-item measure developed by Dean and Kennedy (2009). It consists of six subscales, which make up two scales: catastrophic negativity (CN) and determined resilience (DR). Higher scores in the catastrophic negativity subscale indicate more negative appraisals, whereas lower scores in the determined resilience subscale indicate more positive appraisals. The Polish version of ADAPSS showed good validity and reliability (Byra, 2017b). Cronbach’s alpha for the ADAPSS in the present sample for both subscales was .76.
In a Polish adaptation by Juczyński, the General Self-Efficacy Scale (GSES) contains 10 statements constituting one factor. It is used to determine the intensity of an individual’s general belief about the effectiveness of dealing with difficult situations. Answers to the questions are given on a 4-point scale, where 1 = not at all true, 2 = hardly true, 3 = moderately true, and 4 = exactly true. Higher scores imply greater general self-efficacy. It has satisfactory psychometric properties, including reliability (Cronbach’s α = .85) (Juczyński, 2001). In this study, Cronbach’s alpha was .84.
Data Analysis
The analyses were conducted in two stages. First, descriptive statistics and coefficients of correlations were prepared for the analyzed variables: coping strategies, basic hope, appraisal of disability, and general self-efficacy. Second, to test the hypothesis that general self-efficacy moderates mediation of the relationship between basic hope and coping strategies in women with SCI by appraisal of disability, the Preacher and Hayes’ (2004) procedure of bootstrapping was used. Mediation and moderation analyses of the identified indirect effects were carried out. Two dimensions of disability assessment were taken into account in the mediation analysis: determined resilience and catastrophic negativity. Indirect effects analysis was conducted using the PROCESS macro for SPSS through bootstrapping 5,000 subsamples at a confidence interval (CI) of 95% to test not only the indirect relationship but also the direct relationships between the constructs.
Results
Table 2 presents descriptive statistics for coping strategies, basic hope, appraisal of disability, and general self-efficacy. Participants had the highest scores in the following coping strategies: seeking emotional support, religion, and acceptance. The strategies least often used by them are alcohol/drug use ideation and humor. Most respondents (45.45%) had average, 22.99% had high, and 31.55% had low levels of basic hope. The sten scale analysis shows the overwhelming number (58.82%) of surveyed women had high, 29.95% had average, and 11.23% had low levels of general self-efficacy. Most surveyed women assessed their disability as determined resilience while noticing its negative aspects.
Means, Standard Deviations, and Correlations (Pearson’s r) Between the Analyzed Variables.
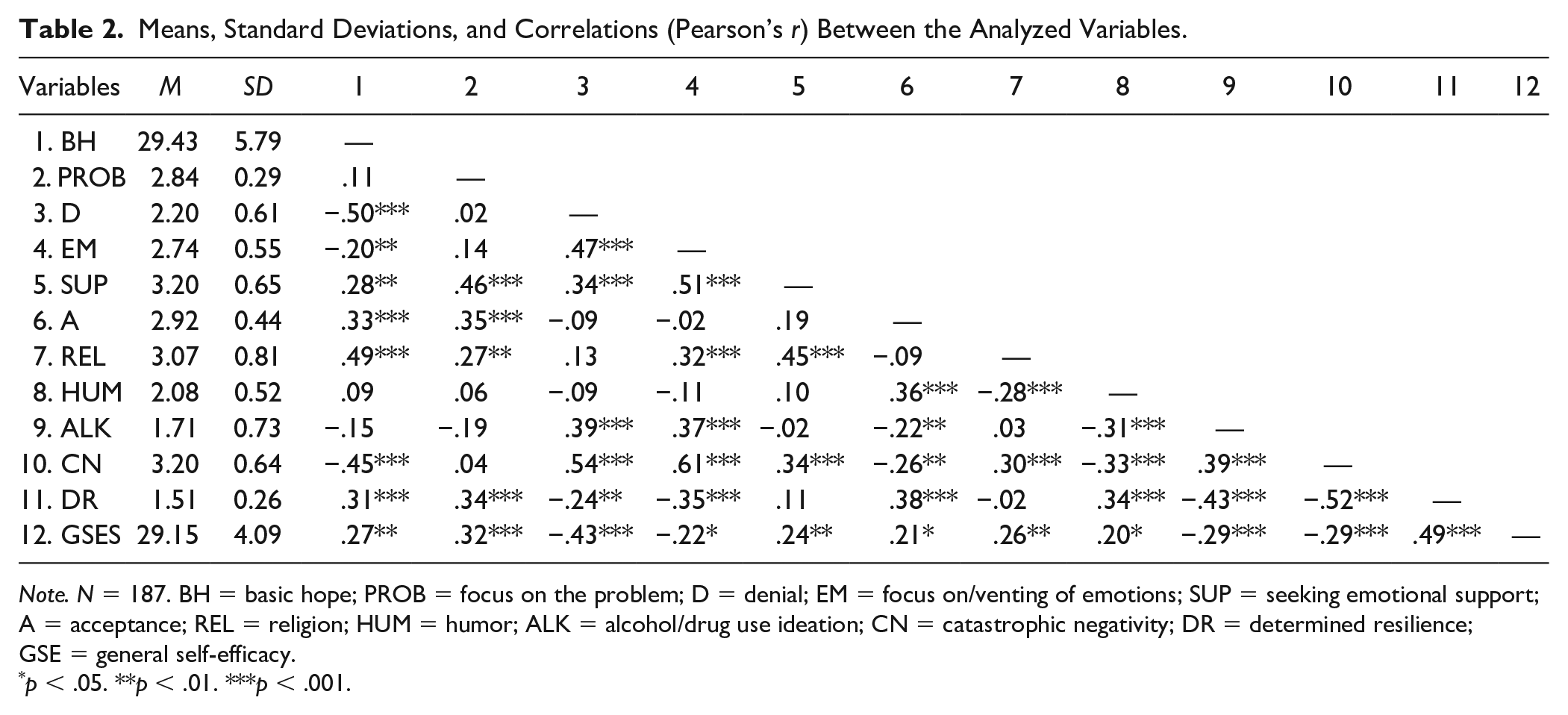
Note. N = 187. BH = basic hope; PROB = focus on the problem; D = denial; EM = focus on/venting of emotions; SUP = seeking emotional support; A = acceptance; REL = religion; HUM = humor; ALK = alcohol/drug use ideation; CN = catastrophic negativity; DR = determined resilience; GSE = general self-efficacy.
p < .05. **p < .01. ***p < .001.
Correlations
We predicted that basic hope and general self-efficacy would be positively associated with adaptive coping strategies and negatively associated with nonadaptive coping strategies. The results of the analysis are presented in Table 2. Basic hope was found to be positively correlated with coping strategies: focus on the problem, seeking emotional support, and religion, and negatively—and most strongly—with denial and focus on emotions. A negative link between basic hope and appraisal of disability as catastrophic negativity and a positive correlation between basic hope and determined resilience were also found. General self-efficacy correlated significantly with all coping strategies, with the strongest and negative link to denial. It also showed connections with appraisal of disability: positive with determined resilience and negative with catastrophic negativity.
Moderation
We predicted that the relationship between basic hope and coping strategies would be mediated by appraisal of disability, and that the strength of this mediation would be moderated by general self-efficacy. Therefore, the next step was moderation mediation analysis. It was assumed that the indirect effect of basic hope on coping strategies by disability appraisals varies as a function of general self-efficacy, where general self-efficacy moderates the path from appraisal of disability (catastrophic negativity or determined resilience) to coping strategies in the surveyed women with SCI. Mediated moderation models were analyzed for coping strategies that were significantly correlated with basic hope. These coping strategies included denial, focus on/venting of emotions, seeking emotional support, acceptance, and religion. No statistically significant correlations were found between basic hope and coping strategies: focus on the problem, humor, and alcohol/drug use ideation.
First, analyses tested whether general self-efficacy moderates mediation of the relationship between basic hope and denial as a coping strategy by appraisal of disability: catastrophic negativity or determined resilience. A significant interactive effect between catastrophic negativity and general self-efficacy was established (B = −0.234, SE = −0.111; CI = [−0.275, −0.116]). With high general self-efficacy, appraisal of disability was a significant negative predictor of denial (B = −0.010, SE = −0.029, CI = [−0.157, −0.039]). In addition, the effect of moderating mediation in the relationship analyzed here was obtained (B = −0.115, SE = 0.012, CI = [−0.036, −0.013]). Yet, this effect was established only for high levels of general self-efficacy (B = −0.188, SE = 0.037, CI = [−0.169, −0.112]), medium general self-efficacy (B = −0.027, SE = 0.029, CI = [−0.079, 0.367]), low general self-efficacy (B = −0.035, SE = 0.068, CI = [−0.103, 0.179]). Therefore, appraisal as catastrophic negativity mediates the relationship between basic hope and denial, when accompanied by high general self-efficacy. In this model, basic hope is a significant negative predictor of appraisal of disability as catastrophic negativity (B = −0.701, SE = 0.131, CI = [−1.150, −0.633]). The analysis showed that general self-efficacy is also a significant moderator of the indirect path between basic hope and denial by appraisal of disability as determined resilience (B = −0.193, SE = 0.071, CI = [−0.091, −0.022]). As in the case of catastrophic negativity, this effect was observed only for high general self-efficacy (B = −0.211, SE = 0.044, CI = [−0.117, −0.012]), medium (B = 0.019, SE = 0.009, CI = [−0.016, 0.087]), and low (B = 0.074, SE = 0.047, CI = [−0.023, 0.164]). Also, a positive interactive effect between disability appraisals as determined resilience and general self-efficacy was observed (B = 0.124, SE = 0.014, CI = [0.115, 0.276]), and basic hope was found to be a positive predictor of determined resilience (B = 0.481, SE = 0.110, CI = [0.263, 0.699]).
Next, analyses tested whether general self-efficacy moderates mediation of the relationship between basic hope and coping strategy as focus on/venting of emotions by appraisal of disability. In the case of catastrophic negativity, the moderation effect was statistically nonsignificant (B = −0.012, SE = 0.003, CI = [−0.008, −0.005]). However, it was established that general self-efficacy significantly moderated the indirect effect of basic hope on this coping strategy by determined resilience. A significant interactive effect between appraisal of disability as determined resilience and general self-efficacy was also noticed (B = −0.117, SE = 0.013, CI = [−0.012, −0.002]). Irrespective of the level of general self-efficacy, the effect of determined resilience on focus on/venting of emotions was negative and significant (high: B = −0.129, SE = 0.027, CI = [−0.182, −0.077]; medium: B = −0.102, SE = 0.021, CI = [−0.142, −0.609]; low: B = −0.073, SE = 0.019, CI = [−0.111, −0.035]). It was also observed that general self-efficacy moderates the mediation effect of determined resilience on the relationship between basic hope and focus on/venting of emotions (B = −0.191, SE = 0.036, CI = [−0.287, −0.021]).
The indirect path between basic hope and coping strategies—seeking emotional support, acceptance, and religion, by appraisal of disability, including general self-efficacy as the moderator of this mediation—was analyzed. The obtained results showed that for all three coping strategies, general self-efficacy does not moderate the indirect path by appraisal of disability as catastrophic negativity. A significant moderated effect of general self-efficacy on the mediation of the relationship between basic hope and these coping strategies by determined resilience was observed (see Table 3).
Moderation of the Indirect Path: Basic Hope and Coping Strategies: Seeking Emotional Support, Religion and Acceptance via Appraisal of Disability as Determined Resilience.

Note. N = 187. CI = confidence interval; GSE = general self-efficacy.
In the case of the relationship between basic hope and seeking emotional support, a moderating effect of general self-efficacy on the indirect path was established. Yet, this effect was obtained only for medium and high levels of general self-efficacy. The moderating effect of general self-efficacy was found also for mediation of the relationship between basic hope and acceptance. All three indirect effects were positive and significant. At the same time, the obtained results showed a statistically significant difference between the indirect effect for low and high general self-efficacy. The mediation analyzed here was stronger for high general self-efficacy. Interesting results were established for religion and the indirect association of this coping strategy with basic hope. Appraisal of disability as determined resilience was found to be a strong mediator of this relationship when accompanied by medium and high general self-efficacy. Nevertheless, negative indirect effects for these levels of general self-efficacy were obtained.
Discussion
The presented analyses tested the link between basic hope, appraisal of disability, general self-efficacy, and coping strategies in women with long-term SCI. Assumptions about these relationships are included in the SCIAM created by Craig et al. (2017) and Middleton and Craig (2008). The role of disability assessment as a mediator of the relationship between basic hope and coping strategies was tested, and the moderating role of general self-efficacy for this mediation. It was found that the assessment of disability as determined resilience was a mediator of the relationship between basic hope and coping strategies: denial, focus on/venting of emotions, seeking emotional support, acceptance, and religion. Assessment of disability as catastrophic negativity was also a mediator of the relationship between basic hope and denial. It was found that the higher the level of basic hope and disability appraisal as determined resilience, the more frequent the use of the coping strategy: seeking emotional support and acceptance. General self-efficacy moderated this mediation. With high general self-efficacy, the mediating role of determined resilience increases, which translates more strongly into the use of these strategies by women with long-term SCI. We also found that determined resilience mediated the relationship between basic hope and denial, focus on/venting of emotion and religion. Here, the mediating effects were negative and were associated with less frequent use of these coping strategies, higher basic hope, and determined resilience. Data also showed the moderating function of general self-efficacy for these mediations. In the case of the focus on/venting of emotions, determined resilience was a strong mediator regardless of the general self-efficacy level. It turned out, however, that high general self-efficacy was responsible for a stronger mediation of the relationship between basic hope and denial by catastrophic negativity.
In line with our expectations, the mediating effect of disability appraisal on the relationship between basic hope and coping strategies was confirmed. Furthermore, it was established that this mediation is moderated by general self-efficacy. These results complement the existing knowledge about coping in women with long-term SCI, indicating the importance of not only specific assessments directly related to disability but also generalized beliefs about the world, one’s own place in it (basic hope), and one’s own effectiveness in dealing with problems (general self-efficacy). It is likely that after a longer period of time since the acquisition of SCI, general self-efficacy may moderate the relationship between basic hope, appraisal of disability, and coping strategies, affecting the very assessment of SCI limitations and the quality of everyday life to a greater degree (Peter et al., 2012).
The mediating effect of disability assessment found here on the relationship between basic hope and coping strategies is consistent with the results of other research involving people with SCI (Kennedy, Smithson, et al., 2010). These results confirm the posited hypothesis (Hypothesis 2) and provide empirical evidence validating the assumptions of SCIAM regarding the nature of the relationship between these variables. In the light of the studies that found that basic hope may both promote positive appraisal of disability and weaken negative appraisal of disability in people with SCI (Byra, 2012), and the fact that disability appraisal determines the way of coping (Kennedy et al., 2009), our findings highlight the role of the general self-efficacy levels in explaining these relationships in women with long-term SCI. The moderating role of the general self-efficacy has been confirmed (Hypothesis 3). The obtained results indicate, therefore, that the level of generalized beliefs about self-efficacy in coping with difficulties, following the assumptions of SCIAM, significantly differentiates the indirect relationship between basic hope and coping strategies moderated by appraisal of disability.
The present study shows that the level of general self-efficacy significantly moderates the relationship between basic hope and denial as a coping strategy, mediated by two types of disability appraisal. Importantly, these mediated paths are significant for high general self-efficacy. Therefore, in women with high levels of general self-efficacy, denial is associated with basic hope in two ways, through (a) negative connections of basic hope with appraisal of disability as catastrophic negativity and positive connections with denial and (b) a positive relationship between basic hope and determined resilience, and negative with denial. These findings are partly consistent with existing study results. Many studies to date (Kaiser & Kennedy, 2011; Kennedy et al., 2009, 2016; Lequerica et al., 2008) reveal that negative assessment of disability—whose consequences are complex, impossible to control and change—correlates with avoidance as a coping strategy in the long-term adaptation process.
The importance of a high level of general self-efficacy revealed in the present research for the mediated relationship between basic hope and denial as a coping strategy shows, on one hand, the complex and ambiguous conditions of using this strategy by women with long-term SCI. On the other hand, it suggests that, in some situations, women with high general self-efficacy assess their disability and its consequences negatively and avoid overcoming obstacles by denying they are real or serious. This may be the case with the permanent unchangeable adverse effects of SCI. Awareness of the impossibility of changing these effects can, therefore, coexist with high general self-efficacy, which is a stable sense of personal competence to effectively deal with various difficult life situations (Luszczynska et al., 2005). In women with long-term SCI, denial can, thus, perform a temporal function by distorting the present situation and giving hope for the future, and a spatial function by limiting their perception only to the section of reality that is free from the adverse effects of SCI. Moreover, it helps women manage feelings of powerlessness and helplessness, allows them to stay motivated, and protects self-esteem and a positive self-image (Livneh, 2009). In the context of struggling with the long-term effects of SCI, where direct confrontation is inconsequential, denial may not have a negative impact but can act as a reliable stress-reducing mechanism (Livneh, 2009). This issue is interesting and complex, and it requires a more thorough examination in subsequent studies.
Our findings in the area of indirect links between basic hope and focus on/venting of emotions as a coping strategy by appraisal of disability also confirmed the importance of general self-efficacy as a moderator. Interestingly, regardless of its level, general self-efficacy moderates only the indirect path by disability appraisal as determined resilience, although the strongest mediation was found in women with high general self-efficacy. The results obtained here align with previous findings, which show that high general self-efficacy associates with positive disability appraisal and correlates negatively with emotional coping in people with SCI (Chevalier et al., 2009; Galvin & Godfrey, 2001).
The moderating role of general self-efficacy was also confirmed in the analysis of the mediating effect of disability appraisals on relationships between basic hope and seeking emotional support, acceptance, and religion as coping strategies. Our findings showed indirect positive associations between basic hope, seeking emotional support, and acceptance in women with at least moderate (or higher) general self-efficacy levels. Thus, they emphasize the key role of general self-efficacy. Admittedly, researchers stress the importance of specific aspects of self-efficacy in people with SCI in coping with particularly difficult situations following SCI (Miller, 2009). However, according to the SCIAM (Middleton & Craig, 2008) and the results obtained here, general self-efficacy as a moderator plays a significant role in explaining the relationship between basic hope and coping strategies mediated by appraisals of disability in women with long-term SCI.
The significant relationship found here between basic hope and selected coping strategies—denial, focus on/venting of emotions, seeking emotional support, acceptance, and religion—is consistent with existing research results (Byra, 2016; Dorset et al., 2017; Kennedy et al., 2009; Lequerica et al., 2008). However, contrary to other studies (Byra, 2012; Trzebiński & Zięba, 2004), no relationship was found here between basic hope and focus on the problem as a coping strategy. Referring to the theses put forward by Folkman (2010) on the links between hope and coping, there are two explanations for the results obtained here: (a) Hope (in this case basic hope) is necessary for those struggling with serious and long-lasting obstacles; (b) but, at the same time, hope is not a resource that marks its presence in every stressful situation and in every process of dealing with it. It is also possible that the relationship between basic hope and focus on the problem in women with long-term SCI is determined by some significant conditions in the long-term adaptation process that are not included in this study (Parashar, 2015). It is worth analyzing this issue in subsequent studies.
In conclusion, the already mentioned specific situation of women with SCI is an important context for the interpretation of the presented relationships between the analyzed variables. The specificity of this situation is expressed in women experiencing greater difficulties and challenges arising from social stereotypes, including those related to the implementation of the role of a wife or a mother. As shown in previous studies, women with SCI reported experiencing environmental barriers more frequently (Forchheimer et al., 2004) and more difficulties with finding and keeping jobs (Krause & Reed, 2011) than men with SCI. They may also experience social distrust of successfully coping with the challenges of daily life, including those related to motherhood, the ability to adequately and well care for their children struggling with the label of “a mother at risk” (Lappeteläinen et al., 2017). Their situation may also involve a daily struggle with disempowering, simplistic, socially accepted, societal narratives of “proper” motherhood and femininity determined by physical appearance (Malacrida, 2009). Hence, it is worth setting the efforts to understand the coping strategies adopted by women with SCI, their sense of self-efficacy, their assessment of their disability, and the relationships between these variables, in the broader context of social conditioning.
Limitations
The presented study shows interesting data on the assumed relationships between variables in SCIAM, which reveal the special role of general self-efficacy levels in women with long-term SCI in determining the relationship between coping strategies, basic hope, and disability appraisals. However, the study has limitations that should be signaled.
First, the studied group of women is significantly heterogeneous in terms of sociodemographics. Although they all have long-term SCI (>10 years), they may have various additional life experiences, resulting from fulfilling (or not) parental, professional, and other roles, which may affect the scope and nature of problems they need to solve. The factors that shape coping strategies for women struggling with the long-term consequences of SCI need explaining. However, over the course of life, problems closely related to SCI are superimposed by other problems related to individual developmental stages and associated with gradually increasing secondary disabilities (Galvin & Godfrey, 2001; Samuel et al., 2007). The present study does not consider what specific difficult situations women with long-term SCI deal with. Second, only women with paraplegia were included in the study to unify the sample in terms of the anticipated consequences of SCI. Extending the study group to people with different levels of SCI would provide additional information on coping strategies for long-term SCI, as well as their relationships with beliefs.
Third, following SCIAM, the gender variable was included in the study and the study focused on women with long-term SCI. To show the extent to which the relationship between basic hope and coping strategies with the participation of disability appraisals as a mediator and general self-efficacy as a moderator is specific for women with long-term SCI, it should also be checked for men. For example, Terrill and Molton (2019) indicate a higher frequency of midlife stressors and higher severity of depressive symptoms in women with a physical disability than in men. The comparison between men and women with long-term SCI is justified because women may face gender stereotyping. There is a greater pressure on women to fulfill maternal or parental roles, plus there are increased social expectations of an ideal female body image (Lappeteläinen et al., 2017).
Fourth, this was a cross-sectional study, which is a significant limitation on the interpretation of the results and inference. Although basic hope and general self-efficacy are considered to be relatively permanent dispositions, coping strategies and disability assessment are dynamic. The cause–effect relationships between these variables, tested in the presented study, were taken from SCIAM assumptions and longitudinal testing would yield more accurate results. Importantly, we obtained relatively low reliability of one of the COPE subscales (Cronbach’s α = .65) measuring the coping strategy focus on/venting of emotions. Conclusions regarding this dimension of coping should, thus, be treated with due caution.
Fifth, the presented study tests only some relationships from the complex SCIAM model. There are several other areas in this model that are not addressed in this study. Future research may analyze the importance of additional mediators of the relationship between biological, psychological, and social factors, and coping strategies such as resilience, motivational processes, as well as adaptive and nonadaptive behaviors.
Implications for Practice
Despite the indicated limitations, the results of the present research can be used for therapeutic purposes because they provide information on the importance of generalized beliefs (basic hope and general self-efficacy) in the application of certain coping strategies in women with long-term SCI, while also stressing the important role of disability assessment. Understanding the relationships between these variables can be significant in designing activities that support effective problem management in this group of women.
Empirical verification of the relationship between basic hope and coping strategies, with the contribution of disability appraisals and general self-efficacy, assumed in the SCIAM model, may be the first step in developing therapeutic and rehabilitation activities for women with long-term SCI. The obtained data show that higher basic hope is associated with more frequent use of adaptive coping strategies (i.e., seeking emotional support, acceptance, religion). On one hand, this indicates the need to appreciate this psychological resource in women with long-term SCI. On the other hand, the results show that the importance of this resource for coping is shaped through the assessment of disability as determined resilience and with the contribution of high general self-efficacy. These results support the need for rehabilitation practitioners to reinforce the constructive assessment of disability: perceiving it as a challenge and a motivating force to overcome the encountered obstacles (Kaiser & Kennedy, 2011). This can be done through specific coping training programs such as the Coping Effectiveness Training (CET; Duchnick et al., 2009) and cognitive–behavioral interventions (Mehta et al., 2011), which are largely based on the cognitive restructuring of the damage and the resulting long-term limitations. As self-assessment of disability is not static and may change with time (Kennedy et al., 2016), women with long-term SCI may need to cognitively rework their perception of disability to deal with problems successfully. The significant contribution of high general self-efficacy to explaining the links between assumptions about the world (basic hope), one’s disability (determined resilience), and adaptive coping strategies, established in the presented study, strengthens the awareness of the significance of this psychological resource as well. It is, therefore, desirable to measure general self-efficacy in women with long-term SCI, which may be important to understand, for example, the overuse of nonadaptive coping strategies. The fact that high basic hope and constructive appraisal of one’s disability may be insufficient for effective coping efforts may be important for rehabilitation counselors. Therapeutic interventions aimed at strengthening self-efficacy may prove necessary. Such interventions should include especially the ones that emphasize the central role of the individual in coping and managing their disability. Therapists should provide clients with the necessary knowledge, skills, and self-confidence to deal with the long-term consequences of SCI (Marks et al., 2005; Munce et al., 2016).
Based on the presented results, appraisal as determined resilience and high general self-efficacy can be construed as powerful tools for the promotion of adaptive coping in women with long-term SCI. Although the causal nature of the relationship between basic hope, determined resilience, and coping strategies cannot be determined on the basis of this cross-sectional study, it can still be argued that rehabilitation practitioners should include interventions that strengthen constructive beliefs in their work with women with long-term SCI. This is important because living with long-term SCI is associated with experiencing the so-called secondary disability and health complications, which translate into one’s assessment of disability (Molton and Yorkston, 2017).
The results of this study also provide empirical support for the hypothesis that high general self-efficacy may be closely related to a realistic assessment of experiencing some of the negative effects of long-term SCI and the use of denial as a coping strategy. As Livneh (2009) points out, denial is an inherent response to psychosocial adaptation, regardless of its stage. Understanding the use of denial in women with long-term SCI can be a valuable tool in planning realistic and comprehensive rehabilitation counseling. These women’s use of denial, while they have high general self-efficacy, may indicate temporary adaptability of this coping strategy, perhaps necessary in managing the long-term effects of SCI.
Conclusions
The following conclusions can be drawn from the presented research: (1) The relationship of basic hope (seen as a personal resource) and coping strategies in women with long-term SCI is mediated by disability appraisals: determined resilience (denial, focus on/venting of emotions, seeking emotional support, acceptance, religion) and catastrophic negativity (only denial); (b) general self-efficacy is an important moderator of the identified mediation. A high overall sense of self-efficacy reinforces the mediating role of disability appraisal as determined resilience, fostering, as a result, the use of constructive coping strategies by women with long-term SCI, mainly seeking emotional support and acceptance.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
Research data cannot be shared.