
Abstract
Objective
To evaluate the prognostic value of the combined neutrophil-to-lymphocyte ratio (NLR) and monocyte-to-lymphocyte ratio (MLR) for adverse outcomes in Taiwanese patients with acute coronary syndrome (ACS).
Methods
This retrospective, single-center, observational cohort study analyzed 653 ACS patients from the Tri-Service General Hospital-coronary artery disease registry (Jan 2016–Aug 2018). NLR and MLR were calculated at presentation. The primary endpoint was a composite of in-hospital mortality and stroke. Optimal cut-off values were determined using receiver operating characteristic curve analysis (NLR > 5.22, MLR > 0.76). Univariable and multivariable logistic regression were used to assess the association of both elevated NLR/MLR with the primary endpoint.
Results
Patients with both elevated NLR and MLR (NLR > 5.22 and MLR > 0.76) demonstrated a significantly higher risk of the primary endpoint compared to the group with no elevation (OR = 7.16) in univariable analysis. This group also experienced longer hospital stays and higher non-cardiovascular mortality. However, this association became non-significant after multivariable adjustment for confounders.
Conclusions
Concurrent elevation of both NLR and MLR at presentation is associated with increased in-hospital morbidity and prolonged hospitalization in ACS patients, although this did not remain an independent predictor in multivariable analysis. Ongoing statin therapy demonstrated a protective association in this cohort. These readily available markers may facilitate early risk stratification.
Keywords
Introduction
Coronary artery disease (CAD) remains the leading cause of mortality globally. 1 In Taiwan, CAD, primarily manifesting as acute coronary syndrome (ACS), is the second leading cause of death and imposes a substantial economic burden on healthcare resources. 2 ACS patients, including those with ST-segment elevation myocardial infarction (STEMI), non-ST-segment elevation myocardial infarction (NSTEMI), and unstable angina (UA), face significant risks of in-hospital mortality (ranging from 5.5% to 18.2%) and future major adverse cardiovascular events (MACEs). 3 Consequently, precise and timely risk stratification is paramount for optimizing management and improving clinical outcomes.
Current evidence highlighted that inflammation in ACS is not merely a localized response to plaque rupture but a systemic “low-grade inflammation” that dictates long-term vascular health. The persistent inflammatory milieu, characterized by the activation of both innate and adaptive immunity, remains a critical driver of MACE even after successful revascularization. 4 Moreover, hematological inflammatory indices have shown prognostic utility in ACS, stable CAD, and other vascular diseases, reflecting the systemic nature of vascular inflammation.5–7 While traditional biomarkers like troponin serve as the gold standard for myocardial necrosis, they offer limited insight into the underlying inflammatory activity.
In the acute phase of myocardial infarction (MI), neutrophils are the earliest cells recruited to the infarct site, where they activate phagocytosis and amplify the inflammatory cascade.8,9 Subsequently, monocytes migrate to the site and differentiate into macrophages; M1-type macrophages are primarily involved in the early clearance of debris, while M2-type macrophages, predominating from approximately 3 days post-MI, promote reparative fibrosis and scar formation. 10 In parallel, lymphopenia reflects stress-related adaptive immune suppression. By integrating neutrophil-driven inflammation, monocyte/macrophage-mediated repair processes, and lymphocyte-associated immune regulation, Neutrophil-to-Lymphocyte Ratio (NLR) and Monocyte-to-Lymphocyte Ratio (MLR) provide a comprehensive representation reflecting the balance between pro-inflammatory triggers and adaptive immune regulation after MI.
A large-scale meta-analysis revealed that high NLR is a potent independent predictor of both in-hospital mortality and long-term MACE in ACS patients. 11 Similarly, the MLR has been independently associated with 30-day and long-term mortality, particularly in STEMI populations.12,13 Moreover, both ratios correlate strongly with coronary lesion complexity (SYNTAX score) and established clinical risk scores such as GRACE.3,10,14
Recently, the combination of NLR and MLR presented its performance superior to either using NLR or MLR alone in predicting long-term MACE in patients with NSTEMI. 15 These hematological markers have also been applied to stratify the ACS patients and predict the response to therapy. 16 Therefore, we retrospectively utilized our CAD registry in Taiwan to further validate the prognostic value of a combined NLR and MLR in patients with ACS. To our knowledge, this was the first time in Taiwan to demonstrate the association of hematologic indices and clinical outcomes in this population.
Methods
Tri-Service General Hospital-CAD registry
This was a retrospective, single-center, observational cohort study utilizing data from the Tri-Service General Hospital-CAD (TSGH-CAD) registry. TSGH is a metropolitan medical center in Taipei, Taiwan. The registry has been collecting data since 2016.
The study was conducted in accordance with the Declaration of Helsinki (1975) and its later amendments (2024). The study protocol was approved by the Institutional Review Board of Tri-Service General Hospital, Taipei, Taiwan (IRB No. A202105210; Approved on January 12, 2022). All patient data were de-identified and anonymized prior to analysis to protect patient privacy; therefore, the requirement for informed consent was waived. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. 17
It enrolls eligible patients admitted with stable angina pectoris or ACS, all of whom underwent coronary angiography (CAG). Patients who received CAG for pre-operative evaluation before major cardiac surgery or post-transplantation follow-up without clinical suspicion of CAD were excluded from this cohort. All data within the TSGH-CAD registry were comprehensively reviewed and collected by a specialized research assistant, encompassing demographic characteristics, medical history, clinical presentation, 12-lead electrocardiography (ECG), laboratory and echocardiographic findings, coronary angiographic phenotypes, interventional procedure details, in-hospital morbidities, mortality, and medication. The registry records medications started at admission (or already in use) and confirms them at discharge, ensuring an accurate record of intended treatment during and after the hospital stay.
Study design and definition
We included patients presenting to the emergency department (ED) with ACS who underwent emergent percutaneous coronary intervention (PCI) between January 2016 and August 2018. ACS was defined as including UA, NSTEMI, or STEMI. Patients were excluded if they: (1) Were diagnosed with stable CAD or underwent elective PCI; (2) had conditions potentially confounding hematological indices, including overt infection, active or inactive malignancy, uremia requiring hemodialysis, or hepatic cirrhosis; or (3) had a fulminant clinical course (e.g. hemodynamic compromise resulting in same-day death).
STEMI was defined by typical symptoms of myocardial ischemia in association with persistent ST-segment elevation in ECG and subsequent release of cardiac biomarkers (i.e. creatine kinase-MB and Troponin-I level). Diagnostic ST-segment elevation in the absence of left ventricular (LV) hypertrophy or left bundle branch block was defined as new ST-segment elevation at the J point in at least 2 contiguous leads of ≥2.5 mm (0.25 mV) in men <40 years, ≥2.0 mm (0.2 mV) in men ≥40 years or ≥1.5 mm (0.15 mV) in women in leads V2-V3 and/or ≥1 mm in other contiguous precordial leads or the limb leads. 18 NSTEMI was defined by clinical symptoms of acute myocardial ischemia in combination with positive cardiac biomarkers (a rise and/or fall of cardiac troponin above the 99th percentile upper reference limit) and/or new ischemic ECG changes of ST segment depression or prominent T-wave inversion.19,20 The definition of obstructive CAD was more than 50% stenosis in one of the major coronary arteries. The multi-vessels CAD was considered at least two or three of the coronary arteries involved with atherosclerosis of significant severity.
The clinical classification used for assessment of disease severity in patients with ACS were Killip classification and TIMI classification for STEMI and NSTEMI individuals, respectively. The Killip classification, first published in 1967 was used frequently to predict mortality in patient with acute MI and this system focused on physical examinations, the development of heart failure and/or cardiogenic shock. 21 The TIMI risk score (age≥65, ≥3 CAD risk factors, known CAD with stenosis ≥50%, aspirin used in past 7 days, severe angina with ≥2 episodes in 24 h, ECG ST-segment changes ≥0.5 mm, and positive cardiac marker) was a prognostication scheme that predicted risk of death and ischemic events in patients with NSTEMI/UA. 22
Hematological measurements
At the time of the ED visiting, venous blood samples were collected from each patient and all hematological and biochemical analyses were performed. Complete blood counts included total white cell counts, hemoglobin, platelet counts, neutrophils, lymphocytes, and monocytes were recorded. NLR was calculated as the ratio of neutrophil to lymphocyte counts. MLR was calculated as the ratio of monocyte counts to lymphocyte counts. Estimated glomerular infiltration rate (eGFR) was calculated using the modification of Diet in Renal Disease equation: eGFR (ml/min/1.73m2)= 186×serum creatinine (mg/dl)−1.154×(age)−0.203×(0.742 if female)×(1.212 if black). 23
Clinical outcomes
The primary endpoint of this study was a composite of in-hospital mortality and in-hospital stroke. Secondary endpoints included each component of the primary endpoint (i.e. in-hospital mortality and stroke) and the length of hospital stay. An exploratory analysis was also conducted to evaluate the causes of in-hospital death, classified as cardiovascular (CV) or non-CV.
Statistical analysis
All continuous variables were presented as mean ± standard deviation for normally distributed data, or as median (interquartile range [IQR]) for non-normally distributed data. Categorical variables were presented as counts and percentages. To compare data between two independent groups, the unpaired Student's t-test or Mann-Whitney U test was used. To compare the differences between groups, one-way analysis of variance, Person chi-square test, Fisher exact tests and Kruskal–Wallis test were used as indicated. For post hoc analysis, Tukey's Honest Significant test, and pairwise Wilcox test were applied when suitable.
Receiver operating characteristic (ROC) curve analysis was utilized to determine the discriminatory ability of NLR and MLR for study outcomes. Optimal cut-off values for NLR and MLR were determined using the maximal Youden index.
To validate the predictive ability of hematological indices for the primary endpoint, univariable and multivariable logistic regression analyses were performed. Variables demonstrating a statistically significant association (p-value < 0.05) in the univariable analysis were entered into the multivariable logistic regression model to identify independent predictors. Multivariate logistic regression, adjusting for patients’ baseline characteristics, laboratory parameters, medications use, and clinical presentation were performed to identify independent predictors of our primary composite endpoint. All statistical analyses were performed with a software package (R 3.4.4), and differences were considered significant as p value <0.05.
Results
Study population
From January 2016 to August 2018, a total of 4061 patients were screened from the TSGH-CAD registry. After applying the exclusion criteria (detailed in the Methods section), 653 patients were ultimately included in the final analysis. The detailed patient selection process is illustrated in Figure 1.

Schematic presentation of the study population. The flow chart demonstrates the selection criteria and patient disposition in the TSGH-CAD registry. CAD: coronary artery disease; ACS: acute coronary syndrome; ACLS: advanced cardiac life support; TSGH-CAD: Tri-Service General Hospital-coronary artery disease.
Cut-off value of NLR and MLR
Given the absence of established reference values for NLR and MLR in ACS patients, ROC curve analysis was performed to determine their predictive ability for the composite endpoint of in-hospital mortality and in-hospital stroke, and to identify optimal cut-off values. The areas under the curve (AUC) for NLR and MLR were 0.511 and 0.487, respectively. Utilizing Youden's index, the optimal cut-off value for NLR was determined as 5.22 (sensitivity: 35.7%; specificity: 74.0%). For MLR, the optimal cut-off value was 0.76 (sensitivity: 14.3%; specificity: 97.5%).
Reclassification according to NLR/MLR ratio
Based on the cut-off value of NLR and MLR, patients were categorized into 3 groups. Patients had neither a higher level than the cut-off value of NLR nor MLR (NLR<5.22 and MLR<0.76) were defined to “No NLR/MLR” group. If patients had one of higher level in NLR or MLR (NLR≥5.22 or MLR≥0.76) were categorized to “One NLR/MLR” group. For those who had both elevated NLR and MLR level (NLR≥5.22 and MLR≥0.76) were referred to “Both NLR/MLR” group. Finally, there were 478, 155, and 20 patients in no NLR/MLR, one NLR/MLR and both NLR/MLR group, respectively.
Baseline characteristics of patients
The demographic characteristics of patients within three groups were demonstrated in Table 1. There were no significant differences among all baseline characteristics, except PAOD, use of MRA, beta-blocker and statin. The “One NLR/MLR” group had higher rate of MRA use then those in “No NLR/MLR” group (24.5% vs. 13%, p = 0.003). There was a significant lower rate of beta-blocker use in “Both NLR/MLR” than “No NLR/MLR”, and “One NLR/MLR” (50% vs. 75.9%, 76.1%, p = 0.030) group. Similar result was also found in statin use (40% vs. 81.8%, 76.8% in “Both NLR/MLR”, “No NLR/MLR”, “One NLR/MLR”, p < 0.001).
Characteristics of Patients With ACS and Different NLR/MLR Statuses.

ACS: acute coronary syndrome; NLR: neutrophil to lymphocyte ratio; MLR: monocyte to lymphocyte ratio; BMI: Body Mass Index; MI: myocardial infarction; CABG: coronary artery bypass grafting; TIA: transient ischemic attack; AF: atrial fibrillation; AFL: atrial flutter; PPM: permanent pacemaker implantation; PAOD: peripheral arterial occlusive disorder; ACE inhibitor: angiotensin-converting enzyme inhibitor; ARB: angiotensin-receptor blocker; MRA: mineralocorticoid receptor antagonist; eGFR: estimated glomerular filtration rate; LAD: left atrial dimension; LVEF: left ventricular ejection fraction; MVD: multi-vessels disease; STEMI: ST-segment elevation myocardial infarction; NSTEMI: non-ST-segment elevation myocardial infarction.
* indicates p < 0.05 compared to no NLR/MLR group.
† indicates p < 0.05 compared to one NLR/MLR group.
Correlation of NLR/MLR and disease severity in patients with ACS
Among our 653 ACS patients, 330 patients were presented with STEMI, 297 patients were NSTEMI, and 26 patients were UA. To test the correlation of disease severity and NLR/MLR level, we used Killip classification and TIMI classification in STEMI and NSTEMI patients, respectively (Figure 2). Among STEMI patients, those in the “Both high NLR/MLR” group had a significantly higher proportion of high Killip classification (p = 0.006). One the other hand, in patients presented with NSTEMI, there was no significant differences of the distribution of TIMI score between the three groups (p = 0.92).

Distribution of Killip classification in patients with STEMI and different NLR/MLR statuses. The Killip classification was significantly higher in both NLR/MLR group than other 2 groups (p = 0.006). However, the incidence of TIMI classification had no differences between the 3 groups (p = 0.92). MLR: monocyte-to-lymphocyte ratio; NLR: neutrophil-to-lymphocyte ratio; STEMI: ST-segment elevation myocardial infarction.
Clinical outcomes
During hospitalization, a total of 40 patients had in-hospital mortality and 3 patients had in-hospital stroke (Table 2). One patient had both a stroke and died during hospitalization. Patients in the “Both NLR/MLR” group exhibited the highest incidence rate for the primary composite endpoint (30.0%, 6/20), significantly higher than the “One NLR/MLR” group (5.8%, 9/155) and the “No NLR/MLR” group (5.6%, 27/478).
Clinical Outcomes of Patients With ACS and Different NLR/MLR Statuses.
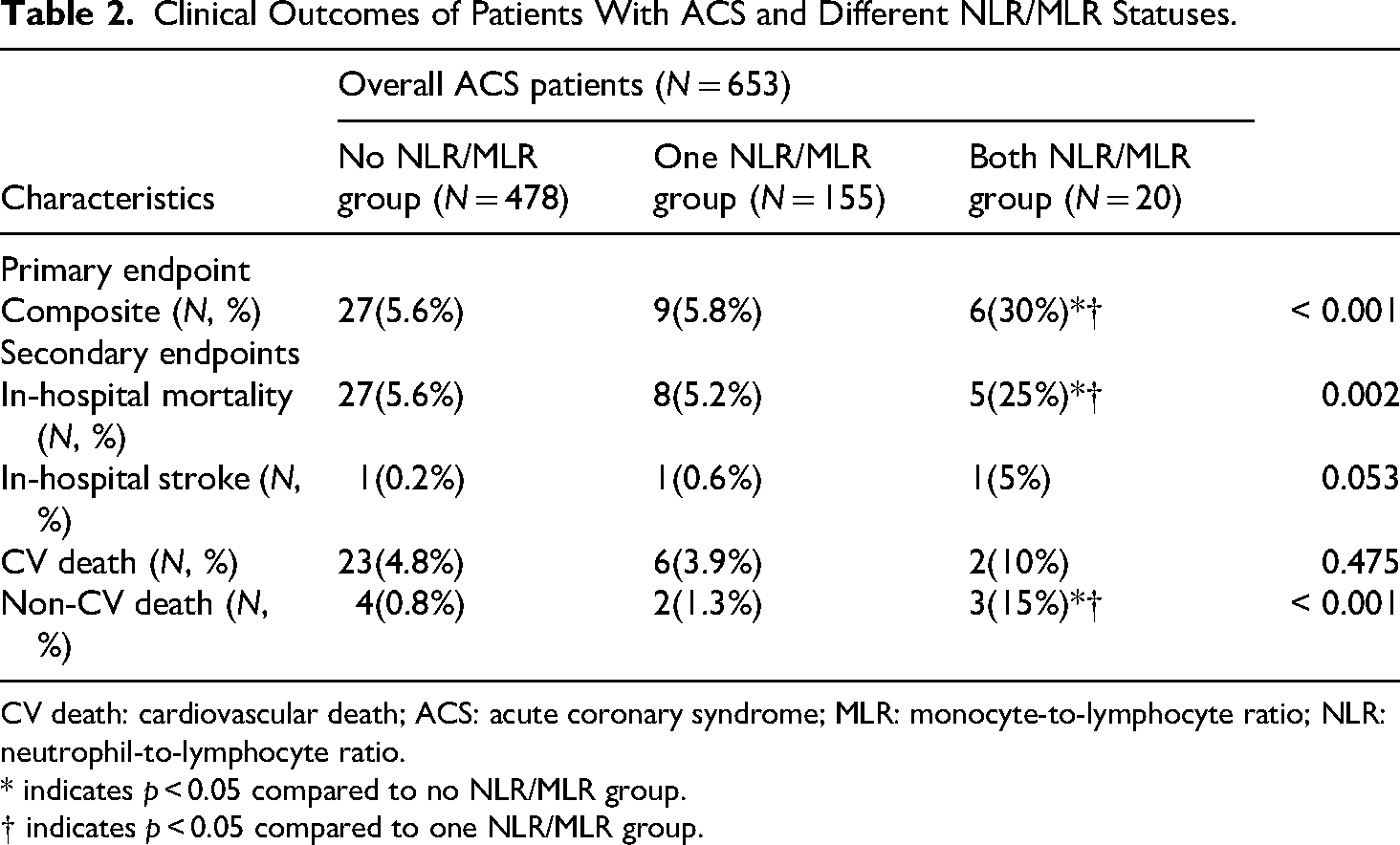
CV death: cardiovascular death; ACS: acute coronary syndrome; MLR: monocyte-to-lymphocyte ratio; NLR: neutrophil-to-lymphocyte ratio.
* indicates p < 0.05 compared to no NLR/MLR group.
† indicates p < 0.05 compared to one NLR/MLR group.
Regarding secondary endpoints, the “Both NLR/MLR” group demonstrated significantly higher in-hospital mortality rates (25%) compared to the “One NLR/MLR” (5.2%) and “No NLR/MLR” (5.6%) groups. Although numerically higher, the in-hospital stroke rate in the “Both NLR/MLR” group (5%) was not reach statistical significance when compared to the “One NLR/MLR” (0.6%) and “No NLR/MLR” (0.2%) groups.
In the analysis of the cause of in-hospital death, no significant differences in CV death were observed across the three groups. However, the “Both NLR/MLR” group had a markedly higher rate of non-CV death (15%) compared to the “One NLR/MLR” (1.3%) and “No NLR/MLR” (0.8%) groups.
As presented in Figure 3, both the “Both NLR/MLR” group (median 8.5 days, IQR 2–13.5, p = 0.06 vs. “No NLR/MLR”) and the “One NLR/MLR” group (median 5 days, IQR 3–8, p < 0.01 vs. “No NLR/MLR”) experienced longer lengths of hospital stay compared to the “No NLR/MLR” group (median 3 days, IQR 2–5). The interval from either admission or procedure date to death showed no statistically significant difference across the three groups.

The length of hospitalization, interval from admission to death and from procedure to death. The length of hospitalization was longer in both NLR/MLR group than one NLR/MLR(p = 0.06) and no NLR/MLR(p < 0.01) group. There was no difference in the interval either from admission or procedure date to death between each group. MLR: monocyte-to-lymphocyte ratio; NLR: neutrophil-to-lymphocyte ratio.
Prognostic value of combination of NLR/MLR
Logistic regression models were constructed to analyze the significant predictors of the primary composite endpoint across different NLR/MLR statuses in ACS patients (Table 3). Univariate logistic regression analysis demonstrated that elevation of both NLR/MLR was significantly associated with an increased risk of the composite endpoint compared to the “No NLR/MLR” group (OR = 7.16, 95% CI = 2.55–20.1; p < 0.001) and the “One NLR/MLR” group (OR = 6.95, 95% CI = 2.16–22.39; p < 0.001).
Univariate and Multivariate Logistic Regression Analysis for Predictors of in-hospital Mortality and Stroke in Patients With ACS and Different NLR/MLR Statuses.

OR: odds ratio; CI: confidence interval; ACS: acute coronary syndrome; MLR: monocyte-to-lymphocyte ratio; NLR: neutrophil-to-lymphocyte ratio; BMI: body mass index; ARB: angiotensin-receptor blocker; LDL: low-density lipoprotein.
Unadjusted model.
Adjusted for Age, BMI, prior history of myocardial infarction, prior history of heart failure, prior history of atrial fibrillation/flutter, estimated glomerular filtration rate, LDL-cholesterol, use of ARB, and statin.
For multivariable logistic regression analysis, variables including age, body mass index (BMI), history of MI, history of heart failure, history of atrial flutter/fibrillation, eGFR, serum low-density lipoprotein cholesterol (LDL-C), angiotensin-receptor blocker (ARB) therapy, and statin therapy were added to the predictive model based on univariate significance (p < 0.05). In the multivariable adjusted model, the association of “Both NLR/MLR” with the primary composite endpoint was no longer statistically significant when compared to “No NLR/MLR” (OR = 2.18, 95% CI = 0.44–10.73; p = 0.598) and “One NLR/MLR” (OR = 1.66, 95% CI = 0.29–9.42; p = 0.832) (Table 3). Independent predictors identified in the multivariable analysis included history of MI (OR = 3.48, 95% CI = 1.12–10.81; p = 0.030) and statin therapy, which demonstrated a strong significant protective effect against the primary endpoint (OR = 0.01, 95% CI = 0–0.06; p < 0.001) (Table 4).
Multivariate logistic regression analysis for predictors of in-hospital mortality and stroke in patients with ACS.

BMI: body mass index; eGFR: estimated glomerular filtration rate; ARB: angiotensin-receptor blocker; ACS: acute coronary syndrome; LDL: low-density lipoprotein.
Discussion
To our knowledge, this is the first analysis specifically evaluating the prognostic value of the combination of NLR and MLR in patients with ACS in Taiwan. This modest-sized, retrospective cohort study revealed several key findings. Elevated NLR and MLR were significantly associated with the composite endpoint of in-hospital mortality and stroke. These patients also exhibited higher Killip classification and prolonged hospital stays. Moreover, our analysis highlighted a strong protective association between statin therapy and improved clinical outcomes in this ACS population.
The role of immune cell system in the pathogenesis of ACS
The major pathophysiology underlying ACS, a spectrum of clinical disorders of myocardial ischemia or infarction, is atherosclerosis, characterized by potential atheromatic plaque disruption leading to rapid thrombosis and cessation of myocardial blood flow. 24 Accumulating evidence underscores the crucial role of the immune system and inflammation not only in atherosclerotic plaque formation but also in the progression of plaque erosion and/or rupture, ultimately culminating in ACS events.25,26
Neutrophils, the most abundant white blood cells, are a key component of the innate immune system and play a vital role in linking immune responses with atherosclerosis. Within atherosclerotic plaques, neutrophils can induce monocyte recruitment and adhesion in early atherosclerosis and promote proinflammatory processes, such as the release of inflammatory cytokines and reactive oxygen species, which are associated with plaque rupture.27,28 Studies have further demonstrated that neutrophil accumulation in eroded arterial plaques can amplify endothelial injury, superficial erosion, and local thrombotic complications via Toll-like receptor 2 signaling, as shown in mouse carotid artery models. 29 These findings support the notion that neutrophils influence atherosclerotic plaque stability and increase clinical thrombotic events.
Monocytes, the largest leukocyte subtype, differentiate into macrophages and myeloid dendritic cells. Macrophage infiltration followed by apoptosis or death of macrophages largely contributes to necrotic core formation within atherosclerotic plaques. 30 Several studies have elucidated the involvement of monocytes in the pathogenesis of both atherosclerosis and ACS. 31 Monocyte activation is an essential process preceding ACS, with activated monocytes interacting with endothelium leukocytes to trigger an inflammatory cytokine cascade. 32 Similar to neutrophils, circulating monocytes expressing TLR families (e.g. TLR-4) are found to accumulate both in the systemic circulation and at sites of plaque rupture. The increment of monocytes may represent a potential mechanism for AMI pathogenesis. 33
The prognostic value of NLR and MLR in ACS
Given the established role of the immune cell system in the pathophysiology and destabilization of atherosclerotic plaques, recent years have seen growing interest in the prognostic value of hematological indices for risk stratification and optimal management in ACS. 34
Regarding our specific indices, NLR has been extensively evaluated, with a large meta-analysis confirming high on-admission NLR as a reliable prognostic factor for short- and long-term adverse outcomes in various ACS types, irrespective of PCI. 14 However, the reported optimal NLR thresholds vary significantly (e.g. 3.04–8.84) across studies, indicating a lack of a universal standard.35,36 In our cohort, ROC analysis determined an NLR cut-off value of 5.22, which aligns with some previous findings, although the individual discriminatory power of NLR (AUC = 0.511) was modest.
MLR, while less frequently investigated in CV disease, has also demonstrated clinical impact on adverse outcomes in CAD patients. Studies show MLR obtained at 48 h post-admission can predict 30-day and long-term mortality in STEMI patients undergoing primary PCI, and increased monocyte counts and MLR are associated with CV mortality post-CAG.12,37 Similar to NLR, a standard MLR threshold is currently undefined. While some research used a lymphocyte-to-monocyte ratio (LMR) of 2.46 (equivalent to MLR of 0.41) as a threshold, our study derived an MLR cut-off value of 0.76. This variability in thresholds may be attributed to differences in the clinical characteristics of the studied populations.
Predictive performance of combination of NLR and MLR
Despite the non-specificity of hematological indices and potential variability in study results, their primary advantage lies in being relatively inexpensive, widely, and easily available for daily clinical practice. Recent literature supports the notion that combining NLR and MLR may offer superior predictive performance compared to individual markers and showed a stronger predictive performance for long-term MACE in NSTEMI patients after primary PCI. 15 While their study used lower cut-off values (NLR 2.15, MLR 0.36) compared to ours, this discrepancy might be attributable to our study population encompassing all ACS types (STEMI, NSTEMI, and UA).
In our study, we similarly validated the prognostic value of the combined NLR and MLR in a broader ACS cohort. Univariate logistic regression analysis confirmed that a high “Both NLR/MLR” status was significantly associated with an increased risk for the primary composite endpoint of in-hospital mortality and stroke (OR = 7.16, 95% CI = 2.55–20.1, p < 0.001 vs. “No NLR/MLR”; OR = 6.95, 95% CI = 2.16–22.39, p = 0.003 vs. “One NLR/MLR”).
However, upon adjusting for confounding variables in the multivariable model, the prognostic significance of concomitant NLR and MLR elevation for the primary composite endpoint was attenuated. This suggests that the initial predictive value of these inflammatory indices may be partially mediated by robust clinical and demographic determinants. Specifically, our results show that a history of MI is a potent independent predictor of adverse outcomes. This observation reinforces the paradigm that pre-existing myocardial injury diminishes cardiac reserve and heightens susceptibility to subsequent ischemic stress, thereby amplifying risk during acute inflammatory states. 38
Our findings are not entirely consistent with prior reports. These differences may reflect heterogeneity in study populations, including genetic backgrounds and baseline inflammatory profiles, or variations in multivariable adjustment strategies. 4 Notably, while many studies have emphasized long-term prognosis, our work focuses on the acute in-hospital prognostic utility of these indices. Crucially, we observed that the “high NLR/MLR” phenotype remained significantly associated with increased in-hospital mortality (predominantly non-CV) and prolonged hospitalization. This highlights the potential of combined NLR/MLR as a surrogate for global systemic vulnerability, extending beyond conventional CV risk stratification.
Anti-inflammatory effect of statin therapy influencing the outcome
During multivariate regression analysis, while the combined NLR/MLR lost statistical significance for the primary endpoint, we observed a strong protective effect of statin therapy on clinical outcomes (OR = 0.01, 95% CI = 0–0.06; p < 0.001). This finding reinforces the intricate relationship between inflammation and statin use. Numerous trials, including MIRACL, 39 PROVE IT-TIMI 22, 40 A to Z 41 and REVERSAL, 42 have consistently shown that statin therapy significantly reduces inflammatory markers like C-reactive protein. This anti-inflammatory effect is known to be both dependent and independent of HMG-CoA reductase inhibition and LDL-C reduction. 43
Intriguingly, patients in the “Both NLR/MLR” group, representing the highest inflammatory burden, also had the lowest rate of statin use (40%), despite experiencing the poorest clinical outcomes. This pattern resembles the “risk–treatment paradox”, in which high-risk patients are paradoxically less likely to receive guideline-directed medical therapy. In our cohort, this under-treatment might be attributed to clinical contraindications (e.g. hypotension or cardiogenic shock often seen in severe inflammation) or “clinical inertia” in managing these complex, critically ill patients.
Consequently, the coexistence of a high intrinsic inflammatory burden and insufficient statin therapy may have contributed to the excess mortality observed in this group, particularly from non-CV causes. Although specific causes of non-CV death (e.g. sepsis) were not individually adjudicated, elevated NLR and MLR likely reflect an underlying infectious or dysregulated immune state that increases vulnerability to fatal non-cardiac events during the acute phase. These findings emphasize the importance of early inflammatory risk assessment and the optimization of statin therapy in ACS management to improve overall clinical outcomes.
Study limitations
Our study had strengths including, firstly, we had a moderately large, studied population that allowed the investigation of NLR/MLR threshold and, secondly, we had a well-established CAD registry. Despite its strengths, several limitations existed. Firstly, consistent with previous research, there is currently no universally accepted, definite standard threshold for NLR and MLR in patients with different types of ACS. While we utilized Youden's index to determine cut-off values, we acknowledge the limitations of this method. The Youden index provides a point estimate that does not account for disease prevalence and can yield different “optimal” cut-offs depending on the dataset, leading to potential issues with reproducibility and “tie” values. The high diversity of thresholds reported across various studies highlights the challenge in establishing a generalized cut-off. Secondly, our study lacked long-term follow-up outcomes. Given the dynamic nature of hematological indices, a single on-admission measurement may have limited predictive power for long-term events. Thirdly, we did not have data on the clinical SYNTAX score, which reflects the severity of CAD. Some studies suggest a correlation between hematological indices and coronary severity, and the absence of this data could be a confounding factor. Fourthly, as a retrospective, single-center cohort study, our findings are inherently subject to potential selection and information biases, and their generalizability to other populations or clinical settings may be limited. Finally, the relatively small sample size of the “Both NLR/MLR” group (N = 20) might have reduced the statistical power for detecting significant associations in multivariate analyses, potentially contributing to the loss of significance for the primary composite endpoint after adjustment.
Conclusion
In patients with ACS, concurrent elevation of both NLR and MLR at first presentation to ER was independently associated with increased risks of in-hospital mortality, stroke, and prolonged hospitalization. These simple and readily available hematological markers may facilitate early risk stratification and guide clinical management in this population.
Footnotes
Acknowledgements
The authors would like to thank all colleagues who contributed to this study.
ORICD information
Yu-Cheng Chen 0009-0002-5899-6106
Chiao-Chin Lee 0000-0002-5220-7551
Ethic approval
This study was ethically approved by the institutional review board (IRB NO. A202105210) in Tri-Service General Hospital, Taipei, Taiwan. The authors have no competing interests to declare that are relevant to the content of this article. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author contributions
Yu-Cheng Chen performed the data analysis, statistical modeling, and drafting the initial manuscript. Chiao-Chin Lee conceived and designed the study, supervised the entire project, critically revised the manuscript, and served as the corresponding author. Tzu-Chuan Huang contributed to the conceptualization and interpretation of the hematological parameters (NLR and MLR). Wen-Yu Lin, Chin-Sheng Lin, Chiao-Hsiang Chang, Jun-Ting Liou, Cheng-Chung Cheng, Shih-Ping Yang, Shu-Meng Cheng, Yen-Lien Chou, Fan-Han Yu, Ya-Ju Chen, Chih-Hsueng Hsu, Tsung-Neng Tsai, Chun-Hsien Wu, Wei-Che Tsai, Tzu-Chiao Lin, Wen-Cheng Liu, Yuan Hung, Da-Wei Chang, Yu-Lan Liu, Wei-Shiang Lin contributed to data acquisition, data validation, and critical review of the manuscript. All authors approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data is not publicly available due to their containing information that could compromise the privacy of research participants and are governed by IRB and hospital regulations.